Organizational management of moderate and severe paediatric traumatic brain injury: results from a European survey
Sarah Hornshøj Pedersen, Radek Frič, Shruti Agrawal, Chiara Robba, Aurelia Peraud, Miroslav Gjurasin, Ondra Petr, Marianne Juhler, Bart Depreitere

TL;DR
A European survey shows low case numbers and uneven access to expertise in managing moderate/severe pediatric traumatic brain injury.
Contribution
First European survey examining organizational management of moderate/severe pediatric traumatic brain injury.
Findings
Most centers reported fewer than 20 pediatric TBI cases annually.
Access to pediatric anesthesiology correlates with hospital size.
Confidence in care delivery is higher in centers with pediatric neurotrauma specialists.
Abstract
Management of moderate/severe paediatric traumatic brain injury (mspTBI) varies across Europe. The decline in case numbers perceived in many regions raises concerns about maintaining high-quality, sustainable care. This study aimed to examine the organization of mspTBI management in Europe, focusing on expertise availability, guideline adherence, neuromonitoring use, and clinician's confidence in care delivery through a survey. A 34-question survey was distributed to European neurosurgical and intensive care communities. Only hospitals treating children with mspTBI were included. Centres were stratified by their catchment population size and their access to dedicated expertise. Seventy-six institutions from 23 countries responded. Most centres reported a mspTBI case load of less than 20 children per year. Access to paediatric anesthesiology was significantly associated with centre…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
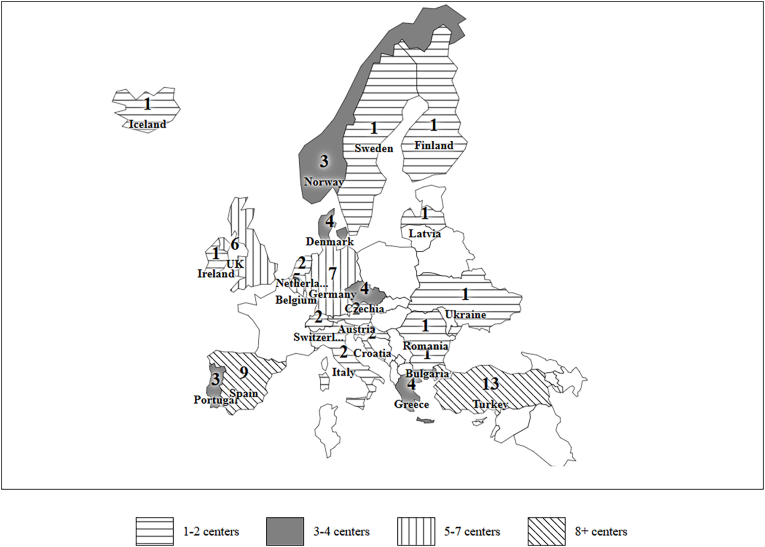 Figure 1
Figure 1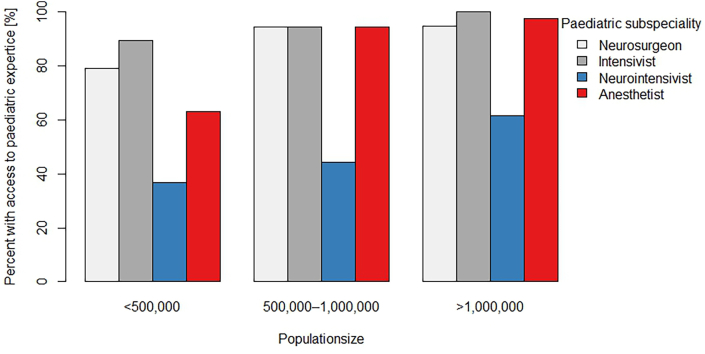 Figure 2
Figure 2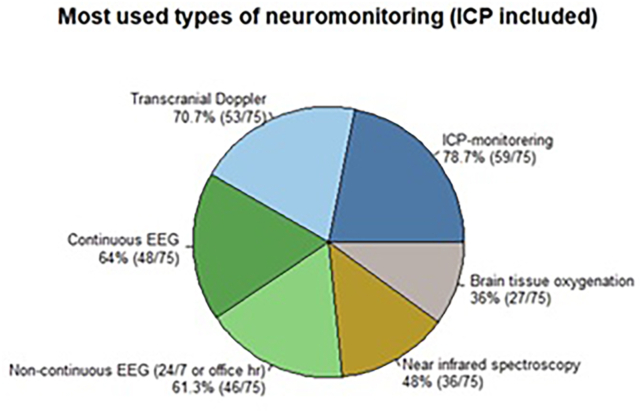 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury and Neurovascular Disturbances · Child Abuse and Related Trauma · Traumatic Brain Injury Research
Introduction
1
Paediatric traumatic brain injury is a major contributor to morbidity and mortality in children worldwide. More seriously injured children, those with moderate to severe traumatic brain injury (mspTBI), have a profound impact on healthcare systems, families, and society (Dewan et al., 2016). While the incidence of mspTBI in children appears to be declining in most high-income countries, including Europe (Guan et al., 2023; Dahl et al., 2021; Maas et al., 2022; Feigin et al., 2021), it remains a high-impact condition requiring prompt, resource-intensive, and often prolonged multidisciplinary care. Optimal management of mspTBI involves coordinated neurocritical care, neurosurgical expertise and paediatric-specific rehabilitation.
There are several different models of practice in the management of mspTBI, with significant variations among countries and in some cases also within the same country (Wickbom et al., 2022; Chung et al., 2024). It is not clear how these variations affect the quality of care for these patients. With the decline in incidence of severely injured children, many centres may find themselves managing fewer cases annually. This trend, although positive, raises critical questions about how to best maintain clinical expertise, allocate resources efficiently, and design models of care that are both effective and sustainable. In particular, understanding current hospital capabilities, paediatric subspecialist availability as well as the requirements for best patient outcomes are important.
Despite the clinical importance of these issues, published data on infrastructure and access to care for mspTBI remain limited in the European context (Bruns et al., 2021; Trefan et al., 2016; Jochems et al., 2021). Further, there is limited consensus on how services should be organized and how clinical expertise can be maintained in the context of decreasing caseloads. To address this gap, we conducted a survey describing the organization and practices of mspTBI management across different European countries.
Methods
2
Population
2.1
The target population consisted of 1) the general neurosurgical community in EANS (European Association of Neurosurgical Societies) member countries, 2) the paediatric intensive care community in ESPNIC (European Society of Pediatric and Neonatal Intensive Care) member countries, and 3) the general intensive care community in ESCIM (European Society of Intensive Care Medicine) member countries. All individual members of the three societies were invited to participate in the survey.
To collect a representative dataset without multiple entries from the same institution, we asked the respondents (neurosurgeons and intensive care specialists) to submit only one survey on behalf of their institution. Duplicates and incomplete surveys were removed from the dataset after clarifying with the respondents. Non-European hospitals and hospitals only treating adults were excluded. There were no additional exclusion criteria. The information provided was treated confidentially and, after closing the dataset, analyzed in an anonymized manner.
Design
2.2
The survey was designed and elaborated in a working group consisting of the authors representing all three scientific societies. Before circulating the questionnaire to members of the EANS, ESPNIC and ESCIM, it was tested, approved and endorsed by all three societies. The survey consisted of 34 questions divided into seven main sections: A) Hospital setting and resources; B) Management of mspTBI in the hospital, distinguishing between children (2–18 years of age) and infants (0–2 years of age); C) Specialist in-charge of mspTBI; D) Availability of paediatric subspecialty expertise; E) Rehabilitation and follow-up; F) Registry; and G) Opinion (the full questionnaire is provided in Supplementary material).
The 34 survey questions generated a large number of answers, from which we selected four focus areas. Within each focus area, one indicator question was selected based on content matching of the focus area, the clarity of the data (i.e., the answer options) and completeness of answers.
Statistical analysis
2.3
We used a stratified approach subgrouping participating centres firstly according to catchment population size (<0.5 million, 0.5–1 million and >1 million), and secondly according to access to subspecialty expertise in paediatric neurosurgery and paediatric intensive care. This strategy was based on the underlying hypothesis that availability of dedicated expertise is related to the size of the catchment population. We subsequently investigated whether access to such expertise in mspTBI care was associated with.
- •adherence to paediatric TBI guidelines
- •use of invasive intracranial (ICP) monitoring
- •use of multimodal monitoring
- •clinician confidence in treatment of children and infants with moderate/severe TBI
Expert availability was defined as the presence of 24/7 coverage, either through a formally established on-call service or availability without formal on-call arrangements. Access was stratified across four paediatric subspecialist domains: neurosurgery, intensive care, neuro-intensive care, and anaesthesia. For analysis, availability within each domain was dichotomized (yes/no). The questionnaire further distinguished between the Scandinavian guidelines for initial management of minor and moderate head trauma in children, 2016 (Astrand et al., 2016); Italian guidelines on the assessment and management of pediatric head injury in the emergency department, 2018 (Da Dalt et al., 2018); Guidelines for the management of pediatric severe traumatic brain injury, 3rd edition, Update of the Brain Trauma Foundation, 2019 (Kochanek et al., 2019); The management of pediatric severe traumatic brain injury: Italian Guidelines, 2021 (Bussolin et al., 2021), and other national or local child-specific guidelines. However, as the recommendations across these are essentially similar, we did not differentiate them in the analysis.
Data are presented as medians and percentages. Centres are compared using Fisher's exact test due the relatively small number of centres in each group. Statistical analyses were conducted in R Studio v 2024.04.2.
Results
3
An overview of participating countries with total estimated paediatric population size as well as number of included centres per country and their characteristics are shown in Fig. 1and Table 1, Table 2. After removal of duplicate institutions and non-European respondents, there were 76 separate entries (institutions) from 23 countries across Europe. The majority were academic and Level 1 trauma centres. More than three quarters of the respondents (n = 59; 78 %) treated both adult and paediatric TBI, while only 17 respondents (22 %) were children-only institutions. One respondent reported treating only adult patients and was thus excluded.Fig. 1. Geographical distribution of centres participating in the survey.Fig. 1. Table 1Demographics of the participating countries.Table 1. CountryEstimate of total population size∗Percent of total population under age 18 year [%]Percent of total population under age 2 year [%]Number of centres responded to the surveyAustria8,980,00019.42.12Belgium11,500,00021.32.45Bulgaria6,800,00017.62.01Croatia3,900,00018.52.12Czechia10,700,00019.02.24Denmark5,890,00020.32.24Finland5,540,00019.22.01Germany83,100,00018.12.07Greece10,400,00018.42.14Iceland375,00020.12.21Ireland5,100,00022.02.31Italy59,000,00017.71.92Latvia1,860,00018.02.01Netherlands17,400,00022.02.52Norway5,420,00021.52.43Portugal10,300,00019.72.13Romania19,000,00020.02.31Spain47,400,00019.02.09Sweden10,400,00020.32.11Switzerland8,900,00018.52.02Turkey86,900,00027.23.013Ukraine37,000,00022.12.41United Kingdom68,000,00020.62.36Number of participating centres per country, in addition to the total population size and percentage children and infants per country (DelSignore and Tasker, 2017).Table 2. Characteristics of participating hospitals.Table 2. CountryHospital type (mixed children/adults or children only)Trauma Centre LevelPopulation sizeAustriamixedlevel 1>1,000,000mixedlevel 1500,000–1,000,000Belgiummixedlevel 1<500,000mixedlevel 1>1,000,000mixedlevel 2<500,000mixedlevel 1500,000–1,000,000mixednot applicable<500,000Bulgariamixedlevel 1500,000–1,000,000Croatiachildrenlevel 1>1,000,000mixedlevel 1>1,000,000Czechiamixedlevel 1>1,000,000mixedlevel 1500,000–1,000,000mixedlevel 1500,000–1,000,000mixedlevel 1>1,000,000Denmarkmixedlevel 1>1,000,000mixedlevel 1500,000–1,000,000mixedlevel 1>1,000,000mixedlevel 1>1,000,000Finlandchildrenlevel 1>1,000,000Germanymixedlevel 1500,000–1,000,000childrenlevel 1>1,000,000mixedlevel 1>1,000,000mixedlevel 1500,000–1,000,000childrenlevel 1<500,000mixedlevel 1>1,000,000mixedlevel 1500,000–1,000,000Greecemixedlevel 3>1,000,000mixedlevel 1500,000–1,000,000childrenlevel 1>1,000,000mixednot applicable<500,000Icelandmixedlevel 1<500,000Irelandchildrenlevel 1>1,000,000Italychildrenlevel 1500,000–1,000,000childrenlevel 1>1,000,000Latviachildrennot applicable<500,000Netherlandsmixedlevel 1>1,000,000mixedlevel 1<500,000Norwaymixedlevel 3>1,000,000mixedlevel 1500,000–1,000,000mixedlevel 2500,000–1,000,000Portugalmixedlevel 1>1,000,000childrenlevel 1>1,000,000childrenlevel 2>1,000,000Romaniamixedlevel 1<500,000Spainmixedlevel 1>1,000,000mixedlevel 1500,000–1,000,000mixedlevel 1<500,000childrenlevel 1>1,000,000mixedlevel 1<500,000mixedlevel 1>1,000,000mixedlevel 1<500,000mixedlevel 1>1,000,000mixedlevel 1>1,000,000Swedenmixedlevel 1>1,000,000Switzerlandchildrenlevel 1>1,000,000childrenlevel 1<500,000Turkeymixedlevel 2>1,000,000mixednot applicable>1,000,000mixedlevel 1500,000–1,000,000mixedlevel 2>1,000,000childrenlevel 1<500,000mixedLevel 2<500,000mixednot applicable<500,000mixednot applicable>1,000,000mixedlevel 3>1,000,000mixedlevel 2<500,000mixednot applicable<500,000mixedlevel 1>1,000,000mixednot applicable<500,000Ukrainemixedlevel 1500,000–1,000,000United Kingdomchildrenlevel 1500,000–1,000,000mixedlevel 1>1,000,000mixedlevel 1>1,000,000mixedlevel 1>1,000,000childrenlevel 1>1,000,000mixedlevel 1>1,000,000Hospital characteristics in terms of paediatric vs. mixed service, trauma centre level and catchment population size.Trauma centre Level 1: most comprehensive trauma care; Level 2: almost full coverage 24 h; Level 3: no 24 h and no full coverage.
Case load and expertise availability
3.1
More than half of the institutions (n = 46; 61 %) reported an annual case load of less than 20 mspTBI in the 2–18 years group, while 87 % (n = 66) reported similar annual case load in the 0–2 years group. The reported median full time equivalent (FTE) specialists per centre were 10 (range 2–50) for neurosurgery and 15 (range 1–140) for intensive care. For both specialties, the median FTE of specialists active in the paediatric subspecialty for more than 50 % of their practice was 2 and 6, respectively. Availability of dedicated paediatric subspecialty expertise relevant for mspTBI is shown in Fig. 2. Availability of pediatric anesthesiology was significantly higher in larger centres (p = 0.001). However, availability of paediatric neurosurgery (p = 0.132), paediatric intensivist (p = 0.111) or paediatric neurointensivist (p = 0.234) was not associated with the centre size. Thirty-six institutions (47 %) reported a 24/7 formal on-call service for paediatric neurosurgery, 65 (86 %) for paediatric intensive care, 20 (26 %) for paediatric neurointensive care and 53 (70 %) for paediatric anaesthesia. Most institutions (72; 95 %) reported access to rehabilitation services following mspTBI, with 51 (67 %) reporting dedicated paediatric rehabilitation.Fig. 2. Availability of paediatric subspecialist care (for neurosurgery, intensive care, neurointensive care and anesthesiology) in participating hospitals in relation to catchment area population.Fig. 2
Adherence to guidelines
3.2
Most respondents (n = 73; 96 %) reported the use of national or international guidelines for managing mspTBI. Of these, 68.5 % applied a single guideline (n = 50), while 24.7 % used two (n = 18). Among respondents using one guideline, the most frequently applied was the Brain Trauma Foundation Guidelines for the Management of Pediatric Severe Traumatic Brain Injury (3rd edition, 2019), used by 41 of 50 respondents (82 %). For those using two guidelines (n = 18), the Brain Trauma Foundation guidelines were included in 17 cases, and were in 11 of these supplemented by a national or local guideline.
Overall, 63 respondents used the Brain Trauma Foundation guidelines, 22 reported using local or national guidelines, 13 used the Scandinavian guidelines for initial management of minor and moderate head trauma in children (2016), 4 used The management of pediatric severe TBI: Italian guidelines (2021), and 1 used the Italian guidelines on the assessment and management of pediatric head injury in the emergency department (2018). Guideline use was independent of 24/7 availability of expertise in the four paediatric subspecialist domains [neurosurgery (p = 1.0), intensive care (p = 1.0), neuro-intensive care (p = 0.605) and anesthesiology (p = 0.319)].
ICP monitoring and multimodal monitoring
3.3
The distribution of the six most commonly available/used neuromonitoring options is shown in Fig. 3. Invasive ICP and transcranial Doppler were the most frequently available/used monitoring methods utilized in 79 % and 71 % of the centres, respectively. Though multimodal monitoring was available/used in 74 centres (97 %), independent of access to paediatric expertise, centres with access to dedicated paediatric subspecialist expertise within the four domains seemed more likely to use ICP monitoring in managing the entire age-spectrum of mspTBI (Table 3).Fig. 3. The six most frequently reported types of neuromonitoring.Fig. 3. Table 3Use of neuromonitoring in children and infants with mspTBI.Table 3ICP monitoring in children age > 2 years old*Access to neurosurgery**Use of ICP monitoring [%] (number of centres)No use of ICP monitoring [%] (number of centres)*Yes81.2 % (56)18.8 % (13)No57.1 % (4)42.9 % (3)*Access to intensive careUse of ICP monitoring [%] (number of centres)No use of ICP monitoring [%] (number of centres)*Yes79.5 % (58)20.5 % (15)No66.7 % (2)33.3 % (1)*Access to neuro-intensive careUse of ICP monitoring [%] (number of centres)No use of ICP monitoring [%] (number of centres)*Yes87.2 % (34)12.8 % (5)No69.4 % (25)30.6 % (11)*Access to anesthesiologyUse of ICP monitoring [%] (number of centres)No use of ICP monitoring [%] (number of centres)Yes80.6 % (54)19.4 % (13)No66.7 % (6)33.3 % (3)ICP monitoring in infants age < 2 years oldAccess to neurosurgeryUse of ICP monitoring [%] (number of centres)No use of ICP monitoring [%] (number of centres)*Yes62.3 % (43)37.7 % (26)No28.6 % (2)71.4 % (5)*Access to intensive careUse of ICP monitoring [%] (number of centres)No use of ICP monitoring [%] (number of centres)*Yes58.9 % (43)41.1 % (30)No66.7 % (2)33.3 % (1)*Access to neuro-intensive careUse of ICP monitoring [%] (number of centres)No use of ICP monitoring [%] (number of centres)*Yes64.1 % (25)35.9 % (14)No52.8 % (19)47.2 % (17)*Access to anesthesiologyUse of ICP monitoring [%] (number of centres)No use of ICP monitoring [%] (number of centres)Yes59.7 % (40)40.3 % (27)No55.6 % (5)44.4 % (4)Multimodal monitoring (not including ICP) in all pediatric patients age > 0 years oldAccess to neurosurgeryUse of multimodal monitoring [%] (number of centres)No use of multimodal monitoring [%] (number of centres)*Yes98.6 % (68)1.4 % (1)No100.0 % (7)0.0 % (0)*Access to intensive careUse of multimodal monitoring [%] (number of centres)No use of multimodal monitoring [%] (number of centres)*Yes98.6 % (72)1.4 % (1)No100.0 % (3)0.0 % (0)*Access to neuro-intensive careUse of multimodal monitoring [%] (number of centres)No use of multimodal monitoring [%] (number of centres)*Yes100.0 % (39)0.0 % (0)No97.2 % (35)2.8 % (1)*Access to anesthesiologyUse of multimodal monitoring [%] (number of centres)**No use of multimodal monitoring [%] (number of centres)*Yes98.5 % (66)1.5 % (1)No100.0 % (9)0.0 % (0)Correlation between availability of paediatric subspecialty expertise within one of the four domains (neurosurgery, intensive care, neuro-intensive care and anesthesiology) and use of monitoring. P values were non-significant, ranging from 0.090 to 1. ICP = intracranial pressure. Multimodal monitoring includes continuous electroencephalogram (EEG), non-continuous EEG (24/7 available), non-continuous EEG (in office hours), amplitude integrated EEG, near infrared spectroscopy (NIRS), brain tissue oxygenation (PbtO2), microdialysis, transcranial Doppler, pressure reactivity index (PRx) and ‘other’.
Confidence in treating children and infants with mspTBI
3.4
Generally, respondents from centres with access to paediatric subspecialist expertise were more comfortable treating children and infants with mspTBI (Table 4). Availability of a paediatric neurosurgeon was significantly associated with the reported confidence to treat all or most children (p = 0.019) and all or most infants (p = 0.003). For children >1 year of age, availability of a paediatric neuro-intensivist was likewise correlated significantly with the reported confidence to treat most/all children (95 % vs 75 %; p = 0.018). Though similar raw data, the correlation was not significant for treating infants (90 % vs 78 %; p = 0.116).Table 4. Confidence in managing children and infants with moderate/severe TBI.Table 4. Comfortable treating mspTBIFor no casesFor a minority of casesFor about half of casesFor most casesFor all casesNot applicable*Access to paediatric neurosurgery (p=0.019)*Yes0.0 % (0)1.4 % (1)4.3 % (3)23.2 % (16)65.2 % (45)5.8 % (4)No0.0 % (0)14.3 % (1)14.3 % (1)42.9 % (3)14.3 % (1)14.3 % (1)*Access to paediatric intensive care (p=1)*Yes0.0 % (0)2.7 % (2)5.5 % (4)26.0 % (19)60.3 % (44)5.5 % (4)No0.0 % (0)0.0 % (0)0.0 % (0)0.0 % (0)66.7 % (2)33.3 % (1)*Access to paediatric neurointensive care∗ 1 missing data (p=0.018)*Yes0.0 % (0)0.0 % (0)2.6 % (1)17.9 % (7)76.9 % (30)2.6 % (1)No0.0 % (0)5.6 % (2)8.3 % (3)33.3 % (12)41.7 % (15)11.1 % (4)*Access to paediatric anesthesiology (p=0.093)Yes0.0 % (0)1.5 % (1)4.5 % (3)23.9 % (16)64.2 % (43)6.0 % (4)No0.0 % (0)11.1 % (1)11.1 % (1)33.3 % (3)33.3 % (3)11.1 % (1)Comfortable treating infants with msTBIFor no casesFor a minority of casesFor about half of casesFor most casesFor all casesNot applicableAccess to paediatric neurosurgery (p=0.0032)*Yes0.0 % (0)0.0 % (0)4.3 % (3)31.9 % (22)56.5 % (39)7.2 % (5)No14.3 % (1)14.3 % (1)14.3 % (1)28.6 % (2)14.3 % (1)14.3 % (1)*Access to paediatric intensive care (p=1)*Yes1.4 % (1)1.4 % (1)5.5 % (4)31.5 % (23)53.4 % (39)6.8 % (5)No0.0 % (0)0.0 % (0)0.0 % (0)33.3 % (1)33.3 % (1)33.3 % (1)*Access to paediatric neurointensive care∗ 1 missing data (p=0.117)*Yes2.6 % (1)0.0 % (0)2.6 % (1)25.6 % (10)64.1 % (25)5.1 % (2)No0.0 % (0)2.8 % (1)8.3 % (3)38.9 % (14)38.9 % (14)11.1 % (4)*Access to paediatric anesthesiology (p=0.057)*Yes1.5 % (1)0.0 % (0)4.5 % (3)29.9 % (20)56.7 % (38)7.5 % (5)No0.0 % (0)11.1 % (1)11.1 % (1)44.4 % (4)22.2 % (2)11.1 % (1)Graded response in confidence related to availability of dedicated paediatric subspecialty expertise in four domains (neurosurgery, intensive care, neuro-intensive care and anesthesiology).mspTBI = moderate and severe paediatric traumatic brain injury.
For improving confidence in treating mspTBI, respondents mentioned specific management guidelines (43 centres (57 %) for children, 40 centres (53 %) for infants), option of tele-consultation with experienced paediatric neurosurgeons/intensivists (12 centres (16 %) each for children and infants), and a regionally organized stepped referral system (13 centres (17 %) for children and 12 centres (16 %) for infants).
Discussion
4
To the best of our knowledge, this is the first survey mapping the models of management of mspTBI in Europe. Our purpose was to explore the availability of dedicated paediatric expertise in managing mspTBI as well as the adherence to guidelines and clinician confidence in treating mspTBI.
Although the survey does not represent all relevant institutions or all EANS, ESPNIC and ESCIM member countries, the information gathered from this survey points out several interesting facts.
Case load of mspTBI
4.1
Overall, the annual number of mspTBI cases in responding European centres is low, but a few centres reported a much higher incidence. We are unable to assess whether this reflects truly higher numbers in some regions due to different epidemiology of mspTBI, higher grade of centralization, or whether the distinction between mild and moderate TBI is different among centres. Most academic large hospitals represented in this survey treat less than 20 children per year. These results align with the reported decline in mspTBI incidence in high income countries (Guan et al., 2023; Dahl et al., 2021; Maas et al., 2022; Feigin et al., 2021). This brings challenges for keeping up clinical experience in managing mspTBI.
Availability of expertise related to centre size
4.2
Our underlying hypothesis that availability of dedicated paediatric expertise could be related to centres' size and the size of population in their respective catchment area was supported by raw numbers for all four domains (neurosurgery, intensive and neurointensive care and anesthesiology), though a significant association could only be documented for availability of paediatric anesthesiology.
Use of neuromonitoring
4.3
Neuromonitoring is nearly universally available/used, with ICP being the most frequently monitored parameter, followed by transcranial Doppler. However, one quarter of the respondents did not use ICP monitoring, which can reflect the inclusion of cases with mild TBI that would also be an explanation for the large number of annual cases reported by some centres. It may also suggest that ICP monitoring is not utilized in some cases, in spite of the existing guidelines recommending this monitoring modality. Electroencephalogram (EEG) and near infrared spectroscopy (NIRS) were available/used by roughly half of the respondents, which could be explained by most participating centres being academic. Overall, the monitoring tools being available/used match well with current insights in recent publications on mspTBI management (Figaji, 2023; DelSignore and Tasker, 2017). Although statistical significance was not reached, likely due to small subgroup sizes, the data strongly suggests a disparity in the application of critical neuromonitoring tools for the most vulnerable age group in centres without dedicated neurosurgical expertise.
Adherence to guidelines
4.4
Almost all participating centres reported the availability and use of guidelines for the management of mspTBI, however, this was not entirely congruent with the clinician's reported levels of confidence. This discrepancy suggests a gap between the availability and application of guidelines, and their perceived practical usefulness. It is also reflected in the suggested ways to improve confidence**:** more specific management guidelines, tele-consultation with experienced paediatric neurosurgeons/intensivists and stepped referral systems. In addition, awareness of guidelines and their contents does not necessarily equate to structured implementation, which requires dedicated tools and frameworks (Pilar et al., 2020). Consequently, adherence to guidelines in paediatric TBI management remains low, with a recent study from the Netherlands estimating adherence rates between 39 and 65 % (Broers et al., 2018). Expertise and guidance should also extend into the post-acute phase of mspTBI, as almost half of affected children have unmet needs months after their trauma (Dahl et al., 2023).
Confidence in treating children and infants with mspTBI related to paediatric expert availability
4.5
A statistically significant association was observed between access to paediatric neurosurgery and confidence in treating both children and infants with similar trends observed for paediatric neuro-intensivist in treating children and paediatric anesthesiology in treating infants with mspTBI. Although some relationships were inconsistent, the overall data suggests that centres with any form of dedicated paediatric expertise tend to report a higher confidence in managing mspTBI.
While the survey does not directly address whether access to paediatric expertise improves outcome, the reported confidence in managing mspTBI may potentially serve as a surrogate measure for quality of care, or this should at least be investigated. The relationship between availability of relevant paediatric expertise and reported confidence supports this hypothesis. Establishing a causal link however, would require comparison of clinical outcomes related to expertise availability, which was not part of this survey.
Overall, the results of this survey indicate that the quality of care in children and infants with TBI could be improved by increasing access to at least one dedicated paediatric specialty relevant for mspTBI. Additionally, they also underscore the need to improve the practical usefulness of trauma guidelines. The finding that tele-consulting with experienced paediatric neurosurgeons/intensivists and a regionally organized stepped referral system scored rather low as options to improve confidence in treating mspTBI, is likely explained by the large majority of participants being tertiary centres, judging they should be the ones consulted or referred to. In other contexts and pathologies, tele-consulting has proven its worth as a viable and cost-effective strategy.
Limitations
4.6
Although the survey was broadly distributed to all EANS, ESPNIC and ESCIM members, more than 90 % of respondents defined their institution as an “academic hospital”. The survey results thus primarily reflect the organization, expertise availability and management policies at specialized tertiary centres and may not be representative for all hospital types. However, as mspTBI in Europe is rarely treated outside tertiary centres, the high proportion of academic hospitals reasonably reflects current clinical practice, thus limiting the possible selection bias. If not, note that this would even further strengthen the relevance of our findings, as this could mean that use of monitoring, guideline adherence and paediatric subspecialty availability is overestimated. To further contextualize representativeness, we have included general demographic data in Table 1 on total and paediatric population sizes in the participating countries. This allowed us to estimate the survey coverage for each country and better understand how representative the sample was.
The survey contained 34 questions with several of these including multiple answer options. To facilitate analysis, we adopted a stratified approach based on selected indicator questions. We acknowledge that this introduces an element of subjective judgement in determining estimation how best to present and summarize the results. However, we are confident that selection of other indicator questions would not have yielded qualitatively different results. We believe that this method provides a reliable descriptive overview of the current status of mspTBI care in European academic hospitals, further supported by the availability of complete response statistics for all questions in the supplementary material.
There are several different models of practice in the management of paediatric TBI, with significant variations, both between countries and, in some cases, within the same country. It is not clear how these variations affect the quality of care of this patient group. This survey was primarily conducted to chart the availability of dedicated mspTBI expertise and paediatric rehabilitation service across Europe. Accordingly, the organizational data obtained in the survey do not permit conclusions regarding the effect of such expertise on clinical outcomes. However, the findings provide a valuable framework for optimizing confidence and for future studies examining the relationship between patient outcomes and the access to dedicated mspTBI expertise.
Conclusion
5
This first European survey exploring the organizational management of mspTBI reveals low overall caseloads and uneven access to paediatric expertise even across academic centres. Confidence in managing mspTBI appears to correlate with the availability of paediatric subspecialists, suggesting that such expertise may serve as a surrogate indicator of quality of care. While guidelines are widely applied, regardless of expert availability, they alone appear insufficient to ensure clinician confidence in management. These findings underscore the need to strengthen both the specificity and practical applicability of guidelines, as well as to improve access to dedicated paediatric expertise in the management of mspTBI.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Astrand R.Rosenlund C.Unden J.Scandinavian Neurotrauma C Scandinavian guidelines for initial management of minor and moderate head trauma in children BMC Med.142016332688859710.1186/s 12916-016-0574-x PMC 4758024 · doi ↗ · pubmed ↗
- 2Broers M.C.Niermeijer J.F.Kotsopoulos I.A.W.Lingsma H.F.Bruinenberg J.F.M.Catsman-Berrevoets C.E.Evaluation of management and guideline adherence in children with mild traumatic brain injury Brain Inj.3282018102810392977509010.1080/02699052.2018.1469047 · doi ↗ · pubmed ↗
- 3Bruns N.Trocchi P.Felderhoff-Müser U.Dohna-Schwake C.Stang A.Hospitalization and morbidity rates after pediatric traumatic brain injury: a nation-wide population-based analysis Front. Pediatr.9202174774310.3389/fped.2021.747743 PMC 851541534660495 · doi ↗ · pubmed ↗
- 4Bussolin L.Falconi M.Leo M.C.The management of pediatric severe traumatic brain injury: italian Guidelines Minerva Anestesiol.87520215675793343278910.23736/S 0375-9393.20.14122-1 · doi ↗ · pubmed ↗
- 5Chung J.Y.Zeller S.L.Cooper J.B.Socioeconomic disparities in pediatric traumatic brain injury transfer patterns: an analysis of area deprivation index and clinical outcomes World Neurosurg.1882024 e 578e 5823883893510.1016/j.wneu.2024.05.166 · doi ↗ · pubmed ↗
- 6Da Dalt L.Parri N.Amigoni A.Italian guidelines on the assessment and management of pediatric head injury in the emergency department Ital. J. Pediatr.441201872933499610.1186/s 13052-017-0442-0PMC 5769508 · doi ↗ · pubmed ↗
- 7Dahl H.M.Andelic N.Løvstad M.Epidemiology of traumatic brain injury in children 15 years and younger in South-Eastern Norway in 2015-16. Implications for prevention and follow-up needs Eur. J. Paediatr. Neurol.31202170773364753210.1016/j.ejpn.2021.02.002 · doi ↗ · pubmed ↗
- 8Dahl H.M.Holthe I.L.Løvstad M.Tverdal C.Andelic N.Myhre M.C.Almost half of children and adolescents had unmet need 6 months after their traumatic brain injury Acta Paediatr.11252023101910283670807510.1111/apa.16693 · doi ↗ · pubmed ↗