Acceptability and effectiveness of stationary bike intervention on health outcomes among older adults: a systematic review of intervention studies
Taiyeba Akter, Md. Moneruzzaman, Kellina Maduray, Manzur Kader

TL;DR
Stationary biking is a low-risk exercise for older adults that can improve physical and cognitive health, with added benefits when combined with virtual assistance.
Contribution
This systematic review synthesizes the effectiveness and acceptability of stationary bike interventions for older adults, highlighting key health outcomes and the role of virtual assistance.
Findings
Stationary biking showed significant improvements in aerobic capacity, cognition, and mobility in older adults.
Virtual aid-assisted stationary biking improved cycling efficiency and cognitive function more than non-assisted methods.
Acceptability of stationary biking was moderate, with 38% acceptance and 13% dropout rates across studies.
Abstract
Promoting physical activity (PA) among older adults is challenging due to physical limitations and varying levels of motivation. Stationary biking is a safe, non-weight-bearing form of exercise that is well-suited to this population. Although several studies have investigated stationary bike (SB) interventions, there is limited synthesis regarding their focus, effectiveness, and acceptability. This study aims to identify the primary focus areas of published SB interventions and evaluate their acceptability and impact on health outcomes in older adults. Following PRISMA guidelines, a comprehensive search of seven databases was conducted up to June 18th, 2023, without restrictions on publication year. After duplicate records were removed, two independent reviewers screened studies in a two-phase process. Eligible studies included original intervention research reporting both baseline and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
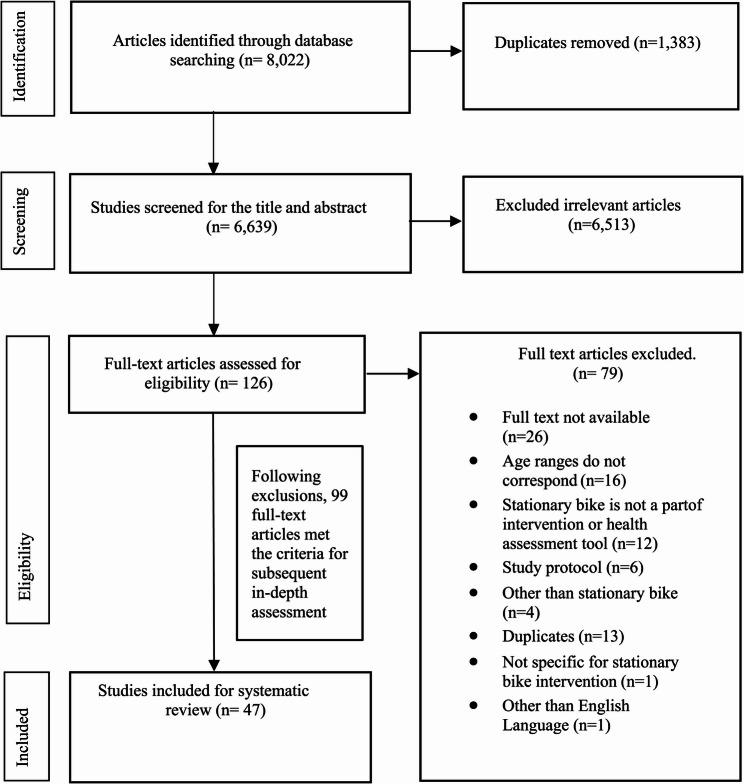 Figure 1
Figure 1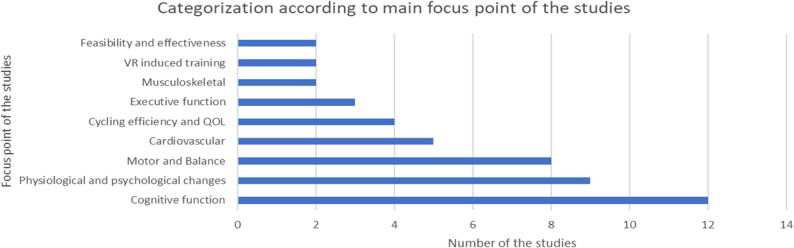 Figure 2
Figure 2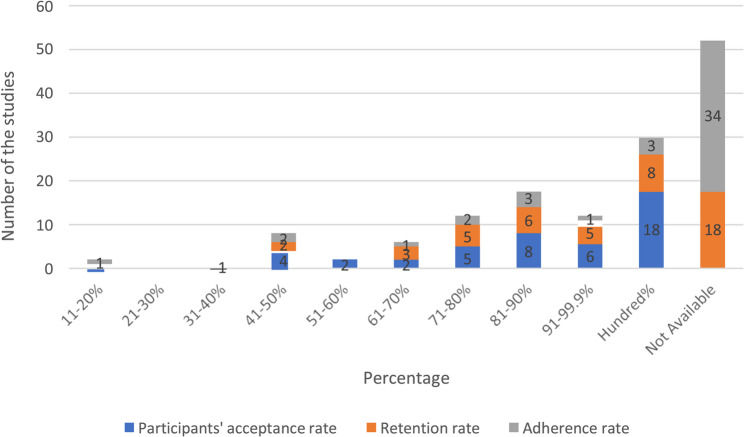 Figure 3
Figure 3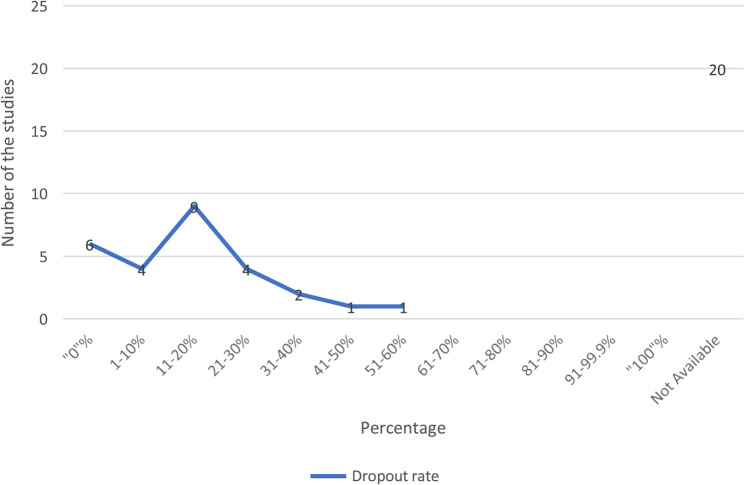 Figure 4
Figure 4- —Dalarna University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhysical Activity and Health · Urban Transport and Accessibility · Balance, Gait, and Falls Prevention
Introduction
Regular physical activity (PA) provides substantial health benefits across all age groups, particularly for older individuals, by promoting prolonged years of active and independent living. The World Health Organization (WHO) projects a significant increase in the global population aged 60 years and above, rising from 12% to 22% between 2015 and 2050, with one in six individuals worldwide expected to be aged 60 years or older by 2030 [1]. Engagement in regular physical exercise and sports throughout life positively impacts cardiovascular, respiratory, metabolic, neurological, and social well-being [2]. Consequently, the WHO recommends that individuals aged 65 years and above engage in at least 150 min of moderate-intensity aerobic physical activity per week, or 75 min of vigorous-intensity aerobic physical activity per week, or an equivalent combination of both. This regimen aims to enhance cardiorespiratory and muscular fitness, bone and functional health, and reduce the risk of non-communicable diseases (NCDs), depression, and cognitive decline [3].
Various forms of endurance exercise training, such as cycle ergometer training [4], walking or jogging [5], and treadmill training [6], have been shown to improve health outcomes. Among these, stationary bike (SB) training stands out due to its ease of use, safety, and low risk of injury [7]. Their key features include adjustable resistance levels for personalized workout intensity, ergonomic seating for comfort, and stability to reduce fall risk [7–9]. SBs are non-weight-bearing, minimizing joint stress compared to jogging or high-impact activities SB exercise is particularly beneficial for its non-weight-bearing nature, which reduces joint impact and overall bodily stress compared to jogging or other high-impact activities [8]. Furthermore, SB training requires less postural control than treadmill walking, making it a suitable option for individuals with balance issues [6]. Additionally, a study by Plante et al. [10] found that VA-assisted stationary biking enhances exercise enjoyment, cognitive function, and reduces perceived exertion in older adults. However, it’s worth noting that VA-assisted biking was not the primary focus in the existing literature and warrants further exploration. Furthermore, systematic reviews specifically addressing the overall acceptability and effectiveness of SB interventions on health outcomes, particularly among older adults aged 60 and above, are currently lacking. Acceptability ensures adherence, as older adults are more likely to continue SB exercises if they are enjoyable and accessible. Factors like ease of use, comfort, and motivation influence participation and long-term benefits. Effectiveness ensures SB exercises improve fitness, strength, and balance while providing accurate performance assessments. Without high acceptability and effectiveness, SB interventions may fail to support active aging. To address this gap, this systematic review aims to comprehensively evaluate the acceptability and effectiveness of SB interventions among older adults. Specifically, the review seeks to: (a) What evidence exists regarding the acceptability of SB among older adults, and (b) What evidence exists for the effectiveness of SB intervention on health outcomes?
In this study, acceptability is defined as participant’s acceptance, dropout, retention, and adherence rates of SB interventions. Older adults are defined as individuals aged 60 years and above [11], with further categorization into younger older adults (aged 60–75 years) and older adults (aged ≥ 76 years) based on previous research [12].
Methodology
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [13], ensuring transparency and rigor in the review process.
Registration
The project was registered with the Open Science Framework (OSF) (Registration https://osf.io/wn3bp), with associated project (link 10.17605/OSF.IO/WN3BP) on April 10, 2025.
Eligibility criteria
The eligibility criteria were established through a two-stage screening process. Initially, screening was performed based on the title and abstract, guided by specific criteria delineating studies centred on bicycles, cycling, or bicycling, particularly those involving older adults or explicitly mentioning an age range of 60 years and above.
Inclusion criteria
For the second stage screening, after obtaining the full texts of potentially eligible studies, the following criteria were applied for inclusion.
- All types of quantitative studies of any duration, assessing the effectiveness of an intervention (randomised or non-randomised),
- Outcomes measured at baseline and post-intervention, with or without follow-up,
- The studies should focus on a subgroup of the aged population aged 60 years and above,
- Addressing stationary biking as a health assessment tool and/or part of an intervention method, and published in the English language.
Exclusion criteria
The exclusion criteria for this review encompassed following parameters.
- Observational studies, including cross-sectional association or correlation studies, were excluded due to their limited ability to establish causality,
- Qualitative studies were excluded as they typically focus on exploring subjective experiences rather than quantifiable outcomes,
- Unpublished or under-review articles, conference abstracts, and publications in languages other than English were excluded to ensure access to peer-reviewed, scientifically rigorous research,
- Furthermore, studies involving forms of bicycling other than stationary bicycling, such as outdoor bicycling or indoor bicycling not part of an intervention, were excluded to maintain consistency in the intervention modality under investigation,
- Study protocols, letters, and commentaries were also excluded from the review due to their preliminary or opinion-based nature. However, relevant references from these excluded sources were screened to identify any articles meeting the inclusion criteria, ensuring a comprehensive examination of the literature.
Information sources
Systematic searches were conducted across seven electronic databases: PubMed, Web of Science, Scopus, Cochrane Library, SportDiscus, CINAHL, and PsychInfo, without applying any filters.
Search strategy
The search strategy was developed in collaboration with an expert library scientist specializing in information retrieval methodologies. We systematically searched for intervention studies using SB as a health assessment tool and/or intervention method among older adults. The search included publications up to June 18, 2023, with no geographical or temporal restrictions and limited to English-language articles. We used a combination of keywords: [“old people” OR “older people” OR “elderly” OR “elders” OR “aging” OR “ageing” OR “old men” OR “old women” OR “older persons” OR “older adults” OR “seniors”] AND [“bicycling” OR “cycling” OR “biking” OR “bike” OR “bicycle”]. Detailed information about the search strategy and keywords is available in Supplementary File S1.
Selection process
All citations were imported into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia; www.covidence.org) and an Excel sheet for the screening process and narrative synthesis. Additionally, citations were imported into EndNote X9 (Clarivate Analytics, Philadelphia, PA, USA) for reference management. A two-stage screening protocol was then implemented, starting with the assessment of each citation’s title and abstract, followed by a thorough evaluation of the full-text articles for potentially relevant studies. Each screening stage was conducted independently by two review authors (TA and MK). After completion, the authors were unblinded to each other’s decisions, and any disagreements were resolved through discussions with additional review team members (MM and KM).
Data collection process
Data from the included studies were extracted and documented through a narrative synthesis by the two independent reviewers (TA and MK). Any discrepancies between the reviewers were discussed and resolved through consensus. Extracted data included the author’s first name, year of publication, country, age range, gender distribution, and study design (RCT or Non-RCT). Further segmentation categorized the type of SB intervention, health conditions of participants, recruitment, dropout, retention, adherence rates, and primary outcomes. However, it is noteworthy that two studies [14, 15] out of 47 could not be tabulated for outcome analysis due to missing “p” values. In such instances, evidence-based theories were judiciously applied for calculation purposes, thereby ensuring methodological rigour and consistency in data analysis. Data were organised in an Excel sheet for systematic synthesis and cross-checking.
Data items
The primary outcome data sought included adherence to the intervention, retention rates, and adverse events. Secondary outcomes included health-related parameters such as cardiovascular fitness, strength, balance, mental health, and quality of life. Data on participant characteristics (age, gender, health status), intervention specifics (type of stationary bike, duration, frequency, and intensity), and study design were collected.
Study quality and risk of bias assessment
In assessing the quality of randomized controlled trials (RCTs) within the scope of this study, two established evaluation tools were utilized: the “PEDro” scale [16] and the Cochrane Handbook for the Risk of Bias Tool, version 2 (ROB 2.0). The “PEDro” scale evaluates studies across eleven criteria, covering aspects such as randomization, blinding, and statistical analysis. Ratings on this scale range from 0 to 10, with scores exceeding 4 indicating fair quality, scores between 6 and 8 denoting good quality, and scores surpassing 8 indicating excellent quality studies [16].
Conversely, non-randomized studies included in this systematic review underwent assessment using the Newcastle-Ottawa Scale (NOS) [17] to gauge their quality and methodological rigor. The NOS evaluates studies based on three primary domains: selection of study groups, comparability of groups, and ascertainment of outcomes. Scores are assigned within these domains to facilitate the critical appraisal of study quality and risk of bias. The quality assessment was performed independently by two authors (MM and KM) Any discrepancies were resolved through discussion with the supervising author (MK).
Effect measures
For each outcome, the effect measures used included adherence rates (percentage of participants completing the intervention), retention rates (percentage of participants remaining in the study until the end), and adverse events (reported incidents during the intervention). Health-related parameters like cardiovascular fitness were measured using heart rate recovery and maximum heart rate (HR) achieved during exercise sessions. Executive function was assessed using standardized cognitive tests specified in each study. Effect sizes (Cohen’s d) were calculated to determine the magnitude of the intervention’s impact where data is available. Applicable, data were extracted on exercise intervention duration, session frequency, and duration to explore their relationship with observed outcomes.
Synthesis methods
Data were synthesized narratively due to the heterogeneity in intervention types and outcomes. Studies were grouped by intervention type, health outcomes, and participant characteristics. Thematic analysis was applied to summarize findings, and results were tabulated for clarity. No meta-analysis was performed due to variability in study designs.
Reporting bias assessment
Due to the narrative synthesis approach, no formal assessment of publication bias was conducted.
Certainty assessment
The overall strength of evidence was assessed considering study quality, consistency of findings, and potential biases.
Results
Study selection
The systematic search yielded 6,639 articles after duplicate removal via Covidence software. Following title and abstract screening, assisted by the software, 126 studies were deemed eligible for full-text review. Subsequent exclusion based on duplicate entries, full-text availability, and relevance reduced this number to 99 articles for manual assessment. Upon full-text evaluation, 47 articles met the criteria for data extraction.
Study characteristics
Table 1 outlines the characteristics of 47 included studies, encompassing a total study population of 2,500 individuals engaged in SB interventions. Among these, 28 (59.57%) studies were RCTs, while 19 (40.43%) were non-RCTs, including Pretest-posttest and Quasi-Experimental studies. A demographic breakdown reveals that 16 (34.04%) studies [10, 18–32] targeted younger older adults aged 60 to 75 years, 5 studies (10.64%) [33–37] focused on older older adults (aged ≥ 76), and 26 (55.32%) [14, 15, 37–60] included both age groups.
Table 1. Characteristics of 47 included studiesCharacteristicsNumber of studies (n),Percentage (%)Study Design Randomized controlled trial28 (59.57) Non-randomized controlled trial19 (40.43)Age range Younger older adults (60–75)16 (34.04) Older older adults (≥ 76)05 (10.64) Both26 (55.32)Gender Male02 (4.26) Female04 (8.51) Both41 (87.23)Health status of the study population Neurological problems15 (31.91) Healthy14 (29.79) Existing Comorbidities (DM, HTN, cancer, and other risk factors)07 (14.89) Physically inactive04 (8.51) Cardiovascular & Respiratory problems04 (8.51) Musculoskeletal problems02 (4.26) Not specified01 (2.13)Types of stationary bikes used for intervention Ergometer28 (59.57) Cybercycle12 (25.53) Recumbent SB05 (10.63) Upright bicycle ergometer01 (2.13) Aqua cycle01 (2.13)Approaches to SB intervention Only SB intervention27 (57.44) SB with virtual aid/electronic device12 (25.53) SB with exercise/cognitive training07 (14.89) SB with medication01 (2.13)DM Diabetes Mellitus, HTN Hypertension, *SB *Stationary Bike
Various types of SB interventions were identified, with ergometers being the most common (61.70%), followed by Cybercycle (SB with virtual aid) in 12 studies (25.53%) [27, 33, 34, 39–43, 49, 52, 54, 59], Recumbent SB in 5 studies (10.63%) [23, 36, 44, 58, 61] and upright bicycle ergometers and aqua cycles (SB in water) each appearing in 2 studies (4.26%) [31, 60] separately. The majority of studies (48.93%) exclusively utilized SB interventions, while 25.53% incorporated SB with virtual aid (VA) intervention, 14.89% combined with exercise/cognitive training, and a single study combined SB intervention with medication (see details in Table 1).
The trend of publications, spanning from 1975 to 2023 with a half-decade interval, is illustrated in Supplementary Fig. 1. It encompasses combined interventions (exercise/cognitive training) and, notably, a single study combining SB intervention with medication (Fig. 1)
Fig. 1PRISMA flow diagram-systematic review: study selection process
Study quality and risk of bias assessment of all RCTs
We evaluated the study quality of all RCTs using the “PEDro” scale [16] and Cochrane Handbook for risk of bias tool “ROB 2.0” [16]. The “PEDro” scale evaluates studies on eleven variables and assigns scores between 0 and 10; a score above 4 indicates fair, while 6 to 8 indicates a study of good quality, and above 8 indicates an excellent quality study.
Regarding the PEDro scale, sixteen studies [18, 22, 23, 28, 30–32, 34–39, 44, 50] scored between 6 and 8, and nine studies [26, 27, 29, 32, 41–43, 57, 60] scored between 4 and 5. Please refer to Supplementary Table 2 for further details.
Regarding RoB 2.0, eleven studies [18, 22, 23, 28, 30–32, 39, 53, 54, 58] are considered as low risk of bias. Two studies [35, 42] had a high risk of bias due to the randomization process and missing outcome data. Other studies [26, 27, 29, 33, 34, 36–38, 41, 43, 44, 50, 56, 57, 60] had overall some concerns because of randomization, selection of reported results, and measurement of the outcome. (see Supplementary Table 3 for further details).
Study quality of all Non-RCTs
Among the remaining 19 non-RCT studies assessed with the Newcastle-Ottawa Scale, nine studies [19, 24, 25, 37, 47–49, 51, 59] achieved the highest scores of 9, indicating strong performance across assessment criteria and robust methodology. Following closely were other studies [9, 20, 21, 52] with a score of 8, highlighting commendable methodological quality. Four studies [14, 40, 46, 55] received a score of 7, indicating a good level of quality in design and execution. One study [45] scored 5, reflecting a lower level of methodological quality, while another study [15] scored 3 due to design limitations and lack of methodological details (see Supplementary Table-4 for further details).
Results of individual studies
Figure 2 illustrates the primary areas of investigation in the 47 included studies. Cognitive function emerged as the most frequent focus, with 12 studies [24, 27, 33, 34, 39, 40, 42, 43, 47, 54, 59, 61]. Other prominent categories include Motor and Balance (seven studies) [10, 22, 32, 38, 44, 48, 51], Physiological and psychological changes (nine studies) [15, 18, 20, 30, 45, 50, 53, 56, 58], Cardiovascular (five studies) [19, 25, 28, 29, 60], Executive function (three studies) [23, 26, 36], Cycling efficiency and Quality of life (four studies each) [14, 21, 46, 52], VA-induced training, and Feasibility and effectiveness (four studies each) [15, 35, 41, 49]. Additionally, studies related to the Musculoskeletal system were represented by two studies [31, 55].
Fig. 2. Categorization according to focus points of the studies. *QOL *Quality of Life, *VR *Virtual reality
Evidence related to the acceptability of SB intervention: Among the 47 included studies, 18 studies [18, 20, 21, 24, 25, 27, 29, 30, 36, 41, 42, 44, 46, 50–52, 56] reported a 100% acceptance rate, 7 studies [27, 32, 43, 49, 53, 54, 57] had a 100% retention rate, and 3 studies [32, 39, 54] reported full adherence. Additionally, 6 studies [32, 43, 49, 53, 54, 57] recorded a 0% dropout rate (see Table 2; Figs. 3 and 4). The second highest acceptability range (81–90%) was observed in 17 studies, with acceptance reported in 8 [19, 23, 38, 40, 47–49, 60], retention in 6 [19, 21, 23, 34–36], and adherence in 3 [15, 23, 49]. In the 91–99.9.9% range, 12 studies showed acceptance in 6 [22, 32–34, 36, 61], retention in 5 [20, 28, 31, 56, 60], and adherence in 1 [37]. The 71–80% range was observed in 12 studies, with acceptance in 5 [37, 39, 43, 55, 59], retention in 5 [15, 22, 39, 40, 55], and adherence in 2 [39, 56] (see Table 2).
Fig. 3. Acceptance, retention, and adherence rate of stationary bikes among the study population
Fig. 4. Dropout rate of stationary bikes among study population
Lower adherence rates were found in 8 studies (41–50%) with acceptance in 4 [10, 26, 28, 35], retention in 2 [36, 42], and adherence in 2 [42, 45]. The lowest range (61–70%) was found in 6 studies, with acceptance in 2 [31, 58], retention in 3 [33, 37, 48], and adherence in 1 [55] (see Table 2).
Dropout rates ranged from 0% to 60%, with 9 studies [19, 21–23, 34, 35, 47, 55, 61] reporting an acceptable 11-20% dropout rate (see Fig. 4). A total of 19 studies [19–23, 28, 31, 32, 34, 35, 43, 47, 49, 53–55, 57, 60, 61] had dropout rates below 20%, while 8 studies [15, 33, 36, 37, 39, 40, 42] exceeded 20% (see Table-2). Three studies [23, 32, 49] demonstrated feasibility with ≥80% acceptance, retention, and adherence, and <20% dropout.
Overall, acceptability rates were 38% for acceptance (18/47 studies), 15% for retention (7/47), 6% for adherence (3/47), and 13% for dropout (6/47).
The effectiveness of SB interventions across health outcomes
The effectiveness of SB interventions varied across health outcomes. Table 2(see also supplementary Table-1) represents an overview of findings from all 47 included studies. As most studies implemented SB in combination with VA, outcomes are reported by intervention modality (SB + VA vs. SB alone) to enable clearer interpretation of their relative effects.
Table 2. Extracted data from 47 included studiesIncluded ArticlesAcceptability of stationary bike interventionDescription of effectiveness-First Author (Year of publication)- (Study design)Offer made to the eligible Participants (n)Number of people randomised.(n) *(for RCT/Quasi ex.)*OrNumber of eligible participants accepted the offer(n) *(other than RCT/Quasi ex.)*Participant’s acceptance rate: RCT/Quasi ex.: [Number of people randomised (n)/offer made to the eligible (n)] x 100 (%)
Other than RCT/Quasi ex.: [Offer accepted by the eligible (n)
/Offer made to the eligible (n)] x 100 (%) (Arring et al.,* 2022*Participants left the intervention (n)Drop-out rate: For RCT/Quasi ex.: [Participants Left the intervention (n)
/no. of participants started stationary bike intervention (n)] x 100 (%)
Other than RCT/Quasi ex.: [Participants left the intervention (n)/Offer accepted by the eligible (n)]x
100(%) (Gupta et al.,* 2016)*Retention rate: RCT/Quasi ex.: No. of completers(n)/p articipants started stationary bike intervention (n)] x100(%)
Other than RCT/Quasi ex.: [No. of completers (n)/offer accepted by the eligible (n)] x 100 (%) (Yu et al.,* 2013)Adherence rate to the prescribed stationary bike exercise (%)Health status of the study population during enrolment processDisease/condition for the interventionWhat found? or↑/↓/no improvement after stationary bike interventionTypes of Stationary bikes with added features for intervention purposesAbbas (2022)[38](RCT)6860(Started SB intervention: 20*,* Completers N/A)88%N/AN/AN/AN/AModerate to severe dementiaBalance and mobilitySignificant increase of balance and reduction of mobility among ergometer, and “ergometer & HIFE group” when compared with “pre- treatment” group.Virtual aid assisted cycle ergometerAnderson- Hanley, C. (2012)[40](RCT)10279(Started SB intervention:38*, Copmleters:30) 77%8(Non-compliant to bike:3, others:5) 21%79%80%HealthyExecutive functionBetter executive function among SB group than traditional SB exercisers.Recumbent stationary bike withvirtual aidAnderson- Hanley (2011)[39](Non-RCT),Quasi experimental)2320*[Started SB intervention:13*,* Completers:10 (T2DM)]87%3(Moved out: 1*,* medical complications:2* ) 23%77%100% (All followed the 3 months of monitored
exercise)) Type-2 Diabetes MellitusExecutive functionT2DM patient exhibited significant gain on Colour trails test to detect executive function than non-DM patient.Cyber cycle vs. ergometerAnderson- Hanley (2018)[42](RCT)111111*(Started SB intervention:46*,* Completers:23)100%23(Knee pain*,* motion sickness*,* Illness/injury: 15*,* too difficult**to perform: 4*,* medical complications:4* ) 50%50%50%Impaired cognition (Mild to moderate)Executive functionExer-tour group (exercise bike with virtual tour) yielded significant improvement on executive function compared to exer- score (pedal-based videogame) group.Recumbent stationary bike with virtual aidAnderson- Hanley (2012)[41](RCT)1414100%N/AN/AN/AN/AHealthyVirtual reality induced competitiveness on exercise effortVirtual social facilitation increased exercise effort among competitiveexercisers.Cyber-cycleAntunes (2015)[18](RCT)4646 (Started SB intervention: 23) 100%N/AN/AN/AN/AHealthyMemory and Physiological functionSignificant improvement in memory, decreased blood viscosity, and higher aerobic capacity in ergometer group compared to control (no intervention)group.Ergometer (Stationary Bike)Barcelos (2015)[43](RCT)644875%00%100%42%HealthyExecutive functionExergaming group performed better interactive mentalchallenge than others.Stationary bicycle with virtual aidBellumori (2017)[44](RCT)2626 (Started SB intervention:14) 100%N/AN/AN/AN/AHealthyMobilityRelatively low dose speed based stationary bike group improved neuromuscular function and tests of mobility compared to control (dailyactivities) group.Recumbent stationary bicycleBrisswalter (2014)[46](Non-RCT), Non-randomised comparative study2020 (≥ 60 yrs.) 100%N/AN/AN/AN/AHealthy TriathleteCycling efficiencyCycling efficiency continued to decrease beyond 60(60–69) years whencompared with 50–59 years group.ErgometerBuccola [45](1975)(Non-RCT), Non-randomised comparative study362056%N/AN/AN/AN/ANot specifiedPhysiological and personality changesIncreased VO2max, reduced BP and weight, and cyclers did not change any personality factors over walk-joggersgroup.ErgometerCallow (2022)[47](Non-RCT), Pretest-posttest)353086%5*(Poor performance:4*,* Failed to* respond: 1) 17%N/AN/AHealthyMemoryBetter mnemonic discrimination performance following ergo cycle exercisegroup.Cycle ergometerCicek (2020)[48](Non-RCT)6758*(Started SB intervention:21*,* Completers: 14*)87%7 (Discontinued :6 others:1)33%67%N/AExisting comorbiditi esMobility and balanceErgometer & treadmill-based program found less effective than video-based program on mobility but foundeffective on balance test.Ergometer and treadmillColombo (2023)[49](Non-RCT), Pretest-posttest141286%00%100%86%Chronic Obstructive Pulmonary Disease (COPD)Acceptability and user experience ofVA based endurance training program.Exercise capacity (walking test) significantlyimproved after VA based exercise intervention.Cycle ergometer with virtualAidCunha (2021) [19](Non-RCT),Non-randomised comparative study8471(Started SB intervention: 17, Completers 15) 85%02 (Due to time commitment) 12%88%N/AHypertensiv e with a stable BP for last 3 monthsEffect of BP after exercise interventionAfter 30 mints of exercise only water- based exercise (swimming) lowered SBP when compared with ergo-cycle group.Cycle ergometerD’Cunha (2021)[33](RCT), Randomised crossover111091%3 (Due to lower
body discomfort) 30%70%N/AImpaired cognition (Mild to moderate)Cycling efficiencyLower response in the SB intervention than the control conditionStationary bike with virtual aidEmery (1994)[20](Non-RCT)6464100%3(not mentioned clearly)5%95%N/AChronic obstructive pulmonarydisease (COPD)Physiological and psychologicalImproved psychological and physiological function.Ergometer (Stationary bike)Ferrai (2004) [21](Non-RCT), Pretest-posttest3232100%4 (Refused to continue-2) 13%88%N/ACOPDCycling efficiency and QOLExercise tolerance and QOL improved (No variation observed in pulmonary functiontest).Ergometer with a mechanical brakeFerraz (2018)[22](RCT)7672*(Started SB intervention:25*)95%5*(Non- adherent:2*,* medical complications:3* ) 20%80%N/ADiagnosed PDWalking capacity among PD patientImproved walking capacity among ergometer, functional training and exer-gaming group.Ergometer (Stationary bike)Gaesser (2018)[14](Non-RCT), Non-randomised comparative study82*(≥ 60 yrs.*)82100%N/AN/AN/AN/AHealthyCycling efficiencyCycling efficiency was not differentwhen compared with younger group.ErgometerGitlin (1992)[50](RCT)267267 (Both intervention and control group
receive ergometer intervention but in different duration,* total completed* intervention: 254) 100%13*(Lack of interest-9*,* and* medical complication-4) N/AN/AN/AHealthyPhysiological and psychologicalBetter QOL found after ergometer exercise intervention.ErgometerHill (2015)[51](Non-RCT), Non-randomised comparative study0909100%N/AN/AN/AN/APhysical inactivityWalking on postural swayPost ergometer exercise balanceimpairments lasted for 10 min.ErgometerHou (2023)[23](RCT)154128*(Started SB intervention 44*,* Completers:38)83%06(Health problems:3, Other reasons:3)14%86%86%HypertensiveMemorysignificant improvements in working memory when comparedwith control group (without exercise)Recumbent stationary bikeJoyce (2014)[24](Non-RCT),Non-randomised comparative study12(≥ 61 yrs.)12100%N/AN/AN/AN/AHealthyCognitionOlder adults adopted more cautious.strategies compared to younger adults (23 ± 2 yrs.)ErgometerKatyal (2003)[25](Non-RCT), Non-randomised comparative study24(≥ 60 yrs.)24100%N/AN/AN/AN/APhysical inactivityCirculatory function among post- menopausalwomenAge and hormone replacement did not affect circulatory function after bikeintervention.ErgometerKwan (2021)[34] (RCT)1817(Started SB intervention: 9*,Completers: 8)94%01(repetitive VA sickness)11%89%n/aImpaired cognitionCognitive functionVA stimulating motor-cognitive training effectively enhances the cognitive function compared to control (non-VA motortraining) group.Cycle ergometerLebeau(2020)[26](RCT)713549%n/an/an/an/aHealthyExecutive functionParticipants performed better on the Trail Making Test and Stroop test after the fitness test compared to theirbaseline.Cycle ergometerLee (2014)[10](Non-RCT), Non-randomised comparative study2412 (SB intervention offered for 12
only) 50%N/AN/AN/AN/AHealthyEffect of gait and balanceStationary bike group improved balance than treadmill group.Ergometer(Stationary bike)Loggia (2021)[52](Non-RCT), Non-randomised comparative study1212100%N/AN/AN/AN/AImpaired cognition(Mild to moderate)Virtual reality upon cycling tendencyMost participants would rather repeat cycling sessions with VA thanwithout VA.Ergometer with or without VALopez-Garcia (2019)[27](RCT)4949100%N/AN/A100%N/A (High adherence but did not mention
percentage) HealthyCognitionErgometer with video game intervention acutely improved choice reaction time.Ergometer with or without video gameMadden [28](2009)(RCT)3618(Completers:17)50%1(Other reasons)6%94%N/AExisting comorbidityArterial stiffness among non-communic able diseases (NCDs)patientsA relatively short aerobic exercise interventionin older adults can reduce arterial stiffness amongNCDs patient.Ergometer with treadmillMahajan (2021)[53](RCT)3413 (Started SB intervention: 6) 38%00%100%N/ASleep impairedTo check the feasibility of the interventionErgo cycle training is feasible for older adults to support a full scale RCT for sleep intervention evident by > 80% asretention rate.ErgometerMiki (2014)[54](RCT)14678 (Started SB intervention: 38) 53%00%100%100%(All participants completed all the sessions with fun)Breast or prostate cancerSpeed feedback therapy on CognitionSpeed-feedback therapy with ergometer group had higher mean FAB score than the control group and suggested an effective intervention forcognition.Ergometer with visual speed back therapyMorita (2013)[29](RCT)131131100%N/AN/AN/AN/AExisting comorbidityCardiovascula r effect on BP, and BMI.Decreased BP and BMI but more in women than man.ErgometerNocera (2020) [30](RCT)3737(Started SB intervention: 25)100%N/AN/AN/AN/APhysical inactivityPhysiological and psychologicalAerobic exercise group improved cardiac fitness and mobility afterintervention.ErgometerPauwels (2018)[55](Non-RCT), Pretest-posttest201575%3(Balance problem:2, ergo-cycle was bigger:1) 20%80%67%Lumber stenosed participantsHome based cycling on lumber stenosisSelf-reported clinical improvement, with reduced radicular pain anddisability.ErgometerPosner (1992) [56](RCT)247247*(Started SB intervention: 166*)100%N/AN/A93%75% (Completed prescribed exercise) Physical inactivityPhysiological response on endurance trainingImproved physiological function (VO2max) among exercise group and decreasedin control group.ErgometerRezasoltani (2020)[31](RCT)4732*[Started SB intervention (aqua bike): 15]68%1(Declined to continue: 1)7%93%N/AKnee osteoarthriti sEffect on Pain for knee OA participants after aqua cyclingAqua-cycling group experienced significant pain reduction (p < 0.001) compared to control (pain relievingmedicine) group.Aqua cycleRidgel (2019)[57](RCT)5816(Started stationary bike intervention:08, Completers:08)18%00%100%N/ADiagnosed Parkinson’s diseaseHigh cadence on motor function of PDpatient.Improved mobility and motor function after high cadence ergo cycling compared to control (stretching)group.Virtual aid assisted ergometer (stationary bike)Salisbury (2022)[58](RCT)674770%N/AN/AN/AN/ADiagnosed Alzheimer disease with dementiaPhysiological Changessignificantly increased peak oxygen (VO2Peak) by 1.28 compared to the control (stretching) group.Recumbent Stationary bikeSchwarck (2021)[59](Non-RCT),Pretest-posttest191474%N/AN/AN/AN/ADiagnosed Alzheimer disease patients with dementiaCognitionReaction time in the picture recognition task significantly decreased.ErgometerTollár (2019)[32](RCT)8883 (Started SB intervention: 27) 97%00%100%100%Participants with mobility difficultiesEffects of exercise on motor and balance, and QOLActivities of daily living, berg balance Score and gait index improved more in exergaming group than ergometergroup.Ergometer (Stationary bike)VanRoie (2017)[35](RCT)19895(Started SB intervention of strict coach together with minimal contact coach: 71*, Completers: 61) 48%10*(Medical complications: 6*,* Loss of**interest: 2*, others: 2) 13% (Directly stated) 86%20%HealthyFeasibility and long-term effectiveness of Ergo- cyclingErgometer intervention ↑QOL among intervention group irrespective of types of supervision (Strict, minimal, and no supervision/controlledcognition)ErgometerWillenheimer (1998)[60](RCT)6150 (Started SB intervention: 23) 82%1 (Developed rheumatoid arthritis) 4%96%N/ADiagnosed Alzheimer diseaseEffect of exercise training on heart failureSupervised exercise training was safe and beneficial in heart failure patients specially men aged≤ 75years with ischemic aetiology.Upright bi- cycle ergometerWu (2023)[36](RCT)5252*(Started SB intervention: 26*, Completers: 11) 100%15(Refused to exercise11, fall:1, medical complications:3).58%42%N/AModerate dementiaCognitive FunctionSignificantly shorter reaction time in exergame post intervention compared to recumbent bikeexercise group.Recumbent bikeYu (2011) [37](Non-RCT), Pretest-post test11873%3(Exerciserelated anxiety- 1)37.5%62.5%97.9% (Average taken) ADCycling intervention on physicalfitnessSignificant reduction of heart rate.ErgometerYu(2021)[61](RCT)10396*(Started SB intervention:64*,* Completers: 53)93%11(Withdrew:5, medical complications:2*,*other reasons:2))*17%83%N/AADCognitive effect on AD patientAerobic exercise failed to show any superior cognitive effect over stretching.ErgometerYu (2013)[15](Non-RCT), Pretest-posttest2928 (Completers: 22) 97%06 (Other reasons) 21%79%86.4%ADRecruitment, retention, and adherence to 6-month cyclingamong AD.Recruitment relies on community partnership and exercise safety improves retentionand adherence.Ergometer (Stationary bicycle)N = 47 studies; RCT Randomized controlled trial, Non-RCT Non randomized controlled trial, HIFE High intensity functional exercise, VA Virtual aid, FAB Frontal Assessment Battery, SBP Systolic blood pressure, DBP Diastolic blood pressure, BP Blood pressure, BMI Body mass index, N/A Not available, SB Stationary bike, T2DM
Effects on aerobic capacity (VO2 max)
The most commonly assessed outcome, VO₂ max, was examined in 10 studies. Of these, 4 showed significant (p ≤ 0.05) [18, 25, 45, 58] and 4 showed highly significant improvements (p ≤ 0.001) [20, 21, 30, 56] after SB intervention. Among RCTs with comparable groups, improvements were reported in 4 studies ([18, 58]: p ≤ 0.05; [30, 56]: p ≤ 0.001), while 2 RCTs found no significant changes [28, 60] (see supplementary Table-1). None of these RCT studies used combined (SB + VA) SB intervention.
Effects on cycling efficiency
The second most outcome, cycling efficiency was assessed in 8 studies (see supplementary Table-1 and Table-2). Among them five studies investigated cycling efficiency in older adults (≥ 60 years) by comparing VA enhanced stationary cycling with traditional non-VA cycling [27, 33, 38, 41, 57]. All five studies demonstrated significantly greater improvements in the VA groups (p = 0.002–0.049), with inferred effect sizes ranging from small-moderate to moderate-large (see Appendix 1). Notably, one study reported gains in both groups, though the effect was larger in the VA condition [57]. Additionally, one study implemented VA-assisted SB without any non-VA comparator and reported statistically significant improvements in cycling efficiency through repeated participation (p < 0.05) [52]. In contrast, two studies also conducted SB interventions without VA; one reported increased cycling efficiency (p < 0.05) [53], whereas the other observed a significant decline (p < 0.05) [46] (see Suppl. Table-1).
Effects on cognition
Cognition was assessed in seven studies, including five RCTs [27, 34, 36, 54, 61]. Most RCTs reported small to large significant improvements (p ≤ 0.05 to p ≤ 0.001) in cognitive performance, particularly in choice reaction (CR) time, compared with control groups. Notably, two of these RCTs incorporated combined SB and VA interventions [27, 54]. Among the five RCTs, two reported decreased CR time [2, 24], while one found no cognitive benefit over stretching in Alzheimer’s disease patients [61]. Additionally, two non-RCT studies also reported improved cognition (p < 0.001) [24], although one did not report a p-value [2] (see Suppl. Table-1).
Effects on executive function
Executive function was assessed in six studies, including five RCTs [26, 40, 42, 43, 61]. Three of these employed combined interventions (SB + VA) and reported small to moderate improvements compared with non-VA groups (p < 0.05 to p < 0.001) [40, 42, 43]. Improvements on the “Colour Trails” test were observed in three studies (p = 0.002, d = 0.5; 0.007; 0.02) [39, 40, 43], while the “Stroop A/C” test showed significant to highly significant gains (p < 0.05 to p < 0.001) in two studies [26, 42]. In contrast, one study reported no group difference [43], and another found no effect of ergometer training on executive function in Alzheimer’s disease patients [61] (see Suppl. Table-1).
Effects on quality of life (QOL)
Five studies assessed QOL among them four studies are RCT and none of them used combined SB intervention [32, 35, 50, 60]. Two COPD studies reported highly significant improvements (p ≤ 0.001) following ergometer intervention [35, 50], and another study found a significant QOL improvement (7/9 score) in COPD patients post-ergometer intervention [21]. Alzheimer’s disease participants also showed statistically significant QOL gains (p < 0.05) [60], while one study found greater improvements with SB interventions compared to non-stationary cycling [32] (see Suppl. Table-1).
Effects on Mobility, gait and balance
The Timed Up and Go (TUG) test was assessed in 5 studies. Three of them are RCT and reported significant (p < 0.05) mobility improvements in healthy, physically inactive, and Parkinson’s disease (PD) participants compared to control group [30, 44, 57], while one of them used combined SB intervention [57]. However, two studies found no mobility benefits [38, 48]; among them one study found no improvement when compared with non-VA SB intervention group [38]. Walking capacity improved significantly in COPD and PD patients [22, 49] but not in individuals with mobility difficulties when compared with control group [32].
Gait outcomes improved significantly in one study (p < 0.01) when compared with control group with combined SB intention [57], while no improvement was seen in another study on physically inactive participants [51]. The Berg Balance Scale (BBS) showed improved balance (p < 0.05) in 3 studies [10, 38, 48] and among them one study found better improvement when compared with non-VA SB group [38]. However, one study found no improvements among mobility-impaired individuals when compared with control group [32] (see Suppl. Table-1).
Effects on memory
Memory improved significantly (p < 0.05; p = 0.012, η² = 0.07) in both healthy [18, 47], and hypertensive participants (compared with control group) [23], but no improvement observe with those with AD when compared with control group [61] (see Table 2 and see Suppl. Table-1).
Miscellaneous findings
Blood pressure decreased significantly (p < 0.05) in two studies [29, 45], however, another study found unchanged [19]. Significant (p < 0.05) reduction of back pain mentioned in two studies [31, 55] and lowering of heart rate in another study [37]. On contrast, another study failed to show any improvement when compared with control group among AD participants [60] (see Suppl. Table-1).
Outcomes of RCT studies: Out of 28 RCT studies (see Suppl. Table-1), positive outcomes were noted, notably improved aerobic capacity (VO_2_ max) in 4 studies (p = < 0.05) [6, 7, 18, 31]. The “Colour Trails” test improved in 2 studies (p = < 0.05) [39, 43], and the “Stroop a/c” test in another 2 studies (p = < 0.05) found improved as part of executive function respectively [10, 42]. Mobility (TUG test) showed improvement in 3 studies (p = < 0.05) [6, 44, 58]. QOL also significantly improved in 3 different studies (p = < 0.05) respectively [3, 62, 63]. Improved overall cognitive function was found in 2 different studies (p = < 0.05) without specifying the outcome of Choice Reaction (CR) time [26, 54]. Memory improved in 2 different studies (p = < 0.05) [18, 24]. Cycling efficiency with and without virtual aid (VA) increased in 2 different studies distinctly (p = < 0.05) [16, 41]. However, Balance (BBS test), Walking capacity, Gait, Pain reduction, & Lowering of BP showed the least significant improvement, each presented in a single study separately ((p = < 0.05) [14, 30, 38, 57, 58].
Upon analysing all the RCTs, several outcomes failed to show any improvements. Notably, Cognitive function was stated in 3 studies, among them 2 showed increased Choice Reaction time indicating decreased cognitive function (p = < 0.05) [11, 64], and another study showed an overall decrease in Cognitive function (p = < 0.05) [61]. The Stroop test and overall executive function as part of Executive function, and Aerobic Capacity both failed to show any improvement in 2 different studies individually (p < 0.05) [28, 43, 60, 61]. Additionally, Cycling with VA and Mobility (TUG) failed to show any improvement as stated in 2 different studies (p = < 0.05) [33, 38]. However, QOL, Balance, and Walking Capacity each of the outcomes failed to show any improvement as stated in a single study (p = < 0.05) [65].
VA-enhanced SB interventions in older adults among RCTs
Table 3 summarizes RCTs in adults aged ≥ 60 years, demonstrating that SB with VA interventions consistently yielded superior outcomes compared to non-VA conditions. VA protocols improved walking distance and perceived exertion (p < 0.05, small-moderate) [27], engagement and exertion in dementia (p = 0.012, small; p < 0.05, small-moderate) [33, 38], executive function in diabetes (p < 0.05, small-moderate) [40], at-risk/mild cognitive impairment (MCI) cohort (p = 0.049, small-moderate) [42], competitiveness in community-dwelling adults (p = 0.003, moderate) [41], and engagement in healthy older adults (p < 0.05, small-moderate) [43]. Additional benefits included adherence and cognitive function in cancer (p < 0.05, small-moderate) [54] and enhanced cycling efficiency in Parkinson’s disease (VA: p = 0.002, moderate; non-VA: p = 0.012, small) [57]. Overall, effects consistently favoured VA interventions.Table 3. Effectiveness of SB with VA vs Non-VA intervention outcome among older adults (≥60 years) in RCTsFirst Author (Year)Sample (≥ 60 yrs) VA Non-VAReported p-valueInferred Effect Size Category*Direction of EffectLópez-García (2019) [27]Healthy older adults Longer distance, higher perceived effort, and ↑cognitionShorter distance & lower perceived effortp < 0.05Small-moderateFavours VAD’Cunha (2021) [33]Older adults with dementia↑ Perceived exertion, better engagementNo improvementp = 0.012SmallFavours VAAbbas (2022) [38]Dementia cohortSignificant ↑ in cycling efficiencyNo improvement p < 0.05Small-moderateFavours VAAnderson-Hanley (2012)[40]Older adults with diabetes↑ Effort and executive functionNo improvementp < 0.05Small-moderateFavours VAAnderson-Hanley (2011)[41]Community-dwelling older adults↑ Exercise effort & competitivenessMinimal change(p value not reported)p = 0.003ModerateFavours VAAnderson-Hanley (2018)[42]At-risk/MCI cohortSignificant ↑ inexecutive function No improvementp = 0.049Small-moderateFavours VABarcelos (2015) [43]Healthy Older adults↑Engagement and executive functionNo improvementp = 0.02Small-moderateFavours VAMiki (2014) [54]Older adults with cancer↑ Adherence and cognitive functionStable performancep < 0.05Small-moderateFavours VARidgel (2019)[57]Older adults with PDSignificant ↑ in cycling efficiencySignificantly ↑ but smaller than VAVA: p = 0.002; non-VA: p = 0.012Small (both improved, VA stronger)Favours VAEffect size categories inferred as follows: p ≤ 0.001 = large, 0.001 < p ≤ 0.05 = small-moderate, non-significant =trivial/no effect; Standard deviations, and sample sizes unable to report as standardized mean differences(e.g., Hedges’ g) could not be calculated directly [66] *VA *Virtual aid, MCI Mild cognitive impairment, RCT Randomized Controlled Trial
Across studies, VA-supported stationary bike interventions were delivered by exercise professionals, researchers, or therapists, with protocols typically involving interactive or videogame-based cycling, cognitive tasks, or prescribed cadence [27, 33, 38, 40–43, 54, 57]. Sessions were most commonly prescribed 2–3 times per week, lasting 30–45 min, over 4–6 weeks or up to 3 months. Interventions were tailored through adjustments to speed, cadence, or HR targets (typically 60–70% HRmax), as well as cognitive challenge scaling (see Appendix:1 TIDieR framework,* more detail in PRISMA checklist Appendix:2*).
Results of syntheses
No meta-analysis was performed due to substantial heterogeneity across the included studies. Possible sources of heterogeneity included differences in study populations (e.g., healthy vs. individuals with chronic diseases), variations in SB intervention types (e.g., ergometers vs. VA-assisted SB), and differing outcome measures and assessment tools. The risk of bias varied, with RCTs generally having a lower risk of bias compared to non-RCTs.
Key Findings Across Syntheses:
- SB interventions demonstrated significant improvements in cognitive function, mobility, and cardiovascular fitness, particularly in physically inactive and cognitively impaired individuals.
- VA-assisted SB interventions showed greater benefits for executive function and cycling efficiency compared to traditional SB.
- Aerobic capacity and mobility improvements were more pronounced in healthy individuals compared to those with pre-existing conditions.
Sensitivity analyses were not conducted due to the narrative synthesis approach. However, subgroup analyses suggest that SB interventions, particularly those incorporating VA, provide significant health benefits for older adults, while physically inactive individuals experienced smaller effects on mobility and aerobic capacity.
Certainty of evidence
The certainty of evidence was assessed considering study quality, risk of bias, and consistency of results.
- RCTs: Generally had lower risk of bias; 16 studies had “good” quality (PEDro score 6–8), while 9 studies scored “fair” (PEDro > 4).
- Non-RCTs: 9 studies had the highest methodological quality (Newcastle-Ottawa Scale score 9), while 5 studies scored between 7 and 8.
- Limitations: Variability in intervention protocols, sample populations, and outcome measures contributed to moderate certainty in the evidence.
Discussion
This systematic review represents the first comprehensive analysis focusing on the acceptability and effectiveness of SB intervention concerning health outcomes among individuals aged 60 and above. Encompassing 47 intervention studies, including 28 RCTs and 19 non-RCT studies, the review revealed an overall acceptability rate of 38%, retention rate of 15%, adherence rate of 6%, and dropout rate of 13%. Collectively, these studies highlight the wide-ranging positive impacts of SB intervention across multiple domains, including cognitive function, motor skills and balance, physiological and psychological well-being, cardiovascular health, executive function, cycling efficiency, quality of life, musculoskeletal health, as well as feasibility and long-term effectiveness.
According to the current evidence, SB is proposed as a suitable form of endurance training for promoting overall physical health among older adults over 60, primarily due to its relative ease of performance and safety, with no associated injuries reported [7]. Furthermore, the use of a bicycle ergometer in SB presents advantages over treadmill walking, particularly for older frail individuals, as it requires less upper body motion, facilitating the recording of vital signs and blood sample collection [67].
Evidence from SB interventions with VA indicates benefits for both cognition and physical performance. Studies reported significant improvements in executive function (d = 0.5) [39], memory *(*η² = 0.07) [47], walking capacity [49], and cycling efficiency with repeated participation [52]. While these findings highlight the potential of VA-supported cycling, the evidence remains mixed in methodological quality, with several studies relying on non-randomized or pre-post designs, reinforcing the need for further high-quality RCTs to confirm these effects.
Across RCTs, VA-enhanced interventions consistently outperformed non-VA conditions in older adults, improving cycling efficiency, cognition, and executive function. Prior studies confirm that interactive technologies enhance motivation and adherence in aging populations [41, 43]. Benefits were observed in healthy adults, as well as in dementia, diabetes, cancer, and Parkinson’s disease cohorts [33, 38, 40, 42, 54, 57]. Although effect sizes were small to moderate, the consistent direction of benefit underscores.
Additionally, based on RCT evidence it is also found that maximum studies recommended 30 min of SB with VA intervention at ~ 60% HRmax, for 2**–3 times per week for at least 4–**6 weeks to achieve significant health benefits (see Appendix: 1). Therefore, SB with VA interventions is a promising tool for promoting physical and cognitive health in late life and require more research.
Comparison with other studies
Although numerous systematic reviews have explored the benefits of SB for the general population, there is a scarcity of studies focusing specifically on older adults aged 60 and above. Compared with earlier reviews, our study offers a more comprehensive synthesis of stationary bike interventions among older adults (≥ 60 years). Prior work often targeted narrower subgroups or reported heterogeneous protocols, which limited generalizability such as [40] & [33]. For a better example Bouaziz et al. (2015) reviewed cycle ergometer training in adults aged ≥ 70 years but our review extends applicability by including both healthy and clinical populations from 60 years onwards without limiting study types. This broader perspective provides more generalizable and evidence-based recommendations for implementation in both clinical and community settings. Therefore, we advocate for more research into SB cycling among older adults (≥ 60 years) to recommend disease specific exercise dosage to get a better health outcome.
Strength of the study
This review is robust due to its comprehensive data collection and rigorous methodology. By searching seven multidisciplinary databases and applying broad selection criteria, we captured a wide range of relevant studies. Independent review, multiple testing of data inclusion, and evidence-based acceptability assessments ensured reliability. Study quality was evaluated using the PEDro scale and ROB 2.0 from the Cochrane Handbook, revealing mostly good quality and low risk of bias. Use of the PRISMA checklist and TIDieR framework enhanced transparency and rigor. Focusing on older adults (60+) addressed a neglected population, and including both RCTs and non-RCTs provided a comprehensive understanding of SB interventions, balancing internal validity with real-world applicability.
Challenges
Included limited access to full-text articles and the lack of a standardized tool for assessing acceptability of SB interventions. Due to sparse data, studies were deemed fully acceptable only with 100% acceptance, adherence, and retention, with no dropouts. Missing data may have affected acceptability estimates, and dropout rates inversely influenced adherence and retention, complicating interpretation. Effect sizes (e.g., Hedges’ g) could not be calculated due to unreported data, so inferred effect sizes were considered [66]. Studies combining SB with VA showed more consistent data than other combinations, highlighting VA as a promising intervention tool. Despite these limitations, the review provides valuable insights into the efficacy of SB interventions in older adults.
Conclusion
A review of 47 studies found that stationary biking shows moderate acceptability (38%) and yields significant benefits in VO_2_ max, cycling efficiency, cognition, executive function, quality of life, and mobility (Timed Up and Go test) in adults aged ≥ 60. When combined with VA, SB improves adherence and further enhances physical and cognitive outcomes across both healthy and clinical populations. Therefore, high quality RCTs are needed to establish optimal exercise prescriptions, and to support stronger evidence for SB combined with VA as a promising, low-risk strategy to promote healthy aging and maintain functional independence in later life.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
Supplementary Material 3.
Supplementary Material 4.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ageing. and health. https://www.who.int/news-room/fact-sheets/detail/ageing-and-health. Accessed 5 Apr 2024.
- 2Global recommendations on physical activity for health. https://www.who.int/publications-detail-redirect/9789241599979. Accessed 5 Apr 2024.
- 3Katyal S, Freeman M, Miller JA, Thomas SG. Short-term aerobic training and circulatory function in women: age and hormone- replacement therapy. 2003.10.1042/CS 2002017912605585 · doi ↗ · pubmed ↗
- 4Anderson-Hanley C, Arciero P. Snyder. Social facilitation in virtual reality-enhanced exercise: competitiveness moderates exercise effort of older adults. CIA. 2011;275.10.2147/CIA.S 25337 PMC 321241922087067 · doi ↗ · pubmed ↗
- 5Colombo V, Mondellini M, Fumagalli A, Aliverti A, Sacco M. A virtual reality-based endurance training program for COPD patients: acceptability and user experience. Disabil Rehabil Assist Technol. 2023:1–10.10.1080/17483107.2023.221969937272556 · doi ↗ · pubmed ↗
- 6Schwarck S, Busse N, Ziegler G, Glanz W, Becke A, Düzel E. Heart rate variability during physical exercise is associated with improved cognitive performance in alzheimer’s dementia Patients-A longitudinal feasibility study. Front Sports Act Living. 2021;3.10.3389/fspor.2021.684089 PMC 831923734337405 · doi ↗ · pubmed ↗