Excess risk and resource utilization in dialysis-dependent patients undergoing total hip arthroplasty: insights from a nationally representative database
David Maman, Yaniv Steinfeld, Yaron Berkovich

TL;DR
Dialysis-dependent patients undergoing hip replacement surgery face much higher risks and costs compared to others, even after adjusting for other health factors.
Contribution
This study provides new evidence that dialysis dependence is a strong independent predictor of worse outcomes after total hip arthroplasty.
Findings
Dialysis-dependent patients had 10.1 times higher in-hospital mortality after THA compared to non-dialysis patients.
Hospital stays were 62.5% longer and hospital charges were 95.8% higher for dialysis-dependent patients.
Major complications were significantly more frequent in dialysis-dependent patients.
Abstract
Total hip arthroplasty (THA) reliably restores function and quality of life in patients with end-stage hip disease. Individuals with end-stage renal disease (ESRD) requiring dialysis are vulnerable to perioperative complications due to immune dysfunction, hemodynamic instability, and impaired wound healing. Evidence on risk-adjusted outcomes remains limited. A retrospective cohort study was conducted using the Nationwide Inpatient Sample (2016–2022). Dialysis dependence was identified using ICD-10-CM Z99.2. Primary outcomes included in-hospital mortality, length of stay (LOS), and hospital charges; secondary outcomes were major complications. Propensity score matching (10:1 nearest neighbour) balanced baseline demographics and comorbidities. Survey weights were used for national estimates. Post-matching outcomes were compared using risk ratios (RR) with 95% CIs. Among 1,957,284 THA…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
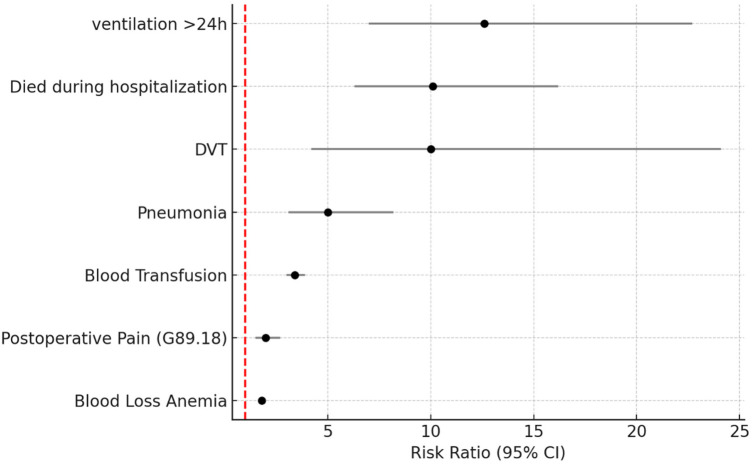 Figure 1
Figure 1| Parameter | No renal dialysis dependence | Renal dialysis dependence | Significance |
|---|---|---|---|
| Total surgeries | 1,954,554 (99.9%) | 2,730 (0.1%) | — |
| Average age (years) | 66.2 | 64.4 | |
| Female (%) | 56.3 | 40.0 | |
| Dyslipidemia (%) | 43.7 | 51.3 | |
| Chronic anemia (%) | 5.6 | 13.7 | |
| Osteoporosis (%) | 4.6 | 5.1 | |
| Type 2 diabetes (%) | 15.6 | 43.8 | |
| Congestive heart failure (%) | 1.2 | 7.1 | |
| Chronic lung disease (%) | 6.6 | 11.5 | |
| Liver disease (%) | 1.2 | 1.8 | |
| History of myocardial Infarction (%) | 3.5 | 7 | |
| History of cerebrovascular accident (%) | 3.9 | 10.3 | |
| Obesity (%) | 24.4 | 24.5 |
| Parameter | No renal dialysis dependence | Renal dialysis dependence | Risk ratio (95% CI) | Significance |
|---|---|---|---|---|
| Died during hospitalization in % | 0.03% | 1.30% | 31.9 (95% CI: 22.7–44.9) |
| Parameter | No renal dialysis dependence | Renal dialysis dependence | Significance |
|---|---|---|---|
| Total surgeries | 27,299 (90.9%) | 2,730 (9.1%) | — |
| Average age (years) | 64.8 | 64.4 | |
| Female (%) | 38.4 | 40.0 | |
| Dyslipidemia (%) | 52 | 51.3 | |
| Chronic anemia (%) | 12.8 | 13.7 | |
| Osteoporosis (%) | 5 | 5.1 | |
| Type 2 diabetes (%) | 43.3 | 43.8 | |
| Congestive heart failure (%) | 6.7 | 7.1 | |
| Chronic Lung disease (%) | 11.3 | 11.5 | |
| Liver disease (%) | 1.8 | 1.8 | |
| History of myocardial infarction (%) | 6.6 | 7 | |
| History of Cerebrovascular accident (%) | 11.1 | 10.3 | |
| Obesity (%) | 24.5 | 24.5 |
| Parameter | No renal dialysis dependence | Renal dialysis dependence | Percent increase | Significance |
|---|---|---|---|---|
| Length of stay mean in days | 2.4 (Std. deviation 1.7) | 3.9 (Std. deviation 3.4) | 62.5% | |
| Total charges mean in $ | 60,741 (Std. Deviation 33,418) | 98,454 (Std. deviation 118,945) | 95.8% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Bone and Joint Diseases · Orthopaedic implants and arthroplasty
Introduction
Total hip arthroplasty (THA) is one of the most common and cost-effective surgical interventions for end-stage hip disease, consistently providing substantial pain relief and functional improvement (1). With an aging population and rising prevalence of degenerative joint disease, the number of primary THA procedures is projected to grow steadily worldwide over the coming decades (2). While perioperative complication rates for THA remain low in the general population, certain subgroups including patients with significant comorbidities are known to have disproportionately higher risks and resource utilization (3, 4).
End-stage renal disease affects patients across a wide age spectrum, though the burden increases markedly with advancing age. Recent epidemiologic reports show that dialysis dependence is most prevalent in older adults, who also represent a growing proportion of candidates for elective THA. Prior studies evaluating arthroplasty outcomes in dialysis-dependent patients although limited in size have consistently demonstrated elevated complication rates, higher perioperative mortality, and greater resource utilization compared with the general population. These findings underscore the importance of studying this high-risk group in a large, nationally representative cohort such as the NIS.
Patients with end-stage renal disease (ESRD) represent a particularly vulnerable population. Dialysis dependence is associated with profound alterations in immune function, bone metabolism, and hemostasis, which may predispose to infection, impaired wound healing, anemia, and cardiovascular instability. These physiological factors, combined with a higher baseline comorbidity burden, may lead to worse perioperative outcomes, longer hospitalizations, and higher costs following elective orthopedic procedures.
Despite these concerns, large-scale studies specifically examining the impact of renal dialysis dependence on THA outcomes remain limited. Most prior investigations have been single-center series or have combined THA and TKA into a single “arthroplasty” cohort, limiting the ability to draw THA-specific conclusions. Furthermore, many reports lack rigorous risk adjustment, leaving uncertainty regarding whether adverse outcomes are attributable to dialysis itself or to confounding patient characteristics (5)
The present study aimed to fill this knowledge gap by leveraging the Nationwide Inpatient Sample (NIS), the largest all-payer inpatient database in the United States, to examine outcomes of primary THA among patients with and without renal dialysis dependence (6). We sought to (1) compare patient demographics and comorbidities between dialysis and non-dialysis groups, (2) quantify differences in perioperative complications, length of stay, hospital charges, and in-hospital mortality, and (3) apply propensity score matching to generate well-balanced cohorts, providing an adjusted assessment of dialysis-specific risk (7).
Materials and methods
Data source
This study utilized the Nationwide Inpatient Sample (NIS), a stratified and weighted database within HCUP. NIS sampling weights, stratification variables, and clustering by hospital were applied according to HCUP recommendations to generate nationally representative estimates.
Exposure definition
Renal dialysis dependence was defined using ICD-10-CM Z99.2. This code generally captures patients receiving chronic dialysis; however, the NIS does not differentiate dialysis modality, ESRD stage, or timing of treatments, and acute/temporary dialysis may be under-captured. This potential misclassification is acknowledged as a study limitation.
Patient selection
We included all adult patients (≥18 years) who underwent elective primary total hip arthroplasty (THA) as identified by relevant ICD-10-PCS procedure codes. We excluded revision THA procedures, urgent or trauma-related admissions, and cases missing key demographic information. Discharges with COVID-19-related codes were omitted to avoid confounding from pandemic-related risk factors.
Renal dialysis dependence was defined by the ICD-10-CM diagnosis code Z99.2 (“Dependence on Renal Dialysis”). Patients were stratified into two cohorts based on dialysis status for comparative analysis.
Variables and comorbidities
Baseline variables included demographic data (age, sex, race, and primary payer) and clinical comorbidities derived from ICD-10-CM codes. Comorbidities of interest included dyslipidemia, chronic anemia, osteoporosis, type 2 diabetes mellitus, congestive heart failure, chronic lung disease, liver disease, prior myocardial infarction, and prior cerebrovascular accident. Obesity was included as an additional risk factor.
Endpoints
Our primary outcomes were:
- In-hospital mortality
- Length of stay (LOS), reported as mean ± standard deviation
- Total hospital charges, reported in U.S. dollars Secondary outcomes consisted of major postoperative complications, including blood loss anemia, perioperative blood transfusion, pneumonia, prolonged mechanical ventilation (>24 h), deep vein thrombosis (DVT), and postoperative pain (ICD-10-CM G89.18). For each binary outcome, risk ratios (RR) with 95% confidence intervals (CI) were computed.
Propensity score matching
Propensity scores were computed using logistic regression including demographics, comorbidities, and hospital characteristics (teaching status, region, and bed size). A 10:1 nearest-neighbour match without replacement was used. Standardized mean differences (SMDs) were examined to confirm covariate balance.
Statistical analysis
After matching, outcomes were evaluated using risk ratios with 95% CIs. Because standard chi-square tests assume independent observations, we conducted sensitivity analyses using variance estimates clustered on matched sets. Results were materially unchanged. The assumption of independence within matched sets is acknowledged as a methodological limitation.
Additional descriptive statistics, including weighted national estimates, standard errors, and confidence intervals, were reviewed to ensure robustness and interpretability of the findings.
Missing data
A complete-case approach was used. Records with missing essential variables were excluded during cohort construction, and the number of exclusions was negligible relative to the overall sample size.
Ethical aspects
Because the NIS is a publicly available, de-identified database, this study was considered exempt from institutional review board (IRB) approval and did not require informed consent.
Results
Table 1 summarizes the demographic and clinical characteristics of all 1,957,284 total THA patients, of whom 2,730 (0.1%) were dependent on renal dialysis. Patients with dialysis dependence were slightly younger than those without (64.4 vs. 66.2 years, p < 0.01) and had a markedly lower proportion of female patients (40.0% vs. 56.3%, p < 0.01).
Several comorbidities were significantly more prevalent in dialysis-dependent patients, including dyslipidemia (51.3% vs. 43.7%), chronic anemia (13.7% vs. 5.6%), congestive heart failure (7.1% vs. 1.2%), chronic lung disease (11.5% vs. 6.6%), liver disease (1.8% vs. 1.2%), history of myocardial infarction (7.0% vs. 3.5%) and cerebrovascular accident (10.3% vs. 3.9%) (p < 0.01 for all).
There were no significant differences between the groups regarding obesity (24.5% vs. 24.4%, p = 0.86).
In-Hospital mortality in patients with and without renal dialysis dependence in total hip arthroplasty
Table 2 presents in-hospital mortality rates for patients undergoing THA, stratified by renal dialysis dependence. Mortality was markedly higher among dialysis-dependent patients (1.30%) compared with those without dialysis dependence (0.03%), corresponding to a 31.9-fold increased risk (95% CI: 22.7–44.9, p < 0.01). This represents the crude (unmatched) mortality difference. The matched mortality effect size is presented in the postoperative complications analysis (RR: 10.1, 95% CI: 6.3–16.2), reflecting the adjusted risk after balancing baseline covariates.
Demographic and clinical characteristics after 10:1 propensity score matching among patients undergoing total hip arthroplasty with and without renal dialysis dependence
To mitigate confounding and reduce baseline imbalances, a 10:1 propensity score matching procedure was applied using demographic and clinical covariates including age, sex, and major comorbid conditions.
Following matching, the two cohorts were closely aligned across all measured variables (Table 3). There were no significant differences in age (64.4 vs. 64.8 years, p = 0.11), sex distribution (40.0% vs. 38.4% female, p = 0.08), or prevalence of key comorbidities such as dyslipidemia, chronic anemia, type 2 diabetes, congestive heart failure, chronic lung disease, and liver disease (p > 0.05 for all comparisons). Rates of prior myocardial infarction, cerebrovascular accident, osteoporosis, and obesity were also comparable.
This high degree of covariate balance supports the validity of subsequent outcome analyses, minimizing residual confounding and allowing for a more accurate assessment of the impact of renal dialysis dependence on perioperative outcomes.
Post-matching comparison of hospital resource utilization
Table 4 summarizes hospital resource utilization after 10:1 propensity score matching. Dialysis-dependent patients had a significantly prolonged length of stay compared to matched controls (3.9 ± 3.4 vs. 2.4 ± 1.7 days, p < 0.01), representing a 62.5% increase.
Similarly, mean total hospitalization charges were markedly higher in the dialysis group (60,741 ± 33,418, p < 0.01), reflecting a 95.8% cost increase despite baseline covariate balance.
These findings suggest that even after accounting for differences in patient characteristics, renal dialysis dependence is independently associated with greater hospital resource consumption during THA admissions.
Postoperative complications after 10:1 propensity score matching among patients undergoing total hip arthroplasty with and without renal dialysis dependence
Figure 1 the risk ratios (RR) and 95% confidence intervals (CI) for major postoperative complications associated with renal dialysis dependence. Patients on dialysis had a 1.8-fold higher risk of blood loss anemia (RR: 1.8, 95% CI: 1.7–2.0, p < 0.01) and a 3.4-fold higher risk of requiring blood transfusion (RR: 3.4, 95% CI: 3.0–3.9, p < 0.01) compared with non-dialysis patients. The risk of pneumonia was also markedly elevated (RR: 5.0, 95% CI: 3.1–8.2, p < 0.01).
Forest plot of postoperative complications after 10:1 propensity score matching Among patients undergoing total Hip arthroplasty With and without renal dialysis dependence.
Severe complications showed even stronger associations: in-hospital mortality was 10.1 times higher (RR: 10.1, 95% CI: 6.3–16.2, p < 0.01), and the risk of requiring mechanical ventilation >24 h was the highest observed, 12.6-fold greater than controls (95% CI: 7.0–22.7, p < 0.01).
The incidence of deep vein thrombosis (DVT) was also significantly elevated (RR: 10.0, 95% CI: 4.2–24.1, p < 0.01), while postoperative pain was doubled (RR: 2.0, 95% CI: 1.5–2.7, p < 0.01). As expected, the magnitude of the mortality association decreased after matching (RR: 10.1) compared with the crude estimate (RR: 31.9), consistent with improved covariate balance.
Discussion
In this large, nationally representative study of nearly two million primary THA patients, renal dialysis dependence was strongly associated with increased perioperative morbidity, mortality, and resource utilization. Even after rigorous 10:1 propensity score matching, dialysis-dependent patients demonstrated >60% longer hospital stays, nearly doubled hospital charges, and a markedly elevated in-hospital mortality risk (10.1-fold after matching), consistent in direction with the larger crude difference observed before matching (31.9-fold). This degree of excess risk far exceeds what is typically observed for other single comorbidities and highlights the substantial vulnerability of this patient population undergoing elective THA (4, 8).
Interpretation of key findings
Our results highlight several clinically meaningful observations. First, dialysis patients undergoing THA had a dramatically higher burden of cardiovascular and hematologic disease, including anemia, congestive heart failure, and prior myocardial infarction, which are well-established predictors of perioperative complications (3). These comorbidities likely contribute to the increased rates of pneumonia, prolonged mechanical ventilation, and blood transfusion observed in this cohort.
Second, the magnitude of risk for hard endpoints was striking: after matching, dialysis-dependent patients had a 10.1-fold higher mortality risk and >12-fold higher need for prolonged ventilation compared with non-dialysis patients. These findings underscore the vulnerability of this population and suggest that standard perioperative protocols may be insufficient to mitigate risk. Dialysis dependence is not merely a marker of comorbidity it is a clinical state characterized by impaired host defense, altered hemodynamics, and metabolic fragility that collectively amplify perioperative hazards.
Comparison to previous literature
Prior work examining THA in dialysis patients has been limited to small single-center cohorts or combined analyses of hip and knee arthroplasty, leading to inconsistent results. Several studies have reported elevated infection rates, increased medical complications, and early mortality among ESRD patients, but few have quantified these risks in a nationally representative and THA-specific cohort. Our study builds on this literature by offering the largest adjusted analysis to date, using modern data and robust matching methodology, thereby providing definitive evidence of the heightened perioperative risk profile for dialysis-dependent patients undergoing THA.
Our findings are consistent with registry-based analyses demonstrating excess complications and poorer implant survivorship in ESRD patients, but they further quantify the economic burden, which has received less attention in the literature. The nearly 96% increase in hospitalization costs has significant implications for bundled payment models and value-based care initiatives (9, 10).
Clinical implications
These results carry immediate relevance for surgical decision-making and perioperative care pathways. Patient counseling should explicitly communicate the elevated risks of complications and death, allowing patients and families to make informed choices. Multidisciplinary preoperative planning including optimization of anemia, nutrition, and cardiovascular status should be considered mandatory. Coordination of dialysis timing to minimize perioperative fluid and electrolyte shifts, along with early involvement of nephrology and anesthesia teams, may mitigate some of the observed risk.
Enhanced recovery after surgery (ERAS) protocols should be specifically tailored to this high-risk subgroup, emphasizing infection prevention, early mobilization, and careful hemodynamic management. Given the high resource utilization demonstrated here, health systems and payers may consider implementing specialized perioperative pathways or postoperative monitoring programs for dialysis patients to improve outcomes and control costs (9, 10).
Strengths and limitations
This study's strengths include its large, nationally representative sample size, ability to generate generalizable risk estimates, and use of propensity score matching to reduce baseline differences and strengthen causal inference. However, some limitations are inherent to the use of administrative databases. The NIS does not include granular clinical details such as dialysis modality, timing relative to surgery, laboratory values (e.g., hemoglobin, electrolytes), or long-term outcomes such as 30-day readmission or prosthetic joint infection. Residual unmeasured confounding remains possible despite matching (5, 11–13). Nonetheless, the consistency and magnitude of the associations observed strongly support the robustness of our finding.
Because the NIS is a stratified, weighted database, survey weights, strata, and hospital-level clustering were applied according to HCUP recommendations. Post-matching analyses assume independence within matched sets; although sensitivity checks using clustered variance estimates yielded similar results, some underestimation of uncertainty remains possible. Dialysis dependence was identified using ICD-10-CM Z99.2, which may not capture all ESRD patients or distinguish chronic from acute dialysis, introducing potential exposure misclassification. Important clinical factors such as frailty, functional status, dialysis modality, and timing of dialysis relative to surgery are unavailable in the NIS and may contribute to residual unmeasured confounding.
Future directions
Future prospective studies should evaluate strategies to reduce perioperative risk in this population, including prehabilitation programs, optimized dialysis scheduling, perioperative erythropoietin and iron therapy, and novel blood management strategies (14–18). Given the substantial economic burden, cost-effectiveness analyses of intensified preoperative optimization protocols in dialysis patients undergoing THA are warranted.
Conclusions
Renal dialysis dependence is a strong independent predictor of adverse outcomes following primary THA. These patients face dramatically higher mortality, complication rates, and resource use, even after adjustment for comorbidities. Our findings emphasize the need for personalized perioperative pathways, meticulous patient selection, and targeted quality improvement efforts aimed at reducing morbidity and optimizing outcomes in this high-risk population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fontalis A Epinette J-A Thaler M Zagra L Khanduja V Haddad FS. Advances and innovations in total hip arthroplasty. SICOT J. (2021) 7:26. 10.1051/sicotj/202102633843582 PMC 8040589 · doi ↗ · pubmed ↗
- 2Shichman I Roof M Askew N Nherera L Rozell JC Seyler TM Projections and epidemiology of primary hip and knee arthroplasty in medicare patients to 2040–2060. JBJS Open Access. (2023) 8:e 22.00112. 10.2106/JBJS.OA.22.0011236864906 PMC 9974080 · doi ↗ · pubmed ↗
- 3Wainwright TW Gill M Mc Donald DA Middleton RG Reed M Sahota O Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: enhanced recovery after surgery (ERAS®) society recommendations. Acta Orthop. (2020) 91(1):3–19. 10.1080/17453674.2019.168379031663402 PMC 7006728 · doi ↗ · pubmed ↗
- 4D’Onghia M Ciaffi J Mc Veigh JG Di Martino A Faldini C Ablin JN Fibromyalgia syndrome—a risk factor for poor outcomes following orthopaedic surgery: a systematic review. Semin Arthritis Rheum. (2021) 51(4):793–803. 10.1016/j.semarthrit.2021.05.01634153893 · doi ↗ · pubmed ↗
- 5Utter GH Cox GL Owens PL Romano PS. Challenges and opportunities with ICD-10-CM/PCS: implications for surgical research involving administrative data. J Am Coll Surg. (2013) 217:516–26. 10.1016/j.jamcollsurg.2013.04.01823891069 · doi ↗ · pubmed ↗
- 6Maman D Fournier L Steinfeld Y Berkovich Y. Etiology, outcomes, and complications of total hip arthroplasty in younger patients: a nationwide big data analysis. J Clin Med. (2024) 13:4535. 10.3390/jcm 1315453539124801 PMC 11313375 · doi ↗ · pubmed ↗
- 7Jain N Phillips FM Weaver T Khan SN Xu T Patterson M Prediction of complications, readmission, and revision surgery based on duration of preoperative opioid use: analysis of major joint replacement and lumbar fusion. J Bone Joint Surg Am. (2019) 101:384–91. 10.2106/JBJS.18.0050230845032 · doi ↗ · pubmed ↗
- 8Jain N Brock JL Malik AT Phillips FM Khan SN. Impact of fibromyalgia on postoperative outcomes after primary total hip arthroplasty: a national database study. J Arthroplasty. (2019) 34(3):497–500. 10.1016/j.arth.2018.11.014 · doi ↗