Genetic liability to psoriasis predicts severe disease outcomes
Jake R. Saklatvala, Samuel Lessard, Maris Teder-Laving, Laurent F. Thomas, Ravi Ramessur, Jonas Zierer, Bjørn Olav Åsvold, Anne Barton, David Baudry, John Bowes, Ben Brumpton, Sandro Bruno, Vinod Chandran, Clément Chatelain, Emanuele de Rinaldis, James T. Elder, David Ellinghaus

TL;DR
This study shows that genetic risk scores can predict which psoriasis patients are more likely to develop severe disease, potentially improving early intervention and resource allocation.
Contribution
The study introduces a genetic polygenic risk score as a novel and effective biomarker for predicting severe psoriasis outcomes.
Findings
Genetic variants in MHC, TNIP1, and IL12B are strongly associated with severe psoriasis.
A psoriasis polygenic risk score (PRS) is a strong predictor of disease severity, comparable to obesity and smoking.
Top 5% of psoriasis cases by PRS are 1.23-2.00 times more likely to have severe disease.
Abstract
Psoriasis is a common inflammatory skin disease with heterogeneous presentation. Up to 30% of individuals have severe disease with a greater surface area of skin involvement, co-morbidity burden and impact on quality of life. Prognostic biomarkers of psoriasis severity could improve allocation of clinical resources and enable earlier intervention to prevent disease progression, and a genetic biomarker would be cost-effective, stable over time, and unaffected by treatment or comorbidity. Psoriasis severity was studied in four European population-based biobanks (Estonian Biobank, HUNT, FinnGen, UK Biobank) and classified based on level of clinical intervention received, with criteria for severe disease including hospitalisation due to psoriasis, use of systemic immunomodulating therapy or phototherapy. Common genetic variants, polygenic risk scores and traditional epidemiological risk…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
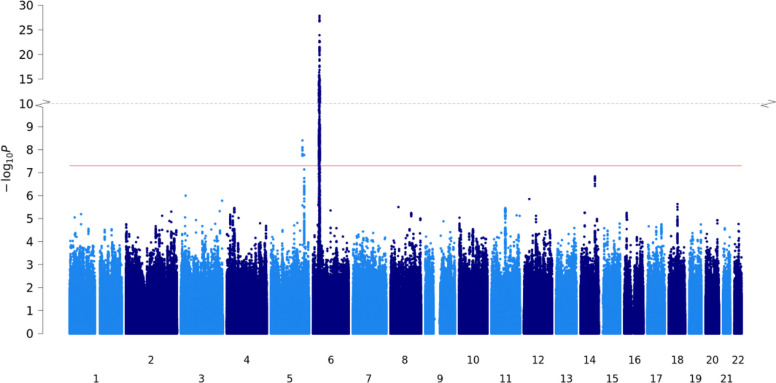 Figure 1
Figure 1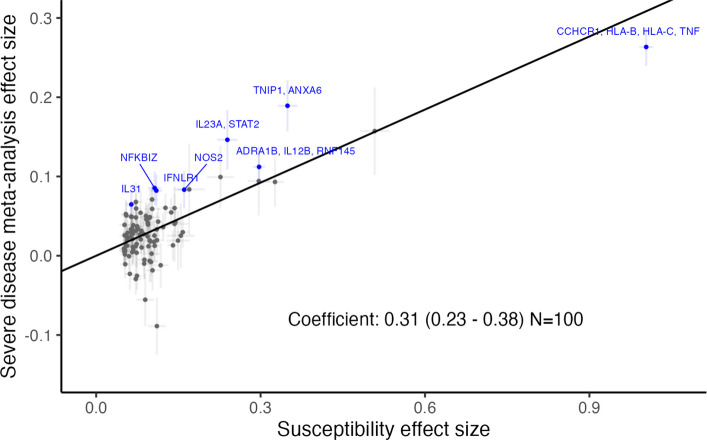 Figure 2
Figure 2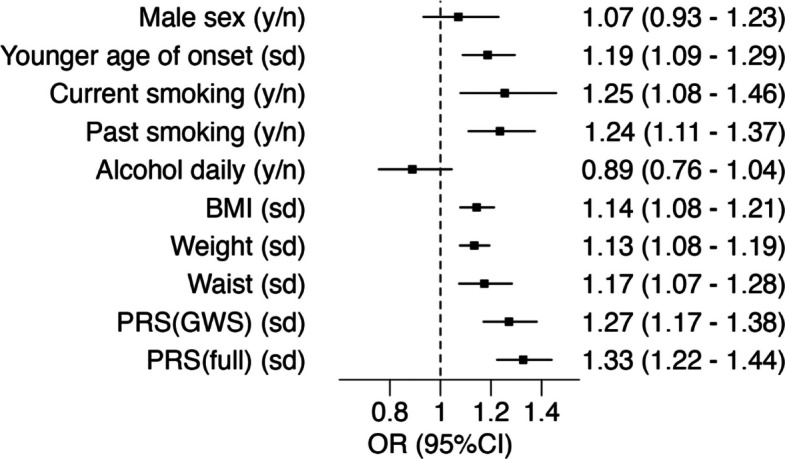 Figure 3
Figure 3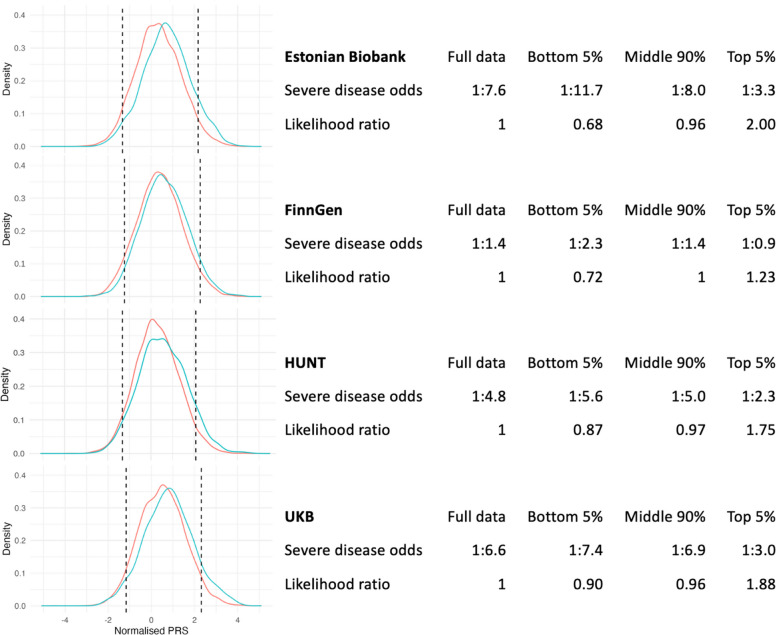 Figure 4
Figure 4- —Innovative Medicines Initiative 2 Joint Undertaking
- —Estonian Research Council
- —Clinician scientist salary award from the department of medicine, University of Toronto
- —UK Medical Research Council Integrative Epidemiology Unit
- —NIHR Advanced Fellowship
- —Wellcome Trust
- —Medical Research Council, Rosetrees Trust, Stoneygates Trust, British Skin Foundation, Charles Wolfson Charitable Trust, anonymous donations from people with eczema, Unilever, Pfizer, Abbvie, Sosei-He
- —Liaison Committee for Education, Research and Innovation in Central Norway
- —Joint Research Committee between St Olavs Hospital and the Faculty of Medicine and Health Sciences, NTNU
- —NIHR Senior Investigator Award
- —Innovative Medicines Initiative 2 Joint Undertaking, 821511
- —Leo Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsoriasis: Treatment and Pathogenesis · BRCA gene mutations in cancer · Biomedical Research and Pathophysiology
Background
Psoriasis is a common inflammatory skin disease in which the extent of skin inflammation and impact on the affected individual can vary greatly [1]. Most affected individuals have relatively mild disease, but an estimated 10–30% of individuals with psoriasis have over 10% of their body surface area affected, a commonly used benchmark for more severe skin involvement [2, 3]. Co-morbid burden and impact on quality of life have been shown to increase with increasing skin severity [4, 5].
Many epidemiological risk factors for psoriasis have also been shown to associate with increased severity, including male sex [6], smoking [7], obesity [8], diet [9] and alcohol usage [10]. Some of these risk factors are modifiable and important to proactively manage. Weight loss following lifestyle intervention, for example, has been demonstrated to reduce psoriasis severity [11]. There have also been dramatic advances in therapeutics driven by better understanding of psoriasis biology, with highly targeted, though costly, systemic immunomodulators delivering clear or nearly clear skin in most individuals.
Severe psoriasis has a considerable societal impact, both directly and due to the high burden of comorbidities. The financial cost is substantial [12], including both the costs of clinical intervention and indirect costs due to lost productivity [13]. Rising demand for dermatology services due to aging populations, recent targeted treatments and the increasing prevalence of common skin conditions presents a further challenge in directing care to individuals efficiently [14]. The current treatment approach for psoriasis is reactive, lacking systematic approaches to stratify the patient population based on prognostic risk. Identification of reliable prognostic indicators for psoriasis would provide opportunities to ease disease burden through a stratified, proactive healthcare approach, including early onward referral from primary care settings, enhanced monitoring of highest-risk populations for skin inflammation and/or comorbidities, as well as recommendation of early lifestyle or therapeutic intervention to reduce and even prevent cumulative impact on quality of life. Psoriatic arthritis, for example, is a well-established inflammatory comorbidity of psoriasis where early identification and treatment can limit permanent functional deterioration [15]. Emerging evidence in psoriasis supports the notion that early intervention may prevent inflammatory memory and increase the chance of long-term drug-free remission [16, 17].
For several common diseases, genetic prediction using polygenic risk scores (PRS) can identify significant proportions of individuals with increased disease risk [18], and the clinical utility of communication of genetic risk has been demonstrated in cardiovascular disease [19, 20].
While psoriasis susceptibility has a strong genetic basis, with heritability of more than 60% [21], and over 100 established susceptibility loci [22], there is comparatively little evidence on the genetic involvement in disease severity. Several small studies have tested a limited number of candidate genetic variants for associations with severity [23] as assessed using objective measures of skin involvement or health care use proxies and report associations with HLA-C06:02* [24–27] and variation at IL23R [28–30], LCE3D [27], NFKBIL1 and IL23A loci [29]. Psoriasis polygenic risk has been tested for association with both disease incidence and clinical features [31, 32], and there is a single study where an increase in psoriasis PRS was reported to be associated with dermatologist-rated severity in a cohort of 654 psoriasis cases, though this could not be replicated with non-HLA polygenic risk alone [33].
Here we report an analysis of 44,904 individuals with psoriasis across four large population-based datasets (UK Biobank, Trøndelag Health Study [HUNT], FinnGen and the Estonian Biobank) to systematically assess the role of genetic variation in psoriasis severity. We took advantage of wide population-scale data collection, including linked electronic health record (EHR) data, to adopt a binary definition of severe disease based on the level of clinical intervention received [34, 35] and evaluated the association of genome-wide genetic variation, genetic instruments in the form of PRS and epidemiological risk factors on a dichotomised psoriasis severity phenotype.
Methods
Population-based cohorts
Four population-based datasets were used, where both psoriasis and severe-psoriasis phenotypes were defined, GWAS were performed (followed by regression of effect sizes), polygenic risk scores (PRS) were compared between severe and non-severe psoriasis populations, and PRS and epidemiological association testing was calculated. Estonian Biobank includes mainly European-ancestry volunteer participants, for whom a variety of health-related and demographic information as well as biological samples have been collected [36]. Of 205,260 individuals, 14,167 were defined as having psoriasis (Additional file 1: Table S1) based on ICD-10 codes in data collected from the biobank’s health database which is regularly linked with national electronic health registries, including hospital databases (Additional file 1: Table S2). FinnGen is a public–private partnership research project that combines genotype data generated from newly collected and legacy samples from Finnish biobanks and digital health record data from Finnish health registries (https://www.finngen.fi/en), with university-hospital-based recruitment [37]. Of 473,681 individuals, 12,708 were defined as having psoriasis (Additional file 1: Table S1) based on ICD codes in inpatient and outpatient visit registries as well as drug purchase and reimbursement records (Additional file 1: Table S2). The Trøndelag Health Study (HUNT) is a population-based cohort where participants were recruited during four community-based recruitment waves and provided information on health-related behaviours, self-reported diagnoses, family history of disease, and underwent physical examinations. Linkage via the Norwegian personal identification number integrates digitised health care information from doctor visits and national health registries including death, cancer and prescription registries [38]. Of 86,405 individuals, 8603 were defined as having psoriasis (Additional file 1: Table S1) based on either self-reporting, a diagnosis by a dermatologist, a diagnosis within hospital records and/or private specialist practitioners (ICD9/10), a GP diagnosis (ICPC-2) or a prescription in the Norwegian Prescription database (ICD10, ICPC-2) (Additional file 1: Table S2). The UK Biobank contains variety of phenotypic and health-related information, including linkage to health and medical records, as well as genome-wide genotype data on volunteers aged 40–69 at recruitment [39]. Of 462,817 European-ancestry individuals, 9426 were defined as having psoriasis (Additional file 1: Table S1) based on diagnosis within hospital inpatient records (ICD10), self-reporting or a GP diagnosis (Read codes), as well as presence in full linked data including GP records (Additional file 1: Table S2).
Psoriasis-only cohorts
Two psoriasis-only cohorts, BSTOP and Novartis clinical trials of secukinumab, were used to compare psoriasis polygenic risk distributions to various UK Biobank sub-cohorts (severe psoriasis, non-severe psoriasis, any psoriasis, non-psoriasis and full population). BSTOP is an ongoing prospective observational study of patients with a primary diagnosis of moderate‒severe plaque psoriasis across > 70 UK dermatology centres, which includes biological sample collection. Full inclusion criteria have been described previously [40], which include having started conventional systemic or biologic therapy within the previous 6 months, with a final genotyped sample size of 4151. Novartis data was collected from five clinical trials of secukinumab in psoriasis (details available on https://clinicaltrials.gov/): CAIN457A2302 (NCT01365455), CAIN457A2303 (NCT01358578), CAIN457A2304 (NCT01406938), CAIN457A2223 (NCT01537432), CAIN457A2403 (NCT03553823). Details of genotyping are described in Additional file 2: Supplementary Methods, with final genotyped sample size of 1461.
Severity phenotype definition in population-based cohorts
We followed recently published guidelines [34] suggesting that a dichotomous definition of psoriasis severity could be employed in population-based datasets, using level of clinical intervention recorded as a proxy for severe disease. Individuals with psoriasis diagnoses were categorised as having severe disease if they had evidence of hospitalisation due to psoriasis or use of systemic immunomodulators (conventional systemic agents, targeted biologics, oral small molecule inhibitors) or phototherapy (narrow-band ultraviolet B radiation, psoralen with ultraviolet A radiation). Remaining individuals with psoriasis were categorised as non-severe. These criteria were applied to individuals with psoriasis in four population-based datasets—Estonian Biobank, FinnGen, HUNT and UK Biobank—with full details of codes and data fields used in Additional file 1: Table S2-S7.
Genotyping and genetic association testing
Genome-wide association studies (GWAS) were performed separately in each population-based cohort ( Biobank, FinnGen, HUNT, UK Biobank) using logistic mixed-effect models comparing individuals with severe disease to those with non-severe disease, controlling for age, sex, genotyping batch(es), relatedness and an appropriate number of ancestry principal components (full details of genotyping, imputation, and cohort-specific models in Supplementary Methods).
QC and meta-analysis
Post-GWAS quality control and harmonisation of summary statistics were performed using GWASinspector [41], mapping to Genome Reference Consortium Human Build 37 patch release 13 reference and filtering for variants with INFO > 0.7 and MAF > 1%. Fixed-effects standard error-weighted meta-analysis was performed using METAL software (version release: 2020–05-05) [42].
Genetic correlation
Genetic correlations were calculated using LDSC [43], comparing the summary statistics of (i) the severe disease meta-analysis and (ii) a psoriasis susceptibility meta-analysis, constraining intercepts to 1. The susceptibility summary statistics were derived from a recently published meta-analysis [22] reanalysed after removing studies that overlap with the cohorts used in the present work (total 19,842 psoriasis cases and 33,108 controls, Additional file 1: Table S8).
Effect size regression
Of the 109 loci (linkage equilibrium [LD]-partitioned genomic regions) associated with psoriasis at genome-wide significance (P < 5.0 × 10^−8^) in the latest susceptibility meta-analysis [22], 100 retained genome-wide significant variants when considering only variants that were present in all four severe disease GWAS. For each of these 100 susceptibility loci, the lead available variant was used in a regression of effect sizes between susceptibility and severe disease, using a Deming regression (constraining the intercept to zero) that accounts for measurement error in both variables. Effect size regressions were performed comparing susceptibility meta-analysis effect sizes against (a) severe disease meta-analysis effect sizes and (b) effect sizes from each severe disease GWAS individually. To check that the observed relationships were robust to the inclusion of three of our severe disease datasets (Estonian Biobank, HUNT and UK Biobank) in the susceptibility meta-analysis, the following sensitivity analyses were performed:
- Using the same 100 lead variants but recalculating the susceptibility effect sizes in a meta-analysis that excludes our severe disease cohorts (described above and in Additional file 1: Table S8).
- Selecting lead variants and corresponding effect sizes for 65 loci that achieve genome-wide significance in the recalculated susceptibility meta-analysis (excluding severe disease cohorts).
For each cohort, an additional follow-up sensitivity analysis was performed omitting the lead variants from the major histocompatibility complex (MHC) LD block due to its large individual effect size.
Polygenic risk score (PRS)
Variants eligible for inclusion in PRS were those available in all of (i) the latest psoriasis susceptibility meta-analysis [22], (ii) all four of the severe disease GWAS summary statistics and (iii) BSTOP imputed genotyping data. In total, 6,461,913 variants were present across all datasets. Two different strategies were employed to construct psoriasis susceptibility PRS:
- PRS_GWS_—65 variants: Genome-wide significant (GWS) variants in the reanalysed susceptibility meta-analysis were assigned to LD-independent blocks [44], and the lead variants from each GWS block was incorporated into the PRS and weighted according to its effect size estimate.
- PRS_full_—513,461 variants: summary statistics from the reanalysed susceptibility meta-analysis (omitting Estonian Biobank, HUNT, UK Biobank and BSTOP cohorts) were analysed using the SBayesR framework to optimise weights [53], using the provided sparse reference LD matrix computed for 1.1 million common variants in 50,000 randomly selected, unrelated UK Biobank participants of European ancestry [45]. To aid model convergence, SNPs with lower sample size (> 3 s.d.) within the susceptibility meta-analysis were omitted, as were SNPs in high LD (R^2^ > 0.9, SNP with lowest susceptibility P-value was retained). For the MHC locus (chr6, 24.0–36.3 Mb), only the lead SNP (lowest P-value SNP from the LD panel: rs9380238) was included.
A sensitivity analysis was performed for both PRS_GWS_ and PRS_full_, constructed without MHC locus variants, giving a further two scores: PRS_GWS-noHLA_ and PRS_full-noHLA_. Additional versions of PRS_full_ and PRS_full-noHLA_ were constructed for comparative analysis of the UKB, BSTOP and Novartis secukinumab trial populations, further filtering input variants to those in the Novartis trials genotyping dataset (initial N = 5,607,229 variants; final N = 487,312 variants), denoted PRSfull and PRSfull-noHLA.
PRS comparison to psoriasis-only cohorts
PRS distributions within the UK Biobank cohort were compared to distributions of equivalent PRS in BSTOP (Biomarkers and Stratification To Optimise outcomes in Psoriasis) and Novartis clinical trials of secukinumab. Distributions were compared to the UK Biobank severe psoriasis population, any psoriasis population and full population, and differences in population means were compared using a two-sided t-test.
Epidemiological associations
Candidate epidemiological risk factors were tested for association with the severe disease phenotype in each of the four population-based cohorts (Estonian Biobank, FinnGen, HUNT, UK Biobank) using univariate (uncontrolled) logistic regression models. The risk factors selected comprised sex, age, age of psoriasis onset, smoking, alcohol intake, and various measures of adiposity (body mass index [BMI], weight, waist circumference). Epidemiological variables were defined in each cohort according to Additional file 1: Table S9. Quantitative variables were standardised to zero mean and unit variance within the psoriasis population. Effects were meta-analysed using a random-effects model (R library “metafor”).
Results
Across four population biobanks (Estonian biobank, FinnGen, HUNT and UK Biobank), we ascertained 44,904 individuals with a diagnosis of psoriasis from EHRs and health history questionnaires (Table 1). This represents an average of 3.7% of participants across the four biobank studies had a linked or self-reported psoriasis diagnosis (Additional file 1: Table S1). Within the psoriasis populations, an average of 21.7% of individuals met our criteria for severe psoriatic disease (evidence of hospitalisation due to psoriasis, taking systemic immunomodulating medication or phototherapy). We noted inter-study variation in this severity proportion with FinnGen exhibiting the highest proportion of severe cases (42.2%, Table 1). Table 1. Number of individuals with severe and non-severe psoriasis within each contributing population-based cohortTotal psoriasisSevere (%)Estonian Biobank14,1671639 (11.6)FinnGen12,7085365 (42.2)Trøndelag Health Study (HUNT)86031491 (17.3)UK Biobank94261243 (13.2)Total44,9049738 (21.7)
To identify genetic variation that influences an individual’s risk of developing severe psoriasis we undertook a case–control genome-wide association study in each of the four component studies. Cases were defined as individuals with a diagnosis of psoriasis and evidence of severe psoriasis (Methods) and controls as individuals with a diagnosis of psoriasis but with no evidence of severe disease. Association summary statistics for 6,544,261 variants tested in all four studies were combined through a fixed-effect inverse-variance weighted meta-analysis. The distribution of test statistics across genetic variants in each of the four GWAS and the resulting meta-analysis indicated that potential sources of systematic bias were adequately controlled (Additional file 1: Table S1, Additional file 2: Figure S1-S2).
Genetic variation at three genomic loci, 6p21.33, 5q33.1 and 5q33.3, were associated with severe psoriasis with evidence of association surpassing the genome-wide significance threshold (P < 5.0 × 10^−8^, Fig. 1). All are established psoriasis susceptibility loci and encompass the MHC region, and the candidate genes TNIP1 and IL12B respectively. Among variants included in the severity meta-analysis, the lead severity-associated variant in the MHC region (rs13203895) also has the lowest susceptibility p-value [22], and the lead severity variant at 5q33.1 (rs74817271) is in near perfect LD with the lead susceptibility variant (rs8177833; R^2^ = 0.99) [46]. These observations that the same genetic variation underlies susceptibility to and severity of psoriasis at both loci is consistent with the notion that there is a shared genetic component to psoriasis susceptibility and severity.Fig. 1. Manhattan plot for severe psoriasis GWAS meta-analysis of 4 population-based cohorts. Axes contain a point for each genetic variant (present in all datasets) ordered by chromosome and base position on the x-axis, with −log10(P-value) of association plotted on the y-axis. Red line indicates genome-wide significance threshold (P = 5 × 10^−8^)
To investigate the potential shared genetic architecture of psoriasis susceptibility and severity, we evaluated the genome-wide genetic correlation between the two traits using independent datasets, revealing evidence of a substantial shared genetic component (rG = 0.697, 95% CI 0.547–0.847). We next sought to establish whether the lead variants at 100 previously reported psoriasis risk loci are also associated with psoriasis severity. We identified 34 loci at which susceptibility alleles were nominally associated with disease severity (P < 0.05) with consistent effect size direction; eight of these surpassed a Bonferroni significance threshold (P < 5.0 × 10^−4^), including the three genome-wide significant loci. Established candidate genes at these loci include the immune-related genes IFNLR1, NFKBIZ, IL23A, IL31, STAT2 and NOS2 (Additional file 2: Figure S3). Across all 100 risk loci, we tested for a systematic relationship between susceptibility and severity effect sizes. This demonstrated a significant positive correlation between the reported effects on psoriasis risk and the observed effect on severe disease (b = 0.31; 95%CI 0.23–0.38; Fig. 2). This positive correlation was observed consistently across each of the four constituent studies, as well as in sensitivity analyses (Additional file 2: Figure S4-S5) and is consistent with a model under which individuals with higher genetic liability to psoriasis are more likely to develop manifestations of severe disease.Fig. 2. Correlation of psoriasis severity and susceptibility effects for SNPs representing 100 established susceptibility loci. x-axis: effect size (beta) for psoriasis susceptibility meta-analysis [22]; y-axis: effect size (beta) estimated for severe disease in the present study. Error bars represent standard errors. Black line represents Deming regression slope fit. SNPs with Bonferroni-corrected P-values < 0.05 are highlighted blue, labelled by implicated genes (from Dand et al. 2025)
To formally investigate the hypothesis that elevated cumulative genetic liability to psoriasis predisposes individuals to develop severe disease, we constructed psoriasis susceptibility PRSs and evaluated their association with psoriasis severity. PRS variant selection and weighting was undertaken using a recent large GWAS meta-analysis of psoriasis susceptibility [22], modified to exclude datasets that overlap with the current study (Additional file 1: Table S8). PRS derived from 65 genome-wide significant lead susceptibility variants (PRS_GWS_) and constructed using Bayesian multiple regression modelling (SBayesR) on genome-wide summary statistics (PRS_full_) were both significantly associated with disease severity, with effect estimates maximised using the PRS_full_ instrument (odds ratio [OR] 1.33, 95% CI 1.22–1.44, P = 1.01 × 10^−11^, Fig. 3). Given the substantial effect of the MHC on psoriasis risk and the association of the same alleles with disease severity, we confirmed that both PRSs remained positively associated with disease severity after excluding genetic variation from the MHC locus (OR_full-noHLA_: 1.31, 95% CI 1.23–1.40, P = 3.39 × 10^−16^, OR_GWS-noHLA_: 1.22, 95% CI 1.19–1.25, P = 7.60 × 10^−55^, Additional file 2: Figure S6).Fig. 3. Association of epidemiological and genetic risk factors with severe psoriasis. Effect estimates are derived from a meta-analysis of unadjusted logistic regression models comparing severe to non-severe psoriasis. y/n: effect size estimated for presence of exposure (“yes”) relative to absence (”no”); sd: effect size estimated per standard deviation change in continuous exposure within the psoriasis population; OR: Odds ratio. Effect sizes presented numerically as odds ratio (with 95% confidence intervals). 1 sd for age of onset is 18.4 years. 1 sd for BMI is 5.4 kg/m^2^. 1 sd for weight is 17.9 kg. 1 sd for waist circumference is 14.7 cm. Cohort-specific standard deviations are shown in Additional file 1: Table S10
To benchmark the magnitude of effect of these genetic instruments, we estimated marginal effects on severity of a series of epidemiological factors with established associations with psoriasis susceptibility and severity (Fig. 3, Additional file 2: Figure S6). The combined sample size of 44,904 individuals represents the largest study to date of the contribution of epidemiological factors to psoriasis severity. We replicate previous reports that earlier age of onset, smoking, and higher adiposity measures (BMI, weight and waist circumference) are associated with severe disease. We saw no significant association with sex in the meta-analysis (OR 1.07, 95% CI 0.93–1.23, P = 0.33). Contrary to some previous reports, frequent alcohol usage was not positively associated with severe disease in any of the studies and exhibited an inverse association within UK Biobank (OR_UKBiobank_: 0.73, 95% CI 0.62–0.85, P = 8.64 × 10^−5^).
Critically, the effect of an increase of one standard deviation of PRS_full_ on risk of severe disease is at least as strong as the effect of a binary or one standard deviation increase of any of the established epidemiological risk factors, including adiposity-related risk factors or smoking.
Given the comparative strength of association of genetic factors over established epidemiological risk factors on disease severity, we next evaluated the ability of different psoriasis susceptibility PRS thresholds to correctly classify individuals at risk of severe disease. We examined the trade-off between a PRS threshold for expedited clinical intervention and the extent to which individuals progressing to severe disease are correctly prioritised using a likelihood ratio for severe disease odds (Additional file 2: Figure S7) across the four different biobanks. As expected, there is variation between biobanks in the discriminatory ability of PRS at different thresholds. A PRS threshold at the 99th percentile of polygenic risk gives a likelihood ratio of between 1.37 and 2.79 (depending on the cohort studied) but suffers from lower sensitivity compared to a more inclusive PRS threshold. A threshold at the 95th percentile of genetic risk among the population with psoriasis offers a balance in sensitivity with an increased likelihood of developing severe disease of between 1.23 and 2.00 compared to the odds at the mean of the PRS distribution (Fig. 4, Additional file 2: Figure S8).Fig. 4. Distributions and performance of susceptibility PRS_full_ in predicting severe psoriasis cases within the cohort psoriasis population in each biobank study. Cut-offs (dashed lines) displayed for individuals within the top 5%, middle 90% and bottom 5% of the (within dataset) PRS distribution. Red line indicates PRS distribution of non-severe psoriasis population. Blue line indicates PRS distribution of severe psoriasis population. Severe disease odds: ratio of individuals with severe disease to individuals without severe disease. Likelihood ratio: ratio between the severe disease odds in each PRS group and the severe disease odds for all psoriasis cases
To further validate the correlation of the psoriasis susceptibility PRS with disease severity, we calculated susceptibility PRS for 4151 individuals with severe psoriasis from the BSTOP registry, a UK-based cohort of individuals ascertained from a severe psoriasis population, and a further 1461 individuals from Novartis clinical trials for secukinumab in psoriasis. The mean of the distribution of the psoriasis susceptibility PRS in these groups is higher than that observed among the 1243 severe psoriasis cases in UK Biobank (P_BSTOP_ = 1.12 × 10^−37^; P_Novartis_ = 2.72 × 10^−13^; Additional file 2: Figure S9, Additional file 1: Table S11). Furthermore, 15.3% of the individuals in the BSTOP cohort have a PRSfull in excess of a threshold defined as the 95th percentile of risk in the UK Biobank psoriasis population (a 3.06-fold enrichment), compared to 9.6% of severe psoriasis cases in UK Biobank (Additional file 1: Table S11). Similarly, 11.6% of the individuals in the Novartis secukinumab trials cohort have a PRSfull in excess of 95th percentile of risk in the UK Biobank psoriasis population (a 2.32-fold enrichment).
Discussion
The path of disease progression is a critical aspect of the psoriasis phenotype that encompasses both the severity of symptoms and the associated comorbidities, significantly affecting patients’ quality of life. Accurate prediction of who is at risk of severe disease has the potential to ensure timely and targeted interventions, to prevent long-term complications (such as psoriatic arthritis) and optimise outcomes. Our results demonstrate the potential of genetic variation in the prediction of severe psoriasis, specifically illustrating how knowledge of the genetic architecture of psoriasis susceptibility can be leveraged to predict severity.
We defined individuals with severe psoriasis based on the extent of clinical care they had received across four population biobanks. Many of the medical intervention proxies used to define the severe disease group may have previously been described as treatments for moderate-to-severe cases, but in accordance with latest consensus [35] we have used binary labelling for our two severity groups (severe/non-severe). This ascertainment approach has a limitation in that differing healthcare and treatment access across different countries, as well as the extent of data capture and linkage, could introduce subtle differences in the psoriasis phenotype being represented here as severe disease. Though we observe an overall rate of severe disease that is consistent with previous studies based on body surface area [2, 3], we do observe an elevated rate of severe disease based on our criteria in FinnGen, and this is likely to also be affected by the hospital-based recruitment strategy of this resource [37].
We identified three individual loci at which genetic variation was associated with psoriasis severity with genome-wide significant evidence. The association signals observed at 6p21.33, 5q33.1 and 5q33.3 are all previously established psoriasis susceptibility loci. Notably, there is also strong evidence of genetic correlation between psoriasis susceptibility and severity when considering either established psoriasis risk loci or common variation across the genome. This relationship between genetic susceptibility and severity is consistent with the liability threshold model of disease, which posits that the manifestation of a complex disease occurs when an individual’s cumulative genetic and environmental risk factors exceed a certain threshold. The results presented in this study are consistent with an extension to this model whereby, once the threshold for disease onset is surpassed, the extent of an individual’s genetic contribution to their disease liability further influences the severity of their disease. This framework enables disease severity to be conceptualised as a continuum, influenced by the extent of an individual’s genetic and environmental liability beyond the initial threshold necessary for disease manifestation.
Consistent with this model, a psoriasis susceptibility PRS is associated with disease severity. The magnitude of effect that is at least as large as established epidemiological factors that have an established association with severity [7, 8]. This includes BMI, weight and waist circumference and daily smoking, which are often cited as principal drivers of severe disease. We did not observe an association between daily alcohol intake and severe disease. There is conflicting evidence of the relationship between alcohol intake and severe psoriasis, with some studies showing increased intake in severe disease [47, 48] and others showing no evidence of increased intake [49, 50]. While cross-sectional studies have limited ability to determine causal relationships, we note also that our phenotype definition may impact our ability to accurately estimate the true association: alcohol is contraindicated with use of methotrexate, one of the systemic treatments used in our severe psoriasis definition.
A clear potential use of a prognostic psoriasis severity biomarker would be the identification of individuals at initial diagnosis that are at highest risk of progressing to severe disease, and therefore most likely to benefit from early onward referral or intervention. Our analysis of different PRS thresholds highlights the challenges of balancing sensitivity and specificity. Any strata of individuals at the high end of the distribution will result in imperfect sensitivity (Additional file 2: Figure S7). The predictive performance varied across cohorts, and the discriminatory ability was most limited in FinnGen, in which a higher proportion of individuals were defined as having severe disease (Additional file 1: Table S1).
While we explored the predictive ability of a genetic instrument on its own, we expect the discriminatory ability to be enhanced through the incorporation of epidemiological factors as well as typing at psoriasis presentation, which are not available in the datasets studied here. Fine-tuning the optimal proportion of high-risk individuals to monitor will require assessment of sensitivity and specificity alongside the economic impact of intervention. A further consideration will be the views of individuals living with psoriasis as to what level of risk is appropriate to trigger early interventions. Future studies, including prospective investigations, will be required to establish the utility of severity prediction and stratification using PRS alone or in combination with established epidemiological risk factors, and whether this improves upon the current paradigm of treating severe disease reactively or stratifying using epidemiological factors alone.
We note the potential impact on our findings of the misclassification of unaffected individuals as psoriasis cases, which would be expected to disproportionately occur in the non-severe group (since the additional evidence that we require to define a psoriasis case as severe also corroborates the psoriasis diagnosis). However, evidence suggests that non-specialist diagnosis of psoriasis tends to be accurate, with at least 90% of psoriasis primary care diagnosis codes corroborated by GPs [51], and that self-reported psoriasis is a good proxy for physician-diagnosed disease [52].
The time taken to progress to severe disease is an important component of disease progression not assessed in the current study and critical to understand when considering future clinical utility of any prognostic strategy. Such an analysis is challenging with current data resources as severity is a composite measure spanning many different sources (across different cohorts). Therefore, defining the point in time when initial diagnosis was made and when progression to severe disease is achieved is limited by the completeness of each individual’s EHR. More complete datasets will be required to investigate the relationship between disease risk burden and the rate of progression to severe disease.
Conclusions
In summary, our study illustrates that a psoriasis susceptibility PRS can predict disease severity, with effect sizes comparable to established epidemiological risk factors such as BMI and smoking. These insights pave the way for a more stratified and proactive healthcare approach, where early identification of high-risk individuals could lead to timely interventions, potentially mitigating the long-term impact of severe psoriasis and improving patient outcomes.
Supplementary Information
Additional file 1: Supplementary Tables S1-S12.Additional file 2: Supplementary Figures S1-S9 and Supplementary Methods.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Odorici G, Paganelli A, Peccerillo F, Serra J, Chester J, Kaleci S, et al. Moderate to severe psoriasis: a single-center analysis of gender prevalence. Italian Journal of Dermatology and Venereology. 2021 May;156(2).10.23736/S 2784-8671.18.06200-430648835 · doi ↗ · pubmed ↗
- 2Elective Care Transformation Programme. Transforming elective care service: Dermatology [Internet]. 2019 [cited 2024 Jul 6]. Available from: https://www.england.nhs.uk/wp-content/uploads/2019/01/dermatology-elective-care-handbook-v 1.pdf
- 3Ramessur R, Dand N, Langan SM, Saklatvala J, Fritzsche MC, Holland S, et al. Defining disease severity in atopic dermatitis and psoriasis for the application to biomarker research: an interdisciplinary perspective. British Journal of Dermatology. 2024 Feb 29;10.1093/bjd/ljae 080PMC 1118892638419411 · doi ↗ · pubmed ↗
- 4Machiela MJ, Chanock SJ. L Dlink: a web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants: Fig. 1. Bioinformatics. 2015 Nov 1;31(21):3555–7.10.1093/bioinformatics/btv 402PMC 462674726139635 · doi ↗ · pubmed ↗
- 5Lloyd-Jones, Zeng et al. Improved polygenic prediction by Bayesian multiple regression on summary statistics. Nat Commu. 2019. 10.1038/s 41467-019-12653-010.1038/s 41467-019-12653-0PMC 684172731704910 · doi ↗ · pubmed ↗