Pathogenesis of tubercular retinal vasculitis: An ongoing quest
Ikhwanuliman Putera, Rina La Distia Nora, Saskia M. Rombach, P. Martin van Hagen, Willem A. Dik

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
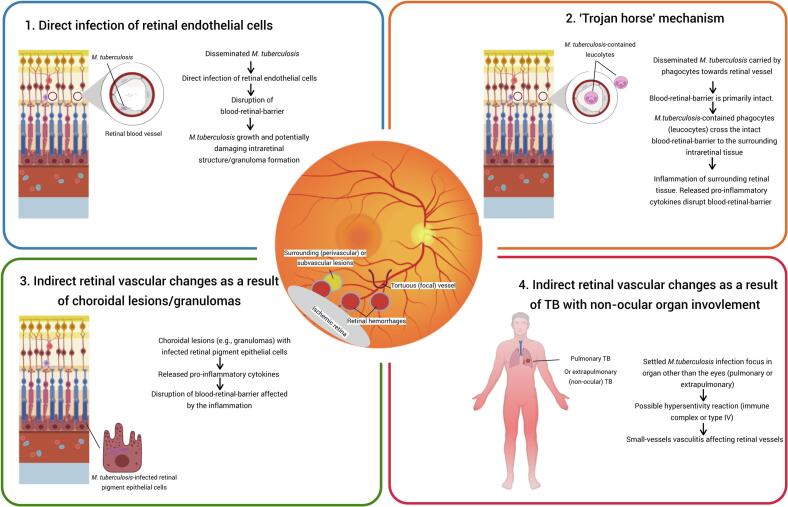 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · IgG4-Related and Inflammatory Diseases · Infectious Diseases and Tuberculosis
Retinal vasculitis is a well-recognized clinical feature that is consistently included in the diagnostic criteria for ocular tuberculosis (OTB), both in the original Gupta et al. classification [1] and the more recent criteria by the Standardized Uveitis Nomenclature (SUN) working group [2]. Notably, the SUN classification specifically highlights occlusive retinal vasculitis as a suggestive phenotype of OTB. We recently reported that that among the common ocular manifestations of uveitis associated with systemic TB, occlusive retinal vasculitis (15.7%) was the most frequent, followed by choroidal granuloma or tuberculoma (13.7%) [3].
Our understanding of the precise pathomechanism underlying retinal vasculitis, particularly tubercular retinal vasculitis (TRV), remains limited. In their initial efforts to classify uveitis, the SUN Working Group recognized retinal vasculitis as a term and clinical entity in need of further rigorous investigation [4]. They defined retinal vasculitis as “evidence of ocular inflammation and retinal vascular changes,” yet the exact nature of these vascular changes, and how to differentiate true inflammatory vasculitis from non-inflammatory vascular abnormalities, such as those seen in in diabetic retinopathy, has not been fully clarified. Retinal vasculitis can occur in a variety of contexts, including infectious uveitis and systemic diseases such as sarcoidosis or Behçet’s disease. Kaza et al. recently evaluated the clinical features of uveitis patients with visible retinal vasculitis, comparing those with evidence of active or latent tuberculosis (TB) to patients with non-TB-associated retinal vasculitis [5]. The study highlighted three features characteristic of TRV: subvascular lesions, focal vascular tortuosity, and occlusive characteristics [5]. However, further stratification based on treatment outcomes (with and without anti-tubercular treatment (ATT)) were not evaluated [5].
A study utilizing a zebrafish model elegantly demonstrated that systemic injection of mycobacteria can induce ocular inflammation resembling OTB, characterized by choroidal lesions and/or retinal vasculitis [6]. The study also observed that retinal vasculitis may occur even in the presence of an intact blood-retinal barrier (BRB). However, it remained unclear whether the mycobacteria crossed the BRB while contained within phagocytic cells or by another mechanism [6].
It can be speculated that the development of TRV may involve one or a combination of several pathomechanisms, as illustrated in Fig. 1. One potential mechanism is supported by our recent findings demonstrating that retinal endothelial cells (RECs) are permissive to Mycobacterium tuberculosis (Mtb) infection [7]. In patients with active TB, Mtb bacteremia has been estimated to occur in approximately 13.5% of adults, with an even higher prevalence of 15.5% among HIV-positive individuals [8]. This bacteremia may allow direct interaction between circulating Mtb and RECs. In our recent in vitro study Mtb infection of REC led to the activation of interferon signalling pathways [7], a response that resembles, at least in part, the innate immune activation observed in Mtb-infected retinal pigment epithelial (RPE) cells [7].Fig. 1. Hypothetical mechanisms involved in the development of tubercular retinal vasculitis. (Created with BioRender.com).
A second proposed mechanism underlying TRV is the “Trojan horse” pathway, wherein Mtb-infected phagocytes cross the BRB without initially disrupting its structural integrity. This mechanism, along with the direct infection of REC, has been implicated in the traversal of mycobacteria across the blood–brain barrier in zebrafish models, providing insight into the pathogenesis of TB meningitis and central nervous system (CNS) TB vasculitis [9]. Both direct REC infection and the “Trojan horse” pathway depend on the ESX-1 secretion system of the mycobacteria [9]. Importantly, the “Trojan horse” route may shield Mtb from direct interaction with RECs, while offering a protected intracellular niche within phagocytes that may favor bacterial survival [9]. Furthermore, histopathological studies of TRV by Basu et al. revealed the presence of intraretinal granulomas adjacent to vessel walls [10]. However, whether TRV primarily results from direct REC infection or from the “Trojan horse” route remains unclear.
An alternative mechanism to those described above is that TRV may arise secondary from choroidal lesions or infection of RPE cells lining the outer BRB, rather than involving the inner BRB. In this scenario, the clinically observed TRV could primarily reflect indirect inflammatory changes rather than direct infection of RECs or other intraretinal structures. A comparable concept has been proposed in vasculitis in birdshot retinochoroiditis, where retinal vascular changes are thought to be secondary to choroidal inflammation. The advent of indocyanine green angiography (ICGA) was pivotal in reshaping this understanding, revealing early hypofluorescent dark dots that were localized in the choroid, often before the characteristic birdshot lesions were visible with fundus examination [11]. Prior to the use of ICGA, retinal vasculitis was commonly noted ‘early’ in the disease course and was interpreted as a primary retinal manifestation. This shift in perspective might suggest that (a subset of) patients with TRV might similarly represent secondary retinal involvement driven by choroidal inflammation. Nevertheless, this mechanism may not explain all cases, as retinal vasculitis has also been observed to occur independently of choroidal inflammation [3].
A final proposed mechanism is that TRV may result from Mtb infection at a distant site. The association of small-vessel vasculitis with active TB elsewhere in the body has been suggested to represent a contributing factor in other vasculitic conditions, such as cutaneous leukocytoclastic vasculitis (CLV) [12]. Notably, vasculitic skin lesions in CLV have been reported to respond favorably to ATT [12]. Although the exact mechanism remains elusive, it is hypothesized this involves a hypersensitivity reaction to Mtb antigens [12].
In summary, TRV is a clinical entity that, in some patients, may represent a true manifestation of TB disease. This underscores the need for further investigation into its underlying mechanisms and the correlation with specific clinical features. Given the suboptimal diagnostic sensitivity of current molecular tests, such as polymerase chain reaction, for intraocular detection of Mtb, the development of alternative biomarkers, such as immune response-derived signatures indicative of active disease, must account for the distinct pathomechanisms that underlie TRV [13]. As research advances, a more refined understanding of OTB/TRV may help to identify which patients truly require ATT, even in the absence of direct microbiological identification of Mtb within ocular tissues, which remains a significant limitation in the current clinical practice.
Funding sources
IP is supported by Indonesia Endowment Fund for Education (Lembaga Pengelola Dana Pendidikan–LPDP, no. 0004535/MED/D/19/lpdp2021). The funding source had no involvement in the collection, analysis, interpretation, writing of the report, or the decision to submit the article for publication.
Declaration of generative AI in scientific writing
During the preparation of this work, the author(s) used ChatGPT (OpenAI, San Francisco, CA) for assistance in proofreading and editing the manuscript for grammar correction. None of the substantive content of this manuscript or its figure was generated through AI. The author(s) reviewed and edited the content as needed and take(s) full responsibility for the final manuscript.
Ethical statement
Ethical approval is not necessary for the present perspective manuscript/study. No patient-related data or animal usage in the preparation of this manuscript.
CRediT authorship contribution statement
Ikhwanuliman Putera: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing. Rina La Distia Nora: Formal analysis, Investigation, Supervision, Validation, Writing – review & editing. Saskia M. Rombach: Formal analysis, Investigation, Supervision, Validation, Writing – review & editing. P. Martin van Hagen: . Willem A. Dik: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gupta A.Sharma A.Bansal R.Sharma K.Classification of intraocular tuberculosis Ocul Immunol Inflamm 2320157132531436110.3109/09273948.2014.967358 · doi ↗ · pubmed ↗
- 2Standardization of Uveitis Nomenclature Working Group Classification criteria for tubercular uveitis Am J Ophthalmol 22820211421513384501410.1016/j.ajo.2021.03.040PMC 8634785 · doi ↗ · pubmed ↗
- 3Putera I.Rothova A.La Distia N.R.Comparison of uveitis manifestations in patients with active systemic tuberculosis and those with positive interferon-gamma release assay without active disease Eye (Lond)392025177217804008962510.1038/s 41433-025-03751-z PMC 12130239 · doi ↗ · pubmed ↗
- 4Jabs D.A.Nussenblatt R.B.Rosenbaum J.T.Standardization of uveitis nomenclature working G. Standardization of uveitis nomenclature for reporting clinical data. results of the first International Workshop Am J Ophthalmol 14020055095161619611710.1016/j.ajo.2005.03.057PMC 8935739 · doi ↗ · pubmed ↗
- 5Kaza H.Tyagi M.Pathengay A.Basu S.Clinical predictors of tubercular retinal vasculitis in a high-endemic country Retina 4120214384443238384110.1097/IAE.0000000000002829 · doi ↗ · pubmed ↗
- 6Takaki K.Ramakrishnan L.Basu S.A zebrafish model for ocular tuberculosis P Lo S One 132018 e 019498210.1371/journal.pone.0194982 PMC 587100329584775 · doi ↗ · pubmed ↗
- 7Putera I.Swagemakers S.M.A.Nagtzaam N.M.A.van Holten-Neelen C.La Distia N.R.de Steenwinkel J.E.M.Mycobacterium tuberculosis infection of retinal endothelial cells induces interferon signaling activation: insights into tubercular retinal vasculitis Invest Ophthalmol Vis Sci 6620254810.1167/iovs.66.9.48PMC 1227907240668059 · doi ↗ · pubmed ↗
- 8Pavlinac P.B.Lokken E.M.Walson J.L.Richardson B.A.Crump J.A.John-Stewart G.C.Mycobacterium tuberculosis bacteremia in adults and children: a systematic review and meta-analysis Int J Tuberc Lung Dis 2020168959022728764110.5588/ijtld.15.0773 PMC 5827940 · doi ↗ · pubmed ↗