Eosinophilic annular erythema: report of four cases in adults and update of the literature
Emilia N. Cohen Sabban, Horacio A. Cabo, Rosario Peralta, Gabriel Salerni, Fernando Stengel, Yolanda Gilaberte, Esteban Maronna

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
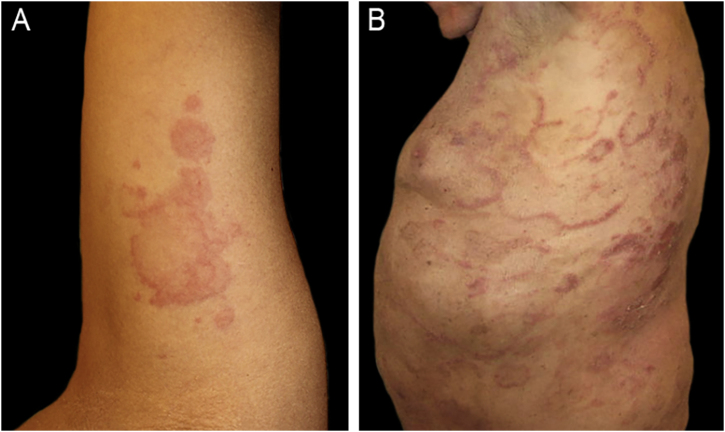 Figure 1
Figure 1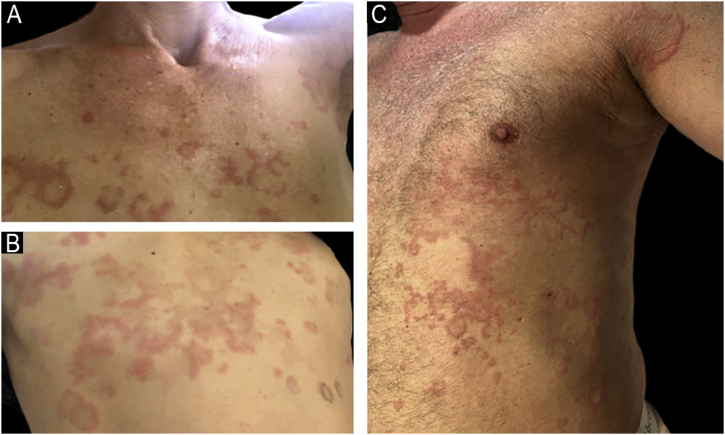 Figure 2
Figure 2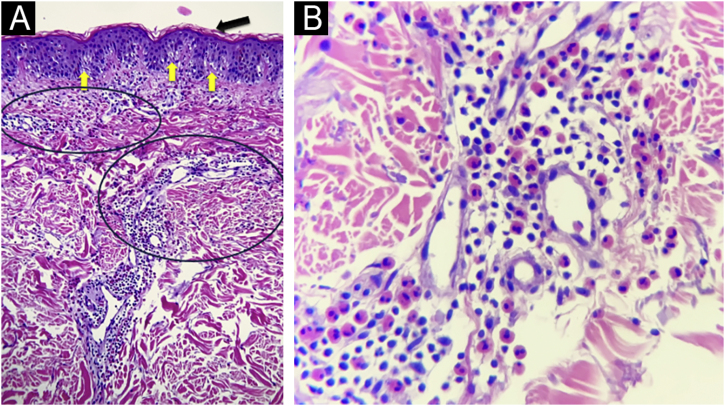 Figure 3
Figure 3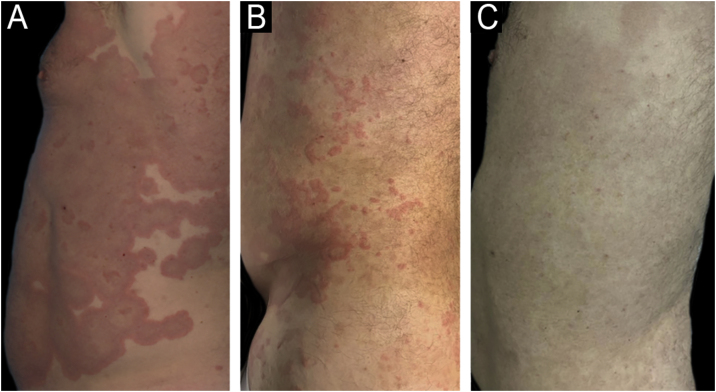 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Oral and Craniofacial Lesions · Eosinophilic Esophagitis
Dear Editor,
Eosinophilic annular erythema (EAE) is an uncommon, usually self-limited dermatosis, first described in infancy by Peterson in 1981.1 The first adult case was reported in 2000 by Kahofer et al.2 EAE belongs to both eosinophil-associated dermatoses and figurate erythemas as well.
The authors report four adult cases of EAE (Table 1) that were histologically proven and assessed at the same institution between 2017 and 2024. Two women and two men, aged 39 to 65 years (median age 53), presented clinically with lesions involving the trunk and extremities (Fig. 1, Fig. 2). Intense itching was the main symptom. No vesiculation, scaling, or central punctum was present. Only Case 2 resolved with post-inflammatory hyperpigmentation. Laboratory tests, including complete blood count, C-reactive protein, erythrocyte sedimentation rate, VDRL, fasting blood sugar, renal and liver function, and direct immunofluorescence, were all normal or negative. On histological examination, all cases revealed similar findings, showing no epidermal involvement. The dermis showed an intense dermal edema, vasodilation, and a moderate mixed infiltrate with abundant eosinophils in a perivascular and interstitial distribution at superficial and deep levels. No flame figures were seen (Fig. 3).Table 1. Clinical data.Table 1. Case nºAge yrs/ GenderConcomitant diseaseType of lesionsLocationHistologyBlood testTreatmentDurationRelapse139 FemaleNoneUrticarial papules and erythematous annular plaquesTrunk and extremitiesDermal edema. Superficial and deep moderate perivascular eosinophilic infiltrate.NormalPrednisone + anti histamines with good response2 yearsYes261 MaleNoneUrticarial papules and annular plaquesTrunk and extremitiesMild spongiosis.Perivascular and interstitial mixed infiltrate with numerous eosinophilsEosinophilia IgE 400 IU/mLPrednisone and hydroxychloroquine were ineffective. Cyclosporine (3.5 mg/Kg/d) with good response. Post inflammatory hyperpigmentation6 monthsNo367 MaleChronic eczemaErythematous macules and plaquesTrunk and extremitiesSpongiosis, dermal edema. Moderate mixed perivascular infiltrate with numerous eosinophilsNormalPrednisone with good response2 monthsNoEpilepsyHypothyroidism445 FemaleAtopic dermatitisAnnular erythematous plaquesTrunk and abdomenModerate perivascular and interstitial mixed infiltrate with numerous eosinophilsNormalPrednisone and antihistaminesAfter 6-months still continuesYesAllergic rhinitisANA+Fig. 1(A) Case 1: Annular plaques with erythematous borders on the right armpit and upper extremity. (B) Case 3: Erythematous macules and plaques with the typical figurate erythema aspect, on the trunk.Fig. 1. Fig. 2(A and B) Case 4: Annular plaques with central healing and erythematous borders on the trunk. (C) Case 2: Urticarial papules and erythematous plaques on the trunk and extremities.Fig. 2. Fig. 3(A) Hematoxilyn & eosin, 100×. Epidermis with orthokeratosis (black arrow) and mild spongiosis (yellow arrows). Dermis with moderate inflammatory infiltrates of perivascular and interstitial disposition. (circles) (B) Hematoxilyn & eosin, 400 ×. A close up of the dermal infiltrates on a perivascular and interstitial disposition made up of lymphocytes and numerous eosinophils.Fig. 3
Case 1
A healthy 39-year-old woman with no relevant past medical history presented with a five-month history of an intermittent skin eruption consisting of urticarial papules and annular plaques with erythematous borders, that enlarged centrifugally and each one disappeared without a trace, lasting up to 48 hours. There was no history of arthropod bites, exposure to pets, recent travel, or use of any medications. A skin biopsy confirmed the diagnosis of EAE. The patient received topical and oral steroids – prednisone 40 mg/od, plus a combination of three antihistamines. Prednisone was slowly tapered down to 4 mg/d over a month. The skin lesions faded gradually, and the pruritus score decreased from 10/10 to 6/10. Prednisone was stopped upon achieving complete remission. She suffered similar outbreaks over two years and finally went into remission.
Case 2
A 61-year-old man with no previous medical history presented with an acute, recurrent, intensely itchy skin rash on the trunk and extremities that affected his quality of life. Physical examination revealed widespread involvement sparing the face, genitalia, oral mucosa, scalp, palms, and soles. Individual lesions had become confluent, developing into large erythematous polycyclic configurations. Laboratory tests revealed eosinophilia of 18%, and an elevated IgE 400 Iu/mL. The patient failed to respond to topical corticosteroids and high-dose antihistamines. Topical and oral prednisone ‒ 40 mg/day followed, with symptomatic relief but incomplete control of lesions. Hydroxychloroquine 200 mg/day was subsequently added with similar results. Finally, oral cyclosporine (3.5 mg/k/day) monotherapy was started, and after two weeks, the majority of the lesions resolved, with significant central post-inflammatory hyperpigmentation. Complete remission of skin lesions was achieved at 4-weeks (Fig. 4), and cyclosporine was gradually tapered and discontinued six months after initiation. At one-year follow-up, the patient has remained relapse-free.Fig. 4. Case 2 Pre- and post-treatment. (A) Baseline (cyclosporine 3.5 mg/k/day). (B) 9 days of treatment. (C) Complete remission at 4-weeks of treatment.Fig. 4
Case 3
A 67-year-old man suffering from chronic eczema for many years presented with a pruritic eruption of erythematous macules and plaques. He had been receiving valproic acid for epilepsy for the past 20-years, lipid-lowering therapy for the past 7-years, and levothyroxine for hypothyroidism. Skin biopsy confirmed the diagnosis. The patient was started on prednisone ‒ 40 mg/day over 40-days with a good response, tapering to 40/20 mg alternate days, then 20 mg/d over two more months, until he was free of lesions.
Case 4
A 45-year-old healthy woman presented with a 4-months history of an intermittent pruritic rash on her trunk and abdomen. As a possible trigger factor, the patient mentioned that the skin rash started after a bee sting during her holidays. There was no history of exposure to pets or use of any medications. Except for her atopic dermatitis, recurrent allergic rhinitis, and a positive Antinuclear Antibody (ANA) at a 1:320 dilution with a fine nuclear speckled pattern (AC-4), her personal medical history and family history were otherwise normal. The patient received oral prednisone 8 mg od and a combination of two second-generation antihistamines as maintenance therapy. This combination achieved pruritus control with lesional improvement. However, relapses occurred upon withdrawal of therapy. The authors have failed to achieve disease control to date.
EAE is an acute, benign, and intensely pruritic dermatosis characterized by recurrent annular, arciform, figurate, or polycyclic erythematous and edematous plaques with a centrifugal growth pattern. The lesions usually arise on the trunk and extremities and most individual lesions tend to disappear within 36–48 hours. The absence of vesiculation and residual scaling distinguishes it from other conditions. At least 82 adult cases have been reported in the literature, including atypical variants with vesiculobullous features or palmoplantar localization.3, 4 Although self-limited, relapses are characteristic of the disease. Regarding the two patients who experienced several relapses during a 2-year follow-up, the authors found no changes in their laboratory tests or other possible explanations for this course.
The pathogenesis remains unclear. Current hypotheses suggest an Interleukin-5 (IL-5) mediated eosinophil recruitment in response to unknown triggers, possibly allergic stimulus or insect bites, as suspected in Case 4. Although eosinophilia is occasionally reported, it is not a common finding.5
Histopathology typically shows dermal involvement with a perivascular and interstitial infiltrate with numerous eosinophils and some lymphocytes without granulomas or vasculitis. Flame figures, characteristic of wells syndrome (WS), are generally absent. Pigmentary incontinence and basal melanosis may lead to post-inflammatory hyperpigmentation, as seen in Case 2.5
Differential diagnoses (Table 2) include other annular dermatoses, such as generalized granuloma annulare, erythema annulare centrifugum, subacute cutaneous lupus erythematosus, erythema multiforme, erythema gyratum repens, and erythema migrans. Eosinophilic disorders to consider include WS, bullous pemphigoid, parasitic infections, arthropod bites, and eosinophilic vasculitis.1Table 2. Differential diagnoses of EAE.Table 2. DermatosisClinical descriptionHistologic featuresGeneralized Granuloma AnnulareMay occur in infancy and adulthood. Asymptomatic or occasionally pruritic, non-scaly erythematous papules and plaques with different morphology, annular, arciform, polycyclic. The etiology is unclear. It may be associated with Diabetes mellitus, thyroid diseases, infections (hepatitis B/C virus, HIV), malignancies, etc.Pattern of either palisading granuloma with focal degeneration of collagen bundles surrounded by lymphocytes, histiocytes, and giant cells, or interstitial distribution of the infiltrate, in the upper and mid-dermis. Abundant mucin depositionErythema Annulare CentrifugumUsually begins in middle age with erythematous papules and plaques that enlarge centrifugally to form rings and arcs with central hypopigmentation. On the inner part of the advancing edge, a fine collarette of scales is described. Each lesion lasts days to months. Face, trunk, extremities. Occasionally, it accompanies an underlying disease (infections, malignancies, etc.)The epidermis often shows areas of mild spongiosis surmounted by focal parakeratosis. Dense perivascular lymphohistiocytic infiltrate in the superficial and deep dermis without eosinophilsSubacute lupusUsually in adults. It presents with erythematous papulosquamous or annular plaques on photo-exposed areas. ANA + and Ro+Interface dermatitis, edema, perivascular, peri-adnexal lymphocytic infiltrate. Positive Direct Immunofluorescence (DIF)Erythema gyratum repensPersistent concentric, arcuate, or polycyclic, scaling plaques, almost always associated with an underlying malignant neoplasm of the breast, lung, stomach, bladder, prostate.Histologically, it shows both, epidermal (hyper and parakeratosis, focal spongiosis), and a dermal component composed by mild perivascular mononuclear infiltrateTinea corporisAnnular erythematous plaques with peripheral leading scale and central healingDirect potassium hydroxide microscopy (KOH) and culture lead to the diagnoses of superficial fungal infectionWells syndromeClinically, it´s characterized by prodromal burning, painful edema, and peripheral induration. The classical description is a cellulitis-like plaque, but then, its clinical polymorphism with erythematous annular and figurate lesions have been described. The lesions usually resolved within a few weeks leaving a slate-grey morphea-like induration. The recurrent course and spontaneous healing after months or years, are features that both entities share.Prominent papillary dermal edema, and interstitial infiltrate mainly eosinophils, are diffusely distributed, and can be localized at the superficial, mid and/or deep dermis and extending into the subcutis. Typical flame figures consisting of degenerated collagen fibers, due to deposits of the major basic protein of the eosinophil.Erythema Gyratum AtrophicansOccurs in newborns as a generalized eruption of erythematous plaques evolving to atrophy and hypopigmentation.Epidermal atrophy, dermal edema, and a mononuclear cell infiltrate are present. DIF reveals granular deposits of IgG, C3, and C4 at the dermoepidermal junction and around the superficial capillariesErythema MultiformeMay occur at any age presenting as symmetrically distributed papules, annular plaques and target-like lesions typically fixed for a minimum of seven days.Interface dermatitis characterized by epidermal basal cell damage, which may be manifested by cell death and/or basal vacuolar change, and a lichenoid distribution of inflammatory cells obscuring the dermoepidermal interfaceErythema Chronicum MigransThere is often a history of an arthropod bite and a resulting central punctum. The non-scaly, usually unique plaque, expands centrifugally as a blue-red urticarial ring over several weeks or months.Mononuclear peri-adnexal and perivascular dermal infiltrate is present.UrticariaEdematous papules that rapidly became large and irregular plaques intensely pruritic. Each lesion lasts no more than 6 -hs and they arise on different locations.Edema and sparse perivascular inflammatory infiltrate in the upper dermisAnnular Erythema of infancyAnnular and figurate pruritic lesions with early age of onset (under 1-year of age) and spontaneous resolution on the trunk and extremities. No prodromes. Sparing the face, genitalia, palms and soles.Perivascular mononuclear infiltrate with few eosinophils; negative DIF; lack of mucin, “flame figures”, vasculitis or granulomasNo Eosinophilia in the majority of cases.Recurrent, chronic, with outbreaks.
There is an ongoing debate regarding whether EAE is a separate entity or a variant of WS. Some authors propose that EAE represents a chronic, treatment-resistant form of WS with higher relapse rates. However, the absence of flame figures, lack of blood eosinophilia, and distinct clinical features support the classification of EAE as an independent condition.6
Associations between EAE and systemic diseases such as autoimmune thyroiditis (Case 3), diabetes mellitus, and systemic lupus erythematosus have been described. El-Khalawany et al. observed that managing systemic comorbidities may contribute to longer remission periods and reduced recurrence.7
Treatment should be individualized based on symptom severity, lesion extent, and associated conditions. Therapeutic options include topical and systemic corticosteroids (0.5–1 mg/kg/day), oral minocycline or doxycycline, hydroxychloroquine (200–400 mg/day), dapsone (50–100 mg/day), low-dose cyclosporine, methotrexate, and antihistamines, alone or in combination. Clinical improvement usually occurred within 2–6 weeks. However, relapses after drug discontinuation are frequent. One case in the literature reported the successful use of narrowband UVB in a corticosteroid and hydroxychloroquine-resistant patient, achieving long-term remission.8, 9
Recent reports have also described successful treatment of refractory cases with biologics such as dupilumab, mepolizumab, benralizumab, and the JAK inhibitor baricitinib, though these remain off-label and are based on isolated cases.10
In conclusion, the authors propose that EAE is a distinct clinical entity, characterized by annular, pruritic, polycyclic plaques. This presentation differs from the more edematous, cellulitis-like lesions of WS, which commonly exhibit peripheral eosinophilia and flame figures on histology. Skin biopsy remains essential for diagnosis. Although therapeutic responses are usually favorable, relapses are common. Further studies are needed to clarify its pathogenesis, classification, and optimal long-term management.
ORCID ID
Emilia N. Cohen Sabban: 0000-0002-5941-7439
Horacio A. Cabo: 0000-0002-8563-7013
Gabriel Salerni: 0000-0001-6386-4402
Fernando Stengel: 0009-0000-7681-2548
Yolanda Gilaberte: 0000-0001-8034-3617
Esteban Maronna: 0000-0002-5144-896X
Financial support
None declared.
Authors' contributions
Emilia N. Cohen Sabban: Data collection, analysis and interpretation; preparation and writing of the manuscript; approval of the final version of the manuscript.
Horacio A. Cabo: Intellectual participation in propaedeutic and/or therapeutic management of studied cases and approval of the final version of the manuscript.
Rosario Peralta: Manuscript critical review, critical literature review and approval of the final version of the manuscript.
Gabriel Salerni: Effective participation in research orientation and approval of the final version of the manuscript.
Fernando Stengel: Critical literature review and approval of the final version of the manuscript.
Yolanda Gilaberte: Preparation and writing of the manuscript and approval of the final version of the manuscript.
Esteban Maronna: Data collection, analysis and interpretation and approval of the final version of the manuscript.
Research data availability
The entire dataset supporting the results of this study was published in this article.
Conflicts of interest
None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Peterson A.O.Jr Jarratt M.Annular erythema of infancy Arch Dermatol.11719811451487212726 · pubmed ↗
- 2Kahofer P.Grabmaier E.Aberer E.Treatment of eosinophilic annular erythema with chloroquine Acta Derm Venereol.80200070711072185010.1080/000155500750012685 · doi ↗ · pubmed ↗
- 3Koh Y.P.Tey H.L.Bullous eosinophilic annular erythema Dermatol Online J.20212710.5070/D 32755362334118823 · doi ↗ · pubmed ↗
- 4Lee H.S.Yang J.Y.Kim Y.C.Eosinophilic annular erythema localized to the palms and the soles Ann Dermatol.2820167697712790428010.5021/ad.2016.28.6.769PMC 5125962 · doi ↗ · pubmed ↗
- 5Nakazato S.Fujita Y.Shinkuma S.Nomura T.Shimizu H.Eosinophilic annular erythema is clinically characterized by central pigmentation reflecting basal melanosis: a clinicopathological study of 10 cases J Eur Acad Dermatol Venereol.312017191619232854360510.1111/jdv.14350 · doi ↗ · pubmed ↗
- 6Heras M.O.Muñoz N.P.Sancho M.I.Millet P.U.Eosinophilic annular erythema in adults: report of two cases and review of the literature An Bras Dermatol.92201765682926745010.1590/abd 1806-4841.20176373 PMC 5726681 · doi ↗ · pubmed ↗
- 7El-Khalawany M.Al-Mutairi N.Sultan M.Shaaban D.Eosinophilic annular erythema is a peculiar subtype in the spectrum of Wells syndrome: a multicentre long-term follow-up study J Eur Acad Dermatol Venereol.2720139739792273188610.1111/j.1468-3083.2012.04616.x · doi ↗ · pubmed ↗
- 8Chastagner M.Shourik J.Jachiet M.Battistella M.Lefevre G.Gibier J.B.Treatment of eosinophilic annular erythema: retrospective multicenter study and literature review Ann Dermatol Venereol.14920221231273471602810.1016/j.annder.2021.07.007 · doi ↗ · pubmed ↗