Risk of major adverse cardiovascular events with aripiprazole versus olanzapine, quetiapine, and risperidone in severe mental illness: a target trial emulation
Alvin Richards-Belle, Naomi Launders, Sarah Hardoon, Kenneth K. C. Man, Neil M. Davies, Elvira Bramon, Joseph F. Hayes, David P. J. Osborn

TL;DR
This study compares the risk of major cardiovascular events among patients with severe mental illness starting different antipsychotics, finding similar long-term risks but higher risk with continued risperidone use.
Contribution
The study provides real-world evidence comparing cardiovascular risks of aripiprazole versus other antipsychotics in patients with severe mental illness.
Findings
Patients initiating aripiprazole had similar five-year MACE risk as those starting olanzapine, quetiapine, and risperidone.
Continued use of risperidone was associated with higher MACE risk compared to aripiprazole.
Antipsychotic selection does not significantly impact long-term cardiovascular event risk for most patients.
Abstract
Initiating aripiprazole as antipsychotic monotherapy rather than olanzapine, quetiapine, or risperidone, might prevent/delay major adverse cardiovascular events (MACEs) over the long-term in people diagnosed with severe mental illness. Using Clinical Practice Research Datalink data, we emulated a trial of aripiprazole versus olanzapine, quetiapine, and risperidone in 20,404 patients 2005–2014. Primary outcome was five-year MACE risk (composite of hospitalisation for acute myocardial infarction or stroke and cardiovascular death). Here we show that patients initiating aripiprazole had a similar five-year MACE risk as those initiating olanzapine (risk ratio: 1.03, 95% CI, 0.78-1.32), quetiapine (1.02, 95% CI, 0.72-1.32), and risperidone (0.88, 95% CI, 0.67-1.17). Risk was lower among patients initiating and continuing aripiprazole versus risperidone (0.58, 95% CI, 0.39-0.84). For patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
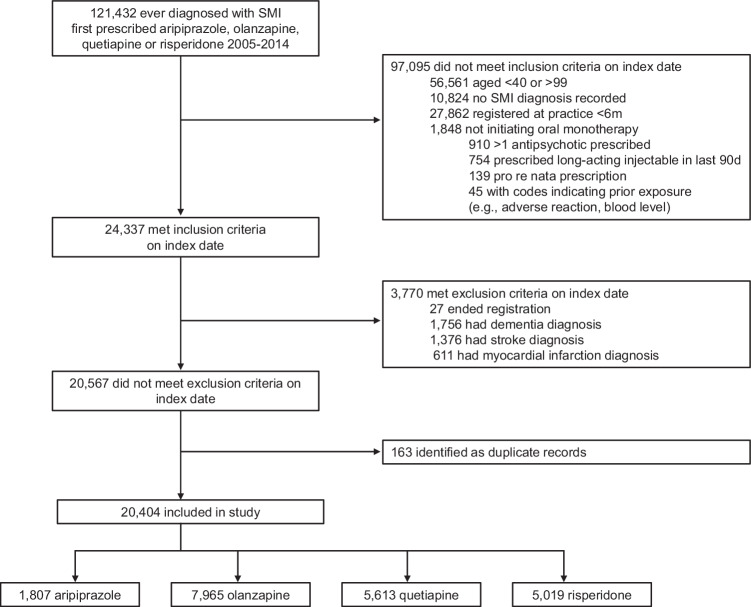 Figure 1
Figure 1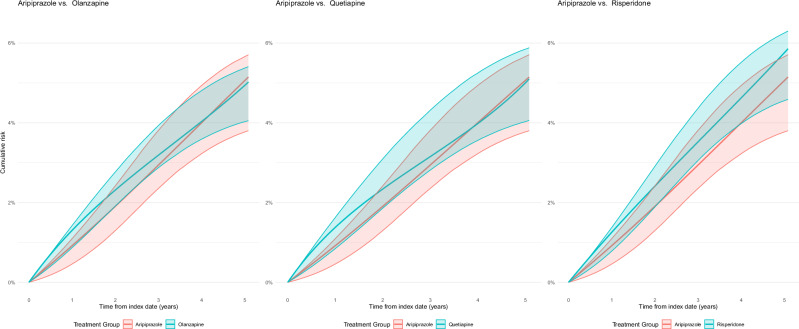 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSchizophrenia research and treatment · Healthcare Decision-Making and Restraints · Electroconvulsive Therapy Studies