Analgesic Effect of Rectus Sheath Block Versus Local Infiltration Analgesia in Laparoscopic Sleeve Gastrectomy: A Randomized Controlled Trial
Artid Samerchua, Kanokkan Tepmalai, Bandhuphat Chakrabandhu, Kittitorn Supphapipat, Panuwat Lapisatepun, Prangmalee Leurcharusmee, Kullaphun Prapussarakul, Thidarut Jinadech, Kotchakorn Jungsakulrujirek, Mullika Wanvoharn

TL;DR
This study compared two pain management techniques after a common weight-loss surgery and found that one method reduced pain in the early recovery period.
Contribution
The study demonstrates that rectus sheath block provides better early postoperative analgesia than local infiltration analgesia after laparoscopic sleeve gastrectomy.
Findings
Rectus sheath block reduced intraoperative fentanyl use and early postoperative pain scores compared to local infiltration analgesia.
Pain during movement was significantly lower with rectus sheath block at multiple time points post-surgery.
Postoperative morphine consumption and recovery metrics were similar between the two groups.
Abstract
Rectus sheath block (RSB) provides reliable anesthesia to the anteromedial abdominal wall and may offer effective pain control following laparoscopic sleeve gastrectomy (LSG). This study aimed to compare the efficacy of RSB versus local infiltration analgesia (LIA), hypothesizing that RSB would provide superior pain relief. In this randomized controlled trial, patients with obesity undergoing LSG received either bilateral ultrasound-guided RSB performed by an anesthesiologist or LIA administered by a surgeon, following anesthesia induction. The primary outcome was intraoperative fentanyl consumption. Secondary outcomes included postoperative pain scores [Numeric Rating Scale (NRS), 0–10], cumulative morphine consumption, and recovery metrics over 48 h. Sixty-nine patients were analyzed (RSB: 35; LIA: 34). Intraoperative fentanyl use was lower with RSB (median difference: − 25 mcg; 95%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
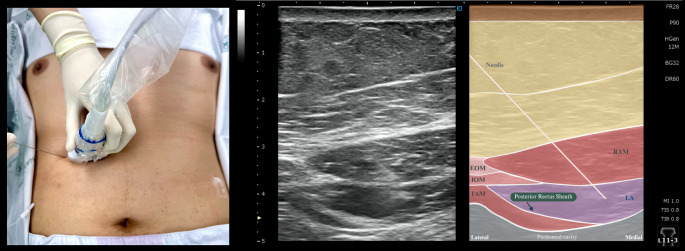 Figure 1
Figure 1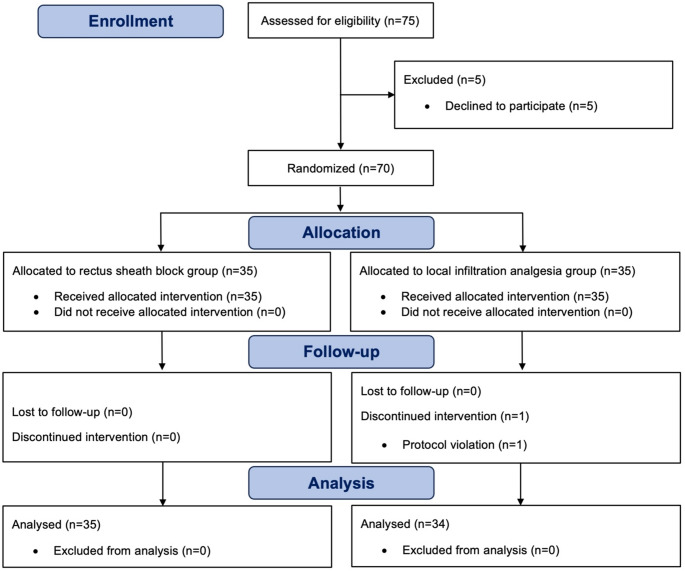 Figure 2
Figure 2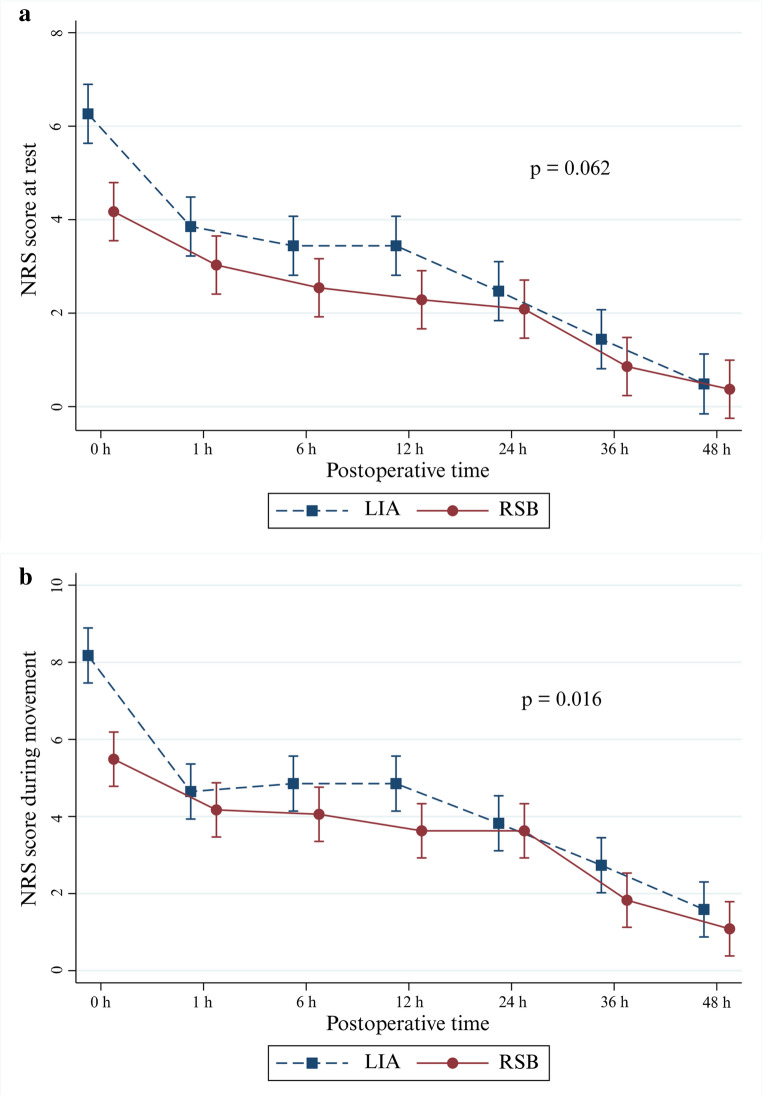 Figure 3
Figure 3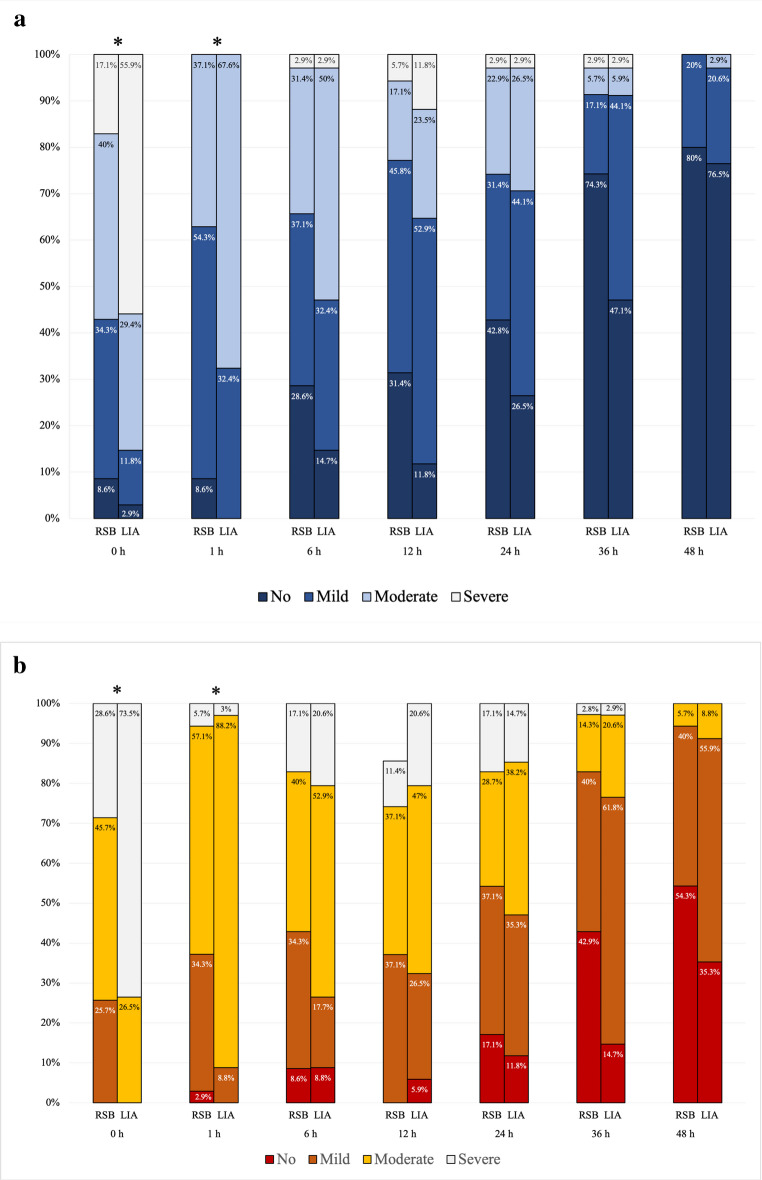 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Bariatric Surgery and Outcomes · Enhanced Recovery After Surgery