Retention and Engagement in Culturally Adapted Digital Mental Health Interventions: Systematic Review of Dropout, Attrition, and Adherence in Non-Western, Educated, Industrialized, Rich, Democratic Settings
Tanya Tandon, Rajashree Biswas, Quentin Meteier, Karl Daher, Omar Abou Khaled, Björn Meyer, Thomas Berger, Rashmi Gupta, Chantal Martin Soelch

TL;DR
This paper reviews how culturally adapted digital mental health interventions affect user engagement in non-Western settings.
Contribution
It identifies that deep cultural adaptations improve engagement and outcomes in non-WEIRD populations.
Findings
Culturally resonant adaptations reduce dropout and increase adherence in digital mental health interventions.
Hybrid human-digital models show better engagement and clinical outcomes like reduced depression and anxiety.
Most studies were of good quality but lacked representative sampling and objective metrics.
Abstract
Digital mental health interventions (DMHIs) offer scalable and cost-effective support for mental health but are predominantly developed in WEIRD (western, educated, industrialized, rich, democratic) contexts, raising questions about their global applicability. Dropout, attrition, and adherence rates critically influence DMHI effectiveness yet remain poorly characterized in culturally adapted formats. This systematic review aimed to (1) synthesize evidence on dropout, attrition, and adherence in culturally adapted DMHIs delivered to non-WEIRD adult populations and (2) assess the methodological quality of the included studies. PsycINFO, PubMed, and ScienceDirect were systematically searched for randomized controlled trials published in English between January 2014 and April 2024. Screening and data extraction followed PRISMA (Preferred Reporting Items for Systematic Reviews and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
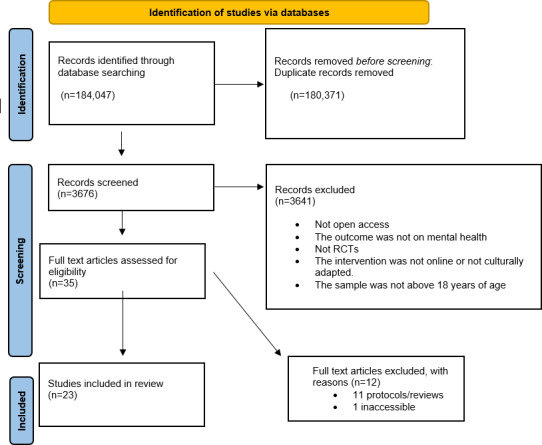 Figure 1
Figure 1| Author and year | Country of origin | Adapted country | Recruitment settings | Age (y), mean (SD) | Demographics | Intervention type | Platform used | Adaptation framework used | Dropout rate (%) | Attrition rate (%) | Adherence rate (%) | Primary outcome measure |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Zhang et al [ | China | China | Not reported | 49.67 (14.49) | Insomnia (chronic insomnia disorder), Chinese; 74.4% female | DCBT-I | Smartphone-based app | Not reported | 11 | 11 | 94 | Insomnia (ISI |
| Spanhel et al [ | Germany | Germany | Online | 26.8 (4.4) | International students in Germany (92.6% with insomnia); 49.4% female | StudiCare Sleep-e based on CBT | Web-based intervention on Minddistrict platform | Adaptation included content (eg, removal of sleep restriction), duration (shortened from 6 to 3 modules), language (translation into English), and the use of students as case examples. | 56 | 46 | 44 | Insomnia (ISI) |
| Zeng et al [ | China | China | Outpatient clinics; online | 28 (5.8) | HIV seropositive individuals with depressive symptoms; 5.33% female. | WeChat-based mHealth | WeChat-based (app-based) | Not reported | 50 | 8 | 100 | Depression (CES-D) |
| Guo et al [ | China | China | Outpatient clinics; online | 28.3 (5.85) | HIV seropositive individuals with depressive symptoms; 7.65% female. | Run4Love based on CBSM | WeChat with multimedia materials, automated tracking, and phone check-ins. | CBSM adapted in Chinese context | 41 | 41 | 50 | Depression (CES-D) |
| Campbell et al [ | United States | United States | Outpatient clinics | 38. 6 (10.3) | American Indian and Alaska Native in the United States; 45.3% female, 1.9% transgender. | TES-NAV | Smartphone app or clinic tablets | Integrated multiframework adaptation: (1) Ecological Validity Model (Bernal et al [ | 49 | 31 | 74 | Abstinence from heavy drinking or drug use (urine screen and self-report) |
| Lindegaard et al [ | Sweden | Sweden | Not reported | 33.86 (8.2) | Depressive Kurdish people of Sweden; 46% female | ICBT | Secure online platform: Iterapi | No formal framework cited | 28 | 44 | 52 | Depression (BDI-II) |
| Silva et al [ | United States | United States (Spanish speaking population) | Not reported | 42.7 (11.6) | Native Spanish speaking individuals; DSM | CBT4CBT | Web based | Cultural constructs by Anez et al [ | 12 | 5 | 88 | Change in SUD |
| Yeung et al [ | United States | United States (Chinese American immigrants) | Online | 50 (14.5) | Monolingual Chinese Americans with depression, 63% female | T-CSCT | Polycom VSX3000 systems were used for videoconferencing. Later, switched to Skype | Culturally sensitive psychiatric consultation using the Engagement Interview Protocol (EIP). | Not stated | Not stated | Not stated | Depression (HDRS17) |
| Sarfraz et al [ | Pakistan | Pakistan | Online | 22.90 (3.57) | Undergraduate and postgraduate university students, 69% female | MTC | Zoom and email | Medical Research Council (MRC) guidelines for complex interventions; Heuristic framework for cultural adaptation | 28 | 28 | 48 | Psychological distress (CORE-OM) |
| Zemestani and Fazeli Nikoo [ | Iran | Iran | Not reported | 29.59 (3.59) | Pregnant women (1‐6 wk of gestational age) | MBCT | In-person group sessions + audio for home practice (offline) | No formal framework cited | 13 | 23 | 87 | Depression (BDI-II); Anxiety (BAI) |
| Spruill et al [ | United States | United States | Outpatient clinics | 43.3 (11.3) | Hispanic ethnicity; 67% primary Spanish speaker; 71% female | Project UPLIFT | Telephone | No formal framework cited—adaptations informed by qualitative research and best practices (eg, focus groups, simplification, cultural tailoring); | 14 | 7 | 75 | Depression (PHQ-9) |
| Zhang et al [ | China | China | Outpatient clinics; online | 30.29 (4.29) | Pregnant women in China | GSH-MBI | WeChat mini-program | No formal framework cited—adaptations relied on culturally tailored content delivered through WeChat. | 19 | 16 | 81 | Depression (EPDS) |
| Benjet et al (2023) [ | Mexico and Colombia | Mexico and Colombia | Online | 21.4 (3.2) | University students; 1038 women (78.7%); 725 participants (55.0%) came from Mexico | i-CBT | Web based | Iterative user-centered model | Not reported | 32 | Not reported | Anxiety (GAD-7) and depression (PHQ-9) scores |
| Vaca et al [ | United States | US Latino adults | Not reported | 36.2 (11.2) | 433 (51.5%) were male, 407 (48.5%) were female and 83% of them were from Puerto Rico | AB-CASI | Computer tablets (iPad 4th Generation; Apple Inc) | Not explicitly named | Not reported | 24 | Not reported | Alcohol Use Disorders (AUDIT) |
| Zhou et al [ | United States | United States (specific adaptation for Black women in the United States) | Not reported | 59.5 (8) | American Black women | SHUTi-BWHS | Web-based | Stakeholder-informed, iterative cultural adaptation process (not explicitly a formal framework, but uses participatory design principles) | 22 | 16 | 78 | Insomnia (ISI) |
| Javier et al [ | United States. | Filipino families | Not reported | 42 (5.6) | Filipino; parents: 81.7% females, 16.3% males | Incredible Years School Age Basic and Advance Programs | Web based | Language, persons, metaphors, content, concepts, goals, methods, and context based on Bernal et al, [ | 18 | 18 | Not explicitly mentioned | Parenting practices (PPI) |
| Owen et al [ | United States | African Americans in the United States | Outpatient clinics; online | 65.9 | African Americans; 14 females and 3 males | CBT | In-person and online group formats | Agricultural Coping Model using amalgam of norms from West Africa, cultural traditions and practices from European/American society, and experiences of historical and contemporary racism in the United States | Not reported | 18 | Not reported | Cognitive function (MoCA) |
| Lindegaard et al [ | Sweden | Sweden (for Arabic-speaking immigrants and refugees) | Online | 37.5 (11.4) | Arabic-speaking population, 25 females and 34 males | ICBT | Web-based with asynchronous therapist messaging and feedback | Iterative adaptation and tailoring process (focus groups + pilot feedback) | 39 | Not reported | Not reported | Depression (PHQ-9) |
| Yamaguchi et al [ | Japan | Japan | Community | 20.25 (1.31) | University students, 26 females and 70 males | FSC | In-person (initial session)+ email follow-up | Not reported | Not reported | 28 | Not reported | Reported behavior, and the other on intended behavior (RIBS-J) |
| Ellis et al [ | United States | Egypt | Not reported | Range 20‐54 (28) | Arabic speaking population, 62 females and 25 males | CBT-based PTSD | Web based | Bernal et al (1995) [ | Not reported | 13 | Not reported | PTSD (PCL-5) |
| Sun et al [ | United States | China | Online | 22.21 (2.67) | University students, 73.7% females | Mindfulness-based mHealth | Web-based via WeChat (mini-program) and Zoom | Informed by focus group input; rapid iterative tailoring (no formal framework named) | 9 | 13 | Not reported | Anxiety (GAD-7); depression (PHQ-9) |
| Jacobs et al [ | United States | Ecuador | Community | ≥18 | Students | Familias Unidas is a parent-centered intervention | In-person sessions; group and family-based, Audio Computer-Assisted Self-Interviewing | Barrera et al’s [ | Not reported | Not reported | Not reported | Drug use (self-reported by adolescents); Adolescent sexual behavior, drug use, and violence (ACASI) |
| Barrera et al [ | United States | Spain | Online | 30.19 (5.57) | Pregnant women, majority resided in Chile, Spain, Argentina, Mexico, Colombia, and the United States. Most were Spanish speaking (82.9%) of Latino/Hispanic ethnic identity (71.3%), and identified their racial background as Caucasian/European (53.2%) or Mestizo (31.8%) | Mothers and Babies Internet Course/Curso Internet de Mamás y Bebés (e-MB) based on CBT approach | Web-based accessed via email login links | Iterative user-feedback model (usability testing, linguistic translation, visual editing) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDigital Mental Health Interventions · Mental Health Treatment and Access · Impact of Technology on Adolescents
Introduction
Digital mental health interventions (DMHIs) have seen explosive growth in recent years [1], offering scalable, cost-effective ways to broaden access, reduce costs, and empower users to self-manage their well-being [23]. These platforms—including mobile apps, video-based therapy, peer-led communities, and interactive web modules—provide flexible, on-demand support [4], with users reporting benefits such as scheduling and location flexibility, low effort, enhanced access and anonymity, greater trustworthiness with facilitators [5]. Pandemic-related demand and advances in digital access have accelerated DMHI development globally [67].
Alongside this expansion, longstanding debates about cultural relevance in public health have extended into the digital realm [89]. Most digital health research remains rooted in WEIRD (western, educated, industrialized, rich, democratic) settings [10-12], raising questions about generalizability. While some small-scale adaptations—such as a sleep-support app tailored for German refugees—have demonstrated high satisfaction and comparable adherence [13]. However, a systematic review of over 10,000 participants found no consistent efficacy advantage for culturally adapted interventions [14]. These mixed findings suggest that adaptation may boost initial uptake but does not guarantee sustained engagement or better outcomes.
A critical factor underlying these mixed results is participant retention [15]. High dropout and attrition can erode both effectiveness and cost-efficiency [16], making retention metrics essential for evaluation. Research typically focuses on three core measures: the dropout rate (discontinuation before completion [17]), the attrition rate (loss to follow-up or ceased usage [18]), and the adherence rate (completion of prescribed sessions [19]). Understanding what drives these outcomes—be it cultural fit, usability barriers, or motivational factors—is key to crafting sustainable, impactful digital interventions [2021].
Therefore, the present systematic review aims to comprehensively examine retention and engagement outcomes in culturally adapted DMHIs implemented among non-WEIRD adult populations. Specifically, this review seeks to (1) synthesize evidence on dropout, attrition, and adherence rates across studies and (2) evaluate the methodological quality of the included trials to identify strengths, limitations, and factors associated with higher retention and adherence.
By addressing these objectives, the review intends to generate evidence-based recommendations to guide the design and implementation of culturally responsive DMHIs worldwide.
Methods
Article Search and Selection
This review was preregistered on PROSPERO (Prospective Specific Evaluation of Reviews) (CRD42025641863 [22]). The literature search took place from February 2024 and ended in July 2024. To ensure comprehensiveness, we used three search strategies: database searches and manual searches of reference lists of relevant articles.
Database Search
The review followed the guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [23]. A comprehensive search was conducted in the following electronic databases: (1) PsycINFO, (2) PubMed, and (3) ScienceDirect. The search strategy was designed to identify both quantitative and qualitative studies focusing on culturally adapted mental health interventions delivered via digital platforms (eg, e-mental health, mobile applications). Search terms were developed using combinations of keywords related to cultural adaptation (eg, “culturally appropriate,” “adapted intervention”) and intervention modality (eg, “digital health,” “mobile app,” “e-mental health”). To ensure breadth and sensitivity, the search strategy incorporated a wide range of related terms. The complete search strategy is provided in Multimedia Appendix 1 [24]. Given that previous reviews included studies up to 2014, only studies published between January 2014 and April 2024 were included. The systematic search process and the rationale for study inclusion and exclusion were documented in accordance with PRISMA standards (see Checklist 1). Two lead authors independently reviewed articles for inclusion, with disagreements resolved through discussion and consensus.
Inclusion and Exclusion Criteria
The population, intervention, control, and outcomes model served as the foundation for the creation of the inclusion criteria [25]. People from non-WEIRD societies were referred to as part of the population [12]. This systematic review focuses on DMHIs adapted for non-WEIRD populations, with clearly defined inclusion and exclusion criteria.
Eligible interventions must be internet-, computer-, or mobile-based to address mental health problems, including depression, anxiety, or trauma.They must also be culturally adapted for the target group to align with the population’s cultural context.The target population includes adults aged 18 years or older from non-WEIRD cultural backgrounds that differ from the original intervention target group.Only randomized controlled trials (RCTs) published in peer-reviewed English-language journals within the last 10 years are included, with no restrictions on the type of setting (eg, rural, urban, clinical, or non-clinical).
Exclusion criteria were excluded if they (1) involved interventions that lack cultural adaptation, (2) targeted individuals under 18 years, (3) were nondigital interventions, (4) were observational studies, case reports, and qualitative studies, and (5) were articles not published in English or outside the 10-year timeframe. By adhering to these criteria, the review will evaluate the impact of cultural adaptations on reducing drop-out rates and the overall effectiveness of these interventions.
Data Screening and Eligibility
After duplicates were removed using EndNote (version 20.3; Clarivate), the remaining records were screened manually using Microsoft Excel. The titles and abstracts were independently screened by two lead authors, based on pre-established inclusion and exclusion criteria. The level of agreement between the screeners was 85% across title/abstract screening, data extraction, and quality assessment stages. Discrepancies were resolved through discussion until consensus was reached.
Data Extraction
Overview
Data extraction was conducted manually using a predesigned Excel spreadsheet. The data extraction plan was developed in accordance with PRISMA guidelines and informed by recent reviews on digital health interventions among minority populations [26-28]. One author extracted the data, and another author independently cross-checked the entries for accuracy. As this is a systematic review, no imputation or sensitivity analyses were conducted. Medians and ranges were calculated only for studies that explicitly reported each outcome, and the number of contributing studies (n) is provided for each summary statistic.
Extraction of Participant Demographics
Demographic information, including participants’ age, gender, and cultural background, was extracted directly from the study descriptions or participant tables. Missing or incomplete demographic data were noted in the extraction sheet.
Extraction of Recruitment Settings
Recruitment methods and settings (eg, community-based, clinical, or online) were coded from the methods section of each study. When not explicitly stated, the inferred setting was noted.
Extraction of Engagement Metrics (Dropout, Adherence, and Attrition)
Engagement data were extracted as follows: dropout was defined as noncompletion of the intervention; attrition as loss to follow-up; and adherence as the proportion of sessions completed. If data were not reported, this was recorded as “not available.”
Extraction of Cultural Adaptation Strategies
Details on cultural adaptation (eg, translation, content tailoring, stakeholder involvement, and iterative feedback) were extracted from intervention descriptions. Adaptations were coded as surface-level or deep-level.
Extraction of Clinical Outcomes
Primary and secondary clinical outcomes (eg, depression, anxiety, insomnia) and their corresponding measurement tools were extracted and coded for direction of effect (improvement, no change, or worsening).
Quality Assessment
Two authors independently conducted the quality assessment of all included quantitative studies using the Appraisal Tool for Cross-Sectional Studies [29]. Disagreements were resolved by discussion. Each item was rated as “yes,” “no,” or “do not know,” with scores assigned according to conventions used in previous reviews [3031]: yes or not applicable (N/A)=1 point; no or do not know=0 points. Total scores ranged from 0 to 20, with studies rated as good (≥15), fair (10-14), or poor (<10).
Results
Study Selection
A total of 184,047 records were identified through the database search. After removing duplicates (n=180,371), 3676 articles remained for title and abstract screening. Of these, 3641 were excluded based on the predefined inclusion and exclusion criteria. The remaining 35 articles were assessed for eligibility by the authors. Eleven studies were excluded at this stage because they were study protocols or review articles, and one study met all inclusion criteria but was excluded from the final review due to inaccessibility; attempts to obtain the full text through institutional subscriptions and direct author contact were unsuccessful. Ultimately, 23 articles were included in the final review. The study selection process is summarized in Figure 1, and detailed study descriptions are available in Multimedia Appendix 2 and Table 1.
PRISMA flowchart. RCT: randomized controlled trial.
Participant Demographics
Participants (n=4656; see Multimedia Appendix 2) represented diverse cultural and demographic backgrounds. Several studies focused on specific subpopulations like pregnant women who were targeted in two studies [476061], while young adults aged 18 to 30 years were the focus of 39% (8/23) [3334444855576162]. Chinese participants were the most frequently represented cultural group, included in 26% (6/23) of studies [32-34434757undefinedundefined]. University students from various countries were the focus in 21% (5/23) of studies [4448555762]. Studies involving Middle Eastern or Arabic-speaking populations accounted for 17% (4/23) [13545661]. A significant proportion of studies examined Hispanic/Latinx participants (7/23, 30%) [40464849586062] and only two studies (2/23, 9%) included Black American participants [5053], and one study (1/23, 4%) evaluated a DMHI among Indigenous communities [35], highlighting ongoing underrepresentation of these groups in culturally adapted digital mental health research, and one study was conducted on Japanese students [55].
Recruitment Settings
Among the 23 included studies, most investigated DMHIs among participants residing in urban settings (8/23, 35%), typically located near metropolitan areas [3235434649505558]. Most of the studies (14/23, 61%) often relied on community-based recruitment methods such as advertisements, mailing lists, and outreach through community centers [3235434446485053-5557586162undefinedundefined]. Internet-based recruitment was the second most common strategy, used in 22% (5/23) of studies, primarily through platforms such as social media [4454555760]. Seven studies (7/23, 30%) recruited participants directly from outpatient clinical settings located in urban areas [32-35434653undefinedundefinedundefined]. A notable proportion of studies (7/23, 30%) recruited through universities and online platforms—to enhance sample diversity and reach [32344748535462]. For six studies (6/23, 26%), recruitment settings were not clearly reported, although some recruitment strategies (eg, convenience or snowball sampling) were described [454750515661].
Engagement Metrics: Dropout, Adherence, and Attrition Rates
Across the 23 included studies, participant engagement varied substantially. Attrition rates—defined as loss to follow-up—ranged from 5.3% to 87%, with a median attrition rate of approximately 18.4% among studies reporting this outcome. While some studies demonstrated relatively low attrition (eg, <15%) [4647565761], some reported notably high rates (>35%) [446062], and five studies did not state attrition rates [3334435458], limiting comprehensive comparison. Attrition rates were reported in 61% (14/23) of studies. Dropout rates, reflecting noncompletion of the intervention, also varied widely, from 0% to 66%, with a median dropout rate of 18.7%. Dropout rates were reported in 17 studies (17/23). Adherence rates, or the proportion of sessions or modules completed by participants, ranged from 26.3% to 100%, with a median adherence rate of approximately 71% in studies that reported these data. Adherence rates were reported in 61% (14/23) of studies. High adherence was reported in programs such as internet-delivered cognitive behavioral therapy (Sleep Healthy Using the Internet for Black women) [50], where over 60% of participants completed all modules. However, 39% (9/23) of studies did not report adherence rates [43485153-58undefinedundefinedundefinedundefinedundefined]
Cultural Adaptation Strategies
Across the included studies, a wide range of cultural adaptation strategies were employed to enhance the relevance and effectiveness of DMHIs for diverse populations. One of the forms of cultural adaptation used in the studies was language translation, implemented in 57% (13/23) of studies to improve linguistic accessibility [32334446-4850515456-5860undefinedundefinedundefinedundefined]. The other forms of cultural adaptation included content and imagery adaptations that were mainly used in 70% (16/23) of studies to align with cultural norms, such as visuals and metaphors tailored for specific populations [33354446-485051535456-5860-62undefinedundefinedundefinedundefinedundefinedundefined]. In 70% (16/23) of studies, cultural values and local practices were integrated into the intervention design, including the incorporation of traditional healing methods for Indigenous groups [33354446-485051535456-5860-62undefinedundefinedundefinedundefinedundefinedundefined]. Stakeholder involvement—including collaboration with cultural experts, local communities, and leaders—was reported in 48% (11/23) of studies [33354446-485051535456-5860-62undefinedundefinedundefinedundefinedundefinedundefined]. Iterative feedback and refinement processes—using focus groups, cognitive interviews, and pilot trials—were used in 43% (10/23) of studies to adjust the interventions based on user responses [33354446-485051535456-5860-62undefinedundefinedundefinedundefinedundefinedundefined]. Only three studies (3/23, 13%) employed the Ecological Validity Framework (EVF), guiding systematic adaptation across multiple cultural dimensions [515661]. Similarly, surface- and deep-structure adaptations—which modify both observable aspects like language and deeper cultural constructs—were applied in 9% (2/23) of studies [4458]. Technology adaptation to locally preferred platforms (eg, WeChat in China) was reported in 35% (8/23) of studies [32334756-586061undefinedundefined]. However, only one study (1/23; 4%) included cultural competency training for providers to ensure culturally sensitive delivery [53].
Clinical Outcomes
The studies included in this systematic review reported various clinical outcomes, focusing on improvements in mental health symptoms, quality of life, and other relevant measures. Most commonly, the studies targeted insomnia and sleep-related issues as primary clinical outcomes (4/23, 17%) [32505462], followed by depression (12/23, 52%) [32-3446-49545760-62undefinedundefinedundefinedundefinedundefinedundefinedundefined] and anxiety (8/23, 35%) [324547-4954566162undefinedundefined]. Other notable outcomes included significant reductions in pregnancy-related anxiety among pregnant women in China using a digital guided self-help mindfulness-based intervention [47] an automated bilingual digital health tool in the United States significantly reduced binge drinking episodes [49].
Methodological Quality Assessment
Overall, most studies (21/23, 91%) were of high methodological quality. Overall, most studies demonstrated clear research aims and employed study designs that were appropriate and well justified in relation to their objectives. The target populations were clearly defined across all studies. Statistical methods were generally well described. Additionally, the key findings of the studies were usually presented clearly, with discussions and conclusions that were largely justified. Most studies also acknowledged their limitations, enhancing transparency. However, improvements are needed in two studies [5862] by ensuring representative sampling, justifying sample sizes, addressing nonresponse bias, and transparently reporting dropout data.
Discussion
Principal Findings
This systematic review synthesized findings from 23 RCTs examining dropout, attrition, and adherence in culturally adapted DMHIs among non-WEIRD adult populations. Participant engagement varied widely, with median dropout and attrition rates around 18% and mean adherence of 71%. Interventions using deep, participatory forms of cultural adaptation—combining translation with locally meaningful content, stakeholder involvement, and iterative refinement—showed the highest adherence (often >75%) and lowest dropout (typically <11%). In contrast, interventions limited to surface-level adaptations such as language translation alone frequently exhibited higher dropout (up to 56%) and lower adherence.
Patterns in Engagement
Dropout rates ranged from 6% to 87% and appeared to vary depending on adaptation depth [4760]. Studies integrating multiple culturally grounded elements (eg, language, imagery, values, and delivery context) reported greater retention and engagement. For instance, Zhang et al [32] integrated culturally specific sleep concepts into a CBT-I intervention, achieving a dropout rate of only 6.09%, while Silva et al [40] used culturally resonant telenovela-style content and reported dropout at 8.4%. These findings indicate that culturally resonant content may be linked to greater trust, relevance, and sustained participation.
Impact of Adaptation Depth
By contrast, interventions that employed surface-level adaptations—such as translation without deeper contextual integration—or lacked explicit cultural adaptation tended to show higher dropout. Spanhel et al [62], for example, provided a non-adapted English CBT intervention to a diverse population and observed a dropout rate of 56%. Similarly, Zeng et al [33] and Guo et al [34] implemented basic linguistic and platform-level adaptations but reported dropout rates of 49.2% and 41%, respectively. These findings suggest that surface-level efforts were typically associated with lower sustained engagement in culturally diverse populations.
Participatory Design and Implementation
The role of participatory design processes emerged as another important determinant of adherence. Studies like Zhou et al [50] and Lindegaard et al [39] used stakeholder input such as including collaboration with cultural experts, local communities, and leaders and iterative design such as using focus groups, cognitive interviews, and pilot trials, which corresponded to relatively low dropout rates (10.5% and 28%, respectively). However, participatory adaptation alone did not guarantee low attrition, as seen in Barrera et al [60], where despite iterative feedback mechanisms, dropout peaked at 86.97%, possibly due to high geographic and contextual diversity or technological barriers. This highlights the need to complement participatory design with context-sensitive implementation strategies.
Engagement and Clinical Outcomes
An overall pattern emerged in which studies with lower dropout rates were often observed alongside stronger clinical outcomes. For instance, Zhang et al [32], Silva et al [40], and Sun et al [57] demonstrated both high retention and significant reductions in insomnia, depression, or anxiety. However, some studies with moderate to high dropout (eg, Refs [4448]) still reported clinical improvements among completers, indicating that while adaptation enhances effectiveness, it may not be sufficient to retain all users without additional strategies to address barriers to access and sustained use.
Despite engagement data from 23 RCTs, a meta-analysis was not possible due to heterogeneity in interventions, populations, outcomes, and definitions of engagement, as well as limited extractable data (≈60%) and small moderator subgroups. We therefore share the descriptive synthesis, and future work using standardized metrics may allow meta-regression.
Strengths and Limitations of Current Evidence
The reviewed studies highlight several strengths of culturally adapted interventions in supporting engagement and clinical outcomes. Many adapted programs demonstrated higher completion and retention rates, such as tailored versions of Sleep Healthy Using the Internet for Black women [50] and Project Using Practice and Learning to Increase Favorable Thoughts for Hispanic adults [46]. Several interventions also reported improved clinical outcomes, including reduced substance use, greater abstinence, and enhanced sleep or mood symptoms. These positive patterns were most often observed in studies incorporating language congruence and cultural values such as communal participation and sensitivity to race-based stressors.
Despite these successes, several limitations emerged. Many pilot trials had small samples, limiting generalizability and highlighting the need for larger, multi-center validation [3239465354]. Perceived cultural relevance also varied within target groups; for instance, in [53], although 84% of participants found the adaptation relevant, some viewed it as “overdone,” reflecting within-group diversity and the importance of facilitator racial matching [53]. Some culturally adapted DMHIs faced challenges in sustaining engagement, such as the online mindfulness course for Pakistani students with high attrition [44] and the Egyptian post-traumatic stress disorder intervention whose participants desired more “human” interaction [56]. A further limitation is that a quantitative meta-analysis or meta-regression was not performed. Considerable heterogeneity in study design, intervention type, and outcome measures—along with inconsistent definitions of adherence and dropout and limited extractable numerical data—made statistical aggregation inappropriate. Subgroup counts were also too small for stable moderator modeling. Moreover, standardized mean differences or confidence intervals for clinical outcomes could not be reported, as most studies used heterogeneous measures and lacked sufficient statistical detail. Consequently, clinical outcomes were synthesized narratively to reflect overall improvement of trends across interventions. Future research should standardize engagement metrics and reporting to enable robust meta-analytic and meta-regression approaches that can better quantify determinants of adherence and attrition. Finally, many studies relied solely on self-reported outcomes and unblinded data collection, increasing the risk of bias [5356]
Conclusion
Drawing from these implications, several key recommendations emerge for future research and practice. First, it is essential to prioritize comprehensive cultural adaptation, moving beyond superficial changes to genuinely embed content and delivery methods within the target culture’s values and sociocultural realities [53]. This includes ensuring language congruence [46] and actively involving community members and cultural experts in the design process to ensure adaptations are relevant and address within-group heterogeneity [53]. Second, to support [22] engagement and retention, hybrid models integrating human support should be considered, as noted by users of a culturally adapted web-based post-traumatic stress disorder intervention for Egyptians who desired more “human” interaction and personalization [56]. Proactive monitoring of engagement metrics is also vital to enable timely re-engagement strategies [33]. Third, given that the perceived cultural relevance can be influenced by the race of the intervention facilitator [53], comprehensive cultural competence and implicit bias training for facilitators are recommended to build trust and address potential microaggressions [53].
Supplementary material
10.2196/80624Multimedia Appendix 1 Complete search strategy used for PsycINFO, PubMed, and ScienceDirect databases.
10.2196/80624Multimedia Appendix 2 Detailed study descriptions (Table 1) of included randomized controlled trials.
10.2196/80624Checklist 1PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Graham AK Lattie EG Powell BJ et al Implementation strategies for digital mental health interventions in health care settings Am Psychol Nov 202075810801092 doi 10.1037/amp 0000686 Medline 33252946 PMC 7709140 · doi ↗ · pubmed ↗
- 2Koh JH Chong LCY Koh GCH Tyagi S Telemedical interventions for chronic obstructive pulmonary disease management: umbrella review J Med Internet Res Feb 16202325 e 33185 doi 10.2196/33185 Medline 36795479 PMC 9982717 · doi ↗ · pubmed ↗
- 3Weatherly S Mc Kenna T Wahba S et al Effectiveness of digital health interventions (DHI) in chronic pain management: a scoping review of current evidence and emerging trends Cureus Oct 20241610 e 72562 doi 10.7759/cureus.72562 Medline 39610577 PMC 11602419 · doi ↗ · pubmed ↗
- 4Early J Gonzalez C Gordon-Dseagu V Robles-Calderon L Use of mobile Health (m Health) technologies and interventions among community health workers globally: a scoping review Health Promot Pract Nov 2019206805817 doi 10.1177/1524839919855391 Medline 31179777 · doi ↗ · pubmed ↗
- 5Wallin EEK Mattsson S Olsson EMG The preference for internet-based psychological interventions by individuals without past or current use of mental health treatment delivered online: a survey study with mixed-methods analysis JMIR Ment Health Jun 14201632 e 25doi 10.2196/mental.5324 Medline 27302200 PMC 4925931 · doi ↗ · pubmed ↗
- 6Wang Q Su M Zhang M Li R Integrating digital technologies and public health to fight COVID-19 pandemic: key technologies, applications, challenges and outlook of digital healthcare IJERPH 202118116053 doi 10.3390/ijerph 1811605334199831 PMC 8200070 · doi ↗ · pubmed ↗
- 7Abernethy A Adams L Barrett M et al The promise of digital health: then, now, and the future NAM Perspect 2022202210 doi 10.31478/202206 e Medline 36177208 PMC 9499383 · doi ↗ · pubmed ↗
- 8MeskóB Drobni Z BényeiÉ Gergely B Győrffy Z Digital health is a cultural transformation of traditional healthcarem Health 2017338 doi 10.21037/mhealth.2017.08.07Medline 29184890 PMC 5682364 · doi ↗ · pubmed ↗