Efficacy, Safety and Tolerability of Volixibat, an IBAT Inhibitor, in Patients With Intrahepatic Cholestasis of Pregnancy
Caroline Ovadia, Sophia Stone, Baha Sibai, Tiago Nunes, Douglas B. Mogul, Jayshree Krishnaswami, Jennifer Kahng, Furong Li, Qurratul Ann Warsi, Elaine Chien, Pamela Vig, Catherine Williamson

TL;DR
Volixibat, a drug for intrahepatic cholestasis of pregnancy, reduced itching and bile acid levels in most patients, with mild side effects and no drug detected in maternal blood.
Contribution
Volixibat shows efficacy and safety in treating intrahepatic cholestasis of pregnancy with minimal systemic absorption.
Findings
Volixibat reduced serum bile acid levels below 6 μmol/L in all patients.
Most participants experienced improved pruritus with treatment.
The main adverse event was diarrhea, which improved with dose reduction.
Abstract
Intrahepatic cholestasis of pregnancy (ICP) presents with cholestatic pruritus, elevated sBA and increased risk of adverse perinatal outcomes. Volixibat is a minimally absorbed IBAT inhibitor that interrupts enterohepatic recirculation. We describe four patients with ICP with pruritus and sBA > ULN treated with volixibat (20 or 80 mg BID orally until delivery), with dose modifications permitted for tolerability. Daily pruritus scores, sBA, liver enzymes, perinatal outcomes and TEAEs were assessed. Over 1000 patients were invited to participate; 26 were screened, and four received volixibat. Three patients experienced reductions in pruritus from baseline regardless of volixibat dose, with intermittent relief coinciding with resumption of dosing when doses were interrupted. sBA nadir values all reached < 6 μmol/L following volixibat. No clinically meaningful changes in laboratory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
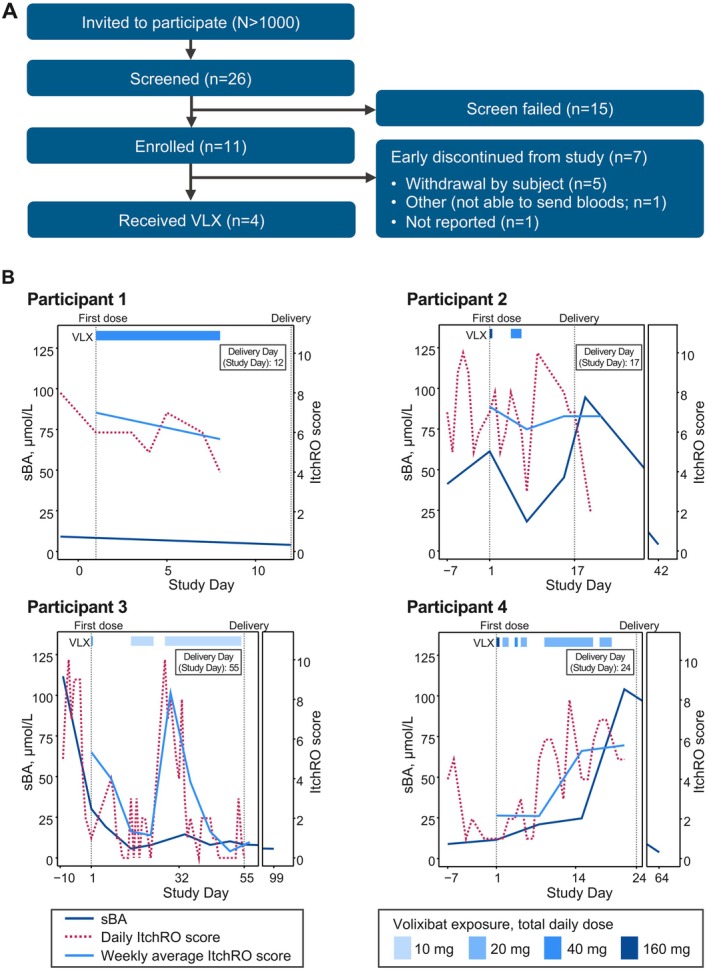 FIGURE 1
FIGURE 1| Participant | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Key baseline demographics | ||||
| Age, years | 20 | 25 | 25 | 38 |
| Pruritus, ItchRO | 7.0 | 7.3 | 5.3 | 2.2 |
| Peak sBA level prior to first dose, μmol/L | 13 | 43 | 112 | 12 |
| Initial dose of VLX, mg | 40 | 160 | 40 | 160 |
| Treatment duration, wk | 1.1 | 0.6 | 5.3 | 2.6 |
| Prior and/or concomitant UDCA usage, dose | No | No | Yes, 500 mg BID | Yes, 500 mg BID |
| Maternal and perinatal outcomes | ||||
| Pruritus, change from baseline to end of treatment, ItchRO | −1.3 | −2.0 | −4.5 | 3.5 |
| sBA, change from baseline to end of treatment, μmol/L | −4.2 | 51.5 | −22 | −6.6 |
| Gestational age at delivery, wk/d | 37/6 | 35/4 | 37/1 | 34/4 |
| Delivery type/mode | Full/V | Preterm/V | Full/C | Preterm/C |
| Labor type | Iatrogenic related to ICP | Spontaneous | Iatrogenic related to ICP | Iatrogenic related to ICP |
| Live birth vs. stillbirth | Live | Live | Live | Live |
| NNU admission | No | Yes | No |
Yes (respiratory support needed) |
| Maternal complications | Yes | No | No | No |
| Postpartum haemorrhage | No | No | No | No |
| ALT change from baseline to end of treatment, U/L | 2 | 4 | 44 | 17 |
| VLX concentrations in maternal venous blood, ng/mL | < 0.05 | < 0.05 | < 0.05 | < 0.05 |
| VLX concentrations in umbilical venous blood, ng/mL | NA | NA | < 0.05 | NA |
- —Mirum Pharmaceuticals, Inc.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug Transport and Resistance Mechanisms · Pregnancy and Medication Impact · Pediatric Hepatobiliary Diseases and Treatments
Introduction
1
Intrahepatic cholestasis of pregnancy (ICP) is the most common liver disorder of pregnancy. Typically, ICP affects 0.7% of pregnant women of European ancestry; it is twice as common in women of South Asian ethnicity [1] and affects approximately 3% of women from the Andean regions of Latin America. Presenting features of ICP are maternal pruritus, raised serum bile acid (sBA) concentrations and hepatic impairment [2]. The pruritus is of variable severity but can prevent sleep and impact the mood of affected women. Complications of ICP can include adverse pregnancy outcomes (e.g., preterm birth, meconium‐stained amniotic fluid, intrauterine fetal death and prolonged admission to the neonatal unit) [3, 4]. The extent of maternal hypercholanemia is related to the risk of some pregnancy complications; in women with sBA concentrations of ≥ 40 μmol/L, there is a significantly increased risk of spontaneous preterm birth and meconium‐stained amniotic fluid, and when concentrations are ≥ 100 μmol/L, there is an increased risk of stillbirth, particularly from 35 weeks' gestation [4, 5].
The medication most commonly used to treat ICP is ursodeoxycholic acid (UDCA). While UDCA has limited impact on pruritus severity [6], it has been shown to reduce the rate of spontaneous preterm birth in ICP [7]. Treatment with UDCA reduces serum concentrations of liver transaminases and the chance of meconium‐stained amniotic fluid, but randomised placebo‐controlled trials have given mixed results regarding the impact on sBA concentrations [6].
Ileal bile acid transporter (IBAT) inhibitors prevent uptake of bile acids from the gut lumen by the ileal apical sodium‐dependent bile acid cotransporter (also called ASBT/SLC10A2). They are effective at reducing hypercholanemia and pruritus in adult and paediatric cholestatic disorders. Specifically, the IBAT inhibitor maralixibat has demonstrated not only statistically significant and clinically meaningful reductions in pruritus, sBA levels and bilirubin but also improvements in quality of life across several cholestatic disorders, including progressive familial intrahepatic cholestasis (PFIC), Alagille syndrome (ALGS), primary sclerosing cholangitis (PSC) and primary biliary cholangitis (PBC) [8, 9, 10, 11]. The impact of IBAT inhibitors on children with PFIC associated with ABCB11 and ABCB4 variants is particularly relevant to ICP, as approximately 20% of affected women have heterozygous pathogenic variants in these genes [12, 13].
The aim of the OHANA trial was to evaluate the safety, tolerability and efficacy of the IBAT inhibitor volixibat when used to treat ICP in women with elevated sBA concentrations and symptomatic pruritus.
Methods
2
Trial Design and Participants
2.1
OHANA (NCT04718961) was a phase 2a/2b, randomised, double‐blinded, placebo‐controlled adaptive clinical trial consisting of two parts (Figure S1). Part 1 was a proof‐of‐concept open‐label study that assessed volixibat dosing range. The goal of Part 2 (double‐blinded randomised period) was to compare the volixibat dose selected from Part 1 with placebo to determine superior efficacy. Because of the early termination of the OHANA trial due to lack of enrollment, data were analysed for the four participants enrolled during Part 1 of the trial and are summarised in this report. Key eligibility criteria and additional methodology are included in the Supporting Information.
Treatment
2.2
After a screening period of up to 10 days, participants were randomised to either 20 or 80 mg twice daily (BID) of volixibat. Study medication dosing began on Day 0 and continued until the end of the treatment period, defined as the day of birth. Dose reduction was permitted at the clinician's discretion. As much as possible, each dose of study medication was administered approximately 30 min before meals. The first dose of study medication was administered under observation in the clinic; monitoring of fetal well‐being was performed before and after dosing.
Assessments
2.3
Efficacy of volixibat on pruritus was assessed by change from baseline to Week 3 of the treatment period (or at birth if this occurred < 3 weeks after commencement of volixibat) in weekly average worst daily itch score as measured by adult Itch‐Reported Outcome (ItchRO), an 11‐point numeric rating scale of worst itch severity ranging from 0 (no itch) to 10 (worst possible itch).
The safety and tolerability of volixibat in participants with ICP during Part 1 were assessed based on the following endpoints: (1) proportion of participants experiencing one or more treatment‐emergent adverse events (TEAEs), serious adverse events (AEs), AEs of special interest, events of clinical interest, or AEs leading to discontinuation of study medication; and (2) proportion of participants experiencing one or more clinically significant laboratory abnormalities. Safety assessments included AEs, clinical laboratory tests, vital signs and physical examinations. Additional fetal safety assessments, including serial ultrasound scans to assess fetal growth and nonstress test/cardiotocography or fetal biophysical profile, were also completed.
Assessments for exploratory objectives included (1) volixibat drug levels in maternal and fetal serum and pharmacodynamic markers in maternal blood in participants with ICP and (2) the effect of volixibat on additional perinatal outcomes.
Data and Statistical Analyses
2.4
The enrolled population consisted of all participants who signed an informed consent form and successfully completed screening. The safety cohort consisted of all participants who received one or more doses of study medication and were classified based on treatment received.
For all safety and tolerability analyses, participants were analysed by the treatment dose received. Since only four participants completed the trial, summary statistics were not calculated. Instead, by‐participant listings were provided for all safety and tolerability variables.
Results
3
Patient Disposition and Baseline Demographics
3.1
OHANA comprised 25 sites in three countries (New Zealand, United Kingdom and United States) and was conducted from May 25, 2021, through December 7, 2022. The study was terminated by the sponsor in November 2022 due to challenges in enrollment in this high‐risk pregnancy population (Figure 1A). Key demographic features of the four participants who received volixibat are shown in Table 1.
(A) Participant disposition. The schematic depicts actual enrollment completed for the OHANA trial. (B) Changes in sBA levels, daily ItchRO scores and weekly average ItchRO scores in the trial participants 1–4. The figure depicts results for each of the three endpoints following initiation and discontinuation of volixibat treatment in enrolled participants. ItchRO, Itch‐Reported Outcome; sBA, serum bile acid; VLX, volixibat.
Efficacy
3.2
Changes in sBA levels, daily ItchRO scores and weekly average ItchRO scores for each of the four participants over the course of the trial are shown in Figure 1B, and additional maternal and perinatal outcomes are listed in Table 1. Following treatment with volixibat, all participants experienced a reduction of sBA levels, with sustained reductions observed over time in three participants (Figure 1B). For three participants, there was a reduction in sBA concentrations at the time of taking volixibat. All sBA nadir values reached < 6 μmol/L following volixibat treatment, either by the delivery date or during follow‐up assessments. Three participants experienced reductions in pruritus, with marked improvements in pruritus scores regardless of volixibat dose and intermittent relief coinciding with the resumption of volixibat dosing when treatment had been interrupted. No significant deficiencies were observed in vitamin A, D and E levels for all participants.
None of the participants had a stillbirth, two delivered at full term and two delivered preterm (Table 1). Both preterm newborns required neonatal unit admission. One participant experienced additional pregnancy‐related complications unrelated to volixibat treatment (preeclampsia with severe features).
Safety
3.3
No clinically meaningful changes in liver enzyme levels or hematology parameters were observed following treatment with volixibat (Table 1). Serum volixibat levels were minimally detected (< 0.05 ng/mL) in maternal (n = 4) and umbilical venous (n = 1) blood.
The most frequently reported TEAEs were gastrointestinal (Table S1). Three of four participants experienced diarrhoea and/or abdominal cramping leading to dose reduction, treatment interruption and/or early discontinuation. One participant tolerated treatment until delivery with no dose modifications due to AEs. At the end of treatment, volixibat concentrations in maternal and umbilical venous blood were < 0.05 ng/mL. None of the TEAEs triggered premature labor.
Conclusions
4
This report of four women with ICP treated with volixibat showed an improvement in pruritus and a sustained reduction in sBA. The principal maternal AE was diarrhoea, which was severe in two participants, both of whom received the higher volixibat dose. With a reduction in volixibat dose, the symptoms of diarrhoea improved in both women. The reduction in sBA concentrations observed following volixibat treatment is of clinical importance due to the concern about spontaneous preterm birth and stillbirth in ICP cases with high sBA concentrations [4, 5]. Three study participants had sBA concentrations above 40 μmol/L, and volixibat treatment reduced sBA levels in two. No significant deficiencies in fat‐soluble vitamins were observed following volixibat treatment; however, vitamin K was not collected.
The reductions in sBA concentrations and severity of pruritus are consistent with the impact of maralixibat, another IBAT inhibitor, on these cholestasis‐associated disease features in nonpregnant individuals in PSC, PBC, ALGS and PFIC [8, 9, 10, 11, 14, 15]. The positive results from the trial in patients with PFIC, which included the largest number of PFIC types ever studied, are of potential relevance to women with ICP, as pathogenic heterozygous nontruncating variants in ABCB11 or susceptibility loci that increase the risk of ICP are reported in ICP cases [12, 13, 16, 17].
In the current study, AEs occurred more commonly in those taking higher doses of volixibat, similar to what has been reported for other IBAT inhibitors [14, 15]. Importantly, the participants in OHANA who received lower volixibat doses did not have diarrhoea that was sufficiently severe to necessitate cessation of treatment. Previous studies of volixibat did not indicate that the high dose used in the OHANA trial would result in marked diarrhoea [18]. Alteration of volixibat dose did not influence the frequency or severity of these AEs, while in the current trial, a reduction in dose did appear to reduce the frequency and severity of diarrhoea in those who initially received the higher dose of the medication. Thus, future studies of IBAT inhibitors in ICP should consider starting treatment at lower doses with gradual dose increases. The low concentration of volixibat in maternal serum is consistent with previous reports that it is minimally absorbed, likely indicating that the fetus will have limited exposure to the medication [18, 19].
There are several limitations in this trial mainly due to sample size. Since only four participants were enrolled in the trial, formal statistical analyses could not be conducted, and only descriptive statistics and individual data for each participant were reported. While there was no control group in this trial due to the fact that this was a proof of concept, dose finding study, outcomes reported here with volixibat were similar to those reported with maralixibat in ICP [20]. Although OHANA was originally planned as a larger scale clinical trial, since only four participants were enrolled, these results reflect what is typically reported in a case series. While the efficacy and tolerability data with volixibat in ICP are promising, these results should be considered hypothesis generating. This study provided early signals of volixibat's potential as a treatment in ICP, but further research needs to be conducted in order to adequately determine the impact of the medication.
In summary, our study shows the potential utility of IBAT inhibitors for the management of cholestatic pregnancies, demonstrating improvements in pruritus and sBA levels. With safety data indicating no adverse fetal event and minimal to no fetal exposure to the medication, this is a promising new avenue of treatment. Patients with ICP appear more susceptible to the gastrointestinal side effects of the medication than those with chronic cholestatic disease; hence, future strategies may necessitate gradual dose increases, titrating to symptoms. Nevertheless, given the absence of any effective alternative treatment for ICP beyond premature delivery, the potential value of this as a novel treatment warrants further research.
Funding
The study was funded by Mirum Pharmaceuticals Inc.
Ethics Statement
The trial complied with consensus ethical principles derived from international guidelines, including the Declaration of Helsinki and the Council for International Organisations of Medical Sciences International Ethical Guidelines, applicable International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use, Good Clinical Practice guidelines and applicable laws and regulations. The trial protocol, protocol amendments and informed consent documents were approved by an institutional review board or independent ethics committee at each site.
Consent
Informed written consent was obtained from all patients for being included in the study.
Conflicts of Interest
Caroline Ovadia is a consultant for Mirum Pharmaceuticals Inc. Sophia Stone and Baha Sibai have nothing to disclose. Tiago Nunes is an employee of and shareholder in Mirum Pharmaceuticals Inc. Douglas B. Mogul is an employee of and shareholder in Mirum Pharmaceuticals Inc. Jayshree Krishnaswami is an employee of and shareholder in Mirum Pharmaceuticals Inc. Jennifer Kahng is an employee of and shareholder in Mirum Pharmaceuticals Inc. Furong Li is a former employee of and shareholder in Mirum Pharmaceuticals Inc. Qurratul Ann Warsi is a former employee of and shareholder in Mirum Pharmaceuticals Inc. Elaine Chien is a former employee of and shareholder in Mirum Pharmaceuticals Inc. Pamela Vig is an employee of and shareholder in Mirum Pharmaceuticals Inc. Catherine Williamson is a paid consultant for Mirum Pharmaceuticals Inc., and Ipsen; previously advised GSK, and was paid to deliver a webinar by Advanz Pharma and a lecture by Ipsen.
Supporting information
Figure S1: Study Design: Open‐Label Proof‐of‐Concept Phase for OHANA Trial. Table S1: Safety Outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1P. Abedin , J. B. Weaver , and E. Egginton , “Intrahepatic Cholestasis of Pregnancy: Prevalence and Ethnic Distribution,” Ethnicity & Health 4, no. 1–2 (1999): 35–37.10887460 10.1080/13557859998173 · doi ↗ · pubmed ↗
- 2C. Ovadia and C. Williamson , “Intrahepatic Cholestasis of Pregnancy,” BMJ Best Practice, reviewed January 20, 2025, https://bestpractice.bmj.com/topics/en‐us/800.
- 3V. Geenes , L. C. Chappell , P. T. Seed , P. J. Steer , M. Knight , and C. Williamson , “Association of Severe Intrahepatic Cholestasis of Pregnancy With Adverse Pregnancy Outcomes: A Prospective Population‐Based Case‐Control Study,” Hepatology 59, no. 4 (2014): 1482–1491.23857305 10.1002/hep.26617 PMC 4296226 · doi ↗ · pubmed ↗
- 4A. Glantz , H. U. Marschall , and L. A. Mattsson , “Intrahepatic Cholestasis of Pregnancy: Relationships Between Bile Acid Levels and Fetal Complication Rates,” Hepatology 40, no. 2 (2004): 467–474.15368452 10.1002/hep.20336 · doi ↗ · pubmed ↗
- 5C. Ovadia , P. T. Seed , A. Sklavounos , et al., “Association of Adverse Perinatal Outcomes of Intrahepatic Cholestasis of Pregnancy With Biochemical Markers: Results of Aggregate and Individual Patient Data Meta‐Analyses,” Lancet 393, no. 10174 (2019): 899–909.30773280 10.1016/S 0140-6736(18)31877-4PMC 6396441 · doi ↗ · pubmed ↗
- 6L. C. Chappell , J. L. Bell , A. Smith , et al., “Ursodeoxycholic Acid Versus Placebo in Women With Intrahepatic Cholestasis of Pregnancy (PITCHES): A Randomised Controlled Trial,” Lancet 394, no. 10201 (2019): 849–860.31378395 10.1016/S 0140-6736(19)31270-XPMC 6739598 · doi ↗ · pubmed ↗
- 7C. Ovadia , J. Sajous , P. T. Seed , et al., “Ursodeoxycholic Acid in Intrahepatic Cholestasis of Pregnancy: A Systematic Review and Individual Participant Data Meta‐Analysis,” Lancet Gastroenterology & Hepatology 6, no. 7 (2021): 547–558.33915090 10.1016/S 2468-1253(21)00074-1PMC 8192305 · doi ↗ · pubmed ↗
- 8E. Gonzales , W. Hardikar , M. Stormon , et al., “Efficacy and Safety of Maralixibat Treatment in Patients With Alagille Syndrome and Cholestatic Pruritus (ICONIC): A Randomised Phase 2 Study,” Lancet 398, no. 10311 (2021): 1581–1592.34755627 10.1016/S 0140-6736(21)01256-3 · doi ↗ · pubmed ↗