Prevalence of Helicobacter Pylori in Obese Adults: A Literature Review
Adéla NOVOTNÁ, Miloš CHUDÝ, Nikol GOTTFRIEDOVÁ, Daniel KARAS, Pavol HOLÉCZY, Marek BUŽGA

TL;DR
This review examines the link between obesity and Helicobacter pylori infection, finding a higher prevalence of the infection in obese individuals.
Contribution
The study provides a synthesis of existing literature on the relationship between obesity and H. pylori prevalence.
Findings
Most studies show a higher prevalence of H. pylori in individuals with higher BMI.
The relationship between BMI and H. pylori infection is not universally agreed upon in the literature.
Further research is needed to confirm the observed association.
Abstract
Obesity is a major health challenge of the 21st century and the number of obese people is increasing worldwide and with it the number of people suffering from obesity-related diseases. The relationship between the presence of obesity and Helicobacter pylori (H. pylori) infection has long been a subject of interest across the literature. The presented review aimed to analyze the prevalence of H. pylori in adults with higher BMI. A literature search was conducted using the electronic databases Scopus, PubMed and Web of science. The term “Helicobacter pylori” was searched with obesity-related keyword combinations. A total of 1.109 records, published in the last 18 years, were identified through the database search. Of these articles, seven were ultimately included in the analysis. Although the studies did not all agree on the same conclusion, most of them have shown that the greater…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
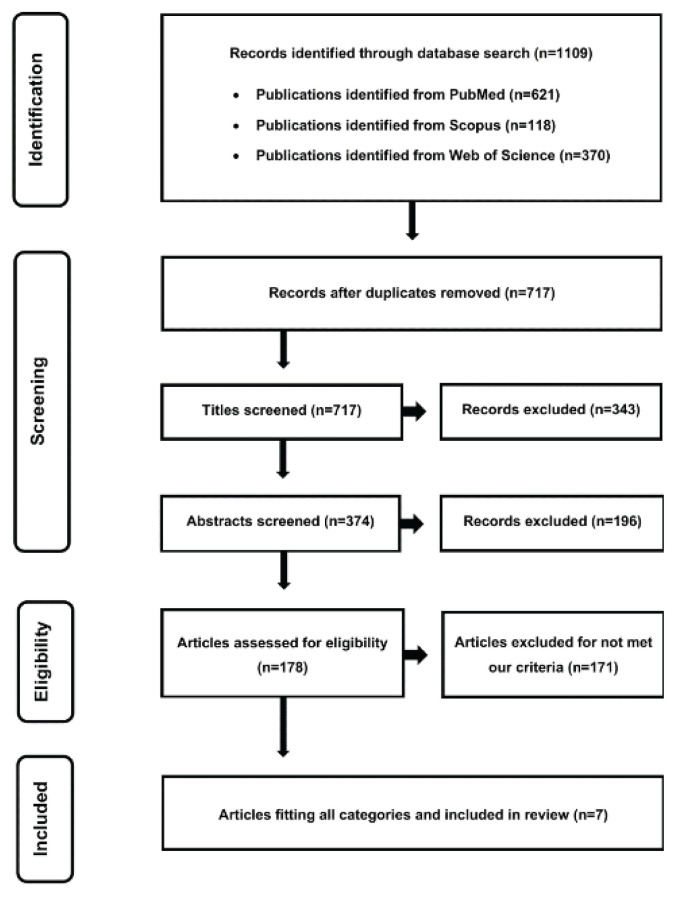 Figure 1
Figure 1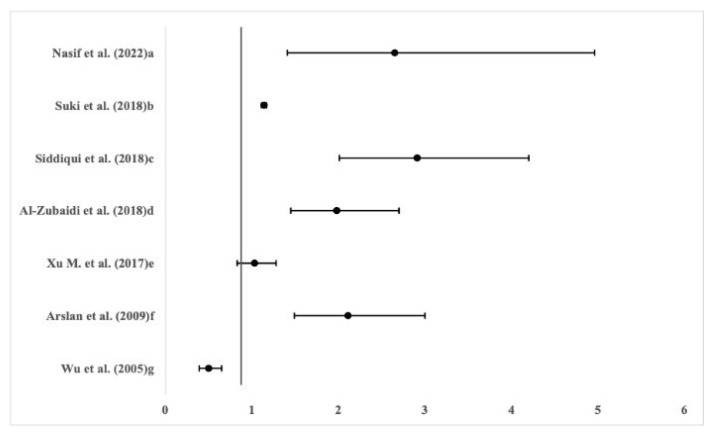 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Microscopic Colitis · Whipple's Disease and Interleukins
Introduction
Obesity is a major disease of the 21^st^ century and its prevalence is increasing in all regions of the world. Between 1980 and 2013, obesity increased globally from 28.8 % to 36.9 % in men and from 29.8 % to 38 % in women, which is alarming as obesity brings along many comorbidities [1]. However, no country has so far succeeded in reversing this pandemic disease. Obesity is part of a global syndrome in which universal societal factors such as the obesity pandemic, the malnutrition pandemic and climate change occur and interact [2,3].
Helicobacter pylori infection has a phenomenon of collective aggregation and represents a major societal problem. Helicobacter pylori (H. pylori) is a gram-negative curved bacteria that adheres to the gastric mucosa and the interstitial space [4]. In 1994, the World Health Organization (WHO) classified H. pylori as a established human carcinogen therefore classified as a Group 1 carcinogen. Current recommendations indicate that H. pylori eradication is indicated in all adults with proven active infection, but routine screening of asymptomatic individuals in the general population is not recommended [5]. Infection can cause stomach diseases such as peptic ulcer disease and gastritis, and approximately 1 % of H. pylori-positive patients develop gastric cancer [6].
H. pylori affects a significant proportion of the global population [7]. According to O’Connor et al., more than 50 % of the population worldwide has been infected with this bacteria, according to Muhammad et al., the global estimated prevalence is around 40–50 % [4,8]. As mentioned, H. pylori infection is strongly associated with gastric ulcers and gastric cancer, and its eradication represents a highly effective method to reduce the incidence and mortality of stomach cancer [9]. A study by Liu et al., focused on risk factors for H. pylori infection, identified age, higher total cholesterol level, lower albumin level, higher low density lipid (LDL) cholesterol level and higher fasting blood sugar level as factors increasing the chance of infection [10].
The results of a large study by Suki et al., show strongly significant differences in the prevalence of H pylori infection in relation to body mass index (BMI) [11]. According to the study by Kamada et al., the correlation between the presence of H. pylori and higher-degree obesity is refuted with the claim that individuals with H. pylori start gaining weight only after undergoing H. pylori eradication [12]. The study by Wu et al., showed an inverse relationship between higher BMI and the presence of H. pylori [13]. The study by Thjodleifsson et al., suggests that H. pylori only accompanies insulin resistance and obesity, while not being related to systemic inflammation [14,15]. Therefore, the association between a higher degree of obesity (or BMI) and the presence of H. pylori in the human body is still considered a controversial topic [16].
This article aims (1) to summarize the knowledge on the prevalence of H. pylori in the obese individuals compared to normal-weight population, and to organize the information gained in this area over the last 20 years. Furthermore, we aim (2) to provide readers with the prevalence of H. pylori in various worldwide.
Materials and Methods
Search strategy
A comprehensive literature search was conducted in the electronic databases Scopus, PubMed, and Web of Science between October 30, 2023, and December 23, 2023. The search strategy combined terms related to Helicobacter pylori and body mass index (BMI). Representative search terms included: [“relation between BMI and Helicobacter pylori,” “obesity and Helicobacter pylori,” and “Helicobacter pylori epidemiology in world populations.”].
Inclusion criteria
Studies were eligible for inclusion if they met the following criteria: (1) Contained predefined keywords related to H. pylori and BMI; (2) Investigated the prevalence of H. pylori infection in relation to BMI in human participants; (3) Were original research articles published between 2005 and 2023; (4) Were written in English.
Exclusion criteria
The following records were excluded: (1) Duplicates retrieved from multiple databases; (2) Non-original works such as book chapters, brochures, or conference proceedings; (3) Studies not directly focused on the prevalence of H. pylori in relation to BMI; (4) Studies that did not clearly describe the diagnostic method for H. pylori detection or lacked sufficient methodological detail; (5) Animal studies.
Results
The initial search identified 1109 records. After removal of duplicates (n=392), 717 unique records remained. Of these, 710 were excluded for not meeting the eligibility criteria, leaving seven articles for final inclusion in the analysis. The study selection process is summarized in Figure 1 (flow diagram).
All seven included studies aimed to investigate the prevalence of H. pylori in overweight/obese and normal-weight people in various regions of the world. Further details of the included studies are shown in Table 1. The oldest study was published in 2005, the most recent in 2022. The studies differed in the number of respondents, with the smallest cohort consisting of 214 individuals (61.2 % male) and the largest of 235107 individuals (35.9 % male). They also differed in the detection method used to determine the presence of H. pylori infection, with four authors using Enzyme-Linked Immunosorbent Assay (ELISA), two using urea breath test (UBT) and one using endoscopy.
The studies did not have the same criteria for selecting obese participants between them, but 71.4 % of the studies included individuals with a BMI>30. Among these studies, the most commonly used method for the detection of H. pylori was the Enzyme-Linked Immunosorbent Assay (ELISA) method, which represents a simple, sensitive, rapid, reliable and versatile test for quantification of antigens and antibodies, and is done from blood serum. It is useful due to the extreme distinguishing ability of antibodies to recognize an almost infinite number of antigenic structures [17]. The second most used method across included studies was the urea breath test (UBT). The UBT is a non-invasive method of detecting H. pylori with high specificity and sensitivity, and is performed from exhaled air. However, the specificity of this test is decreased if other urease-producing bacteria are present in the intestine of the subject [18]. Endoscopic examination/Endoscopic resection, used in one study, allows the collection of a representative sample for definitive histopathological evaluation, which may also refine the diagnosis, including the assessment of the depth of invasion [19]. The study by Suki et al., with the largest cohort consisted of 32824 subjects with higher BMI, revealed the strong association between H. pylori infection and BMI, while the prevalence in obese subjects was 65 % [11]. The study by Arslan et al., had the smallest cohort with 103 participants with higher BMI, and the prevalence in obese subjects was 57.2 % [16].
In all of these studies, the study population was predominantly from countries located on the Asian continent, so we do not have sufficient information to compare this trend in, e.g., Europe. The selected studies compared a study group of subjects with normal BMI (normal-weight individuals) with a group with higher BMI, and investigated the possible difference between the obese and normal-weight individuals. The values at Figure 2 below represent the odds ratios of seven selected studies and describe the relationship between the prevalence of H. pylori infection and higher BMI.
The average prevalence in the entire study cohorts was 55.17±7.09 %. The minimum prevalence was 41.5 % and the maximum was 62.40 % [16,26]. The mean prevalence in the obese groups was 63.66±13.11 %, with minimum prevalence of 43.7 % and maximum 80.60 % [13,20]. According to the conclusions of the 71.4 % included studies, the prevalence of H. pylori is significantly higher in the obese individuals compared to those with normal weight, and to general population. A different conclusion was found in a study by Xu et al., which observed no significant difference between these groups [21].
The oldest study by Wu et al. reported completely different conclusions. In this study, authors found an inverse relationship between obese and normal-weight participants, i.e., suggested that obesity may act as a protective factor for the H. pylori infection [13].
The method used to detect H. pylori varied across studies, however, it did not play a primary significant role in the difference between groups. Another factor that may have influenced the results, was the nationality of the study population. Studies in Chinese, Israeli, Turkish, Pakistani, Saudi Arabian and Taiwanese populations have shown different results in the association of H. pylori between overweight/obese and normal-weights individuals, as well as in prevalence of general population.
Although the authors found very interesting results, research in this area is still insufficient. Further in-depth research is needed to better understand the BMI-HP relationship.
Discussion
Helicobacter pylori remains a widespread infection with significant clinical consequences, including its well-known role in chronic gastritis, peptic ulcers, and gastric cancer. Although the World Health Organization classifies H. pylori as a Group 1 carcinogen, the relationship between H. pylori infection and body mass index (BMI) is complex and not yet fully understood.
The seven studies reviewed here present fairly consistent findings regarding the association between BMI and H. pylori prevalence. Early studies, such as Wu et al., suggested a potential protective effect of higher BMI against H. pylori infection. However, the year of publication (2005) of this study may play a role, as the other included studies were published in time period 2009–2022. Another factor possibly affecting the findings of this one study, may be that it is not reported, whether the study subjects had already undergone eradication for H. pylori before the study [13]. More recent research, including Suki et al., reported a significant positive association, suggesting that obesity may increase the risk of H. pylori infection. These conflicting results are likely due to differences in study design, diagnostic methods (including but not limited to ELISA, urea breath tests, and endoscopy), and varying population characteristics, such as age, geographic region, diet, and socioeconomic factors. A systematic review and meta-analysis by Hooi et al. that looked at the prevalence of H. pylori in 62 countries revealed that there are huge differences in the prevalence of this bacteria between countries [23]. The prevalence of H. pylori ranged from 18.9 % (Switzerland) to 87.7 % (Nigeria), and based on prevalence estimates, it was found that approximately 4.4 billion people were infected with H. pylori in 2015, meaning that more than half of the world’s population was infected with H. pylori [23]. A systematic review by Peleteiro et al. including studies from 1968–2013 looked at the prevalence of H. pylori in 22 countries – 5 countries from South and North America, 6 countries from Asia, 10 countries from Europe and 1 country from Oceania (Australia) [24]. It notes that the prevalence is generally higher in countries in North/South America and Asia, especially compared to Europe [24]. For example study by Bureš et. al. showed that the overall prevalence of H. pylori infection in the czech population is 23.5 %. The overall prevalence of H. pylori in the Czech Republic, central Europe, has declined significantly over the past 10 years, from 41.7 % in 2001 to 23.5 % in 2011 [28]. At the same time, the prevalence was found to be almost twice as high in countries with a high incidence of stomach cancer. According to this review, there is also a possible correlation between the age of individuals and H. pylori infection, with the risk of infection increasing with increasing age [24].
In addition, the association with H. pylori may be mediated by the presence of metabolic comorbidities, such as dyslipidemia, insulin resistance, and hypertension, which are frequently observed in individuals with obesity. This complex interaction makes it difficult to establish a direct cause-and-effect relationship and emphasizes the importance of using analytical methods that account for these possible confounding factors.
Regional differences in H. pylori prevalence further highlight the influence of environmental and lifestyle factors. For example, prevalence may be affected by genetic predispositions or region-specific dietary habits. Socioeconomic status and living conditions also modify the risk of exposure, as reflected by the globally observed differences in prevalence between developing and developed countries.
Given the inconsistencies and limitations of current research, future studies should adopt standardized diagnostic criteria and methodologies to improve comparability. Moreover, multinational cohort studies with comprehensive data on metabolic health, environmental exposures, and genetic factors are needed to clarify the relationship between BMI and H. pylori and to inform targeted prevention and treatment strategies.
Conclusions
The prevalence of Helicobacter pylori infection varies considerably by country, region, and socioeconomic status, with developing countries generally exhibiting higher rates than developed ones. Whether obesity is an independent risk factor for H. pylori infection remains unclear. Most studies suggest that individuals with higher BMI tend to have a higher prevalence compared to normal-weight individuals, although results are not fully consistent. These inconsistencies may be influenced by differences in study design and population characteristics. Further research using standardized diagnostic methods and diverse populations is necessary to clarify the relationship between BMI and H. pylori infection and its clinical significance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ng M Fleming T Robinson M Thomson B Graetz N Margono C Mullany EC Global, Regional, and National Prevalence of Overweight and Obesity in Children and Adults during 1980–2013: A Systematic Analysis for the Global Burden of Disease Study 2013 Lancet 201438476678110.1016/S 0140-6736(14)60460-824880830 PMC 4624264 · doi ↗ · pubmed ↗
- 2Morshed AB Kasman M Heuberger B Hammond RA Hovmand PSA Systematic Review of System Dynamics and Agent-Based Obesity Models: Evaluating Obesity as Part of the Global Syndemic Obes Rev 201920 Suppl 216117810.1111/obr.1287731317637 · doi ↗ · pubmed ↗
- 3Swinburn BA Kraak VI Allender S Atkins V Baker PI Bogard JR Brinsden H The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission Report Lancet 201939379184610.1016/S 0140-6736(18)32822-830700377 · doi ↗ · pubmed ↗
- 4O’Connor AO’Morain CA Ford AC Population Screening and Treatment of Helicobacter pylori Infection Nat Rev Gastroenterol Hepatol 20171423024010.1038/nrgastro.2016.19528053340 · doi ↗ · pubmed ↗
- 5Chey WD Leontiadis GI Howden CW Moss SFACG Clinical Guideline: Treatment of Helicobacter pylori Infection Am J Gastroenterol 201711221223910.1038/ajg.2016.56328071659 · doi ↗ · pubmed ↗
- 6Wang F Meng W Wang B Qiao L Helicobacter pylori-Induced Gastric Inflammation and Gastric Cancer Cancer Lett 201434519620210.1016/j.canlet.2013.08.01623981572 · doi ↗ · pubmed ↗
- 7Dharan M Wozny D Helicobacter pylori Infection and Small Intestinal Bacterial Overgrowth - More than What Meets the Eye World J Clin Cases 2022107209721410.12998/wjcc.v 10.i 21.720936158005 PMC 9353905 · doi ↗ · pubmed ↗
- 8Muhammad JS Zaidi SF Sugiyama T Epidemiological Ins and Outs of Helicobacter pylori: A Review J Pak Med Assoc 20126295595923139983 · pubmed ↗