Associations between appetite loss and psychopathology as well as gender differences in adolescents with major depressive disorders
Jinyue Xue, Lewei Liu, Jingwen Shang, Yachen Feng, Xianlin Sun, Jiawei Wang, Changhao Chen, Zhiwei Liu, Feng Geng, Daming Mo, Xiangfen Luo, Xiangwang Wen, Lei Xia, Huanzhong Liu

TL;DR
This study finds that appetite loss is common in adolescents with depression, especially girls, and is linked to symptoms like sleep issues and depression severity.
Contribution
The study identifies gender-specific associations between appetite loss and clinical symptoms in adolescents with major depressive disorders.
Findings
Appetite loss was independently associated with gender, BMI, depression severity, and insomnia in adolescents with MDD.
Female patients showed stronger associations between appetite loss and BMI, depression severity, and insomnia compared to males.
Combining clinical factors improved prediction of appetite loss, with better accuracy in females than males.
Abstract
Appetite loss is frequent in patients with major depressive disorders (MDD). However, research on the association between appetite loss and psychopathology symptoms in adolescents with MDD remains limited, particularly regarding gender differences. Therefore, this study aimed to explore these associations and potential gender differences. A cross-sectional study carried out between January to December 2021 in eight hospitals, recruiting 364 adolescents with MDD. It utilized the Hamilton Depression Scale (HAMD), the Positive and Negative Suicide Ideation Scale for Adolescents (PANSI), the Chinese version of the Epworth Sleepiness Scale (ESS), the Insomnia Severity Index (ISI), and the Chinese version of the Internet Addiction Test (IAT) to assess patients’ depressive severity, suicidal ideation, sleepiness, insomnia, and internet addiction, respectively. Logistic regression was employed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
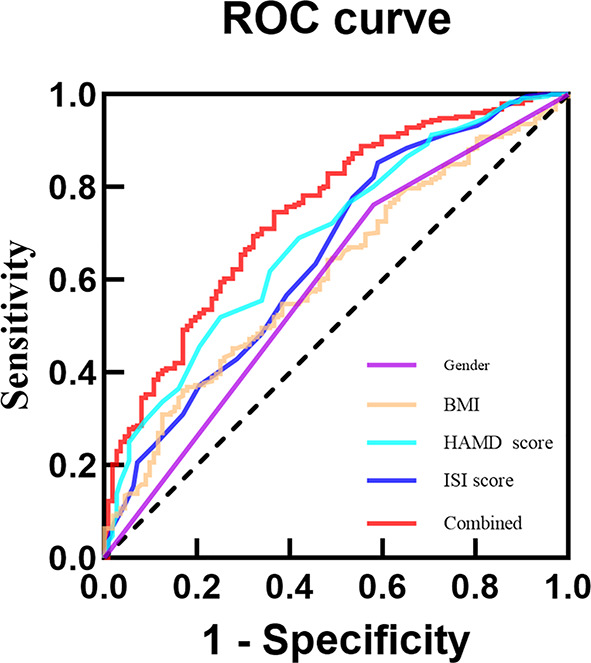 Figure 1
Figure 1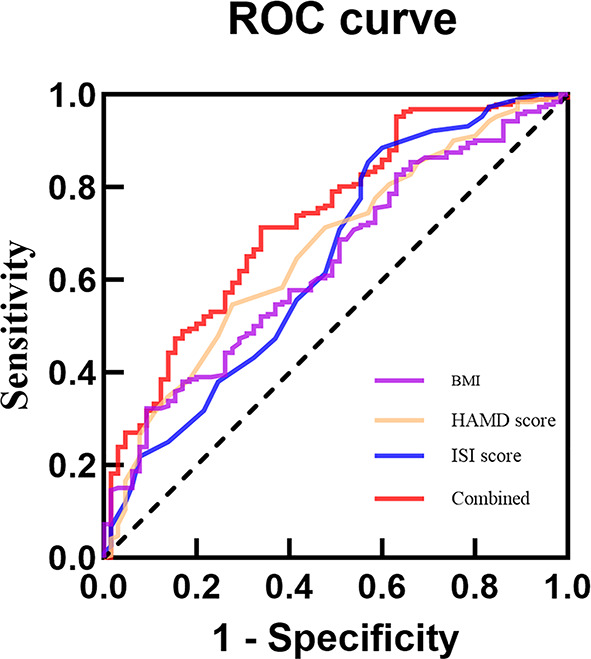 Figure 2
Figure 2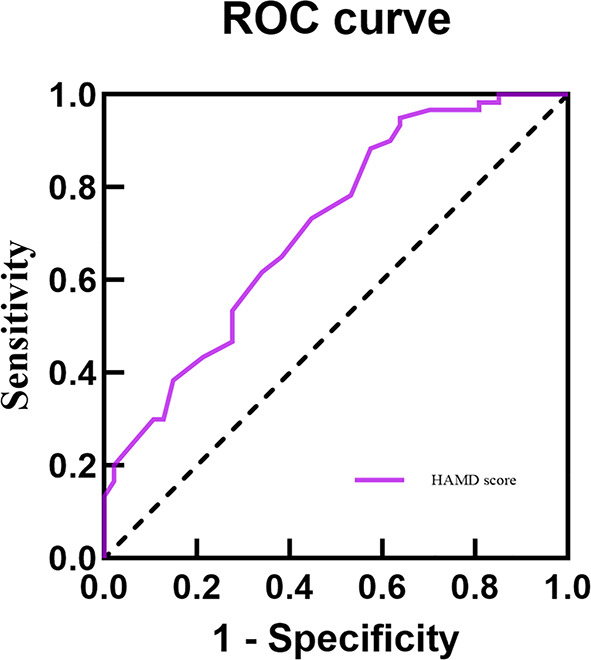 Figure 3
Figure 3- —the National Natural Science Foundation of China
- —the Research Fund Project of Anhui Translational Research Institute
- —the Scientifc Research Project of Anhui Higher Education Institutions
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEating Disorders and Behaviors · Sleep and related disorders · Body Image and Dysmorphia Studies
Introduction
Major depressive disorder (MDD) is a frequent and serious mental disease in adolescents [1]. A Chinese epidemiological study showed that the prevalence of MDD in adolescents has reached 2.0% [2]. MDD not only affected the emotional state of adolescents, but was often accompanied by a range of somatic symptoms, in which changes in appetite are more common [3]. Appetite loss was frequently associated with depression, and a previous study showed that approximately half of patients with MDD experienced appetite loss [4]. Adolescents are still developing physically and mentally, and patients with MDD during this stage are more prone to eating disorders (ED) due to impaired emotions, cognition, and self-control [5]. However, despite previous studies investigating appetite loss in patients with MDD, research specifically targeting adolescents with MDD remains scarce. Given that appetite loss may impact treatment adherence and overall recovery, its prevalence and associated factors in adolescents with MDD warrant further investigation.
Research has indicated that appetite loss was strongly linked to a variety of psychopathological symptoms. For example, research has found that when adolescents experienced depressive moods, their eating behaviors were also influenced by these moods [6]. Another investigation showed that patients with appetite loss usually manifested more pronounced symptoms of depression [7]. There was also study that have found a correlation between appetite loss and suicidal ideation (SI) [8]. Additionally, studies have shown that excessive internet use may increase the risk of developing anorexia nervosa by causing adolescents to develop distorted body image [9, 10]. Notably, most of the aforementioned studies have focused on adults or individuals with anorexia nervosa, while research on adolescents with MDD remains insufficient.
Importantly, gender differences in these associations may exist, potentially arising from a multifaceted interplay of physiological, psychological, and sociocultural factors. For example, a 4-year longitudinal investigation revealed that female adolescents with MDD were more prone to developing ED than males, driven by factors such as body dissatisfaction, depressive symptoms, body mass index (BMI), and perfectionism [11]. Another clinical study further revealed that depression tends to be more severe when BMI was at lower levels in patients with chronic anorexia nervosa [12]. Females’ risk of depression appears to be more strongly influenced by changes in BMI. They often exhibit heightened concerns about their self-image and frequently resort to extreme dietary control to manage their weight, which not only exacerbates their psychological burden but also increases the risk of developing anorexia nervosa in the future [13, 14]. In addition, insomnia in females was also associated with appetite loss. A community-based study showed that females reported more appetite loss than males due to poor sleep [15]. Nonetheless, research on gender differences in the associations between appetite loss and a variety of psychopathological symptoms in adolescents with MDD remains relatively limited and warrants further in-depth exploration.
The above studies have shown that appetite loss may be linked with various factors, and that these factors differ across genders. However, existing studies have not systematically explored the potential mechanisms underlying these connections in adolescents with MDD. In particular, possible gender differences have been largely overlooked. Therefore, the study sought to investigate the associations between appetite loss and psychopathology in this population, including depressive severity, SI, sleepiness, insomnia, and Internet addiction (IA), as well as gender differences in these associations.
Methods
Participants
This study employed a multi-site, convenience-consecutive sampling method from January to December 2021, selecting adolescent patients with MDD from outpatient and inpatient departments across eight hospitals covering northern, central, and southern Anhui Province (the Fourth Affiliated Hospital of Anhui Medical University, the Fourth People’s Hospital of Hefei, the Second Affiliated Hospital of Anhui Medical University, Bozhou People’s Hospital, Suzhou Second People’s Hospital, Second Affiliated Hospital of Bengbu Medical University, Ma’anshan Fourth People’s Hospital, and Fuyang Third People’s Hospital). This approach ensured sample representativeness and minimized regional bias. All Participants were enrolled by qualified, board-certified psychiatrists or higher-level mental health specialists using DSM-5 criteria and standardized assessment tools. Evaluators from eight centers underwent centralized training, and all treatments were administered according to clinical guidelines. Inclusion criteria: (1) aged 12 to 18 years old, with adequate reading comprehension ability; (2) meeting the diagnostic criteria for MDD as defined in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5), and independently diagnosed by two psychiatrists with the title of attending physician or above; (3) After obtaining written informed consent from the parent or legal guardian, and confirming through one-on-one communication that the subject fully understands the process, the subject voluntarily signs the informed consent form. Exclusion Criteria: (1) Diagnosed with schizophrenia, bipolar disorder, intellectual disability, or other mental disorders according to DSM-5; (2) Presence of severe infection, organic brain disease, autoimmune disease, or other major physical illnesses (e.g., gastrointestinal disorders, endocrine abnormalities or chronic diseases); (3) Use within the past 4 weeks of medications that may affect appetite, including but not limited to prokinetic agents, appetite suppressants, or appetite stimulants. In this study, the sample size was initially calculated using the formula n = Z²p(1-p)/d². Here, n represents the sample size, Z is the value corresponding to the 95% confidence interval (which was 1.96), d denotes the marginal error (which was set at 0.05), and p is the prevalence (Based on previous literature, approximately 65% of patients with MDD experienced appetite loss. Therefore, we set the p-value to 65% [16]). The minimum sample size obtained was 350. Finally, this study recruited 364 adolescents with MDD. The average age of all patients was 15.25 ± 1.63 years, their age at onset was 13.75 ± 3.64 years, duration of illness was 20.68 ± 16.91 months, and 70.6% of the patients were female (Table 1).
Table 1. Comparison of sociodemographic and psychopathological data of patients in the appetite loss and non-appetite loss groups in the total sampleVariablesTotal sample(N = 364)Appetite loss(N = 252)Non-appetite loss (N = 112)t/Z/χ^2^ p Cohen’s dAge (years), mean (SD)15.25 ± 1.6315.19 ± 1.6415.40 ± 1.601.1660.2440.132Gender, n (%) Males107 (29.40)60 (23.81)47 (41.96)12.314 0.001* 0.132 Females257 (70.60)192 (76.19)65 (58.04)BMI (kg/m^2^), mean (SD)21.22 ± 4.4020.80 ± 4.3822.17 ± 4.312.759 0.006 0.313Age at onset (years), mean (SD)13.75 ± 3.6413.68 ± 4.1413.91 ± 2.120.5520.5810.063Duration of illness (moths), median (P_25_, P_75_)15.00(8.00,27.00)18.00(12.00,31.50)12.00(6.00,24.00)1.372 ^a^ 0.020 0.072Antidepressants, n (%) None132(36.26)95(37.70)37(33.04)2.0040.367 SSRIs203(55.77)140(55.56)63(56.25)0.074 Others29(7.97)17(6.75)12(10.71)Study pressure, n(%) Small20(5.49)14 (5.56)6(5.36)3.2240.119 Average141(38.74)90 (35.71)51(45.54)0.094 Large203(55.77)148 (58.73)55(49.11)HAMD score, mean (SD)26.84 ± 7.6828.46 ± 7.0223.18 ± 7.86-6.387 < 0.001* 0.725PANSI score, mean (SD)47.91 ± 11.9049.61 ± 11.0744.09 ± 12.84-4.178 < 0.001* 0.474ESS score, mean (SD)9.49 ± 4.589.25 ± 4.6210.04 ± 4.441.5400.1240.175ISI score, mean (SD)12.45 ± 5.8713.48 ± 5.4710.12 ± 6.08-5.021 < 0.001* 0.594IAT score, mean (SD)51.68 ± 15.6252.30 ± 16.0150.30 ± 14.68-1.1240.2620.128BMI, body mass index; SSRIs, selective serotonin reuptake inhibitors; HAMD, Hamilton depression scale; PANSI, positive and negative suicide ideation inventory scale; ESS, Epworth sleepiness scale; ISI, insomnia severity index scale; IAT, internet addiction testBolded p value: < 0.05; SD: standard deviation^a^ Mann-Whitney U-test. Cohen’s d indicates the effect size* indicated variables with p < 0.05 after FDR adjustment
This study was approved by the Ethics Committee of the Fourth Affiliated Hospital of Anhui Medical University (202009-kyxm-04). Furthermore, all procedures conformed to the ethical standards of the 2013 version of the Helsinki Declaration (https://www.wma.net/policies-post/wma-declaration-of-helsinki/). Written informed consent was obtained from all participants and their legal guardians after they were fully informed about the study.
Study instruments
Sociodemographic information
We collected detailed sociodemographic information from study participants by distributing self-administered questionnaires, including age, gender, BMI, academic stress, age at onset, duration of illness, and use of antidepressant medication.
Depressive
The Hamilton Depression Scale (HAMD) was used to assess the degree of patients’ depressive symptoms over the past week [17]. The scale includes 24 items and uses a 5-point rating system, and it has higher total scores being associated with greater severity of depressive symptoms. And HAMD has been widely used in studies of adolescents with MDD [18]. Based on previous research, the present study categorized patients according to their HAMD item 12 (gastrointestinal symptoms) scores. Participants scoring 0 points were defined as the non-appetite loss group (n = 112), while those scoring 1 or 2 points were defined as the appetite loss group (n = 252) [16]. To avoid potential confounding effects of this item, Item 12 was excluded when analyzing the correlation between depressive symptoms (assessed by HAMD-24) and appetite loss.
SI
The Positive and Negative Suicidal Ideation Scale (PANSI) was used to assess the degree of SI in subjects over the past two weeks [19]. The scale includes 14 items and uses a 5-point rating system, with higher total scores reflecting more severe SI. The Chinese version of PANSI has been widely used in Chinese adolescents with MDD [20].
Daytime sleepiness symptoms
The Chinese version of the Epworth Sleepiness Scale (ESS) was used to assess the degree of daytime sleepiness symptoms in different situations [21]. The scale includes 8 items and uses a 3-point rating system, with higher scores reflecting more severe sleepiness. The ESS scale has good reliability and validity in the Chinese population [22].
Insomnia
The Insomnia Severity Index (ISI) includes 7 items to assess the degree of insomnia over the past two weeks [23]. The scale uses a 5-point rating system, with higher scores reflecting more severe insomnia. The ISI scale has been widely used in adolescents with MDD [24].
IA
The Chinese version of the Internet Addiction Test (IAT) was used to measure IA [25]. The scale includes 20 items and uses a 5-point rating scale, with higher scores reflecting more severe IA [26]. Previous study has shown that the Chinese version of the IAT was reliable and valid for adolescents [27].
Statistical analysis
Perform statistical analysis using SPSS23.0. The Kolmogorov-Smirnov test assessed normality of continuous variables. Continuous variables with normal distribution were summarized as mean ± standard deviation (SD), and t-test was used for comparison between groups; measures with non-normal distribution were expressed as M (P_25_, P_75_), and Mann-Whitney U-test was used for comparison between groups. Categorical variables were presented as percentages (%), and the chi-square tests were used for comparison between groups. In multifactorial analyses, stepwise logistic regression analysis was used to identify independent factors associated with appetite loss in adolescents with MDD. Finally, the area under the curve (AUC) was calculated using the receiver operating characteristic (ROC) curve to evaluate the predictive value of each independent factor for appetite loss. Two-sided tests were employed for all statistical analyses, with a significance level set at p < 0.05.
Results
Comparison of sociodemographic and psychopathological data
In the total sample, the prevalence of appetite loss in adolescents with MDD was 69.2%, with 74.7% in females and 56.1% in males. The results of univariate analysis showed that compared to the non-appetite loss group, patients with appetite loss had a lower BMI (t = 2.759, p = 0.006), longer duration of illness (t = 1.372, p = 0.020), and higher scores of HAMD (t = -6.387, p < 0.001), PANSI (t = -4.178, p < 0.001) and ISI (t = -5.021, p < 0.001) (Table 1).
Gender differences between sociodemographic and psychopathological data
Tables 2 and 3 summarized the results of univariate analysis in female and male patients, respectively. In female patients, the scores of HAMD, PANSI and ISI were significantly higher in the appetite loss group than in the non-appetite loss group (p < 0.05), while BMI and ESS score was significantly lower in the appetite loss group than in the non-appetite loss group (p < 0.05). In male patients, the appetite loss group had higher scores of HAMD, PANSI, ISI and IAT (p < 0.05).
Table 2. Comparison of sociodemographic and psychopathological data in the appetite loss and non-appetite loss groups in female patientsVariablesAppetite loss(N = 192)Non-appetite loss (N = 65)t/Z/χ^2^ p Cohen’s dAge (years), mean (SD)15.01 ± 1.6915.12 ± 1.600.4710.6380.068BMI (kg/m2), mean (SD)20.20 ± 3.4221.90 ± 4.163.271 0.001* 0.469Age at onset (years), mean (SD)13.26 ± 1.8613.49 ± 2.160.8320.4060.119Duration of illness (moths), median (P_25_, P_75_)18.00 (12.00, 35.00)12.00 (6.00, 24.00)1.161 ^a^0.0590.072Antidepressants, n (%) None68 (35.42)19 (29.23)0.8590.651 SSRIs109 (56.77)40 (61.54)0.058 Others15 (7.81)6 (9.23)Study pressure Small8 (4.17)5 (7.69)5.5560.062 Average67 (34.90)31 (47.69)0.147 Large117 (60.94)29 (44.62)HAMD score, mean (SD)28.64 ± 7.1424.25 ± 7.80-4.182 < 0.001* 0.600PANSI score, mean (SD)50.40 ± 11.0146.14 ± 13.71-2.268 0.026 0.362ESS score, mean (SD)9.17 ± 4.6610.62 ± 4.742.157 0.032 0.309ISI score, mean (SD)13.49 ± 5.5210.18 ± 6.46-3.694 < 0.001* 0.573IAT score, mean (SD)51.33 ± 15.7350.85 ± 16.43-0.2110.8330.030BMI, body mass index; SSRIs, selective serotonin reuptake inhibitors; HAMD, Hamilton depression scale; PANSI, positive and negative suicide ideation inventory scale; ESS, Epworth sleepiness scale; ISI, insomnia severity index scale; IAT, internet addiction testBolded p value: < 0.05; SD: standard deviation^a^ Mann-Whitney U-testCohen’s d indicates the effect size* indicated variables with p < 0.05 after FDR adjustment
Table 3. Comparison of sociodemographic and psychopathological data in the appetite loss and non-appetite loss groups in male patientsVariablesAppetite loss(N = 60)Non-appetite loss(N = 47)t/Z/χ^2^ p Cohen’s dAge (years), mean (SD)15.75 ± 1.3415.79 ± 1.530.1340.8940.026BMI (kg/m^2^), mean (SD)22.72 ± 6.2422.54 ± 4.54-0.1690.8660.033Age at onset (years), mean (SD)15.03 ± 7.6914.49 ± 1.93-0.4730.6370.092Duration of illness (moths), median (P_25_, P_75_)20.00 (6.25, 30.00)12.00 (4.00, 24.00)0.710 ^a^0.4630.069Antidepressants, n (%) None27(45.00)18 (38.30)3.4570.178 SSRIs31(51.67)23 (48.94)0.180 Others2 (3.34)6 (12.77)Study pressure Small6 (10.00)1 (2.13)2.6790.262 Average23 (38.33)20 (42.55)0.158 Large31 (51.67)26 (55.32)HAMD score, mean (SD)27.92 ± 6.6321.70 ± 7.79-4.455 < 0.001* 0.868PANSI score, mean (SD)47.10 ± 10.9541.26 ± 11.06-2.728 0.007 0.531ESS score, mean (SD)9.50 ± 4.529.26 ± 3.90-0.2950.7690.057ISI score, mean (SD)13.45 ± 5.3810.02 ± 5.58-3.219 0.002* 0.627IAT score, mean (SD)55.40 ± 16.6249.55 ± 11.98-2.113 0.037 0.396BMI, body mass index; SSRIs, selective serotonin reuptake inhibitors; HAMD, Hamilton depression scale; PANSI, positive and negative suicide ideation inventory scale; ESS, Epworth sleepiness scale; ISI, insomnia severity index scale; IAT, internet addiction testBolded p value: < 0.05; SD: standard deviation^a^ Mann-Whitney U-testCohen’s d indicates the effect size* indicated variables with p < 0.05 after FDR adjustment
Independent factors associated with appetite loss
In the total sample, the results showed that Gender (OR = 0.559, 95% CI = 0.331 ~ 0.944, p = 0.029), BMI (OR = 0.925, 95% CI = 0.876 ~ 0.977, p = 0.005), HAMD score (OR = 1.080, 95% CI = 1.041 ~ 1.120, p < 0.001) and ISI score (OR = 1.073, 95% CI = 1.024 ~ 1.124, p = 0.003) were independent correlated of appetite loss in adolescents with MDD. In female patients, BMI (OR = 0.872, 95% CI = 0.806 ~ 0.945, p = 0.001), HAMD score (OR = 1.062, 95% CI = 1.016 ~ 1.110, p = 0.008) and ISI score (OR = 1.077, 95% CI = 1.017 ~ 1.141, p = 0.012) were independently associated with appetite loss. In male patients, only HAMD score (OR = 1.133, 95% CI = 1.062 ~ 1.209, p < 0.001) was independently associated with appetite loss (Table 4).
Table 4. Independent factors associated with appetite loss by multivariate Stepwise logistic regression analysisVariablesβSDWald χ^2^OR95% CI p Total sample Gender-0.5810.2674.7390.5590.331 ~ 0.944 0.029 BMI-0.0780.0287.7330.9250.876 ~ 0.977 0.005 HAMD score0.0770.01917.1291.0801.041 ~ 1.120 < 0.001 ISI score0.0700.0248.8681.0731.024 ~ 1.124 0.003 Female BMI-0.1360.04111.2970.8720.806 ~ 0.945 0.001 HAMD score0.0600.0236.9771.0621.016 ~ 1.110 0.008 ISI score0.0740.0296.3411.0771.017 ~ 1.141 0.012 Male HAMD score0.1250.03314.1621.1331.062 ~ 1.209 < 0.001 BMI, body mass index; HAMD, Hamilton depression scale; ISI, insomnia severity index scale Bolded p value: < 0.05; SD: standard deviationOR, odds ratio; CI, confidence interval
ROC curve analysis of appetite loss
This study conducted ROC curve analysis to explore the predictive value of independent factors for appetite loss. In the total sample, the results showed that the AUC values for Gender, BMI, HAMD score and ISI score in predicting appetite loss in adolescents with MDD were 0.591, 0.612, 0.689 and 0.652, respectively. Additionally, when these four indicators were combined, the AUC value increased, indicating improved predictive ability for appetite loss (AUC = 0.746, 95% CI = 0.692 ~ 0.800), with enhanced sensitivity and specificity compared to individual indicators (Table 5; Fig. 1). In female patients, the AUC values for BMI, HAMD score and ISI score alone in predicting appetite loss in adolescents with MDD were 0.636, 0.665 and 0.642, respectively. Combining these four indicators y increased the AUC value to 0.732, sensitivity of 71.4% and specificity 66.2% (Table 5; Fig. 2). HAMD score alone predicted appetite loss in male adolescents with MDD with an AUC value of 0.713, sensitivity of 95.0%, and a specificity of 36.2% (Table 5; Fig. 3).
Fig. 1ROC curve analysis of appetite loss in adolescents with MDD in the total sample of Gender, BMI, HAMD score and ISI score
Fig. 2ROC curve analysis of BMI, HAMD score and ISI score on appetite loss in female adolescents with MDD
Fig. 3ROC curve analysis of HAMD score on appetite loss in male adolescents with MDD
Table 5ROC curve analysis of appetite loss in adolescents with MDDVariablesAUC95% CISensitivity(%)Specificity(%) p Total sample Gender0.5910.526 ~ 0.6560.7620.420 0.006 BMI0.6120.551 ~ 0.6730.3610.830 0.001 HAMD score0.6890.631 ~ 0.7470.6910.580 < 0.001 ISI score0.6520.590 ~ 0.7150.8530.411 < 0.001 Combination0.7460.692 ~ 0.8000.7460.634 < 0.001 Female BMI0.6360.560 ~ 0.7110.3230.908 0.001 HAMD score0.6650.590 ~ 0.7400.5470.723 < 0.001 ISI score0.6420.560 ~ 0.7240.8850.400 0.001 Combination0.7320.661 ~ 0.8110.7140.662 < 0.001 Male HAMD score0.7130.615 ~ 0.8460.9500.362 < 0.001 BMI, body mass index; HAMD, Hamilton depression scale; ISI, insomnia severity index scale; AUC, area under curveBolded p value: < 0.05; OR, odds ratio; CI, confidence interval
Discussion
In this study the results showed that the prevalence of appetite loss in adolescents with MDD was 69.2%, higher than that of adult patients (56.5%) [16]. In terms of gender differences, female patients exhibited a higher incidence rate (74.7%), contrasting with that observed in male patients (56.1%). Currently, the mechanisms underlying gender differences in appetite loss remain incompletely understood. However, relevant study suggested these disparities may relate to gender-specific hormonal variations and differing coping strategies for depressive emotions [28]. Additionally, women often face greater societal pressure regarding body image due to cultural aesthetic standards (e.g.,“thinness equals beauty”) [29]. This dissatisfaction and anxiety about body shape may also be associated with appetite loss [30]. For example, Ferreiro’s research indicated that appetite loss in many adolescent females was linked to dissatisfaction with their body shape [11]. Furthermore, this study found that appetite loss was correlated with lower BMI values, consistent with previous finding in adults [31]. This phenomenon occurring more frequently in females may also be related to their excessive focus on their own body shape. However, future large-scale cohort studies are needed to systematically investigate gender differences in appetite loss in adolescents with MDD, the gender specificity of the association between appetite loss and BMI, and whether such differences persist into adulthood.
In terms of clinical symptoms, appetite loss was associated with the severity of depressive symptoms, previous studies have also yielded consistent results [7, 32]. This association involves multiple potential mechanisms, including psychological and neurobiological mechanisms. First, from a psychological mechanism perspective, depression often manifests as anhedonia, where diminished pleasure from food may trigger avoidance of eating behaviors [33, 34]. Additionally, adolescents with MDD frequently experience emotional dysregulation, which can contribute to the emergence of eating issues [35]. Harrison’s research further revealed that patients with MDD commonly exhibit negative cognitive biases, holding pessimistic views about themselves, their environment, and the future [36]. These negative cognitions may be linked to diminished interest in food; when patients develop the belief that “eating cannot improve mood or bring pleasure” they may experience appetite loss. From a neurobiological perspective, this may also be associated with endocrine dysregulation in depressed individuals, such as abnormally elevated cortisol levels [4, 37].
This study found that appetite loss in patients may be correlated with SI, although the regression analysis did not show statistical significance. This result may be related to the potential influence of antidepressant medication on the association between the two. Studies on adolescent populations indicated that individuals with depression frequently exhibit higher rates of SI [38], and appetite loss can also serve as an early warning indicator for SI and self-harm behaviors [8]. Given the close association between appetite loss and depression, we hypothesize that adolescents with MDD frequently experience emotional distress. This not only heightens the risk of SI but may also diminish interest in food, leading to inadequate nutritional intake. Nutritional deficiencies may further impair physical functioning and psychological resilience, making it harder to cope with life stressors and challenges, thereby intensifying SI. Additionally, interpersonal theories suggested that individuals may perceive themselves as a burden to loved ones, and this sense of burden was closely associated with SI [39]. Adolescents with MDD may harbor similar cognitive patterns, attempting to reduce their perceived burden on the family by eating less. However, current research on the association between SI and appetite loss primarily focuses on individuals with ED. For instance, multiple studies reported relatively higher risks of SI among those with ED [40–42]. Therefore, the specific patterns and underlying mechanisms linking appetite loss to SI in adolescents with MDD require further validation through high-quality research.
Additionally, this study indicated that in adolescents with MDD, female patients exhibit an independent association between appetite loss and insomnia. Previous research has demonstrated that most adolescents with MDD have sleep disorders, usually manifested as insomnia symptoms such as difficulty falling asleep or staying asleep [43]. Current research on the association between appetite loss and insomnia remains predominantly focused on adult and elderly populations. For instance, study in adults has found a strong correlation between appetite loss and insomnia, with reduced sleep duration further amplifying the association between depressive symptoms and insomnia [44]. Studies in the elderly population further revealed that moderate-to-high risk of appetite loss was associated only with insomnia in female seniors [45, 46]. In patients with anorexia nervosa, women typically report more sleep-wake disturbances and difficulty falling asleep [47]. Regarding the mechanisms linking appetite loss and insomnia, research suggested this may involve interactions between orexin, sleep arousal and appetite regulation [48]. For instance, appetite loss may reduce intake of melatonin-rich foods. Melatonin, a hormone secreted by the pituitary gland that plays a role in the sleep-wake cycle, has been reported to enhance sleep efficiency [49]. It is important to note that while previous studies have explored the mechanisms linking sleep and appetite, these mechanisms remain unclear across different age groups and genders. In particular, there was a lack of research on gender-specific mechanisms underlying the association between appetite loss and insomnia in adolescents with MDD. Additionally, this study also found that appetite loss in female adolescent patients with MDD was negatively correlated with sleepiness levels (i.e., sleepiness was positively correlated with increased appetite), although regression analysis did not reveal statistically significant differences. This may be closely related to the small sample size in the female subgroup and insufficient statistical power. Similar findings have been reported in previous studies, such as study on adolescent populations indicated that higher sleepiness levels were associated with stronger food cravings [50]. Similar trends have been observed in adult study, where sleepiness usually accompanies increased appetite [51]. This suggested that the negative association between sleepiness and appetite loss may be consistent across age groups, though further validation is needed. Although our findings indicated that the link between appetite loss and insomnia/sleepiness was more pronounced in female patients, the lack of large adolescent samples with MDD specifically designed to validate this association underscores the need for future studies with expanded sample sizes to confirm both the association and the robustness of gender differences.
Finally, in male adolescents with MDD, IA may be associated with appetite loss, although regression analysis did not show statistical significance. This result may be related to insufficient sample size. A cross-sectional study of adolescents indicated that high-risk male internet users reported skipping meals, appetite loss, and irregular eating patterns more frequently than females [52]. This suggested potential gender differences in the association between internet usage patterns and appetite symptoms, though evidence for its mechanisms in the context of adolescents with MDD remains limited. Varchetta’s research also indicated that males typically engage more enthusiastically than females in internet activities such as gaming and esports [53]. Such behaviors require prolonged focus and sedentary periods, potentially reducing physical activity [54]. This, in turn, may indirectly appetite loss by affecting gastrointestinal function and metabolic rhythms. Based on this, we hypothesized that the association between internet addiction and appetite loss in male adolescents may be linked to sedentary behavior and decreased physical activity. However, current research has not thoroughly examined the specific mechanistic pathways underlying the “internet addiction—sedentary/reduced activity—appetite loss” sequence in adolescents with MDD. Exploration of other potential mechanisms, such as neurobiology, also remains limited. Additionally, mechanistic studies examining gender differences, particularly variations in this association between male and female adolescents with MDD, remain markedly insufficient. Therefore, future large-scale, prospective foundational research is essential to further explore this topic.
However, there were several limitations to this study. First, most patients in this study were taking antidepressants. The cross-sectional design cannot distinguish between drug effects and genuine associations, limiting causal inference. Furthermore, medications were only broadly categorized without specifying particular drugs, dosages, or treatment durations, potentially obscuring key associations or weakening the study’s findings. Future research should document detailed medication information and employ longitudinal designs to further validate the authenticity of these associations. Second, the research measurement tools and indicators were insufficiently refined. Appetite assessment relied solely on a single item from the HAMD, with data primarily based on self-reported information and lacking support from nutritional biomarkers or objective biochemical indicators. Future studies should adopt standardized scales combined with objective biochemical indicators to enhance the accuracy and reliability of results. Third, although this study’s sample originated from eight medical institutions in Anhui Province, both the overall and male subgroup sample sizes were limited. Furthermore, the sole focus on adolescents with MDD and the absence of adult controls may compromise the generalizability of results and hinder the identification of age-related differences. Future studies should expand sample sizes, conduct prospective studies or randomized controlled trials, and include adult controls to refine the design. Fourth, the exploration of gender difference mechanisms was insufficient, with related discussions lacking empirical support. Key indicators such as standardized body image assessment scales and hormone level testing were not incorporated. Subsequent studies should supplement these with appropriate assessment tools and physiological testing, systematically elucidating specific mechanisms through longitudinal data.
Conclusion
Adolescents with MDD, particularly females, faced a heightened risk of appetite loss. Additionally, appetite loss was significantly associated with multiple clinical symptoms, and these associations showed certain gender differences. Therefore, in clinical management, healthcare providers should pay attention to risk factors associated with anorexia, particularly gender differences. Furthermore, future research should include more high-quality prospective studies to provide deeper insights into the mechanisms underlying appetite loss in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mora F, Alvarez-Mon MA, Fernandez-Rojo S, Ortega MA, Felix-Alcantara MP, Morales-Gil I, Rodriguez-Quiroga A, Alvarez-Mon M, Quintero J. Psychosocial factors in adolescence and risk of development of eating disorders. Nutrients 2022;14(7). 10.3390/nu 14071481 PMC 900286835406094 · doi ↗ · pubmed ↗
- 2Hinojo-Lucena FJ, Aznar-Díaz I, Cáceres-Reche MP, Trujillo-Torres JM, Romero-Rodríguez JM. Problematic internet use as a predictor of eating disorders in students: a systematic review and meta-analysis study. Nutrients. 2019;11(9). 10.3390/nu 11092151 PMC 676989931505749 · doi ↗ · pubmed ↗
- 3Hyldelund NB, Byrne DV, Chan RCK, Andersen BV. The relationship between social anhedonia and perceived pleasure from food-an exploratory investigation on a consumer segment with depression and anxiety. Foods. 2022;11(22). 10.3390/foods 11223659 PMC 968957836429251 · doi ↗ · pubmed ↗
- 4Sander J, Moessner M, Bauer S. Depression, anxiety and eating disorder-related impairment: moderators in female adolescents and young adults. Int J Environ Res Public Health. 2021;18(5). 10.3390/ijerph 18052779 PMC 796748633803367 · doi ↗ · pubmed ↗
- 5Patel RS, Machado T, Tankersley WE. Eating disorders and suicidal behaviors in adolescents with major depression: insights from the US hospitals. Behav Sci (Basel). 2021;11(5). 10.3390/bs 11050078 PMC 815910334069446 · doi ↗ · pubmed ↗
- 6Liu S, Wang X, Zheng Q, Gao L, Sun Q. Sleep deprivation and central appetite regulation. Nutrients. 2022;14(24). 10.3390/nu 14245196 PMC 978373036558355 · doi ↗ · pubmed ↗
- 7Meng X, Li Y, Li S, Zhou Y, Gan RY, Xu DP, Li HB. Dietary sources and bioactivities of melatonin. Nutrients. 2017;9(4). 10.3390/nu 9040367 PMC 540970628387721 · doi ↗ · pubmed ↗
- 8Varchetta M, Tagliaferri G, Mari E, Quaglieri A, Cricenti C, Giannini AM, Martí-Vilar M. Exploring gender differences in internet addiction and psychological factors: a study in a Spanish sample. Brain Sci. 2024;14(10). 10.3390/brainsci 14101037 PMC 1150598839452049 · doi ↗ · pubmed ↗