Migration of Fish Bones to the Bile Duct Following Hepaticojejunostomy
Kenta Yoshida, Tsuyoshi Hayashi, Kazuki Hama, Ryo Ando, Haruka Toyonaga, Tatsuya Ishii, Toshifumi Kin, Masayo Motoya, Kuniyuki Takahashi, Yuko Omori, Satoshi Ota, Akio Katanuma

TL;DR
Fish bones can migrate to the bile duct after certain surgeries, causing issues that can be safely treated with endoscopic procedures.
Contribution
This study characterizes fish bone migration into the bile duct following hepaticojejunostomy and evaluates endoscopic treatment outcomes.
Findings
11 patients with fish bone migration in the bile duct were successfully treated with endoscopic removal.
Computed tomography reliably detected fish bones as high-density structures in the bile duct.
Single-balloon enteroscopy was effective for removing fish bones and associated biliary stones.
Abstract
Migration of fish bones into the bile duct is rare, but can cause bile duct stone formation or acute cholangitis. Herein, we examine the characteristics of this phenomenon. This single‐center, retrospective study enrolled patients with a history of fish bone extraction from the bile duct by an endoscopic procedure at our hospital between June 2016 and November 2023. Patient characteristics, treatment details, and clinical course were assessed from the electronic medical records. A total of 11 patients were enrolled, including 10 who underwent subtotal stomach‐preserving pancreaticoduodenectomy with Child's reconstruction and one who underwent extrahepatic bile duct resection with choledochojejunostomy. The median time between surgery and endoscopic treatment was 84 months (range 12–124). On computed tomography (CT), all fish bones were detected as high‐density dots or linear…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
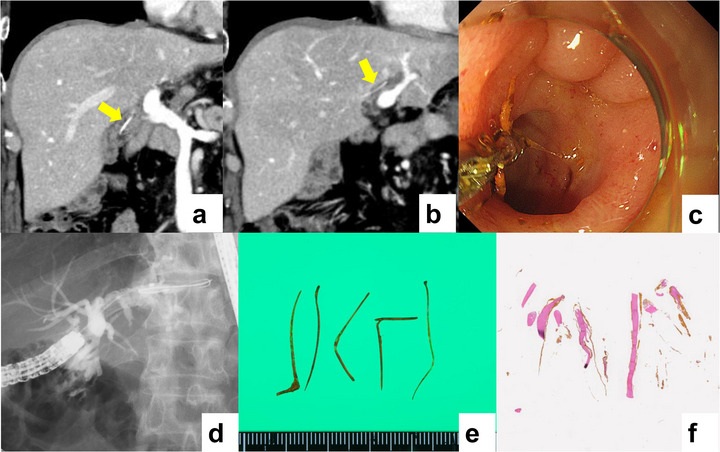 FIGURE 1
FIGURE 1| Number of patients, n | 11 | |
|---|---|---|
| Sex, male/female, n | 9/2 | |
| Median Age (range), years | 76 | (61‐83) |
| Primary disease | ||
| Bile duct cancer, n | 9 | |
| Pancreatic cancer, n | 2 | |
| Adenoma of the ampulla of Vater, n | 1 | |
| Pervious surgical procedure | ||
| Subtotal stomach‐preserving pancreaticoduodenectomy, n | 10 | |
| Extra hepatic bile duct resection, n | 1 | |
| Median time to diagnosis from operation (range), months | 84 | (12‐124) |
| Reason for performing endoscopy | ||
| Foreign body or biliary stone on imaging examination, n | 6 | |
| Cholangitis, n | 3 | |
| Elevation of biliary enzymes, n | 2 |
| Scope used (%), n | ||
|---|---|---|
| SIF‐H290S | 10 | (90.1) |
| SIF‐Q260 | 1 | (9.9) |
| Devices for removal (%), n | ||
| Forceps alone | 3 | (27.3) |
| Basket alone | 2 | (18.2) |
| Balloon alone | 1 | (9.1) |
| Forceps + basket + balloon | 1 | (9.1) |
| Forceps + basket | 1 | (9.1) |
| Forceps + balloon | 1 | (9.1) |
| Basket + balloon | 1 | (9.1) |
| Median procedure time (range), min | 40.5 | (9‐54) |
| Median number of fish bones (range), n | 2 | (1‐13) |
| Coexistence of bile duct stones (%), n | 7 | (63.6) |
| Complete removal (%), n | 11 | (100) |
| Adverse events (%), n | 3 | (27.2) |
| Number of recurrence (%), n | 2 | (18.2) |
| No | Ref.no | Author | Year | Country | Age | Sex | Reason for treatment | Detection in imaging | Primary disease | Prior surgery | Time to diagnosis from surgery (month) | Treatment | Removal | Adverse event | Length of fish bone (mm) | Bile duct stone | Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 5 | Natusui | 2022 | Japan | 66 | M | cholangitis | CT | AC | PD | 48 | percutaneous | success | none | 30 | exist | none |
| 2 | 6 | Suzuki | 2022 | Japan | 73 | M | FB | CT | IPMN | PD | 180 | endoscopy | success | none | 18 | exist | none |
| 3 | 7 | Ishikawa | 2021 | Japan | 67 | M | FB | CT | PC | PD | 36 | operation | success | none | 30 | exist | none |
| 4 | 8 | Hirata | 2021 | Japan | 70 | M | cholangitis | CT | GC | DG | NA | endoscopy | success | none | 20 | none | none |
| 5 | 9 | Kunovsky | 2021 | Czech | 79 | F | FB | US | NA | NA | NA | endoscopy | success | none | 30 | none | none |
| 6 | 10 | Wu | 2020 | China | 62 | M | recurrence | NA | AC | PD | 36 | surgery | success | none | 26 | exist | none |
| 7 | 11 | Akahane | 2019 | Japan | 50s | M | FB | CT | BDC | PD | 12 | SR | NA | NA | 30 | none | none |
| 8 | 11 | Akahane | 2019 | Japan | 60s | F | FB | CT | DC | PD | 18 | SR | NA | NA | NA | none | none |
| 9 | 11 | Akahane | 2019 | Japan | 70s | M | FB | CT | BDC | PD | 16 | SR | NA | NA | NA | none | none |
| 10 | 11 | Akahane | 2019 | Japan | 70s | M | FB | CT | BDC | PD | 9 | SR | NA | NA | NA | none | unclear |
| 11 | 11 | Akahane | 2019 | Japan | 60s | F | FB | CT | PC | PD | 36 | SR | NA | NA | NA | none | none |
| 12 | 11 | Akahane | 2019 | Japan | 60s | M | FB | CT | PC | PD | 21 | SR | NA | NA | NA | exist | none |
| 13 | 12 | Koga | 2018 | Japan | 71 | M | cholangitis | CT | BDC | PD | 12 | endoscopy | success | none | unclear | none | none |
| 14 | 13 | Sakakida | 2018 | Japan | 78 | F | cholangitis | CT | DC | PD | 108 | endoscopy | success | none | 20 | exist | none |
| 15 | 14 | Kim | 2004 | Korea | 75 | F | cholangitis | CT | NA | NA | NA | percutaneous | success | none | 15 | exist | none |
| 16 | 14 | Kim | 2004 | Korea | 67 | M | cholangitis | PTC | NA | NA | NA | percutaneous | success | none | 15 | exist | none |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Foreign Body Medical Cases · Pediatric Hepatobiliary Diseases and Treatments
Introduction
1
Biliary infections, including cholangitis, cholecystitis, and hepatic abscesses, are primarily caused by biliary obstruction due to biliary stones or malignant diseases. Standardized methods for the diagnosis and treatment of biliary infections have already been established based on studies including a large number of patients, and have been described in several guidelines [1, 2]. Biliary foreign bodies can cause biliary infections, although prior reports are largely limited to case reports/series [3, 4]. Most biliary foreign bodies are remnants of medical material following biliary surgery or endoscopic retrograde cholangiopancreatography (ERCP) procedures, whereas a smaller proportion result from bullet or shrapnel injury. However, some biliary foreign bodies originate from ingested materials, such as teeth and bones. Of these, reports of fish bones are extremely rare, with only 16 reported cases [5, 6, 7, 8, 9, 10, 11, 12, 13, 14].
In our hospital, we have experienced several cases of cholangitis caused by fish bones in patients with a history of hepaticojejunostomy. In this study, we retrospectively reviewed all patients with fish bones identified as a biliary foreign body from the endoscopy database of Teine Keijinkai Hospital, describing the patients’ characteristics, treatment, and clinical courses.
Accordingly, we conducted this study to clarify the clinical characteristics, imaging features, and endoscopic treatment outcomes of fish bone migration into the bile duct after hepaticojejunostomy.
Methods
2
Patients
2.1
We enrolled patients who underwent endoscopic extraction of fish bones from the endoscopy database of the Teine Keijinkai Hospital between June 2016 and November 2023. The following data were collected from the electronic medical records: age, sex, prior history of biliary surgery, reason for performing endoscopy, imaging findings before treatment, time between biliary surgery and endoscopy, details of the endoscopic procedure, adverse events (AEs) after treatment based on the ASGE definition [15], and clinical course.
Treatment Strategy and Device Selection
2.2
It is essential to carefully review pre‐procedural CT images and intraprocedural fluoroscopic findings to confirm the number and precise locations of migrated fish bones, as multiple fish bones may migrate into the bile duct.
In patients who have undergone hepaticojejunostomy, reaching the anastomotic site using a conventional side‐viewing duodenoscope is often difficult. Therefore, a single‐balloon enteroscope with an overtube was used to reach the anastomosis.
When a fish bone was directly visible endoscopically at the hepaticojejunostomy site, forceps extraction was selected as the first‐line approach. Standard biopsy forceps were frequently used because of their sufficient grasping ability for elongated foreign bodies. In such cases, the forceps were carefully adjusted so that the long axis of the fish bone was aligned with the bile duct axis, thereby reducing the risk of bile duct injury during extraction.
When the fish bone was not visible at the anastomotic site or when biliary stones had formed around the fish bone as a nidus, basket extraction was selected as the first‐line approach. Previously, wire‐guided 8‐wire Dormia‐type baskets were mainly used. More recently, spiral‐type baskets, which are increasingly used in bile duct stone extraction, have also been employed, with rotation applied as needed to facilitate efficient retrieval of fish bones. During basket use, the deployment direction was also adjusted to align as closely as possible with the bile duct axis to enable safe extraction. In patients with an acute angle at the biliary branch, partial basket opening under guidewire guidance and gentle sliding along the duct facilitated appropriate advancement.
If resistance was encountered during extraction, there was a risk of bile duct injury due to the sharp edges of the fish bone. In such situations, the angle and position of the device were readjusted before further attempts. If resistance was encountered at the anastomotic site, balloon dilation was considered.
When removal using a single device was difficult, switching between multiple devices, including retrieval balloons selected according to the bile duct diameter, enabled successful extraction in most cases.
Because fish bones may fracture into multiple fragments during retrieval, the bile duct was swept several times to confirm the absence of residual fragments.
After extraction from the bile duct, the fish bones were retrieved extracorporeally through the scope when feasible. If through‐the‐scope retrieval was difficult, the fish bones were carefully withdrawn into the overtube under direct endoscopic visualization, avoiding mucosal injury.
Complete removal was defined as the absence of apparent residual fish bones on post‐procedural endoscopic images and cholangiographic findings.
Because most patients had undergone surgery for malignant disease, post‐procedural imaging follow‐up was mainly performed using CT in conjunction with routine surveillance for tumor recurrence or metastasis. Particular attention was paid to new linear high‐density structures in the bile duct suggestive of recurrent fish bone migration.
Results
3
Patient Characteristics
3.1
A review of our database between June 2016 and November 2023 revealed 9078 cases of ERCP procedures (8335 and 743 cases with normal and surgically altered anatomy, respectively), of which fish bones were extracted from 11 patients (1.5% of patients with surgically altered anatomy) (Table 1). All patients had a history of pancreaticobiliary neoplasms; overall, 10 underwent subtotal stomach‐preserving pancreaticoduodenectomies (SSPPD) with Child's reconstruction and one underwent extrahepatic bile duct resection with choledochojejunostomy. The median time between prior surgery and endoscopic treatment was 84 months (range 12–124). The most common reason for performing endoscopy was the detection of biliary stones or foreign bodies in the imaging diagnosis (54.5%), followed by the onset of cholangitis (27.3%), and elevated biliary enzymes (18.2%).
Regarding imaging examinations before the endoscopic procedure, computed tomography (CT) was performed in all patients. A retrospective review of CT imaging data revealed that foreign bodies could be visualized as high‐density dots or linear substances in the bile duct (Figure 1a,b). Differentiation of migrated fish bones from surgical clips after choledochojejunostomy or calcified debris was possible because fish bones showed intraductal positioning within the bile duct, a linear or slightly curved shape, and an absence of metal artifacts typically seen with surgical clips. Magnetic resonance imaging (MRI) and abdominal ultrasound (US) were performed in two and four patients, respectively; however, only a linear hyperechoic substance in the bile duct was detected in patients who underwent US.
The patient was a 62‐year‐old man with a history of pancreaticoduodenectomy with reconstruction for bile duct cancer 7 years prior to requiring extraction of a fish bone. Highly dense linear materials were detected in the bile duct on enhanced computed tomography (a, b). All fish bones were successfully extracted using forceps via single‐balloon enteroscopy, without any adverse events (c, d, Video). Biliary stones were also removed by sweeping with a balloon catheter (Video). Five fish bones were removed from the patients (e), pathologically examined by Hematoxylin‐eosin staining, and found to be elongated, unstructured material with bile deposits, consistent with fish bones (f).
Endoscopic Procedure
3.2
The details of the endoscopic procedures are summarized in Table 2. All procedures were performed using single‐balloon enteroscopy‐assisted ERCP in patients with surgically altered anatomies. Using a combination of forceps, basket catheters, and balloon catheters (Figure 1 c,d), all fish bones and 7 coexisting biliary stones were successfully removed. The median duration for fish bone removal (defined as the duration from endoscope insertion to withdrawal) was 40.5 (range 9–54) minutes. Overall, 3 cases of mild cholangitis were observed, all of which resolved with the administration of antibiotics. Of the 11 patients, histological interpretation was performed on 7 extracted samples. Histopathological examination with hematoxylin and eosin staining showed a bony matrix composed of collagen fibers, consistent with bone tissue. No cellular components suggestive of synthetic foreign bodies were observed (Figure 1 e,f). One patient had one recurrence, and another had two recurrences of biliary migration of the fish bone; however, all recurrent cases were successfully treated using single‐balloon enteroscopy.
Discussion
4
In the present study, we showed that migration of fish bones into the bile duct in patients who underwent biliary surgery is a rare but clinically significant complication.
In normal anatomy, unless endoscopic sphincterotomy for extraction of biliary stones or large‐bore stent placement for biliary stricture is performed, the migration of dietary contents into the bile duct is rare due to the action of the Oddi sphincter. In contrast, in cases with surgical anastomosis between the digestive tract and bile duct, dietary contents may easily enter the bile duct due to the sufficient diameter of the anastomosis for migration. However, biliary reconstruction surgery is performed by creating a jejunal afferent limb, and the migration of dietary contents is considered a rare phenomenon. Overall, there have been 10 prior studies investigating fish bone migration to the bile duct, including 16 case reports of fish bone migration to the bile duct, and 12 in patients with choledochojejunostomy (75.0%, Table 3). Considering the limited population of patients who undergo choledochojejunostomy, this procedure should be considered one of the strongest factors for the migration of fish bones [5, 6, 7, 8, 9, 10, 11, 12, 13, 14].
One prior case series revealed that the majority of fish bones that migrated to the bile duct spontaneously disappeared during observation [11]. Of the 11 patients included in the present study, 8 were asymptomatic and could have been managed without aggressive treatment. However, foreign bodies in the bile duct are associated with stone formation in 69.8% of cases, and this rate is particularly high when the foreign bodies are derived from dietary contents [16]. The removal of biliary stones using balloon‐assisted enteroscopy, rather than percutaneous or surgical procedures, is currently performed safely and effectively in the majority of patients who undergo biliary surgery with reconstruction of the jejunal limbs [17]. All 11 patients successfully underwent removal of the fish bone without serious adverse events using single‐balloon enteroscopy. Thus, immediate removal of fish bones at the time of detection could be considered a treatment option.
In a retrospective review of CT scans prior to treatment, fish bones were detected as tiny or linear hyperdense materials in the bile duct in all patients (Figure 1 a,b). Biliary surgery with reconstruction is usually performed to cure pancreatic or biliary neoplasms. The majority of patients undergo planned imaging diagnosis as surveillance for recurrence and unexpected adverse events, and CT is the most common imaging modality. In such cases, careful review of the CT images would detect the migration of the fish bone into the bile duct before the appearance of clinical signs of biliary congestion. Furthermore, it is possible to determine the bile duct branches that have migrated using CT. Imaging before the endoscopic procedure is helpful to ensure an efficient and safe treatment (Figure 1a,b).
Previous reports describing pathological evaluation of migrated fish bones have demonstrated characteristic findings of bone tissue, including a bony matrix composed of collagen fibers on hematoxylin and eosin staining, and calcium‐phosphate–dominant composition on component analysis [8, 13, 16]. The histopathological features in our cases were consistent with these findings, supporting the diagnosis of migrated fish bones rather than other foreign materials.
This was a single‐center, retrospective case series study. From our database, we included 11 patients treated with an endoscopic procedure for migrating fish bones. However, not all patients who underwent biliary surgery were routinely followed with CT, and asymptomatic fish bone migration without biliary congestion may therefore have been overlooked. No fish bone migration was detected in patients without choledochjejunostomy who underwent ERCP; however, the endoscopist may have failed to detect the presence of fish bones in the core of the stones removed during the procedure. As such, the actual frequency of fish bone migration into the biliary tract remains unknown. This limitation will only be addressed in a prospective observational study.
In conclusion, this case series shows that the migration of fish bones into the bile duct is not uncommon in patients who undergo biliary surgery with reconstruction using the afferent limb. Further, our experience suggests that most migrated fish bones can be detected using CT and safely extracted using single‐balloon enteroscopy.
Author Contributions
Kenta Yoshida, Tsuyoshi Hayashi, and Akio Katanuma conceived and designed the study, and drafted the initial manuscript. Kazuki Hama, Ryo Ando, Haruka Toyonaga, Tatsuya Ishii, Toshifumi Kin, Masayo Motoya, and Kuniyuki Takahashi contributed to case registration.Yuko Omori and Satoshi Ota performed the pathological diagnosis and histological evaluation. All authors contributed to manuscript preparation and have read and approved the final version.
Funding Information
The authors received no specific funding for this work.
Ethics Statement
This single‐center, retrospective, case series study was approved by the Institutional Review Board of Teine Keijinkai Hospital in Sapporo City, Hokkaido, Japan (approval number: 2‐023402‐00; registration date: 25/01/2024). Informed consent for participation was obtained using the opt‐out method listed on the hospital website.
Conflicts of Interest
All authors declare no conflicts of interest. The study was not registered in a clinical trial registry (N/A). Animal studies were not applicable (N/A).
Supporting information
Video S1: Endoscopic removal of a migrated fish bone from the bile duct using single‐balloon enteroscopy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1T. Mayumi , K. Okamoto , T. Takada , et al., “Tokyo Guidelines 2018: Management Bundles for Acute Cholangitis and Cholecystitis,” Journal of Hepato‐Biliary‐Pancreatic Sciences 25, no. 1 (2018): 96–100.29090868 10.1002/jhbp.519 · doi ↗ · pubmed ↗
- 2J. L. Buxbaum , C. Buitrago , A. Lee , et al., “ASGE Guideline on the Management of Cholangitis,” Gastrointestinal Endoscopy 94, no. 2 (2021): 207–221.34023065 10.1016/j.gie.2020.12.032 · doi ↗ · pubmed ↗
- 3J. L. Ban , F. M. Hirose , and J. R. Benfield , “Foreign Bodies of the Biliary Tract: Report of Two Patients and Review of the Literature,” Annals of Surgery 176 (1972): 102–107.4624865 10.1097/00000658-197207000-00018 PMC 1355282 · doi ↗ · pubmed ↗
- 4M. Yu , B. Huang , Y. E. Lin , et al., “Acute Obstructive Cholangitis due to Fishbone in the Common Bile Duct: A Case Report and Review of the Literature,” BMC Gastroenterology 19 (2019): 177.31699035 10.1186/s 12876-019-1088-8PMC 6839197 · doi ↗ · pubmed ↗
- 5K. Natsui , M. Maruyama , and S. Terai , “Intrahepatic Bile Duct Foreign Body With Cholangitis After Pylorus‐Preserving Pancreatoduodenectomy: Is It a Fish Bone?,” Gastroenterology 163, no. 4 (2022): e 18–e 20.10.1053/j.gastro.2022.05.01735580659 · doi ↗ · pubmed ↗
- 6Y. Suzuki , T. Ishizawa , N. Makino , et al., “A Case of Successful Removal of a Migrated Fish Bone in the Bile Duct After Pancreaticoduodenectomy Using Overtube‐Assisted Cholangioscopy,” Clinical Journal of Gastroenterology 15, no. 2 (2022): 493–499.35133627 10.1007/s 12328-021-01579-0 · doi ↗ · pubmed ↗
- 7T. Ishikawa , H. Kawashima , E. Ohno , et al., “Endoscopic Removal of a Fish Bone Piercing the Bile Duct After Pancreaticoduodenectomy,” Endoscopy 53, no. 5 (2021): E 164–E 165.32818989 10.1055/a-1224-3724 · doi ↗ · pubmed ↗
- 8K. Hirata , D. Kawamura , and M. Orita , “A Case of a Common Bile Duct Stone That Formed Around a Fish Bone as a Nidus After Distal Gastrectomy With Roux‐en‐Y Reconstruction,” Surgical Case Reports 7, no. 1 (2021): 58.33630177 10.1186/s 40792-021-01142-6PMC 7907409 · doi ↗ · pubmed ↗