Maternal infection during pregnancy and the risk of childhood cancer: a systematic review and meta-analysis
Loviisa Mulanje, Lara Kim Brackmann, Alicia Lübtow, Hajo Zeeb, Wolfgang Ahrens, Manuela Marron, Rajini Nagrani

TL;DR
This study finds that maternal infections during pregnancy may increase the risk of childhood cancer, with specific infections linked to specific cancer types.
Contribution
The study provides a comprehensive meta-analysis linking specific maternal infections to childhood cancer risks, offering insights for targeted prevention.
Findings
Maternal infections during pregnancy are associated with a 36% increased risk of childhood cancer overall.
Sexually transmitted infections and viral infections are strongly linked to higher cancer risks, including leukemia.
Genitourinary tract infections are specifically associated with increased risks of leukemia and solid tumors.
Abstract
Maternal infections during pregnancy may increase the risk of childhood cancer (CC) in offspring by affecting foetal immunity and genetics. Existing evidence seems inconclusive, necessitating a comprehensive review to understand this association. We aimed to evaluate the risk of various CC outcomes following prenatal exposure to different types of maternal infections. We searched Medline, Web of Science, Embase, Cochrane Library, and bibliographies for relevant studies from inception to October 2025. The study protocol was registered in PROSPERO (ID:CRD42023483706). We included original human epidemiological studies that examined the association between maternal infections during pregnancy and CC with appropriate reference groups and no language restrictions. We excluded studies if they were reviews or reports, if they did not assess individual-level infection or if they used therapies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
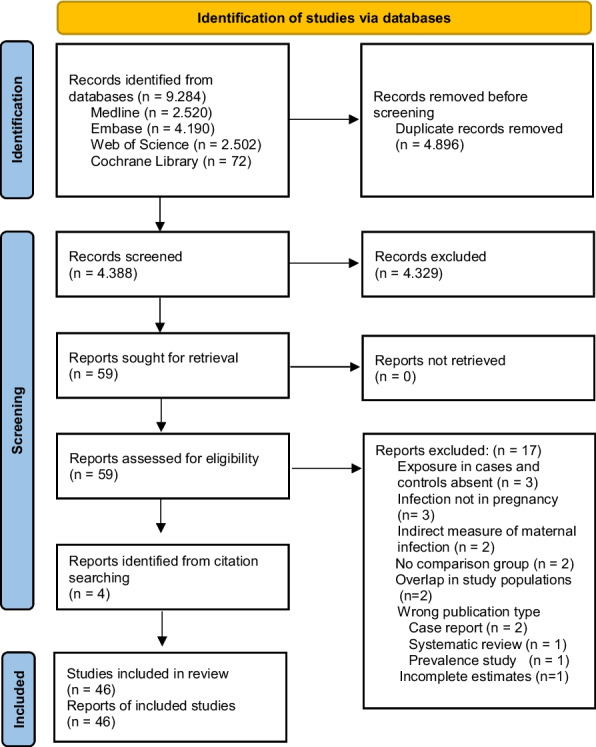 Figure 1
Figure 1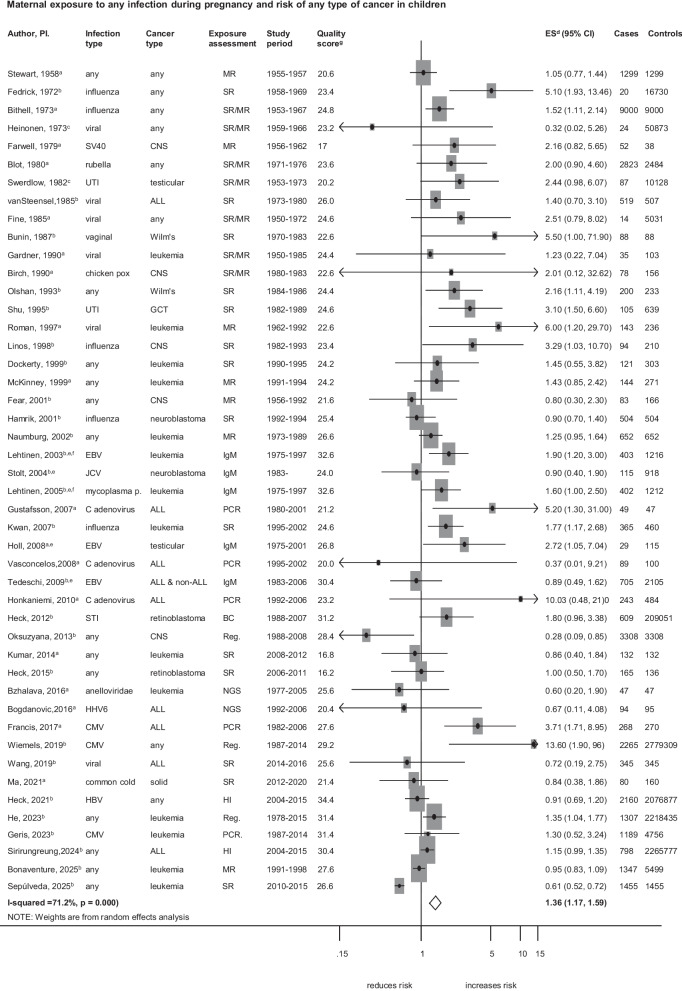 Figure 2
Figure 2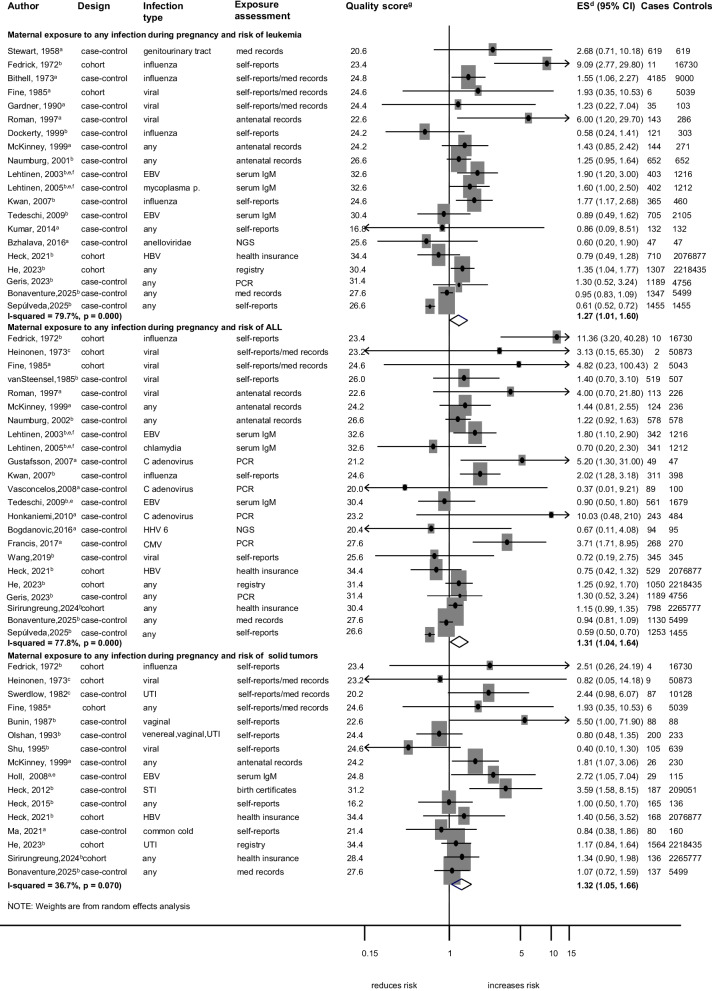 Figure 3
Figure 3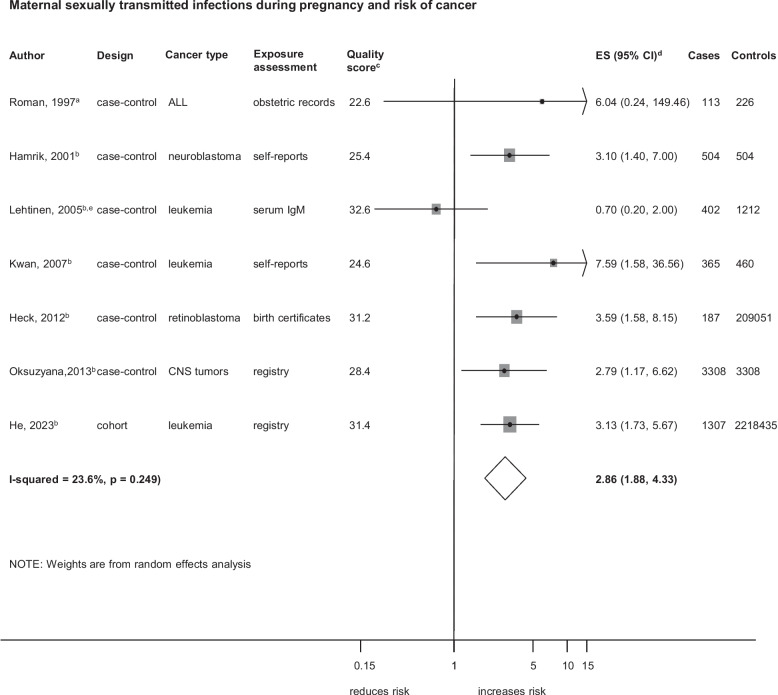 Figure 4
Figure 4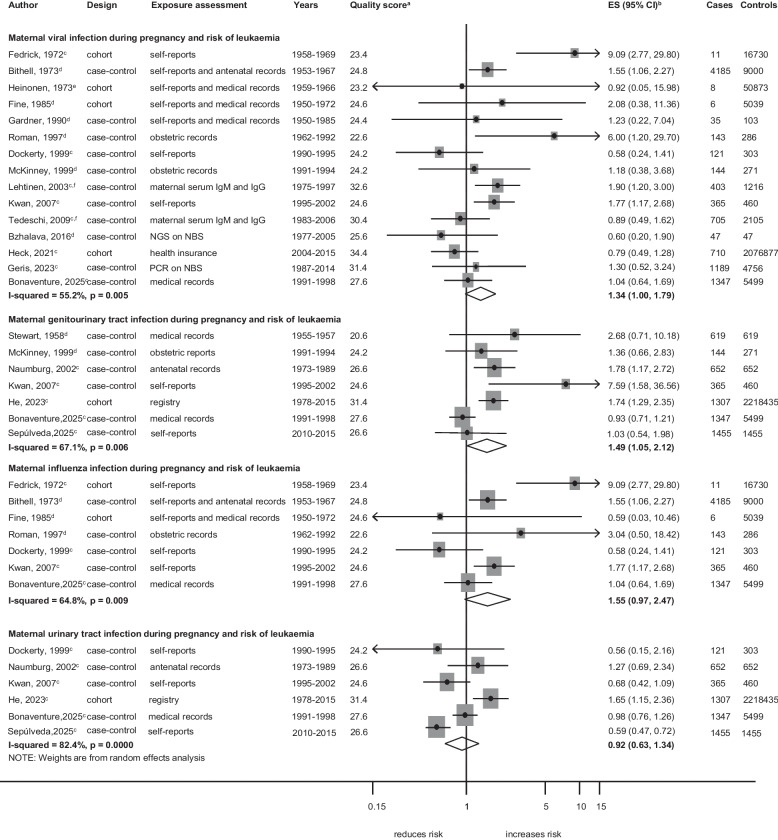 Figure 5
Figure 5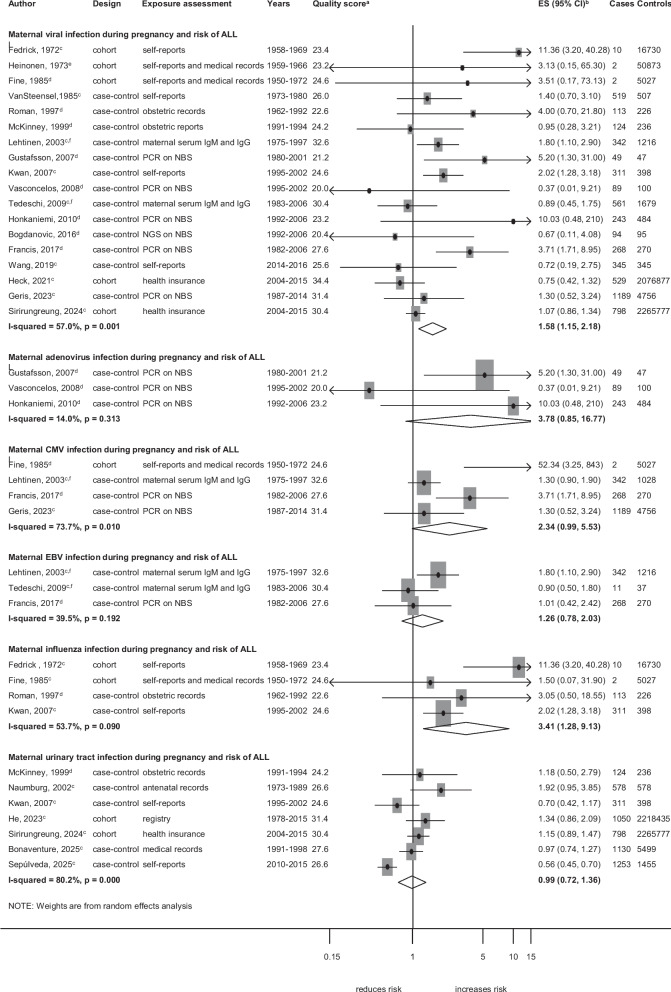 Figure 6
Figure 6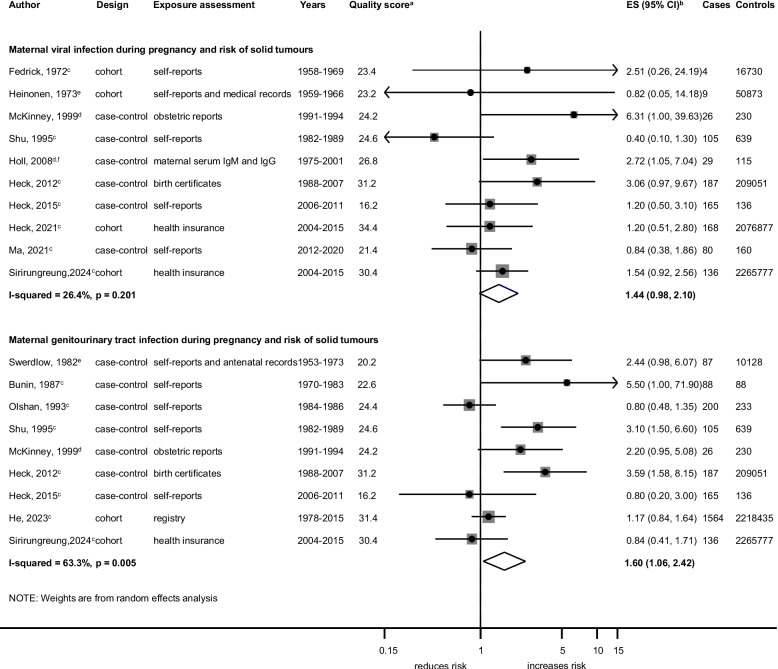 Figure 7
Figure 7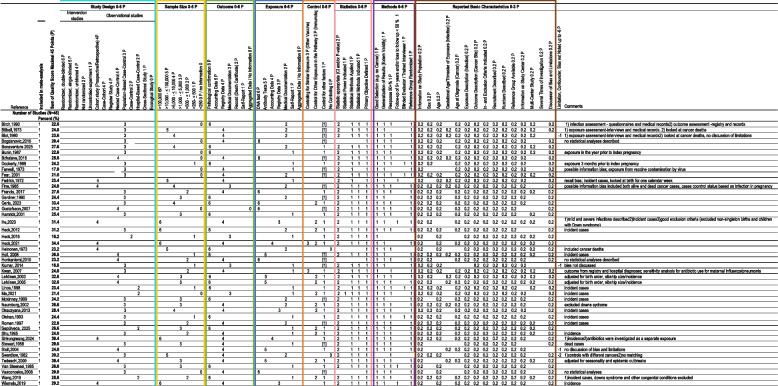 Figure 8
Figure 8- —https://doi.org/10.13039/501100001659Deutsche Forschungsgemeinschaft
- —Leibniz-Institut für Präventionsforschung und Epidemiologie – BIPS GmbH (5712)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Risks and Factors · Acute Lymphoblastic Leukemia research · COVID-19 Impact on Reproduction
Background
Cancer is a global health problem not only among older populations but also among children and adolescents with approximately 400,000 cases diagnosed every year in individuals aged 0–19 years [1]. The aetiologies of childhood cancer, remain largely unknown, despite being studied for decades. While rare genetic syndromes and high-dose ionising radiation are known risk factors for childhood cancer [2, 3], they only account for a small percentage of cases. Hence, further research is necessary to identify other factors associated with the development of cancers in childhood. As approximately half of childhood cancers are diagnosed before five years of age in utero exposures are of interest.
Maternal infections during pregnancy are common, with varying impacts on foetal development depending on the type of infection and the maternal and foetal immune response. Beyond the known adverse perinatal outcomes of pregnancy infections, such as low birth weight, intrauterine growth restriction, prematurity and congenital anomalies [4], emerging research suggests that infections during pregnancy might also be associated with cancer in the offspring. Infections during critical windows of foetal development may influence carcinogenesis through multiple mechanisms involving inflammation and immune modulation [5], with subsequent DNA damage or epigenetic modifications [6, 7]. Some viruses with known oncogenic potential, such as the Hepatitis B virus (associated with hepatocellular carcinomas), may cross the placenta and mediate direct effects on foetal genetics, ultimately influencing the risk of cancer in the offspring. Other infections, mainly ascending infections from the lower genital tract, may be vertically transmitted across the maternal-foetal membranes and may cause an altered foetal immune response [8]. In the absence of direct vertical transmission, infections may still trigger a foetal inflammatory response through the maternal metabolites and by-products of infection and also mediate epigenetic changes which might contribute to cancer susceptibility [7].
Despite suggestive findings of an association between infections during pregnancy and cancer in offspring from epidemiological studies in the last five decades, the evidence is limited and inconsistent, particularly concerning the pathogen type and specific cancer subtypes. A meta-analysis of 20 studies, published in 2019, found that influenza, varicella, and rubella infections of the mother during pregnancy were associated with an increased risk of childhood leukaemia [9]. However, this meta-analysis did not consider other pregnancy infections and was limited to leukaemia.
Therefore, to close this gap, we conducted a comprehensive systematic literature review and meta-analysis on the association between diverse maternal infections during pregnancy and the risk of various childhood cancers in the offspring.
Methods
Search strategy and selection criteria
Our systematic review and meta-analysis was conducted in accordance with the Meta-analysis of Observational Studies in Epidemiology (MOOSE) [10] and the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) [11] guidelines (Additional file 1: Table. S1) and was registered in PROSPERO (registration number: CRD42023483706). Two researchers (LM and LKB) systematically searched the Medline, Embase, Web of Science and Cochrane Library databases for articles published until October 2025, without language restrictions. We used subject headings and keywords in English, based on the search structure of the literature database, to combine terms related to the population (pregnant women and their offspring), exposure (prenatal infection), and outcome (childhood cancer). A detailed description of the search strategy, developed with the help of an experienced research librarian (LC), is provided in Additional file 2: Table. S2. The reference lists of the included studies were reviewed to identify additional relevant articles. Duplicate entries were removed using EndNote. Two reviewers (LM and LKB) independently screened the titles, abstracts and full-text articles. We included studies if they were human epidemiological research on maternal infections during pregnancy and their association with childhood cancer, with appropriate reference groups (controls without cancer; any other control definition critically assessed). Maternal infections were self-reported by mothers, abstracted from medical records, or assessed in biospecimens such as maternal blood during pregnancy or neonatal dried blood spots, with early neonatal infections considered indicative of congenital infections, acquired in utero. We excluded studies if they were reviews or reports, if they did not assess individual-level infection or if they considered antibiotics or other therapies for infections as exposure to infection. We only included studies with quantitative risk estimates (odds ratio (OR), relative risk (RR), or hazard ratio (HR)) or measures of variability (variance, standard error (SE), standard deviation (SD), confidence interval (CI)) or sufficient data to calculate crude risk estimates. We used the different quantitative risk estimates (OR, RR, HR) with the knowledge that they yield similar results in rare outcomes such as childhood cancer [12]. For studies with overlapping populations, the most recent publication was selected. Disagreements regarding the review of the articles were resolved by consensus with other authors (RN and MM). A detailed description of the study selection is shown in Fig. 1.Fig. 1PRISMA 2020 flow diagram for the selection of studies
Data extraction and quality assessment
Two of us (LM and LKB) extracted data from each publication as follows: first author name, study design, location, period, number of cases, reference group details, cancer outcome, age at diagnosis, type of infection, method of infection and outcome assessment, matching and adjustment factors, statistical approaches, and risk estimates. Immunoglobulin M (IgM) was selected as a marker of recent infection when multiple immunoglobulins were reported and the model with the most confounder adjustments was used to minimize confounding where multiple adjustment models were reported (Additional file 3: Table. S3).
We assessed the quality of the studies using a scoring system adapted from the Newcastle–Ottawa Scale (NOS) and Risk Of Bias in Non-randomized Studies of Exposure (ROBINS-E) and of Intervention (ROBINS-I) tools. This scoring system expands on the original NOS, recognizing the NOS’s limitation in extensively appraising observational studies, and includes the risk of bias considerations from ROBINS. The tool is described elsewhere [13]. Briefly, it consists of 8 categories with basic study-level characteristics and elements for risk of bias assessment, with a maximum quality score of 45 points. Studies are classified studies as high- or low-quality using a cut-off at the 4th quintile score. Two authors (LM and LKB) independently extracted quality-related items from the included studies, and a third author (RN) resolved disagreements. Detailed quality criteria are available in Table 2.
Statistical analysis
Pooled estimates (ES) with 95% confidence intervals (CIs) were calculated using random-effects models when at least three studies investigated the same exposure–outcome relationship (i.e., maternal infection during pregnancy and a specific childhood cancer type) [14]. We conducted a total of 33 analyses, examining the association between maternal infections during pregnancy and childhood cancer, focusing on infections and cancers with sufficient data (at least three studies per analysis) for evaluation. To provide an initial summary estimate of the overall association between maternal infections during pregnancy and risk of childhood cancer, we first conducted an overall meta-analysis including all eligible studies. This broad analysis was intended to offer a general overview before performing stratified analyses by type of infection and by specific childhood cancer type. For specific infections, we analysed infections by pathogen type (bacterial and viral), by affected body site (respiratory tract, urinary tract, and genitourinary tract infections (GUTIs)) and by mode of transmission (sexually transmitted infection (STIs)). For cancer types, we analysed leukaemia (all histological subtypes together and acute lymphoblastic leukaemia (ALL) separately), lymphoma (all subtypes collectively due to insufficient data (less than three studies) for individual subtypes), central nervous system tumours (CNS) and neuroblastomas, and solid tumours (including germ-cell tumours, hepatic tumours, hepatoblastomas, retinoblastomas, testicular cancers, and Wilms tumours). Solid tumours were analysed as a group also due to insufficient data for individual tumour types. One study did not specify the type of infection and was included under the “any infection” category [15]. When multiple infection types or cancer outcomes were reported, we selected the most general and prevalent infection and cancer type. For instance, in the study by Roman et al. [16], which examined both general and specific viral infections in relation to leukaemia and non-Hodgkin lymphoma, we included general viral infection and leukaemia as the representative exposure and outcome respectively.
We quantified heterogeneity using the I^2^ statistic, categorized as low (≤ 50%), moderate (> 50–75%), or substantial (> 75%), with its statistical significance assessed using the Q statistic (p value for heterogeneity, (p)). To explore potential effects on heterogeneity, we conducted sensitivity analyses by omitting studies one at a time for each analysis [17]. We also conducted subgroup analyses stratified by study characteristics, including study design (case–control or cohort), type of infection assessment (self-reported data, medical records, or biological specimens), type of outcome assessment (cancer registry/pathological confirmation), confounder control (adjustment for basic factors, additional factors, or other infections), geographic region (Asia and Oceania, Europe, and North America), study period (pre- or post-2000), and overall study quality (high or low). In addition, we conducted meta-regression analyses to examine the influence of these study-level characteristics on the effect estimates to further identify and explain potential sources of heterogeneity. The statistical significance of each covariate was evaluated using a p-value threshold of 0.05. For meta-analyses including ≥ 5 studies we evaluated whether publication bias was present by visually inspecting a funnel plot and applying Egger’s asymmetry test [18]. A significant Egger’s test (p < 0.05) and/or asymmetry in the funnel plot were considered indicative of publication bias. In such cases where evidence of publication bias was observed, we applied the Duval and Tweedie trim-and-fill method to estimate the potential effect of missing studies on the pooled results [19]. All analyses were performed in Stata version 18 (StataCorp LP, College Station, TX, USA).
Results
Study characteristics and quality of included studies
We identified 9,284 articles from the four databases with 4,896 duplicates removed and 4,329 excluded based on title and abstract screening, leaving 59 articles for full-text evaluation (Fig. 1). An additional four articles were identified from references in these 59 papers. Seventeen full-text articles were excluded based on our exclusion criteria (Additional file 4: Table. S4), leaving 46 studies for the review and meta-analysis [15, 16, 20–63]. Three studies were excluded from the meta-analysis: two because they were based on overlapping study populations [64, 65] and one because it did not report estimates of risk [66].
The 46 studies included in the meta-analysis were published between 1958 and 2025 and were conducted in Asia or Oceania (13%), Europe (50%), and North America (37%), with sample sizes ranging from 90 to 2,782,507 participants per study (Table 1). Most studies focused on cancer diagnoses within the first 18 years of life, with some exceptions extending to 20, 30, or 40 years of age [16, 30, 56]. Table 1. Characteristics of studies included in meta-analysisFirst Author, YearLocationStudy yearsNo. of CasesNo. of ControlsAge RangeOutcomeInfectionResultsOutcome AssessmentExposure AssessmentStudy DesignCommentQuality Birch, 1990 [20] England (North Western, West Midlands, Yorkshire)1980–198378156< 15 yearsCentral Nervous SystemChickenpox, measles, influenza, UTI, "other" infectionsNo associationRegistrySelf-reported questionnaires with some verification with medical recordsPopulation-based Case–ControlMat: age, sex; hospital controls without neoplastic disease, genetic, constitutional disease, malformation or chronic disease22.6 Bithell, 1973 [21] UK (England, Wales, Scotland)1953–196790009000≤ 16 yearsLeukaemia, other lymphatic tissue disease, other tumoursInfluenza, chicken pox, rubella, other viral infectionsIncreased risk after influenza and chickenpox infectionRegistrySelf-reported interviews and antenatal records where possiblePopulation-based Case–ControlCancer deaths; Mat: sex, date of birth24.8 Blot, 1980 [22] UK (England, Wales, Scotland)1971–197628232484≤ 15 yearsChildhood cancer (leukaemia, brain tumours, neuroblastoma, ovarian cancer)ChickenpoxNo associationRegistrySelf-reported interviews and antenatal records where possiblePopulation-based Case–ControlCancer deaths; Mat: age, sex, nearness of residence to case child23.6 Bogdanovic, 2016 [23] Sweden1992–20069595≤ 17 yearsALLHHV6, Human Parvovirus B19, HERV (DNA)No associationRegistryUnbiased NGS on neonatal blood spots NBSPopulation-based Case–ControlMat: age and birthplace18.4 Bonaventure, 2025 [61] England and Wales1991–199828855499< 15 yearsleukaemia, lymphoma, CNS tumours, embryonal tumours or otherAny infection, urinary tract infection, genital infection, influenza, chickenpoxIncreased risk of lymphoma after urinary tract infectionPathological confirmation and RegistryMedical recordsPopulation-based Case–ControlAdj: age, year of birth, General practitioner record abstraction statusMat: age and sex27.6 Bunin, 1987 [24] USA (Philadelphia)1970–19838888< 15 yearsWilm's tumourVaginal infectionIncreased riskPathological confirmationTelephone interviews on exposures in the year prior to index pregnancyPopulation-based Case–ControlAdj: demographical differences between cases and control and risk factors; Mat: race, birth date, telephone area code and exchange22.6 Bzhalava, 2016 [25] Sweden1977–20054747≤ 15 yearsChildhood leukaemia and lymphomaAnelloviridae, "unclassified viruses", environmental viruses, papillomaviridaeNo associationRegistryNGS of maternal first trimester (14 weeks gestation) seraNested Case–ControlMat: gender, date of birth of child (± 2 months), mother’s age at serum sampling (± 2 years), date at serum sampling (± 2 months) and alive and free from leukaemia/lymphoma at the time of index child diagnosis23.6 Dockerty, 1999 [26] New Zealand1990–1995121303< 15 yearsChildhood leukaemiaInfluenza, cystitis or kidney infection, cold sores/oral herpes, any other infection (rubella, measles, chicken pox, shingles, mumps, glandular fever, pneumonia, hepatitis B, malaria, leptospirosis)No associationPathological confirmationSelf-reported questionnaire on maternal infection in pregnancy or in the 3 months before the pregnancyPopulation-based Case–ControlAdj: age, sex, child’s social class, household crowding, mother’s educational level; Mat: age, sex24.2 Farwell, 1979 [27] USA (Connecticut)1956–19625238≤ 19 yearsCNS TumoursSV40 virus in polio vaccineIncreased risk of medulloblastoma after antenatal exposure to SV40RegistryQuestionnaires to obstetricians on polio vaccination during pregnancyPopulation-based Case–ControlMat: gender, date of birth, town of birth17.0 Fear, 2001 [28] UK1956–199283166< 15 yearsPrimary malignant neoplasm of the brain or other part of the nervous systemDefinite & probable Viral infection—defined by ICD-10 (rubella, mumps, varicella, herpes zoster)Increased risk after infection of definite viral origin during pregnancy; no association with probable viral infectionRegistryMaternal obstetric notes on nursing cards at the study hospitalsPopulation-based Case–ControlAdj: age, sex; Mat: birth, sex, month, year of birth21.6Fedrick, 1972 [29]UK (England, Wales, Scotland)1958–19692016,730≤ 11 yearsChildhood cancerInfluenzaIncreased riskRegistry and Individual physiciansSelf-reported questionnaires on exposure during pregnancyRetrospective cohortAdj: birth date23.4 Fine, 1985 [30] UK1950–197225702475≤ 40 yearsMalignant disease (ICD codes (9th revision) 140–208; 230–234Viral infection (influenza, varicella, herpes zoster, mumps, rubella, measles, hepatitis, CMV, miscellaneous viruses)Increased risk of cancer among those exposed to herpes viruses, specifically varicella and cytomegalovirusDeath certificates, questionnaire to general practitionerself-reported interviews or medical records from general practitionerCohort studyMat: sex and date and area of birth24.6 Francis, 2017 [31] USA (California)1982–2006268270≤ 18 yearsALLCMV and EBVIncreased risk of ALL with CMV infection; no association with EBVRegistryDroplet digital PCR on NBSPopulation-based Case ControlMat: date of birth, race, sex25.6 Gardner, 1990 [32] UK (West Cumbria)1950–1985971001≤ 25 yearsLeukaemia, NHL, HLViral infections (chickenpox, influenza, rubella)No associationHospital records, death certificates, registries and pathological reviewSelf-reported questionnaires, obstetric records, general medical recordsPopulation-based Case ControlMat: sex, date of birth24.4 Geris, 2023 [62] USA1987–201411894756< 15 yearsALLCMVNo association for overall ALL; increased risk of hyperdiploid ALLPathological confirmationPCR on NBSPopulation-based Case ControlAdj: mother’s age at birth, maternal diabetes, birth weight, categorical gestational age, and presence of congenital anomalyMat: year of birth, sex, and mother’s reported race and ethnicity33.4Gustafsson, 2007 [33]Sweden1980–20014947≤ 17 yearsALLC adenovirus DNAIncreased riskNo informationNested PCR on NBSNested Case–ControlMat: birth date and birthplace19.2Hamrick, 2001 [34]USA and Canada1992–1994504504< 19 yearsNeuroblastomaHepatitis, rubella, measles, mumps, influenza, chickenpox or shingles, mononucleosis, other infectious diseases, UTI, STIIncreased risk with chickenpox and STIPathologically confirmed cases from National Cancer Institute-sponsored paediatric collaborative clinical trials groups, the Children’s Cancer Group (CCG) and the Paediatric Oncology Group (POG)Self-reported interviewsPopulation-based Case–ControlAdj: child’s gender, mother’s race and education, and household income in the birth year; Mat: date of birth25.4 He, 2023 [35] Denmark1978–201543622,218,435< 15 yearsAny childhood leukaemia, ALL, AML, other childhood cancers, including brain tumours, lymphoma, and other cancersAny infection, respiratory tract, genitourinary tract (i.e. urinary and genital tract), digestive system infection, sexually transmitted infections, other infectionsIncreased risk of childhood leukaemia after any maternal infection, genital tract infection, UTI and STI; no association between maternal infection and childhood brain tumours, lymphomas, or other cancersRegistryRegistryProspective cohortAdj: age at childbirth, education level, parity, cohabitation during pregnancy, diabetes during pregnancy (including pre-pregnancy diabetes and gestational diabetes), year of delivery, and season of deliver (spring, summer, autumn, or winter) maternal comorbidities duringpregnancy: hypertensive disorders, anaemia, obstetric haemorrhage, hyperemesis, and asthma30.4 Heck, 2012 [36] USA1988–2007609209,051< 6 yearsRetinoblastoma (Bilateral and Unilateral)Sexually transmitted infection (STI) (genital herpes, syphilis, chlamydia, gonorrhoea)Increased risk of bilateral retinoblastoma after STI in pregnancyPathological confirmationBirth certificatesPopulation-based Case ControlAdj: year of birth, father's age, urban or rural country of residence, mother's race and birthplace; Mat: year of birth31.2 Heck, 2022 [38] Taiwan2004–201521602,076,877< 11 yearsAll cancersHepatitis B and CIncreased risk of all childhood cancers after Maternal HCV infectionRegistryNational health insurance research databaseRetrospective cohortAdj: birth year, parental age and child’s viral hepatitis status, family income, urban or rural area of residence, parity, child’s sex, parental HIV infection, other parent’s viral hepatitis status and maternal country of birth32.4 Heck, 2015 [37] USA and Canada2006–2011252136< 15 yearsRetinoblastomaAny infectious disease, respiratory infection, flu or cold, STI, other viral infections (hepatitis B and C, shingles, HPV, herpes, stomach virus, Murray infection, and Fifth disease), all bacterial infections, UTINo associationMedical documentation—hospital or by the Children’s Oncology Group (COG)Self-reported phone interviewsCase–controlAdj: age, biological relative status of parents, child’s age at interview, mother’s race/ethnicity, mother’s educational attainment, household income, mother’s age at birth, and maternal smoking in the month before or during pregnancy; Mat: age and biological relative status of parents16.2 Heinonen et al. 1973 [39] USA1959–19662450,867≤ 4 yearsMalignant neoplasmsSpontaneous viral infection—not specifiedNo associationPathological confirmationSelf-reported interview, review of hospital and other records and confirmation by attending physicians whenever possibleProspective cohortno adjustment23.2 Holl, 2008 [40] Finland, Sweden, Iceland1975–2001662580—26 yearsTesticular cancerEBV and CMV (IgM, IgG)Increased risk of TC with high level of maternal EBV IgG; Decreased risk of TC with CMV IgG positivityPathological confirmationFirst trimester maternal serum IgM and IgGNested Case–ControlMat: date of birth of son (± one month)24.8 Honkaniemi, 2010 [41] Sweden1992–2006243484≥ 67 days—≤ 15 yearsALLC adenovirus (DNA)No associationRegistryNested PCR in NBS 3–5 days of ageNested Case–ControlMat: birthplace and birthdate21.2 Kumar, 2014 [15] India2008–2012132132< 18 yearsLeukaemia—ALL and AMLAny infection—not specifiedNo associationMedical documentationSelf-reported interviews on exposure during pregnancyPopulation-based Case ControlMat: age, sex, residency16.8 Kwan, 2007 [42] USA1995–2002365460< 15 yearsLeukaemia, ALL and c-ALL (Common ALL)Influenza/pneumonia, STI, UTIIncreased risk of childhood leukaemia and ALL with influenza/pneumonia and Increased risk of childhood leukaemia with STIRegistrySelf-reported interviews on exposure during 3 months before pregnancy and during pregnancypopulation-based Case ControlAdj: household income, maternal education, maternal age at birth of child, antibiotic use; Mat: date of birth, sex, Hispanic ethnicity, maternal race, maternal county of residence at birth24.6 Lehtinen, 2003 [43] Finland and Iceland1975–19974031216< 15 yearsLeukaemiaEBV, CMV, HHV6 (IgG and IgM)Increased risk of childhood leukaemia and ALL with maternal EBVPathological confirmationMaternal serum IgG and IgM antibodies at 12–14 weeks gestationNested Case–ControlAdj: birth order, sibship size; Mat: age at serum sampling, date of specimen collection, date of birth and sex of offspring, country30.6 Lehtinen, 2005 [44] Finland and Iceland1975–19974021212≤ 15 yearsLeukaemiaChlamydia, Helicobacter pylori, Mycoplasma pneumoniae in first trimesterIncreased risk of childhood leukaemia with H. pylori IgGPathological confirmationMaternal serum IgG and IgM antibodies at 12–14 weeks gestationNested Case–ControlAdj: birth order, sibship size; Mat: age at serum sampling, date of specimen collection, date of birth and sex of offspring, country30.6 Linos, 1998 [45] Greece1982–199394210≤ 17 yearsBrain tumours and neuroblastomasInfluenzaIncreased risk of brain tumours and neuroblastomaPathological confirmationSelf-reported interviews—(influenza diagnosis based on response regarding physician visit)Hospital-based Case–controlAdj: maternal smoking during pregnancy, paternal smoking prior to birth of index child, age of index child23.4Ma, 2021 [46]China2012–202080160< 17 yearsSolid tumoursCommon coldNo associationMedical documentationSelf-reported questionnairesCase–controlMat: birth weight, gestational age, residence, and pregnancy BMI21.4 McKinney, 1999 [47] Scotland1991–1994390716≤ 14 yearsLeukaemia, lymphomas, CNS tumours and other solid tumoursAny infection, respiratory tract infection, viral infection, genitourinary infection, fungal infectionIncreased risk of "other solid tumours" with respiratory tract infectionsPathological confirmationMother's hospital obstetric recordsPopulation-based Case–ControlMat: age (to within one calendar month), sex and health board area of residence24.2 Naumburg, 2002 [48] Sweden1973–1989652652≤ 16 yearsChildhood leukaemia (lymphatic and myeloid leukaemia)Lower genital tract infections, UTI, ‘‘other infections’’ (such as pneumonia, gastroenteritis, sinusitis, common cold)Increased risk of childhood leukaemia with lower genital tract infectionRegistryAntenatal, obstetric, and other standardized medical recordsPopulation-based Case–ControlAdj: mothers age, parity, mode of delivery (vaginal or caesarean), maternal smoking, elapsed time from rupture of the membranes to delivery, gestational age at birth, birth weight, birth weight for gestational age, and type of birth (single or multiple); Mat: sex and year and month of birth26.6Oksuzyan, 2013 [49]USA1988–200833083308< 16 yearsCNS and brain tumoursGenital herpes and infections (non-sexually transmitted -including pyelonephritis, hepatitis B and rubella)Increased risk of CNS Tumours with genital herpes; Decreased risk with non STIRegistryRegistryPopulation-based Case–ControlAdj: child's race, birth weight, gestational age, birth order, mother's age, father's education and source of payment for delivery; Mat: date of birth (± 6 months) and sex -cancer free27.4 Olshan, 1993 [50] USA1984–1986200233≤ 15 yearsWilm's TumourVenereal disease, vaginal or UTI, rubella, measles, flu, mononucleosis, chickenpox, genital herpes, or “other infections during pregnancy"Increased risk with "other infections”; no association found for the restPathological confirmationSelf-administered questionnairePopulation-based Case- ControlAdj: household income and father's education; Mat: age at diagnosis and geographic area24.4 Roman, 1997 [16] UK1962–19921773543 months ≤ 29 yearsleukaemia and NHLViral infection, influenza, vulvar warts, herpes simplex, rubellaIncreased risk of leukaemia after viral infection; Increased risk of non-Hodgkin's lymphoma after viral infectionRegistryMother's hospital obstetric recordsPopulation-based Case ControlMat: hospital catchment area of birth, sex and year and month of birth22.6Sepúlveda-Robles, 2025 [63]Mexico2010–201514551455< 18 yearsAcute leukaemiaAny infection, respiratory infection, gastrointestinal infection, UTI, vaginal infectionReduced risk of leukaemia with respiratory infection and UTIPathological confirmationSelf-reported standardized questionnaireHospital-based case controlAdj: child’s sex, age, birth weight, birth order, and standard of livingMat: age and health institution26.6 Shu, 1995 [51] USA, Canada1982–1989105639< 15 yearsMalignant Germ Cell TumoursAny virus infection, UTI, other infectionIncreased in risk of MGCT with UTIRegistrySelf-administered questionnairePopulation-based Case–ControlAdj: age, gender, gestational age, number of livebirths, maternal education, maternal smoking in pregnancy; Mat: area and age24.6 Sirirungreung, 2024 [52] Taiwan2004–201514092,265,777< 15 yearsALL, CNS tumours, Hepatoblastomas and MedulloblastomasMedically diagnosed infection—grouped based on pathogen type (viral or bacterial) and affectedorgan system (such as the respiratory, enteric or urinary tract)Increased risk of ALL after any infectionRegistryInsurance dataCohort studyAdj: sex, birth year, maternal age, family income, urbanization level, parity28.4 Stewart, 1958 [53] UK1955–195712991299Leukaemia, other cancersInfections of genitourinary tract, rubella, mumps, herpes zoster, infective hepatitisNo associationRegistryInterviews by survey doctors on exposure during pregnancyPopulation-based Case–ControlMat: age, sex, locality, live healthy child20.6 Stolt, 2005 [54] Finland1983115918NeuroblastomaPolyomavirus BK and JC virus (Specific IgG and IgM antibodies to BK and JC virus & PCR for BK virus DNA)No associationRegistryFirst trimester sera: Serology—Specific IgG and IgM antibodies to BK and JC virus & Virology: PCR for BK virus DNAnested case–controlAdj: age at serum sampling; Mat: maternal age at serum sampling and municipality of residence22.0 Swerdlow, 1982 [55] UK1953–19738710,128< 16 yearsTesticular CancerCystitis, renal infections, any non-venereal UTI, tuberculosisIncreased risk of cancer death with tuberculosis and cystitis in pregnancyRegistryInterviews and antenatal records where possible on exposure during pregnancyPopulation-based Case Controlno matching/adjustment20.2 Tedeschi, 2009 [56] Finland and Iceland1983–20067052105≤ 20 yearsALL and non-ALLEBV (VCA IgM, early antigen IgG and IgM, ZEBRA IgG and IgM)No associationRegistryFirst-trimester maternal serum antibodiesNested Case–ControlAdj: birth order, sibship size Mat: mother's country, age at serum sampling, date of specimen collection and, for the offspring characteristics, date of birth (2 months) and gender of the child28.4 Van Steensel-Moll, 1985 [57] Netherlands1973–1980519507< 15 yearsALLViral infections—not specifiedNo associationPathological confirmationSelf-administered questionnairePopulation-based case controlAdj: age and sex Mat: date of birth, sex, place of residence26.0 Vasconcelos, 2008 [58] USA, California1995–200289100< 15 yearsALLAdenovirus DNAVirus not detected in casesRegistryPCR on neonatal blood spotsPopulation-based Case ControlMat: birthdates, gender, ethnicity and geographic region of birth18.0 Wang, 2019 [59] China2014–2016345345≤ 15 yearsALLViral infections—rubella, measles, cytomegalovirus, toxoplasma infection, but not including common viral infections like colds and influenzaNo associationPathological confirmationself-reported questionnaire by trained interviewerHospital-based Case–controlAdj: child’s age, gender, residence region, birth weight, delivery mode, household per capita annual income, familial history of leukaemia and other cancer, exposure to pesticides, parental age at delivery, parental educational level, paternal exposure to pesticides, paternal cigarette smoking and paternal heavy alcohol drinking; Mat: age, gender, residency25.6 Wiemels, 2019 [60] Sweden1987–201431982,779,309< 15 yearsHaematological malignancies and CNS tumoursClinically apparent CMVIncreased riskRegistryRegistryRetrospective cohortAdj: congenital malformations, deformations, chromosome abnormalities, and small or large for gestational age28.2Study quality assessed using the self-developed scoring tool from −6 to 45 scoreAbbreviations: Adj adjusted factors, Mat matching factors, ALL acute lymphoblastic leukaemia, CMV cytomegalovirus, CNS central nervous system, EBV Epstein Barr virus, HERV Human endogenous retrovirus, HHV human herpes virus, IgG immunoglobulin, IgM immunoglobulin, MGCT malignant germ-cell tumours, NHL non-Hodgkin lymphoma, PCR polymerase chain reaction, UTI urinary tract infection, STI sexually transmitted infection
The distribution of selected quality-related factors is shown in Table 2. The majority of the 46 papers were case–control studies (n = 39), which included eight nested, 27 population-based, and four hospital-based case–control studies. The remainder were cohort studies (n = 7). For outcome assessment, over half (57%) used registry data [16, 20–23, 25, 27–29, 31, 35, 38, 41, 42, 48, 49, 51–56, 58, 60], 37% used pathological confirmation [20, 24, 26, 34, 36, 39, 40, 43–45, 47, 50, 57, 59, 61–63] and nine percent used medical documentation [15, 30, 37, 46]. For exposure assessment, 74% used non-laboratory data: interviews and self-completed questionnaires [15, 24, 26, 27, 29, 34, 37, 42, 45, 46, 50, 51, 53, 57, 59, 63], medical documentation (antenatal or obstetric records, birth certificates) [16, 20–22, 28, 30, 32, 36, 38, 47, 48, 55, 61], registry data [35, 49, 60], and health insurance data [38, 52]. The remaining 26% of studies used laboratory data (DNA or IgM) [23, 25, 31, 33, 40, 41, 43, 44, 54, 56, 58, 62]. Over 95% controlled for basic confounders only (age, sex, place of residence) while only a few considered more confounders: hepatitis in pregnancy [37], prenatal antibiotic use [42], maternal comorbidities in pregnancy [35] and perinatal factors [37, 42, 45, 46, 48, 49, 51, 59, 60]. Table 2. Quality assessment of studies included in the meta-analysis [15, 16, 20–33, 35–37, 39–48, 50–53, 55–63]
Meta-analysis
The overall analysis showed that maternal infection during pregnancy was associated with an increased risk of childhood cancer (ES = 1.36; 95%CI, 1.17–1.59; I^2^ = 71.2%; p < 0.001; Fig. 2). We observed evidence of publication bias in this analysis; after correcting for publication bias using the trim-and-fill method, four additional studies were added, yielding ES = 1.32; 95%CI, 1.13–1.54) (Additional file 5: Fig. S1). Excluding single studies did not substantially alter the pooled estimate (Additional file 6: Table. S5). Subgroup and meta-regression analyses by study-level characteristics on confounder adjustment, exposure and outcome assessment methods gave similar results in terms of strength and direction of association (Additional file 7: Table. S6 and Additional file 8: Table. S7). However, the effect estimates differed when the analyses were stratified by study period. For example, we did not observe a positive association in the subgroup of recently conducted studies (P_meta-regression_ = 0.014; Additional file 8: Table.S7). When restricted to high-quality studies (n = 10), the association remained positive (ES = 1.25; 95% CI, 0.99–1.58), although it did not reach statistical significance (Additional file 7: Table. S6).Fig. 2. Maternal exposure to any infection during pregnancy and the risk of any type of cancer in children Overall analysis with all studies included in the meta-analysis. Exposure and outcome selection from individual studies depends on broad or general types and a larger number of cases. a crude odds ratio taking matching into account. b Adjusted estimate as indicated by the published study. c no adjustment/matching. d ES includes single-study odds ratios or hazard ratios and summary odds ratios. e first-trimester maternal serum samples. f studies likely to be from the same population. g quality score, high quality ≥ 28.4, low quality < 28.4. Abbreviations: ALL, acute lymphoblastic leukaemia; BC, birth certificate; ES, estimate; CI, confidence interval; CNS, central nervous system; EBV, Epstein Barr virus; GCT, germ cell tumour; HHV6, human herpes virus 6; HI, health insurance; IgM, Immunoglobulin M; JCV, human polyomavirus 2; MR; medical records; mycoplasma p., mycoplasma pneumoniae; NGS, next generational sequencing on neonatal blood spots; PCR, polymerase chain reaction on neonatal blood spot; Reg, registry data; SR, self-report; STI, sexually transmitted infection; SV40, simian virus 40; UTI, urinary tract infection. Weights are from random effect analysis
Associations between any maternal infection during pregnancy and different cancer types are shown in Fig. 3 and Additional file 9: Fig. S2. Any maternal infection during pregnancy was associated with an increased risk of overall leukaemia (ES = 1.27; 95%CI, 1.01–1.60; I^2^ = 79.7%; p < 0.001), ALL (ES = 1.31; 95%CI, 1.04–1.64; I^2^ = 77.8%; p < 0.001) and solid tumours (ES = 1.32; 95%CI,1.05–1.66; I^2^ = 36.7%; p = 0.070) (Fig. 3). We observed publication bias in the analyses for leukaemia and ALL, with weaker pooled estimates after applying the trim and fill method (ES = 1.14; 95% CI, 0.87–1.49 and ES = 1.20; 95% CI, 0.89–1.62; Additional file 5: Fig. S1). Results from the leave-one-out sensitivity analysis indicated that omitting any single study did not substantially alter the pooled estimates, suggesting that the findings were robust (Additional file 6: Table. S5). However, we noted weaker associations when the analysis was limited to recently conducted studies (P_meta-regression_ = 0.009) and slightly stronger associations in cohort studies (P_meta-regression_ = 0.014) for any maternal infection and risk of ALL (Additional file 8: Table. S7).Fig. 3. Maternal exposure to any infection during pregnancy and risk of leukaemia (all subtypes), ALL and solid tumours. Leukaemia includes all subtypes; solid tumours include Wilms tumours, retinoblastomas, hepatoblastomas, malignant germ cell tumours, and testicular cancers. a crude odds ratio taking matching into account. b Adjusted estimate as indicated by published study. c no adjustment/matching. d ES includes single-study odds ratios or hazard ratios and summary odds ratios. e first-trimester maternal serum samples. f studies likely to be from the same population. g quality score, high quality ≥ 28.4, low quality < 28.4. Abbreviations: ALL, acute lymphoblastic leukaemia; AN, antenatal; CI, confidence interval; CMV, cytomegalovirus; EBV, Epstein-Barr virus; ES, estimate; HBV, hepatitis B virus; HHV6, human herpes virus 6; IgM, Immunoglobulin M; med records, medical records; mycoplasma p., mycoplasma pneumoniae; NGS, next-generation sequencing on neonatal blood spot; PCR, polymerase chain reaction on neonatal blood spot; UTI, urinary tract infection; STI, sexually transmitted infection. Weights are from random effect analysis
Associations between specific maternal infections during pregnancy and overall childhood cancer are shown in Fig. 4, Additional file 10: Fig. S3, Additional file 11: Fig. S4 and Additional file 12: Fig. S5. STIs were associated with an increased risk of overall childhood cancer (ES = 2.86; 95%CI, 1.88–4.33;* I*^2^ = 23.6%; p = 0.249; Fig. 4). Viral infection (ES = 1.43; 95% CI, 1.18–1.74; I^2^ = 52.3%; p < 0.001; Additional file 10: Fig. S3), cytomegalovirus (CMV) infection (ES = 2.10; 95%CI, 1.02–4.34; I^2^ = 67.1%; p = 0.010) and rubella infection (ES = 2.04; 95%CI, 1.11–3.75; I^2^ = 0%; p = 0.738; Additional file 11: Fig. S4) were associated with an increased risk of childhood cancer. GUTIs (ES = 1.52; 95%CI, 1.05–2.19; I^2^ = 69.3%; p = 0.001) were also associated with an increased risk of childhood cancer (Additional file 12: Fig. S5). We observed publication bias only for the analyses of viral infections and childhood cancer, with the estimate changing marginally after adjustment using the trim-and-fill method with three additional studies included (ES = 1.40; 95%CI, 1.14–1.71; Additional file 5: Fig. S1). Although study-level characteristics did not appear to influence these associations, our subgroup analysis assessing the CMV and risk of childhood cancer showed a stronger association in cohort studies. The leave-one-out sensitivity analysis indicated that the results were robust for most associations. However, the positive association between CMV infection and the risk of childhood cancer emerged only after excluding the studies by Holl et al., 2008 [40] and Lehtinen et al., 2003 [43], whereas the association for EBV infection became significant only when the study by Tedeschi et al., 2009 [56], was excluded (Additional file 6: Table. S5). When restricted to high-quality studies the association remained strongly positive for between STIs (n = 4; ES = 2.44; 95% CI, 1.36–4.38) and GUTIs (n = 1; ES = 2.42; 95%CI,1.50–3.91) and were weaker for viral infections (n = 7; ES = 1.35;95%CI,0.95–1.86) and CMV infection (n = 3; ES = 1.73;95%CI,0.68–4.39) (Additional file 7: Table. S6). All the studies in the analysis of rubella infection and childhood cancer were of low-quality (Additional file 7: Table. S6). We did not find an association between bacterial infections and childhood cancer risk.Fig. 4. Maternal sexually transmitted infections (STIs) during pregnancy and the risk of overall childhood cancer STIs here include broad categorization of STIs (collectively including chlamydia, gonorrhoea, genital ulcers, genital herpes, human papillomavirus, vulvar warts) and specific STIs in the studies by Roman, 1997 [16] (vulvar warts), Lehtinen, 2005 [44] (chlamydia) and Oksuzyan, 2013 [49] (genital herpes). a crude odds ratio taking matching into account. b Adjusted estimate as indicated by published study. c Quality score, high quality ≥ 28.1, low quality < 28.1. d ES includes single-study odds ratios or hazard ratios and summary odds ratios. e first-trimester maternal serum samples. Abbreviations: ALL, acute lymphoblastic leukaemia; CNS, central nervous system; ES, estimate; CI, confidence interval; IgM, Immunoglobulin M. Weights are from random effect analysis
Associations between specific maternal infections during pregnancy and specific cancer types are shown in Figs. 5, 6 and 7 and Additional file 13: Fig. S6 and Additional file 14: Fig. S7. GUTI was associated with an increased risk of leukaemia (ES = 1.49; 95%CI,1.05–2.12;* I*^2^ = 67.1%; p = 0.006; Fig. 5). Viral infection (ES = 1.58; 95%CI, 1.15–2.18; I^2^ = 57.0%;* p* = 0.001) and specifically influenza (ES = 3.41; 95%CI, 1.28–9.13; I^2^ = 53.7%;* p* = 0.090) were associated with an increased risk of ALL subtype (Fig. 6). GUTI was associated with an increased risk of solid tumours (ES = 1.60; 95%CI, 1.06–2.42; I^2^ = 63.3%;* p* = 0.005; Fig. 7). This association was weaker when the analysis was limited to cohort studies (P_meta-regression_ < 0.001) and to studies that adjusted for additional confounders (P_meta-regression_ = 0.006), whereas slightly stronger associations were observed for studies that used medical records as exposure assessment methods (P_meta-regression_ = 0.019). In the analyses assessing GUTIs and risk of leukaemia, we observed a weaker association for the subgroup of case–control studies and in those relying on self-reports for exposure assessment (Additional file 8: Table. S7). The leave-one-out sensitivity analysis revealed that the association between influenza infection and the risk of leukaemia became apparent only after the exclusion of one study by Dockerty et al. Similarly, an association between viral infection and the risk of solid tumours was observed when either the study by Shu et al. or Ma et al. was excluded (Additional file 6: Table. S5). Publication bias was not observed in these analyses. The detailed results for sensitivity analyses and subgroup analyses by study-level characteristics for each observed association are summarized in Additional file 6: Table. S5, Additional file 7: Table. S6 and Additional file 8: Table. S7. Fig. 5. Specific maternal infections during pregnancy and the risk of leukaemia. a quality score, high quality ≥ 28.4, low quality < 28.4. b ES includes single-study odds ratios or hazard ratios and summary odds ratios. c Adjusted estimate as indicated by published study. d crude odds ratio taking matching into account. e no adjustment/matching. f first-trimester maternal serum samples. Abbreviations: ES, estimate; CI, confidence interval; IgM, Immunoglobulin M; NGS, next-generation sequencing; NBS, neonatal blood spot; PCR, polymerase chain reaction. Weights are from random effect analysisFig. 6Specific maternal infections during pregnancy and the risk of acute lymphoblastic leukaemia (ALL). a quality score, high quality ≥ 28.4, low quality < 28.4. b ES includes single-study odds ratios or hazard ratios and summary odds ratios. c Adjusted estimate as indicated by published study. d crude odds ratio taking matching into account. e no adjustment/matching. f first-trimester maternal serum samples. Abbreviations: ALL, acute lymphoblastic leukaemia; CI, confidence interval; CMV, cytomegalovirus; IgM, Immunoglobulin M; EBV, Epstein Barr virus; ES, estimate; med records, medical records; NGS, next-generation sequencing on neonatal blood spot; PCR, polymerase chain reaction on neonatal blood spot. Weights are from random effect analysisFig. 7Specific maternal infections during pregnancy and the risk of solid tumours. Solid tumours include those broadly categorized as “solid tumours” in the studies and individual solid tumour types in specific studies: Wilms tumours, retinoblastomas, hepatoblastomas, malignant germ cell tumours, and testicular cancers. Viral infection types in this category include general viral infection and specific viral infections such as influenza, common cold, Epstein-Barr virus and genital herpes (a) quality score, high quality ≥ 28.4, low quality < 28.4. b ES includes single-study odds ratios or hazard ratios and summary odds ratios. c Adjusted estimate as indicated by published study. d crude odds ratio taking matching into account. e no adjustment/matching. f cancers except leukaemia, brain tumours and lymphomas. Abbreviations: ES, estimate; CI, confidence interval; IgM, Immunoglobulin M; IgG, Immunoglobulin G. Weights are from random effect analysis
Discussion
Our meta-analysis demonstrates a positive association between maternal infections during pregnancy and the risk of cancer in the offspring overall, and particularly leukaemia and solid tumours. Notably, STIs, GUTIs and viral infections were associated with an increased cancer risk in the offspring. There are some biologically plausible mechanisms linking specific maternal infections to the development of certain childhood cancers. We discuss these potential links by examining the results according to both the type of infection and the type of cancer outcome.
Sexually Transmitted Infections (STIs)
We found that STIs of the mother during pregnancy were associated with an increased risk of cancer in the offspring as supported by seven studies, four of which were high-quality studies: one cohort study using registry-confirmed infections [35] and three high-quality case–control studies, using birth certificates and registry data [35, 36, 49] for infection assessment and maternal bacterial antibodies [44] respectively. Majority of the studies examined STIs (including chlamydia, gonorrhoea, genital ulcers, genital herpes, human papilloma virus (HPV)) as a broad group of infections, except for three studies which considered chlamydia, genital herpes and vulvar warts separately [16, 44, 49]. The positive association persisted across all subgroup analyses based on study-level characteristics. In addition, we confirmed with the leave-one-out cross-validation method that the association was not driven by a single study, highlighting the robustness of our finding. These methodological considerations provide strong evidence supporting a positive association between maternal STIs during pregnancy and childhood cancer. Previous research has reported potential biological mechanisms linking STIs during pregnancy to adverse outcomes in offspring. For example, bacterial STIs from ascending infections such as chlamydia and gonorrhoea, and transplacentally transmitted infections like syphilis, can lead to perinatal complications such as preterm birth and low birth weight and congenital anomalies, which are risk factors for various childhood cancers [8, 67–69]. Persistent inflammation and cellular damage triggered by STIs may create a micro environment conducive to carcinogenesis in the developing foetus [70]. Similarly, viral STIs such as HPV also present a potential risk, although vertical transmission is relatively rare [71], HPV DNA has been detected in placenta, amniotic fluid and foetal membranes, implying in utero transmission [71, 72]. HPV’s ability to persist, activate and replicate in differentiated squamous epithelial cells [73] may explain associations observed with certain epithelial-origin childhood cancers, such as retinoblastomas [74] and CNS tumours. While we could not assess individual STIs due to lack of pathogen-specific data in most studies, the consistent associations observed in high-quality studies, together with the biological mechanisms discussed, strengthen the evidence for the association between STIs in pregnancy and cancer in the offspring. Nonetheless, we cannot rule out the possibility of residual confounding from unmeasured confounders such as maternal smoking, alcohol use, or other health behaviours that may be associated both with STI and childhood cancer.
Genitourinary Tract Infections (GUTIs)
GUTIs during pregnancy were associated with an increased risk of overall childhood cancers, particularly leukaemia and solid tumours. For leukaemia, the analysis was based on seven studies with the positive association persisting across study-level characteristics including confounder adjustment and study quality. A strong positive association was found in the only high-quality study which was a cohort study design with record-based exposure assessment and adjustment for key confounders [35], with evidence of weaker associations in the remaining studies. This aligns with the previous meta-analysis by He [9], strengthening the evidence for the association between GUTIs and leukaemia.
For the association between GUTIs during pregnancy and risk of solid tumours, the analysis was based on nine studies of various tumour types (germ-cell tumours, hepatic tumours, hepatoblastomas, retinoblastomas, testicular cancers, and Wilms tumours) [24, 36, 37, 47, 50, 51, 55]. Due to the small number of individual solid tumour cases, we analysed these outcomes collectively. Our subgroup analysis showed a weaker association in studies with a cohort design and in those that reported estimates adjusted for additional confounders. The positive association was no longer observed in the more recently conducted studies. Further, the positive association with solid tumours was weaker in high-quality studies and was mainly driven by a single study on retinoblastomas [36], limiting its generalizability to other solid tumours and suggesting that GUTIs may specifically influence the risk of retinoblastomas. It is also plausible that there may be some confounding factors that may have led to this result, or the result could be a random observation. Nevertheless, GUTIs may be vertically transmitted across the maternal-foetal membranes and may cause an altered foetal immune response [8] or indirectly trigger a foetal inflammatory response through the infection metabolites, which can mediate epigenetic changes and subsequently increase cancer susceptibility [7].
Viral infections
Our meta-analysis found that maternal viral infections during pregnancy were associated with an increased risk of childhood cancer overall and particularly with ALL. Specifically, CMV and rubella virus infection showed an elevated risk of overall childhood cancer, while influenza infection was positively associated with ALL, aligning with findings from He et al. [9]. Several biological mechanisms may underlie these associations. In the development of childhood leukaemia specifically, the current theory postulates a two-stage process: the first “stage” occurs in utero, where viral integration or inflammation induces initial genetic changes, and the second postnatally, with additional mutations or environmental factors driving leukaemia progression [75]. Viral infections, such as influenza and CMV, may cause damage and inflammation to the placenta and alter the microenvironment of the foetal bone marrow, promoting leukemogenesis. Although these mechanisms are biologically plausible in linking viral infections to childhood cancer, evidence from high-quality studies in our meta-analysis was weaker. Further, for influenza, the exposure assessment mainly relied on self-reported symptoms rather than laboratory-confirmed diagnoses, raising a possibility of misclassification as there are other flu-like illnesses such as CMV, which may partly explain the observed association between “influenza” and leukaemia risk. For rubella, the findings were from few studies of low-quality evidence, limiting their validity. Although no studies in our meta-analysis captured exposures during the COVID-19 pandemic, the potential for viral-modulated effects remains relevant. A recent 2025 study by Behnaz et al. [76] examined early exposure to COVID-19, combining the pre-pregnancy and pregnancy periods, and reported an increased risk of childhood cancer in offspring. Although this study was not included in our meta-analysis due to its combined exposure period, it highlights the need for further research on infections during the post-pandemic period to better understand the potential effects on childhood cancer risk.
Bacterial vs. viral aetiology
In the present meta-analysis, we observed that maternal viral infections were more strongly associated with childhood cancer risk than bacterial infections. However, this may be influenced by the fact that evidence on bacterial infections is limited, with only four studies assessing their association compared to 36 studies on viral infections. Furthermore, since most studies assessing STIs and GUTIs included in the meta-analysis did not specify the causative pathogens, we could not confirm this assumption. Nevertheless, we acknowledge the need to further explore the biological mechanisms linking bacterial infections to childhood cancers. While viral infections have been more extensively studied in relation to oncogenesis, bacterial infections may also play a role through distinct mechanisms. For instance, Escherichia coli (E.coli) is the most common cause of GUTIs, and several STIs including chlamydia, gonorrhoea, and syphilis, are of bacterial origin. Although the evidence on bacterial infections and childhood cancer risk remains limited, the association is biologically plausible. Bacterial infections during pregnancy may ascend the genital tract or cross the placenta, triggering inflammatory responses. Such inflammation could lead to epigenetic modifications or adverse birth outcomes like low birth weight and prematurity, both of which have been linked to increased cancer risk in the offspring. A clearer distinction between bacterial and viral mechanisms is needed in future research to better understand their respective roles in early-life cancer development.
Medication use and inflammatory pathways
Beyond all the aforementioned mechanisms linking maternal infections during pregnancy to cancer in the offspring, medications that act through inflammatory pathways, such as fever-reducing analgesics, could influence the development of childhood cancers as observed in our meta-analysis between medications during pregnancy and childhood cancer risk [77].
Strengths and limitations
The strengths of our analysis include the assessment of diverse infections and cancer outcomes that have not been comprehensively studied before, providing a broader understanding of maternal infections in pregnancy and risk of childhood cancer. We set a minimum threshold of three studies per analysis, which potentially improved the statistical power and reduced potential outlier effects. Our self-developed quality assessment tool allowed for a thorough appraisal of the studies with methodology and risk of bias considerations. We conducted extensive sensitivity and subgroup analyses to assess heterogeneity, which improved the interpretability and robustness of our results.
However, our systematic review and meta-analysis has several limitations that should be considered when interpreting the findings. Firstly, most studies in this meta-analysis relied on maternal self-reported infections during pregnancy, which may be prone to recall bias. While such misclassification is often assumed to be non-differential, the predominance of case–control designs in the included studies raises the possibility of differential misclassification, as mothers of affected children may recall exposures differently from controls. As a result, the direction of bias cannot be assumed, consistent with recent methodological discussions [78]. Secondly, the inadequate adjustment of key confounders such as perinatal factors, other infections during pregnancy, maternal health behaviours (including smoking or alcohol consumption) and comorbidities may have complicated isolating the effects of maternal infections during pregnancy on cancer in the offspring. Thirdly, the general lack of precise timing regarding gestational age at infection limits our ability to identify potential windows of vulnerability, which could inform prevention strategies. Furthermore, most of the included studies did not distinguish between acute and chronic infections or the severity of the infections, which hindered deeper insights into the mechanisms of the association with childhood cancer and the risk categorisation. Our observation of publication bias in the analysis for overall maternal infections and overall cancer risk, leukaemia and ALL, and for viral infections and overall cancer risk may have led to an overestimation of the true association and a distorted conclusion, as studies with significant findings are more likely to be published than those with null results. However, the trim-and-fill method yielded only modestly attenuated pooled estimates, indicating that the association between maternal infections during pregnancy and childhood cancer risk remained largely consistent. Lastly, our attempt to explore general potential mechanisms by pooling diverse infection types and cancer outcomes may have resulted in biased estimates. However, the overall association remains biologically plausible given the role of inflammation in carcinogenesis.
Conclusions
In conclusion, our systematic review and meta-analysis indicates that maternal infections during pregnancy are associated with an increased risk of childhood cancer. Specifically, STIs, GUTIs, and viral infections showed increased risk of overall childhood cancer, with GUTIs and viral infections also linked to higher risk of leukaemias. In light of these findings, primary prevention of pregnancy infections may be a valuable strategy to reduce potential cancer risk in offspring. Promoting good health and hygiene practices, as well as vaccinations against vaccine-preventable diseases such as influenza during pregnancy, could offer benefits beyond immediate maternal and foetal health. For STIs and GUTIs, routine screening and timely treatment, where available, may help prevent adverse perinatal outcomes and, potentially, long-term health risks, including cancer in children. As research on the subject of maternal infections and cancer risk is still currently underdeveloped, there is a need for large-scale prospective studies stratified by pathogen type as well as mechanistic studies to advance knowledge in this area. Future research should provide a comprehensive exposure assessment that considers the timing, chronicity, severity, and therapeutic interventions for maternal infections during pregnancy, as these factors may yield valuable insights.
Supplementary Information
Additional file 1: Table. S1: PRISMA checklist.Additional file 2: Table. S2: Search strategy.Additional file 3: Table. S3: Extracted data and estimates for the meta-analysis Abbreviations: AML, acute myeloid leukaemia; ALL; acute lymphoblastic leukaemia; CMV, cytomegalovirus; CNS, central nervous system; EBV, Epstein Barr virus; ES estimate; IgG, immunoglobulin G; IgM, immunoglobulin M; LCI, lower confidence interval; NHL, non-Hodgkin lymphoma; TTV, torque teno virus; TTMV, torque teno mini virus ; TTMDV, torque teno midi virus; UCI, upper confidence interval; UTI, urinary tract infection.Additional file 4: Table. S4: Studies excluded from systematic review and meta-analysis. Additional file 5: Fig.S1: Publication bias for maternal infection during pregnancy and risk of cancer. Trim and fill analyses were conducted for meta-analyses with evidence of publication bias. Abbreviations: CI, confidence interval; Conf, confidence; Eff, effect; Err, error; logor, log odds ratio; MSE, mean square error; P, P-value; REML, restricted maximum likelihood; se; standard error; SND, standard normal deviate; Std, standard.Additional file 6: Table. S5: Sensitivity analysis – leave-one-out meta-analysis.Additional file 7: Table. S6: Summary of meta-analyses showing positive associations. Heterogeneity was examined with the I² statistic, categorized as low (≤50%), moderate (>50-75%), or substantial (>75%), with statistical significance assessed using the Q statistic (P-value for heterogeneity).Study quality (maximal score = 45) was stratified above the 4th quintile for quality score (≥28.4 = high quality) and below (<28.4 = low quality). Publication bias was assessed using Egger tests and funnel plots for analyses which had at least 5 studies. Abbreviations. ALL, acute lymphoblastic leukaemia; CI, confidence interval; CMV cytomegalovirus.Additional file 8: Table. S7: Subgroup analyses of observed associations by study-level characteristics. *P values for the subgroups are calculated using meta-regression, some P values not possible/not done due to few available studies for meta-regression, and some omitted due to collinearity. For exposure assessment, if studies report more than one method of assessment the most valid exposure assessment method is chosen. For outcome assessment, no registry means outcome assessed using methods other than registry or pathological confirmation. For confounder adjustment, basic means matching, or adjustment for basic characteristics e.g., age, sex, region; other factors include adjustments for comorbidities, genetic disorders, proxies for infection exposure such as sibship size, mode of delivery; similar factors include adjustments for other infections and antibiotics. Quality, high ≥ 28.4, cut off and low < 28.4 from the quality assessment tool. Abbreviations: ES estimate; UCI, upper confidence interval; LCI, lower confidence interval; Ref, reference value for subgroup analyses involving three categories.Additional file 9: Fig.S2: Maternal exposure to any infection during pregnancy and the risk of CNS tumours and neuroblastomas and lymphoma. Lymphoma includes all subtypes. a) crude odds ratio taking matching into account. (b) Adjusted estimate as indicated by published study. (c) no adjustment/matching. (d) ES includes single-study odds ratios or hazard ratios and summary odds ratios. (e) first-trimester maternal serum samples. (f) quality score, high quality ≥28.4, low quality <28.4. Abbreviations: CNS, central nervous system; CI, confidence interval; ES, estimate; IgM, immunoglobulin M; JCV, human polyomavirus 2; SV 40, simian virus 40. med records, medical records. Weights are from random effect analysis.Additional file 10: Fig.S3: Maternal Infection by type of pathogen – viral and bacterial, and overall childhood cancer risk. Abbreviations: ES, estimate; CI confidence interval.Additional file 11: Fig.S4: Specific viral infections and overall childhood cancer risk. Abbreviations: CMV, cytomegalovirus; EBV, epstein-barr virus; ES, estimate. CI, confidence interval.Additional file 12: Fig.S5: Maternal Infection by affected body system and overall childhood cancer risk. Abbreviations: ES, estimate; CI, confidence interval.Additional file 13: Fig.S6: Specific maternal infections during pregnancy and the risk of central nervous system tumours and neuroblastomas. (a) quality score, high quality ≥28.4, low quality <28.4. (b) ES includes single-study odds ratios or hazard ratios and summary odds ratios. (c) Adjusted estimate as indicated by published study. (d) crude odds ratio taking matching into account. (e) no adjustment/matching. (f) first-trimester maternal serum samples. Abbreviations: CNS, central nervous system; ES, estimate; CI, confidence interval; IgM, Immunoglobulin M; IgG, Immunoglobulin G. Weights are from random effect analysis.Additional file 14: Fig.S7: Maternal viral infection during pregnancy and the risk of lymphoma. Lymphoma includes all subtypes. (a) quality score, high quality ≥28.4, low quality <28.4. (b) ES includes single-study odds ratios or hazard ratios and summary odds ratios. (c) Adjusted estimate as indicated by published study. (d) crude odds ratio taking matching into account. Abbreviations: ES, estimate; CI, confidence interval. Weights are from random effect analysis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kumar M, Saadaoui M, Al Khodor S. Infections and Pregnancy: Effects on Maternal and Child Health. Front Cell Infect Microbiol. 2022;12:873253.10.3389/fcimb.2022.873253 PMC 921774035755838 · doi ↗ · pubmed ↗
- 2Djomkam Zune AL, Olwal CO, Tapela K, Owoicho O, Nganyewo NN, Lyko F, et al. Pathogen-Induced Epigenetic Modifications in Cancers: Implications for Prevention, Detection and Treatment of Cancers in Africa. Cancers (Basel). 2021;13(23):6051.10.3390/cancers 13236051 PMC 865676834885162 · doi ↗ · pubmed ↗
- 3Ma SN, Hu XT, Cai WS. Association between exposure during pregnancy and the risk of developing solid tumors in second children: Results from a Chinese matched case-control study. Early Hum Develop. 2021;154:105292.10.1016/j.earlhumdev.2020.10529233517172 · doi ↗ · pubmed ↗
- 4Sepúlveda-Robles O, Flores-Lujano J, Núñez-Enríquez JC, Jiménez-Hernández E, Duarte-Rodríguez DA, Martín-Trejo JA, et al. Early Infection Incidence and Risk of Acute Leukemia Development Among Mexican Children. Cancers. 2025;17(5):733.10.3390/cancers 17050733 PMC 1189964640075581 · doi ↗ · pubmed ↗
- 5Lübtow A, Marron M, Nagrani R, Mulanje L, Ahrens W, Brackmann LK. Prenatal exposure to medication and risk of childhood cancer: a systematic review and meta-analysis. BMC Cancer. 2025;25:1841. 10.1186/s 12885-025-15316-0.10.1186/s 12885-025-15316-0PMC 1266706241272611 · doi ↗ · pubmed ↗