Comparative study between lateral extra-articular tenodesis versus anterolateral ligament reconstruction in combination with anterior cruciate ligament reconstruction
Hossam El-Azab, Omar Abdelkareem, Abdel Rahman Hafez, Moustafa Elsayed, Mohamed Ali

TL;DR
This study compares two surgical techniques used alongside ACL reconstruction and finds both improve knee stability, with no significant difference in outcomes after two years.
Contribution
A direct comparison of lateral extra-articular tenodesis and anterolateral ligament reconstruction combined with ACL-R in a prospective randomized clinical trial.
Findings
Both LET and ALL groups showed significant improvement in Tegner-Lysholm scores after two years.
No significant difference in clinical outcomes or failure rates between the two groups.
Both procedures reduced the number of patients with positive pivot shift and Lachman tests.
Abstract
Residual laxity after anterior cruciate ligament reconstruction (ACL-R) is found in some cases. Nowadays, anterolateral augmentation procedures are performed to prevent this laxity. A prospective randomized comparative clinical study took place from January 2021 to November 2022. The study included 48 patients after exclusion of losses to follow-up, who acquired ACL-R combined with either lateral extraarticular tenodesis (LET) in 25 or anterolateral reconstruction (ALL) in 23 patients. The patients were evaluated with the Tegner-Lysholm score, and follow-up was for 26 ± 7 months. Also, laxity tests, pivot shift and Lachman preoperatively and postoperatively were evaluated. The failure rate was assessed. Tegner-Lysholm score improved significantly from 51.28 preoperatively to 93.76 points two years postoperatively in the LET-group and from 54.55 preoperatively to 94.23 points two years…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
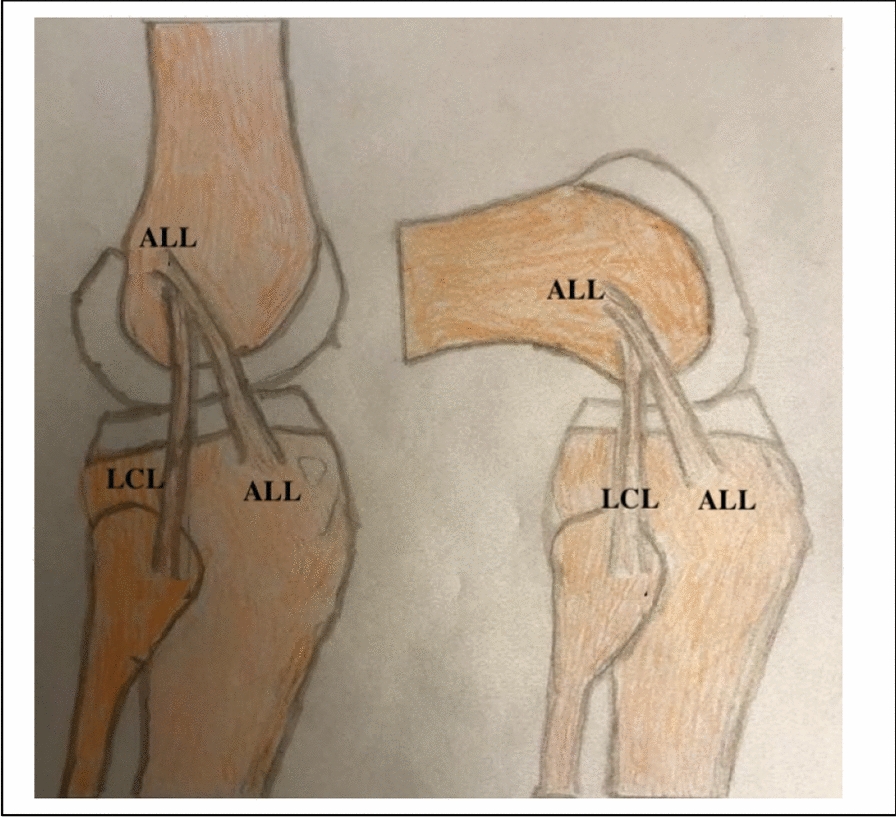 Fig. 11
Fig. 11- —Sohag University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Total Knee Arthroplasty Outcomes · Lower Extremity Biomechanics and Pathologies
Introduction
Residual instability of the knee joint remains a major concern after successful anterior cruciate ligament reconstructions (ACL-R). It accounts for more than 25% of patients [1]. Those patients complain of an inability to return to their previous level of sports [2–4].
Recently, considerable attention has been given to residual instability of the knee as a major issue regarding when patient can return to sports after ACL-R [5]. This instability should be addressed at the time of ACL surgery to improve patient outcomes [6]. Addressing this instability can be done with an anterolateral augmentation. The anterolateral augmentation procedures are either lateral extraarticular tenodesis (LET) or anterolateral ligament reconstruction (ALL-R) techniques [6–8].
There are many techniques for LET from the iliotibial band (ITB) for the femoral side attachment, either an interference screw, staple, a suture anchor [9] or only a high-resistance suture [10].
Also, many modifications in ALL reconstruction techniques have been reported, all of which suggest varying femoral fixation points [11]. Also, ALL grafts are tendons, either from the hamstring or the peroneus longus [12].
Despite the biomechanical evidence suggesting that LET or ALL combined with ACL-R have a better outcome regarding anterolateral instability compared with isolated ACLRs [13–17], the clinical differences of these procedures are still debatable.
The comparison of either additional procedure to ACL reconstruction was the objective of this study. The hypothesis was that tendon reconstruction in ALL is better than the iliotibial tract tenodesis in the LET technique in combination with ACL-R.
Materials and methods
This study was conducted to determine which of the two maneuvers is better to augment ACL-R, either with ALL or LET procedures, to improve the outcome. The study was approved by the local ethics committee with the approval number 395/2020. Informed consent was signed by every patient before participation. A prospective randomized comparative clinical study with a parallel group design took place from January 2021 to November 2022. Sixty patients with an ACL tear and highly positive pivot shift tests (grade II or III) were operated on, and follow-up was for 26 ± 7 months. Randomization was performed at patient admission to allocate the patients into two groups, 50% each: ACL-R with LET and ACL-R with ALL.
Patient demographic data are enumerated in Table 1.Table 1. Patient demographic data (N. 25; LET and No. 23 ALL groups)ParameterLET groupALL groupMean age at surgery (years) (SD)26 (**± 6.7)24 (± 5.4)Male/female21/419/4Athletes2118Professional75Side (right/left)17/816/7Mechanism of injurySport injurySocialMotor car accident15641553Interval between injury and surgery (months) [18]8 (± 3.7)7 (± **5.7)Meniscal surgeryMeniscal-repair No (%)Menisectomy No (%)4 (16%)7 (28%)4 (17.4%)6 (26%)N: Number, SD: standard deviation
Patients were collected from the sports medicine clinic, examined clinically, and investigated with MRI.
Inclusion criteria
- ACL rupture detected by clinical examination and Magnetic Resonance Imaging (MRI).
- Skeletally mature patient (Age 18–35 years).
- High positive pivot shift test of grade II or III.
Exclusion criteria
- Revisions or ACL rupture in the opposite knee.
- Multiple Ligament injuries.
- Articular cartilage defect requiring treatment; Outerbridge more than grade II.
- Malalignment, more than three degrees (varus or valgus)
- General hyperlaxity.
Surgical technique
Anatomic ACL reconstruction was performed in a standardized fashion by the same surgeon in all cases. Choice of procedure was made on admission to the department before surgery, either to do ACL-R combined with LET or ALL in a 1:1 ratio with complete randomization.
ACL-R with LET
ACL-R was performed in the standard fashion using a triple hamstring graft [19, 20]. Semitendonosus-Gracilis (STG) tendon graft (6 strands). Femoral and tibial fixations were performed with bioabsorbable interference screws (Smith & Nephew Endoscopy). Then, the modified Lamaire procedure was performed according to.
Getgood et al. [21] (Figs. 1, 2, 3 and 4). The iliotibial band graft diameter was measured. Fixation at the distal femur was done with the knee held at 60° of flexion and neutral rotation of the tibia.Fig. 1. Illustration showing LET technique
Fig. 2. Intra-operative photo, present strand of LET in the ITB before cutting
Fig. 3. Intra-operative photo showing how the prepared ITB graft passed under LCL
Fig. 4. Intra-operative photo showing fixation of LET graft in the femoral tunnel by an interreference screw
ACL-R with ALL
ACL-R was performed in the standard fashion according to de Oliveira et al. [22] STG in quadruple strands [20] plus the peroneus longus tendon in a single strand (total 5 strands) (Fig. 5). ACL-graft and peroneus longus tendon graft diameters were measured. Femoral and tibial fixations were performed with bioabsorbable interference screws (Smith & Nephew Endoscopy). Fixation of the ALL graft at the proximal tibia with the knee held at 30° of flexion and mild valgus ( Figs. 6, 7 and 8).Fig. 5. Intra-operative photo showing the quintuple (5 strands, 4 hamstrings + one peroneus longus) graft for ALL
Fig. 6. Illustration of ALL technique in the knee,
Fig. 7. Intra-operative photo showing the single strand peroneus longus graft emerging at femoral opening
Fig. 8. Intra-operative photo showing the single strand peroneus longus graft routed downwards to the proximal tibia, emerging at proximal tibia
Rehabilitation
All patients, whatever the group, underwent identical postoperative physiotherapy rehabilitation unless a meniscal repair was concomitantly done. Meniscal repair was performed in eight patients (four in the LET group and four in the ALL group). Attention was given to meniscus repair in the first six weeks [23], then they continued the rehabilitation program as the other patients.
Rehabilitation was tailored for each patient, and postoperative visits were frequent for the professional players to guide them. It aimed at preventing reinjury and enabling return to sports [24].
Physical rehabilitation for ACL-R with augmentation was carried out as reported by El-Azab et al. [25].
Outcome measures
The primary outcome measure was the Tegner-Lysholm Knee Score (TLS) [26], designed to evaluate the clinical outcomes of knee ligament surgery, particularly for symptoms related to instability; therefore, it was suitable.
TLS was originally published in 1982 and later modified in 1985 [26] and is a patient-reported questionnaire consisting of pain (25 points), instability (25 points), locking (15 points), swelling (10 points), limp (5 points), stair climbing (10 points), squatting (5 points), and the need for support (5 points). Scores range from 0 (maximum instability) to 100 (no instability). The examination was done both preoperatively (preop.) and at two-year postoperatively (postop.).
Secondary outcome measures were the pivot shift test and its grading according to Jakop [27], the Lachman test and its grading according to Gurtler [28], and complications (Table 6).
Follow-up examinations were done in the outpatient clinic and planned for 2 weeks, 6 weeks, 6 months, 1 year, and 2 years postoperatively. Professional athletes were followed as the other patients, but at nine months, follow-up was weekly during their return to play to guide them.
In the last follow-up, patients filled out TLS helped by the clinician, who explained and translated the score. To reduce bias, the clinician was blinded to the clinical data, and the patients’ knees were covered with a bandage to hide individual groups.
Statistical analysis
Analysis of data was done with SPSS software (Version 25; SPSS Inc, Chicago, Illinois, USA). Descriptive statistics for variables such as age, sex, duration of symptoms, and concomitant meniscus lesion were calculated. The mean was calculated for the TLS score. Paired student tests (P-value) were used to compare TLS before and two years after the operation and between individual groups at the final follow-up. A p-value of less than or equal to 0.05 was considered statistically significant.
In this study, we used a convenience sample, where all cases admitted to the hospital in the study period, between January 2021 and November 2022, who agreed to the inclusion and exclusion criteria and agreed to participate in the study, were included. So, power analysis was not performed.
Result
Sixty consecutive patients were operated on in both groups. There were 49 men and 11 women, 38 right and 22 left knees. (Table 1). Five patients from the LET group and seven patients from the ALL group were lost to follow-up. Finally, 48 patients (80%) or knees, as there were no bilateral cases, participated in the study. Further, at the final follow-up, two patients from each group were excluded due to ACL-R failure. Therefore, there were 23 patients in the LET group and 21 patients in the ALL group.
TLS in both LET and ALL groups showed significant improvement after two years (Tables 2 and 3). However, the improvement at two-year follow-up between both groups was nonsignificant (P-value = 0.24) (Table 4).Table 2. Tegner-Lyshom score for the group of LET, preop. and postop. (N. 25 at surgery and 23 at two-year follow-up) (Fig. 9)Tegner-Lyshom scoreTegner-Lyshom score preopTegner-Lyshom scorePostopP-valueLimp (5 points)1.88 ± 3.34.36 ± 0.2 < 0.00001Support (5 points)4.04 ± 2.74.28 ± 0.70.004638Locking (15 points)8.12 ± 7.414.2 ± 0.7 < 0.00001Instability (25 points)8.8 ± 6.523.8 ± 0.8 < 0.00001Pain (25 points)14.4 ± 5.324.0 ± 0.8 < 0.00001Swelling (10 points)5.68 ± 2.48.72 ± 0.5 < 0.00001Stair-climbing (10 points)4.96 ± 3.69.04 ± 0.5 < 0.00001Squatting (5 points)3.4 ± 2.54.36 ± 0.6 < 0.00001Total (100 points)51.28 ± 19.6293.76 ± 15.33 < 0.00001Preop: Preoperative, Postop: PostoperativeTable 3Tegner-Lyshom score for the group of ALL, preop. and postop. (N. 23 at surgery and 21 at two-year follow-up) (Fig. 9)Tegner-Lyshom scoreTegner-Lyshom score preopTegner-Lyshom scorepostopP-valueLimp (5 points)1.91 ± 2.44.26 ± 0.4 < 0 00001Support (5 points)3.08 ± 1.74.36 ± 0.60.009597Locking (15 points)7.86 ± 6.513.91 ± 0.8 < 0.00001Instability (25 points)6.89 ± 7.723.8 ± 1.2 < 0.00001Pain (25 points)13.08 ± 9.824.13 ± 0.6 < 0.00001Swelling (10 points)5.82 ± 4.59.13 ± 0.5 < 0.00001Stair-climbing (10 points)5.39 ± 1.89.13 ± 0.6 < 0.00001Squatting (5 points)2.52 ± 3.44.6 ± 0.3 < 0.00001Total (100 points)54.55 ± 19.594.23 ± 9.6 < 0 .00001Preop: Preoperative, Postop: PostoperativeTable 4Comparison of Tegner-Lyshom score between the group of LET (N. 23) and the group of ALL (N. 21) at two-year follow-upTegner-Lyshom scoreTegner-Lyshom score LET groupTegner-Lyshom score ALL groupP-valueLimp (5 points)4.36 ± 0.24.26 ± 0.40.217488Support (5 points)4.28 ± 0.74.36 ± 0.60.953224Locking (15 points)14.2 ± 0.713.91 ± 0.80.309886Instability (25 points)23.8 ± 0.823.8 ± 1.20.528064Pain (25 points)24.0 ± 0.824.13 ± 0.60.420886Swelling (10 points)8.72 ± 0.59.13 ± 0.50 .217488Stair-climbing (10 points)9.04 ± 0.59.13 ± 0.60.628064Squatting (5 points)4.36 ± 0.64.6 ± 0.30 .689878Total (100 points)93.76 ± 15.3394.23 ± 9.60 .249659
Patients experienced a satisfactory feeling of stability at final follow-up, despite the result of the pivot shift test found at physical examination (Table 5).Table 5. Pivot shift and Lachman tests of patient’s knees before the operation and at final follow upPivot shift testGroup of LETP valueGroup of ALLP valueP valuePrePostpre & postPrePostpre & postbet. LET & ALL at final follow upNegative020 < 0.0001019 < 0.00010.13657Positive GI0301Positive GII10091Positive GIII150140Lachman testNegative021 < 0.0001020 < 0.00010.21537Positive GI0201Positive GII11080Positive GIII140150The difference after two years for each group together with the difference between both groups (positive tests) at two years follow-up were recorded. (N. preop. LET 25, ALL 23 but N. at final follow up. LET 23 and ALL 21)Preop: Preoperative, Postop: Postoperative
There were five patients at final follow-up with a positive pivot shift test (three patients in the LET group (13%), grade I, and two patients in the ALL group (9.5%), grade I and II). Those five patients underwent MRI, which showed an intact ACL graft. The Lachman test was positive in three patients in both groups, grade I in two patients (8.7%) in the LET group and one patient (4.7%) in the ALL group. The differences between both groups regarding pivot shift and Lachman tests at final follow-up were nonsignificant (P-value was 0.13, 0.21, respectively).
Different parameters were measured between the two methods and recorded (Table 6).Table 6. Characters of LET and ALL groups (LET group N. 25 at surgery and 23 at two-year follow-up, ALL group N. 23 at surgery and 21 at two-year follow-up)Character, parameterACL-R with LETfrom ITBACL-R with ALLFrom PLP valueAnatomicalNon-anatomicalAnatomicalInvasiveness (Fig. 10)More invasiveLess invasiveGraft Length changes, histologyIsometric as a non-stretchable structurecontain no elastic fibers, elongatedNon-isometric containselastic fibersstretchable,no elongationGraft harvesting time, min13.48 ± 4.6 5.0 ± 3.50.00028Mean graft diameter mm4.1 ± 2.76.54 ± 2.930.03391Mean incisions length, cm8 ± 53.5 ± 3.50.00124Return to sports at 9 months (N.)Return to previous sport level at 11 ± 4 mo. (N.)211718150.3098860.421147ComplicationsInfection, (N.)Lateral knee painat 6 weeks (N.)at 6 months (N.)ACL Failure21142/25 (8%)1702/23 (8.7%)0.3053190.1586410.0230950.466202
Discussion
The most important findings in this study were the significant improvement of clinical scores after ACL surgery combined with an augmentation procedure and no residual instability. However, this improvement did not differ significantly between the LET and ALL groups after two years.
TLS for the LET group was improved significantly at follow-up. This corresponds to Goncharov et al. [29], who found TLS improved significantly in medium-term follow-up after LET.
TLS for the ALL group was improved significantly at follow-up. This corresponds to Rosenstiel et al. [30], who found Lysholm scores improved significantly at follow-up after 3.9 years [31].
In the current study, TLS between both groups was not significantly different at follow-up (P-value = 0.24). In contrast to Helito et al. [32] in their retrospective study, who found a significant improvement of Lysholm scores [31] of the ALL group than the LET group (P-value = 0.047).
There is a significant reduction in positive pivot shift and Lachman tests between preoperative and two-year follow-up for both groups (Table 5). This confirmed the efficacy of both procedures in reducing hyperlaxity suggested in biomechanical studies [9, 13, 14]. However, the differences in pivot shift and Lachman tests between both groups at two-year follow-up were nonsignificant. This result corresponds to the retrospective study by Helito et al. [32], who found that the difference in the pivot shift test and KT-1000 examination (instrumental Lachman) between both groups was nonsignificant.
Lateral-side knee pain was described more by LET than ALL patients at 6 weeks, then only by LET patients at 6 months (Table 6). This result is similar to Helito et al. [32], who found lateral side knee pain lasted for 4.3 ± 2.1 months after LET and for 2.2 ± 1.3 months after ALL. The difference was significant (P value < 0.00001).
The incidence of ACL failure in this study was 8% for the LET and 8.7% for the ALL groups, and the difference was nonsignificant (P value = 0.46) (Table 6). This corresponds to Helito et al. [32], who found a failure rate of 2.2% for the LET group and 7.3% for the ALL group, and the difference was nonsignificant (P-value = 0.34). Revisions of failure here enabled a second look after the combined procedure, and were not mentioned in the literature before. Revision, also of augmentation, was done, either from the same side in the case of LET or the contralateral side in the case of ALL.
No biomechanical superiority of either ALL or LET combined with ACL-R was found [33]. However, several comparative biomechanical studies between LET and ALL combined with ACL-R suggested that LET restricts rotatory instability more than ALL-R [14]. Also, in other biomechanical studies [9, 13, 14], the incidence of overconstraint of the knee is a permanent sequel in all literature after LET, but is controversial after ALL.
Our hypothesis was not confirmed regarding the clinical outcome; ALL was not better than LET after two years of follow-up. However, intraoperative observation and findings in follow-up can help us make a decision.
“ àla carte approach“ was suggested by Shybut [34], who recommended that when pivoting, action is needed, LET is best performed, but when lesser demands are needed, ALL is best performed. We don’t agree; our argument is the expected deterioration of the function after LET in long-term follow-up. Also, Maffulli et al. [35], in their systematic review, concluded that [35]. LET was associated with a higher reoperation rate than ALL. So, it is not recommended.“ àla carte approach “ was suggested by Shybut [34], who recommended that when pivoting, action is needed, LET is best performed, but when lesser demands are needed, ALL is best performed. We don’t agree; our argument is the expected deterioration of the function after LET in long-term follow-up. Also, Maffulli et al. [35], in their systematic review, reported greater clinical outcomes for LET. However, in the long term, we expected deterioration. In addition, they concluded that [35]. LET was associated with a higher reoperation rate than ALL. So, it is not recommended (Figs. 9, 10).Fig. 9. Graph showing LET and ALL change between preop. and postopFig. 10Intra-operative photo showing comparison of skin incisions of LET and ALL
Native anterolateral ligament (ALL) (Fig. 11).
Illustration of native ALL and its attachments
The structure was first described by Segond in 1879 and redescribed by Claes in 2013 [36]. Ahn et al. [37] reported, the constant femoral attachment of the ALL as posterior and proximal to the lateral femoral epicondyle (LFE). ALL runs obliquely along the anterolateral aspect of the knee. Its attachment distally on the anterolateral tibia was situated midway between Gerdy’s tubercle and the fibular head. The histological findings of the ALL demonstrate a separate ligamentous structure, which was clearly distinguished from the anterolateral knee joint capsule and the ITB [38].
Quantitative analysis of ALL was reported by Helito [39],, mean length of 41.5 ± 6.7 mm in 90° of flexion and 38.5 ± 6.1 mm in full extension. The mean width was 8.3 ± 2.1 mm. ALL contains elastic fibers, which allow the ligaments to stretch to some extent. Elastin content has been reported to range from 0.25% to 10% of the tissue’s dry weight; so, it is stretchable during knee motion [40].
Biomechanical studies [33, 41] have shown that the native ALL functions as a secondary stabilizer to the ACL in resisting anterior tibial translation and internal tibial rotation. However. ALL has a minor role in the presence of an intact ACL. Several cadaveric studies [42, 43] demonstrated the ALL and investigated the role of the ALL on rotatory instability in ACL deficiencies by sequential sectioning of the ACL and ALL [44]. They found that the role of ALL in rotatory instability increased in ACL-deficient knees.
Anterolateral ligament reconstruction (ALL) ( Figs. 5, 6, 7 and 8).
Several biomechanical studies demonstrated improved rotational instability and restoration of normal knee kinematics through ALL-R combined with ACL-R [11, 45].
It is advantageous to use the peroneus longus tendon here because it is sufficiently long while preserving the large-diameter status of the ACL graft. The large-diameter ACL graft decreases the incidence of failure [25, 46]. When hamstring tendons are used for ALL-R [47], this will be at the expense of ACL graft diameter.
ALL-R, using a tendon (hamstrings or peroneus longus tendons) that mainly contains collagen and elastin fibers [48]. So, its structure is suitable to reproduce the native ALL ligament.
ALL-R has separate attachment points close to the native ALL attachment sites of the femur and tibia (Fig. 9).
ALL-R is anatomically based and can be percutaneously performed with one or two small incisions on the femoral and tibial sides. ALL-R, when correctly fixed in full extension and neutral rotation, has been shown to restore normal knee kinematics and avoid overconstraint, as reported by Inderhaug et al. [41]. This makes a strong predilection for this procedure. Also, Getgood et al. [49] found with ALL-R, there was no incidence of overconstraint of the knee. Neri et al. [50] reported that ALL-R did not elevate the lateral femorotibial pressure. In contrast, an anatomic ALL-R in conjunction with ACL-R, was reported by Engebretsen et al. [51], led to a significant overconstraint of the knee. DePhillipo et al. [11] reported overconstraints of internal rotation using the posterior/proximal ALL femoral attachment point, but no overconstraints using the anterior/distal ALL femoral attachment point.
Lateral extraarticular tenodesis (LET) (Figs. 1, 2, 3 and 4).
LET is an augmentation procedure for providing added stability to the lateral aspect of the knee and reducing anterolateral knee instability [52]. It was performed with a strand of ITB fixed over the knee joint [21].
Histologically, the ITB consists mainly of collagen fibers, as confirmed by Kittl et al. [53]. There is a small amount of elastic fibers amongst the layers of collagen, which allow it to be slightly elastic, helping it act as a spring. However, this does not give it the ability to stretch like a muscle. So, in various knee motions with length changes, the graft may be stretched or elongated as it is isometric. Kernkamp [54] reported, an increase in the distance between the attachment points of 6% could lead to permanent graft elongation and eventual graft failure.
We theorize, LET subsequently may not restore the native kinematic state of the knee in the long term because LET often tends to elongate over time, with the return of anterolateral rotatory instability.
Additionally, there is concern regarding the nonanatomic nature of LET procedures, the potential for overconstraining the knee, and restricted internal tibial rotation [14], which led to a decrease in their popularity. Neri et al. [50] and Inderhaug et al. [41] reported, early arthritis in the lateral compartment after the LET. This was confirmed by MRI analysis of the lateral compartment, where Firth et al. [55] found early changes in the articular cartilage of the lateral compartment after the LET.
There are some limitations of the study, including the study population being limited to 23 LET and 21 ALL patients. Also, no power analysis was performed, which may not be enough to detect a significant difference. About surgical technique, ACL reconstruction was performed differently between the two groups (triple hamstring graft in LET versus STG in quadruple strands plus peroneus longus tendon in a single strand in ALL), which may have biased the results. Although patients covered their knees with a bandage, the individual groups were not completely concealed, and the investigator still could differentiate. The lack of blinding leads to bias, affecting the overall result. The pivot shift assessment is based on the skills of the examiner, which could bias the results of rotational instability in this study. Regional differences in the physiotherapy program between patients were possible. However, despite our appreciation of the limitations of our investigation, we believe that the results of this study could be useful in the future development of prospective long-term comparative studies.
Conclusions
The clinical outcome and stability after anterior cruciate ligament reconstruction combined with either lateral extraarticular tenodesis or anterolateral ligament reconstruction improved significantly after two years. However, no significant difference between them was found after two years. Both groups had comparable failure rates. However, the intraoperative and postoperative findings support anterolateral ligament reconstruction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shashwat Agrawal, A. S. H., B. Seetharama Rao, Prajwal P. Mane, Chethan B. Shetty, Vikrant Khanna, Samarth Thakkar, Prajwal M. Divakar, Ankita Nigam, "Peroneus Longus Tendon Autograft for Primary Arthroscopic Reconstruction of the Anterior Cruciate Ligament," Muscles, Ligaments and Tendons Journal,10.32098/mltj.02.2023.08, 2023.