Fertility intentions and influencing factors among women of reproductive age in Madhesh Province, Nepal: a population-based analysis of the 2022 Nepal demographic health survey
Bijaya Mani Devkota, Suman Chandra Gurung, Amshu Dhakal

TL;DR
This study examines why women in Nepal's Madhesh Province decide whether to have more children, finding that age, number of children, and media exposure are key factors.
Contribution
The study identifies specific demographic and socio-economic factors influencing fertility intentions in Madhesh Province, a region with persistent high fertility rates in Nepal.
Findings
Younger women (15–24 years) have significantly higher fertility intentions compared to older women.
Rural women have 33% lower odds of wanting more children than urban women.
Exposure to print media, such as newspapers, is inversely associated with fertility intentions.
Abstract
Fertility intentions or desires for future childbearing are necessary variables in understanding reproductive behavior, particularly in transitioning societies like Nepal. Despite a national decline in fertility rates, regional disparities persist, notably in Madhesh Province, where socio-economic and cultural barriers remain entrenched. This study explores the socio-economic and demographic factors influencing fertility intentions among women of reproductive-age in Madhesh Province. A cross-sectional analysis of secondary data from Nepal Demographic Health Survey (NDHS) 2022 was conducted. This study concentrated on women aged 15–49 years and residing in Madhesh, selected through a multistage stratified sampling approach. A weighted sub-sample of 1,643 women was analyzed using descriptive statistics and binary logistic regression to explore the determinants of fertility intentions.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
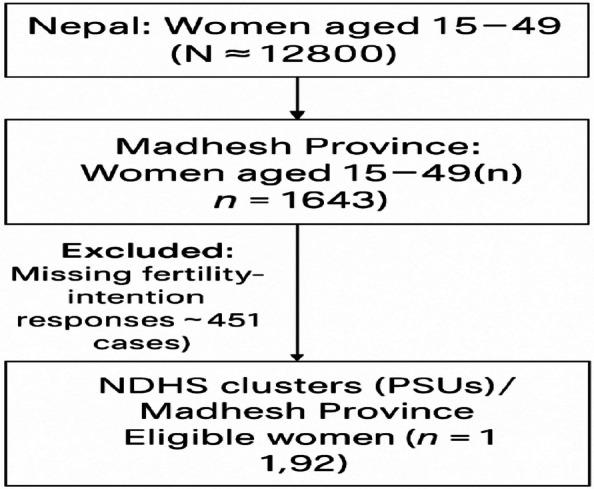 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Health and Technologies · Global Maternal and Child Health · Family Dynamics and Relationships
Background
Fertility Intention can be defined as people’s desire to have children and pursuit of childbirth which is impacted by the expectation of the number, timing, gender and quality of the children [1]. It is an individual’s stated plan or decision regarding whether to have pr not have more children in future. Although fertility intention is widely used in population and reproductive-health research, it is also repeatedly confused with other similar concepts such as fertility preference, fertility desire, and fertility expectation. Although related, these concepts measure different dimensions of reproductive choice. Various chapters of DHS Program gave several definitions. Fertility preference refers to a person's wanted number or childbearing timing, reflecting normative aspirations or cultural ideals. Fertility desire reflects an individual's personal want or emotional tendency to have children, which is typically driven by affective and psychosocial considerations. Fertility expectation, on the other hand, refers to what people expect to happen considering their socio-economic situation and limitations.
For this research, fertility intention is defined as a proximal and implementable choice how frequently a woman reports planning to have (or not have) more children under the existing conditions in her life. Understanding fertility intentions is crucial for analyzing reproductive behavior, contraceptive use and population change, particularly in societies undergoing rapid demographic transitions such as Nepal. Understanding fertility intention is crucial for analyzing population trends, family planning behaviors and reproductive health dynamics. Unlike fertility outcomes, fertility intention reflects personal and household aspirations shaped by the socio-economic, cultural, and psychological factors [2, 3]. In Nepal, a country experiencing significant socio-political change, where women navigate tensions between tradition and modernity, investigating fertility intentions is especially relevant. These insights are vital for designing programs that promote reproductive autonomy, reduce unwanted pregnancies, and improve maternal and child healthcare [4, 5]. This study addresses the need for a clear conceptualization of fertility intention, defined here as an individual’s expressed desire or plan to have children in the future.
Nepal’s total fertility rate (TFR) declined from 4.6 in 1996 to 2.1 in 2022 [6, 7]. However, provincial disparities persist. The Provincial fertility estimates and socio-economic indicators of NDHS 2022 and CBS 2021 data demonstrated that Madhesh has one of the highest total fertility rates (2.9), lowest female literacy (55%), and lowest modern contraceptive prevalence (34%) among provinces of Nepal. The fertility intentions of women in this region remain poorly understood, especially amidst recent federalization and evolving health policies. These contextual factors make Madhesh a critical region for examining fertility behavior in Nepal’s federal system.
Fertility intentions are shaped by a complex set of demographics, socio-economic and cultural factors including age, parity, education, household income, employment, access to services and exposure to media [8, 9]. Empowerment through education or decision-making autonomy typically reduces desired family size and increases contraceptive use [10]. Conversely, poverty, gender discrimination, and limited contraceptive access create structural restrictions, particularly in the regions like South Asia and sub-Saharan Africa, hindering women’s ability to align intentions with outcomes [11, 12]. In Nepal, however, women’s fertility intentions are often constrained by the expectations of husbands and in-laws, leaving little room for personal negotiation. [13, 14].
While national-level studies in Nepal reported education, wealth and age as major predictors, Women here face layered disadvantages regarding reproductive choice [15]. For instance, Terai Dalit and Muslim women in Madhesh experience severely limited access to antenatal care and skilled birth attendance, yet their fertility aspirations remain under-researched [16]. Although national studies identify education, age, and wealth as key determinants, these findings may not fully capture the Madhesh Province’s unique socio-cultural environment, where deep-rooted patriarchy persists [17]. Understanding the interplay between these factors and fertility intentions is critical for addressing regional disparities in family planning and reproductive health.
Previous evidence from culturally similar regions of India and rural Ethiopia suggests that fertility intentions are strongly mediated by local norms, dowry practices and gender dynamics [18, 19]. Such findings highlight the need for localized research to plan and design interventions suited to provincial realities rather than relying solely on national average data.
Guided by the demographic and health transition framework, this study examines the determinants of fertility intentions among women of reproductive age in Madhesh province using the most recent NDHS 2022 data. By incorporating key variables such as parity, age, residence, education, caste and media exposure, it offers new insights into factors shaping women’s reproductive plans in a province where fertility decline has been slower than elsewhere in Nepal. Findings are expected to inform provincial level reproductive health strategies and contribute to the broader evidence base on fertility behavior in transitioning societies.
The demographic and health transition framework provides a useful lens to understand fertility intention shifts in Nepal. While rising literacy, health infrastructure, and urbanization generally predict declining fertility preference, this decline often conflicts with persistent social norms and economic structures. In Madhesh, for instance, fertility intentions remain high alongside an unmet need for contraception [20, 21]. Bridging this gap requires timely, geographically disaggregated empirical evidence.
This study utilizes the data from the Nepal Demographic Health Survey (NDHS) 2022 to examine fertility intentions and their socio-economic and demographic determinants among women aged 15–49 in Madhesh Province. Using logistic regression within a population-based framework, it identifies key predictors of fertility intentions such as education, household wealth, occupation, age, parity, caste/ethnicity, and media exposure. Provincial-level analysis is particularly important in Nepal’s post-federalization context, where provincial governments are now responsible for health planning and service delivery [22] Despite increasing national attention to fertility trends, existing studies often rely in aggregated national data and overlook subnational diversity of the country. Empirical research specifically focused on Madhesh province, a region marked by pronounced socio-economic inequalities, embedded gender norms and cultural heterogeneity remains limited [23].
This study addresses that gap by providing a disaggregated, evidence-based understanding of fertility intentions in Madhesh province. The findings have both academic and policy significance offering insights to inform culturally sensitive reproductive health programs, guide resource allocation and support the empowerment of marginalized women [24]. Ultimately, this research contributes to linking reproductive intentions with outcomes in one of the Nepal’s most socio-economically vulnerable regions.
Methods
This study employed a quantitative, cross-sectional design using secondary data from the 2022 NDHS Survey to assess factors influencing fertility among reproductive-age women in Madhesh Province.
Study design
The analysis used a nationally representative dataset from NDHS [25], collected via a multi-stage stratified cluster sampling method. The NDHS gathered demographic, health, and reproductive information from women aged 15–49 years across all the provinces of Nepal. This study particularly analyzed data for women residing in Madhesh Province. The cross-sectional approach allowed for the examination of the relationship between socio-demographic factors and fertility intentions at a single point in time.
Sample and sampling procedure
The NDHS used a two-stage stratified sampling design. The initial selection involved rural and urban strata, followed by the systematic selection of enumeration areas (EAs) and then households within those EAs. For this study, a weighted sample of reproductive-age women (15–49 years) living in Madhesh Province was extracted. Women who provided responses to key fertility preference questions regarding desire for more children, timing, and family size were included in the analysis. The final sample size was determined based on completeness of responses and the availability of relevant variables for analysis.
Model of diagnostics sample frame
Figure 1 presents the Diagnostic Sample Frame Model showing the hierarchical sampling plan and derivation of the analytical sample of the total population of reproductive age. The sampling was based on NDHS clusters (PSUs) and then household of the eligible women respondents (1192 from 12,800 national data) were selected with the use of PPS techniques and design weights.Fig. 1. Model of Diagnostics sample frame. Source for Fig. 1: Computed from NDHS 2022
Data analysis methods
Descriptive statistics characterized the respondents background characteristics. Logistic regression analyses identified the socio-demographic and reproductive health factors associated with fertility intentions. Both unadjusted and adjusted odds ratios (ORs) with a 95% confidence interval (CIs) were calculated. Statistical significance was set as p < 0.05.
An applied NDHS sampling weights, PSU, and strata. The survey-weighted logistic regression yielded a highly significant model (Wald χ^2^ = 182.4, p < 0.001) with a pseudo-R^2^ of 0.29. Variance Inflation Factors (VIF)indicated low inter-predictor correlation (max VIF = 2.1). The sparse-cell issues were resolved through category merges, and sensitivity checks using a simplified model confirmed the robustness of the main results (Table 1).Table 1. Model-diagnostic weighted logistic regressionDiagnostic itemDescription/ValueSurvey designsvyset psu = v021; strata = v022; pweight = v005/1 000 000Estimator usedSurvey-weighted logistic regression (svy: logit)Sample size (unweighted)1 643 (observed); 1192 (Adjusted model)Wald χ^2^ (df = 12)182.4 (p < 0.001) — Model significantPseudo R^2^0.29Multicollinearity (VIF)Mean = 1.6; Max = 2.1 → no multi-collinearityZero/near-zero cellsResolved by merging sparse age (40–49) and minor religion groupsSurvey weights appliedNDHS design accounted for clustering and stratificationRobustness checkSimplified model (excluding media variables) → same direction and significanceInterpretationFindings stable; model fit adequate; no multi-collinearity or design bias detected
The main result measure was fertility intention, derived from NDHS questions v602 and v605, which ask a woman how many more children she wants. It was coded dichotomously as: code 1 = desires more children, and 0 = does not desire more children, including undecided, sterilized, or infecund respondents. This definition meets DHS analytical requirements and allows for comparability with other fertility intention studies [6, 26]. Explanatory variables of major relevance were chosen on the basis of theoretical and empirical evidence supporting their association with fertility behavior (Table 2).Table 2. Description of variablesVariableNDHS CodeRecodingReferenceDependent Variablev602/v6051 = Wants more children; 0 = Does not want/undecided/sterilized—Age (years)v01215–19, 20–24, 25–29, 30–34, 35–39, 40–4915–19Residencev025Urban/RuralUrbanParity (number of living children)v2180, 1–2, 3–4, 5 + (children alive)0Education (women)v106No education/Primary/Secondary/HigherHigherNewspaper exposurev157Not at all/< 1 per week/≥ 1 per week ≥ 1 per weekWealth quintilev190Poorest → Richest (5-level DHS index)RichestReligionv130Hindu/Muslim/Other (merged Buddhist, Kirat, Christian)HinduCaste/Ethnicityv131Other Terai/Terai Dalit/OtherHill Brahmin
Ethical consideration
This study used publicly available secondary data from the 2022 NDHS, which was conducted by the Ministry of Health and Population (MoHP) in collaboration with ICF, following all ethical guidelines. The data protocol ensures participant confidentiality and safety. No personal identifiable information was used in this analysis, and data access was granted by the DHS Program [7].
Results
Analysis of the 2022 NDHS data revealed multiple factors associated with fertility intentions among women in Madhesh Province, Nepal, including wealth, education, age, residence, occupation, caste/ethnicity, religion, and media exposure. These have been presented in Table 1. Socio-economically, women in the middle and poorer wealth quintiles reported higher fertility intentions (15.6% each) compared to those in the richest quintile (6.0%). Education was a significant determinant: women with primary education (20.2%) and secondary education (18.8%) expressed higher fertility intentions compared to those with no formal education. (14.5%) or tertiary education (1.3%). A similar trend was observed for partner’s education: partners with secondary education were associated with higher fertility intentions (15.5%) than those with no formal education (7.8%).
Table 3 also presents that demographically, fertility intentions were highest among younger women, especially those aged 15–19 (26.5%) and 20–24 age group. Fertility intentions declined significantly with increasing age, nearly disappearing among women aged 40-44and 45–49 years. Parity had a significant negative relationship with fertility intention. Only one-third of the women had no children (33.8%), and this group had the highest ambition of having more children (33.2%). Women having 3–4 children (23.0%), and those having 5 or above children (3.9%), on the other hand, had little intention to have further children (2.6% and 0.2%, respectively). The negative correlation of the parity levels shows that more parity is closely linked with the completed fertility. (Table 1). Urban women expressed slightly higher fertility preferences (41.7%) than rural women (13.1%). Women’s employment status also influenced fertility intentions, with non-working women (29.2%) and those employed in agriculture (18.1%) expressing a stronger desire for more children. Caste/ethnicity and religion were also significant. Women from other Terai castes (26.1%) and Terai Dalits (11.1%) reported higher fertility intentions, as did Muslim women (9.7%). Media exposure was also associated with fertility intentions; women who regularly accessed newspapers, radio, and television expressed stronger fertility desires than those with no media exposure. Women who watched television at least once a week showed a relatively higher fertility intentions (19.3%) than those who had never watched television (23.9%). These findings demonstrate the complex interplay of economic status, access to information, and social-cultural identity in shaping reproductive aspirations within Madhesh Province.Table 3. Fertility preferences across women’s socio-economic status and their demographic characteristicsVariablesNumber(N)Percent (%)Fertility preferences**No (%)****Yes (%)**Socio-economic variablesWealth quintile Poorest1258.83.85.0 Poorer42225.710.215.6 Middle53129.714.115.6 Richer39823.711.012.7 Richest16712.16.16.0Level of education No education56835.821.314.5 Primary54832.312.120.2 Secondary49129.710.918.8 Higher362.20.91.3Partner’s level of education No education24320.712.97.8 Basic42532.918.714.2 Secondary42434.719.215.5 Higher846.63.92.7 Highest615.22.62.6Demographic variables Age 15–1946227.30.826.5 20–2443627.38.518.8 25–2927617.111.25.9 30–3418911.69.12.5 35–391368.27.50.8 40–44965.75.40.3 45–49482.72.7Parity No children55733.80.633.2 1–2 children65339.420.718.7 3–4 children37123.020.32.6 5 + children623.93.70.2Residence Urban94774.432.741.7 Rural69625.612.513.1Occupation Not working last 12 months71645.816.629.2 Professional/technical523.21.22.0 Clerical90.80.10.6 Sales and service684.32.61.7 Skilled manual704.82.22.6 Unskilled manual301.71.10.5 Agriculture69839.521.418.1 OtherCaste/Ethnicity Hill Brahmin201.81.20.6 Hill chhetri121.00.60.4 Terai brahmin/chhetri463.11.41.7 Other terai caste76747.721.626.1 Hill dalit90.60.30.3 Terai dalit33318.17.011.1 Newar220.80.40.4 Hill janajati452.91.81.1 Terai janajati1316.53.33.3 Muslim25617.47.79.7 Other20.10.1Religion Hindu1,35581.036.744.3 Buddhist281.20.70.5 Muslim25517.37.69.7 Kirat30.40.10.2 Christian20.10.10.1Frequency of reading newspaper or magazine Not at all1,47689.341.048.3 Less than once a week1147.43.34.1 At least once a week533.30.92.4Frequency of listening to radio Not at all1,08166.530.236.3 Less than once a week37522.310.112.2 At least once a week18711.24.96.3Frequency of watching television Not at all71444.620.723.9 Less than once a week34420.58.911.6 At least once a week58534.915.619.3Source: Computed from NDHS 2022
Table 4 presents the results of both unadjusted (Model 1) and adjusted (Model 2) logistic regression analyses identifying factors associated with fertility intentions among women of reproductive age in Nepal. The unadjusted analysis revealed significant associations with several socio-economic variables. For example, belonging to the "poorer" wealth quintile increased the odds of fertility intentions (cOR = 1.56, 95% CI: 1.15–2.13) compared to the richest quintile. However, this association lost significance after adjustment (aOR = 1.16, 95% CI: 0.67–2.02). Likewise, women with no education (cOR = 0.47, 95% CI: 0.25–0.86) and partners with no education (cOR = 0.60, 95% CI: 0.36–0.99) showed significantly lower fertility intentions in the unadjusted model, but these effects became non-significant after accounting for confounding factors.Table 4. Socioeconomic and demographic factors associated with fertility preferences among women of reproductive age in NepalVariablesModel 1 cOR 95% CIModel 2 aOR 95% CISocio-economic variablesWealth quintile Poorest1.34 (0.91–1.98)1.29 (0.66–2.54) Poorer1.56 (1.15–2.13)***1.16 (0.67–2.02) Middle1.12 (0.83–1.51)1.05 (0.63–1.74) Richer1.17 (0.86–1.59)1.11 (0.69–1.80) RichestRefRefLevel of education No education0.47 (0.25–0.86)**1.11 (0.35–3.51) Primary1.15 (0.62–2.13)0.93 (0.30–2.88) Secondary1.19 (0.64–2.21)0.88 (0.30–2.62) HigherRefRefPartner’s level of education No education0.60 (0.36–0.99)**0.77 (0.41–1.45) Basic0.76 (0.47–1.22)0.95 (0.52–1.75) Secondary0.81 (0.50–1.30)1.21 (0.65–2.25) Higher0.68 (0.38–1.24)1.33 (0.58–3.04) HighestRefRefDemographic variables Age 15–19RefRef 20–240.07 (0.04–0.12)0.14 (0.08–0.25) 25–290.02 (0.01–0.03)0.03 (0.02–0.06) 30–340.01 (0.01–0.02)0.02 (0.01–0.03) 35–390.00 (0.00–0.01)0.01 (0.00–0.02) 40–440.00 (0.00–0.01)0.00 (0.00–0.01) 45–490 (0–0.001) ***—Parity No childrenRefRef 1–2 children23.898(8.389–68.078) ***18.205(5.579–59.404) *** 3–4 children3.589(1.269–10.151) **2.808(0.902–8.739) * 5 + children0.544 (0.162–1.821)0.575(0.162–2.041)Residence UrbanRefRef Rural0.82 (0.67–1.00)0.67 (0.49–0.92)Occupation Not working2.77 (1.76–4.36)1.27 (0.59–2.72) Professional/technical2.78 (1.43–5.42)**2.48 (0.83–7.45) Skilled manual1.87 (1.04–3.38)0.80 (0.31–2.05) Unskilled manual0.78 (0.33–1.80)1.07 (0.27–4.28) Agriculture1.33 (0.84–2.09)1.21 (0.56–2.58) Sales/service (Ref)RefRefCaste/Ethnicity Hill Brahmin (Ref)RefRef Hill Chhetri1.13 (0.36–3.56)3.05 (0.58–15.92) Terai Brahmin/Chhetri2.29 (0.97–5.39)2.17 (0.57–8.26) Other Terai Caste2.36 (1.16–4.79)**1.37 (0.46–4.09) Hill Dalit1.64 (0.45–6.01)2.98 (0.46–19.22) Terai Dalit3.09 (1.49–6.39)1.55 (0.49–4.93) Newar2.29 (0.68–7.69)4.54 (0.87–23.70) Hill Janajati1.24 (0.52–2.97)0.39 (0.07–2.07) Terai Janajati1.97 (0.91–4.28)1.77 (0.54–5.82) Muslim2.43 (1.17–5.03)0.00 (0.00–NA)Religion HinduRefRef Buddhist0.56 (0.25–1.26)6.21 (1.00–38.39) Muslim1.05 (0.83–1.32)547,308 (0.00–NA) Kirat1.25 (0.28–5.59)8.67 (0.51–148.28) Christian1.20 (0.11–13.33)-Frequency of reading newspaper or magazine Not at all0.47 (0.27–0.81)0.49 (0.21–1.16) Less than once a week0.49 (0.27–0.92)0.38 (0.15–0.99) At least once a weekRefRefFrequency of listening to radio Not at all0.94 (0.70–1.25)1.34 (0.83–2.16) Less than once a week0.95 (0.68–1.31)1.42 (0.84–2.41) At least once a weekRefRefFrequency of watching television Not at all0.93 (0.76–1.14)1.20 (0.86–1.69) Less than once a week1.05 (0.82–1.34)1.17 (0.79–1.71) At least once a weekRefRefN16431192PseudoR^2^0–0.3780.285Exponential coefficients presented; 95% confidence intervals in bracketscOR Crude Odds Ratio, aOR Adjusted Odds RatioSignificance levels:^^p < 0.05^^p < 0.01^^p < 0.001
Age came out as a major determinant in both the models. Fertility intentions decreased progressively with age relative to 15–19-year reference group, reaching near-zero probability (aOR ≈ 0.00) among women aged 40–44 years. Rural residence was associated with lower odds of fertility intentions compared to women living in urban areas (aOR = 0.67, 95% CI: 0.49–0.92).
The parity was significantly and gradual associated with fertility intention. The women with 1–2 children were significantly more likely to have further birth intentions as compared to those with none (aOR = 18.21, 95 percent CI = 5.58 59.40, p = 0.001). The magnitude of the association decreased with the increased parity-women with 3–4 children had a modest relationship (aOR = 2.81, 95% CI = 0.90874), women with more than 5 children had no significant association (aOR = 0.58, 95% CI = 0.16204). This trend indicates that fertility intention is decreasing as the number of children is increasing (Table 2). Occupational status was significant in the unadjusted model; for example, women in professional/technical occupations had substantially higher odds (cOR = 2.78). However, these associations attenuated after adjustment. Findings for ethnicity and religion were mixed; Terai Dalit (cOR = 3.09), Muslim (cOR = 2.43), and Newar women (aOR = 4.54) showed higher fertility preferences initially, but these associations became statistically insignificant after adjustment, implying that their effects are mediated by other factors. Media exposure showed a protective effect; women who read newspapers less than once a week had lesser odds of fertility intentions (aOR = 0.38, 95% CI: 0.15–0.99) compared to weekly readers. In summary, key predictors of fertility intentions identified in this study include younger age, rural residence and media exposure. Wealth status, education, and religious affiliation did not retain significant independent associations after adjustment for confounders.
Discussion
This study examined the socio-economic and demographic determinants of fertility intentions among women of reproductive age in Madhesh Province using the data derived from the 2022 Nepal Demographic and Health Survey [6]. After adjusting for major covariates (age, parity, education and residence); age, parity and media exposure remained the most significant predictors of fertility intentions. In contrast, the effects of wealth, education, caste and religion became statistically insignificant after adjustment. These results highlight the complex and context-specific nature of reproductive decision making in Madhesh province, consistent with theoretical expectations of fertility behavior [8, 27].
Age emerged as the strongest determinants. Younger women particularly those aged 15–24 years and with fewer children, were substantially more likely to express desire for additional children. This pattern aligns with evidence from South Asia and sub-Saharan Africa, where younger women’s fertility intentions reflect incomplete family formation and sociocultural norms that favor larger families early in reproductive life [8, 26]. Fertility intentions declined sharply with increasing age likely due to both biological constraints and societal expectations that discourage childbearing at older ages [28].
Place of residence also showed an interesting pattern. Contrary to earlier propositions that rural women have higher fertility desires [27], the adjusted results indicated that rural women in Madhesh were less likely to want more children than urban women. This reversal may reflect recent urbanization trends, improved access to education and family planning information in rural areas, and migration of higher fertility households to urban centers. It also may suggest that urban women, influenced by social expectations of larger families or differing life-stage structures are more likely to plan additional births. These findings should, however be interpreted cautiously, as unmeasured factors such as migration or employment could also explain the variation [6, 29]. Education, wealth status and occupation were significantly associated with fertility intentions in the unadjusted analysis, but these relationships became non-significant once confounding factors were controlled for. This suggests that their effects may be mediated by variables such as age, and access to information rather than acting independently. Evidence from the other South Asian regions similarly indicated that reproductive autonomy and exposure to information often have stronger predictive power than formal education in shaping fertility behavior [30, 31]. The disappearance of occupational effects after adjustment implies that employment alone does not determine fertility preferences without considering the wider socio-cultural context [32].
Caste, ethnicity and religion produced mixed results. While Terai Dalits, Muslims, and Newars initially appeared more likely to intend further childbearing, these differences lost statistical significance after adjustment. Contrarily, Buddhist women showed higher odds in the adjusted model though the sample size warrants cautious interpretation. This pattern suggests that caste and religion influence fertility more indirectly through disparities in education, access to health services and gender norms rather than as standalone cultural determinants [33, 34].
Media exposure, especially newspaper reading, was inversely associated with fertility intentions. Women who reported reading newspapers less than weekly had lower odds of intending more children than regular readers (aOR = 0.38, 95% CI: 0.15–0.99), suggesting that exposure to reproductive health information through print media may promote smaller family. The weaker associations found for radio and television may reflect content gaps, accessibility differences or varying audience engagement. Comparable findings from other low and middle-income countries show that print media often conveys more targeted reproductive health messages than radio or television [35–37].
These results indicate that fertility intentions in Madhesh are driven more by lifestage and informational factors than by structural variables such as education or wealth status. The findings emphasize the importance of designing media-based, youth-focused and rural-sensitive reproductive health programs and of addressing underlying gender norms that continue to shape fertility decisions among the marginalized groups [38].
A key strength of this study is the use of most recent, nationally representative NDHS 2022 dataset, enhancing the reliability and generalizability of the findings for Madhesh Province. The large sample size and use of both unadjusted and adjusted regression models strengthen the analytical rigor and help minimize bias. However, some limitations should be acknowledged. The cross-sectional design prevents drawing causal conclusions, and self-reported fertility intentions may be influenced by recall or social desirability bias, especially among older and women with low education. In addition, small subgroup sizes for certain religious minorities limited the statistical precision, resulting in wider confidence intervals [39].
Conclusion
This study provides a population-based understanding of fertility intentions among women of reproductive age in Madhesh Province, Nepal, using data from the 2022 Nepal Demographic Health Survey (NDHS). The findings reported age, residence and media exposure as the most significant determinants of fertility intentions. Although wealth, education, and caste/ethnicity initially appeared influential, their effects diminished after adjusting for confounding factors.
Younger women, those with one to two children, urban residents, and women with access to print media were more likely to express fertility intentions, suggesting that reproductive decision-making in Madhesh is shaped by both life-stage and informational factors rather than by structural or economic status alone.
To align fertility intentions with positive reproductive health outcomes, targeted awareness initiatives particularly through accessible and culturally relevant print media should be strengthened. Policies should focus to reduce the urban–rural disparities in family planning access and address persistent social and gender norms influencing fertility behavior. Provincial health authorities are encouraged to develop youth-centered, equity-focused reproductive health strategies that empower women, improve access to contraception and foster informed reproductive choices across diverse communities in Madhesh Province.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hussain R et al., Unmet Need for Contraception in Developing Countries: Examining Women’s Reasons for Not Using a Method, New York: Guttmacher Institute; 2016. https://www.guttmacher.org/report/unmet-need-for-contraception-in-developing-countries
- 2Ministry of Health and Population (Mo HP) & ICF. Nepal Demographic and Health Survey 2022. Kathmandu, Nepal: Mo HP, ICF. 2022. https://dhsprogram.com/publications/publication-fr 368-dhs-final-reports.cfm.
- 3Ministry of Health and Population (Mo HP). Nepal Demographic and Health Survey 2022. Kathmandu, Nepal: Mo HP, ICF. 2022 https://dhsprogram.com/pubs/pdf/FR 368/FR 368.pdf.
- 4Wasti SP, van Teijlingen E, Rushton S. et al. Overcoming the challenges facing Nepal’s health system during federalisation: an analysis of health system building blocks. Health Res Policy Sys 21, 117 (2023). 10.1186/s 12961-023-01033-2.10.1186/s 12961-023-01033-2PMC 1062117437919769 · doi ↗ · pubmed ↗
- 5DHS Program. Available datasets. The DHS Program. 2022. https://dhsprogram.com/data/available-datasets.cfm.
- 6Westoff CF. Fertility preferences and unmet need for family planning. DHS Analytical Studies No. 5. ORC Macro. 2012. https://dhsprogram.com/pubs/pdf/as 5/as 5.pdf.
- 7UNFPA. State of adolescents and youth in Madhesh Province, Nepal. United Nations Population Fund Nepal. 2021. https://nepal.unfpa.org.
- 8Pandey JP, Dhakal MR, Karki S, Poudel P, Pradham MS. Maternal and child health in Nepal: The effects of caste, ethnicity, and regional identity [Internet]. Calverton, Maryland, USA: ICF International; 2013. (DHS Further Analysis Reports No. 73). http://dhsprogram.com/pubs/pdf/FA 73/FA 73.pdf