Primary Thyroid Tuberculosis Masquerading as a Follicular Neoplasm With Tracheal Compression: A Case Report
João Varanda, Daniel Martins, Hugo Pais Moreira, Antónia Póvoa, Bela Pereira

TL;DR
A rare case of thyroid tuberculosis was mistaken for a thyroid tumor, but molecular testing confirmed tuberculosis and avoided unnecessary surgery.
Contribution
Highlights the importance of considering tuberculosis in thyroid nodules with granulomas and the utility of molecular testing for accurate diagnosis.
Findings
Thyroid tuberculosis can mimic follicular neoplasms with imaging and cytology.
Molecular testing confirmed Mycobacterium tuberculosis in a thyroid lesion with granulomas.
Anti-tuberculosis therapy resolved the condition without further surgery.
Abstract
Thyroid tuberculosis (TB) is a rare form of extrapulmonary infection that can mimic thyroid neoplasms. Diagnosis is challenging due to nonspecific imaging and cytology. We report a case of a 77-year-old female with a history of subtotal gastrectomy for gastric adenocarcinoma. Surveillance CT revealed right-lobe-predominant thyroid enlargement causing tracheal compression. Ultrasound showed a multinodular goitre with a 4.1-cm solid nodule (Thyroid Imaging Reporting and Data System (TI-RADS) 3) and a 1.7-cm hypoechoic nodule (TI-RADS 4). Fine-needle aspiration cytology (FNAC) of the smaller nodule suggested a follicular neoplasm. The right thyroid lobectomy was performed. Histology revealed a follicular adenoma with epithelioid granulomas, and polymerase chain reaction (PCR) confirmed Mycobacterium tuberculosis (M. tuberculosis) complex DNA. The patient completed standard…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
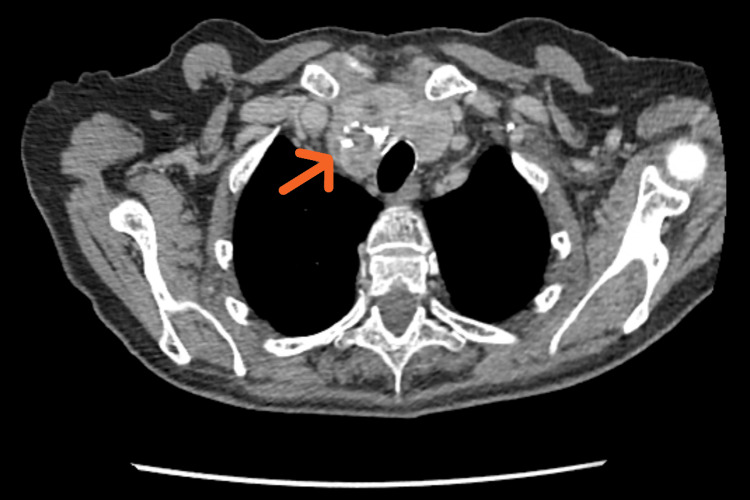 Figure 1
Figure 1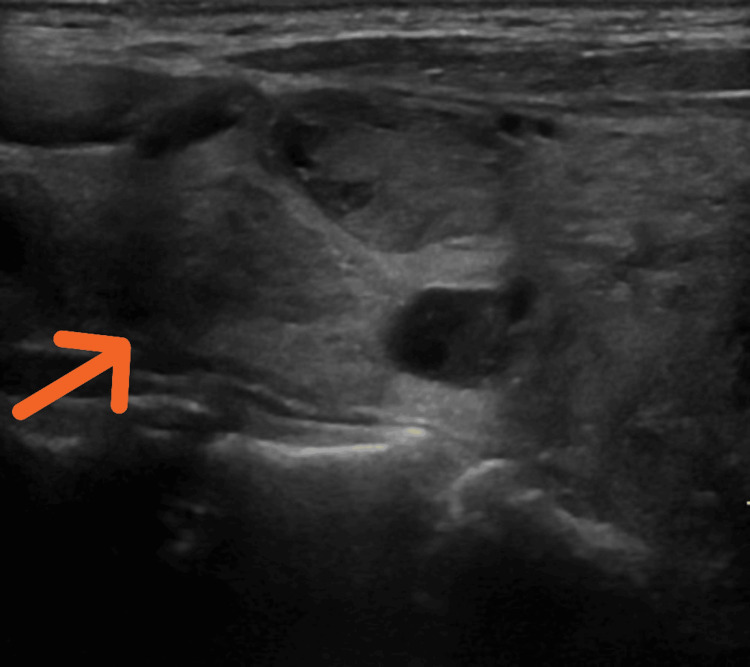 Figure 2
Figure 2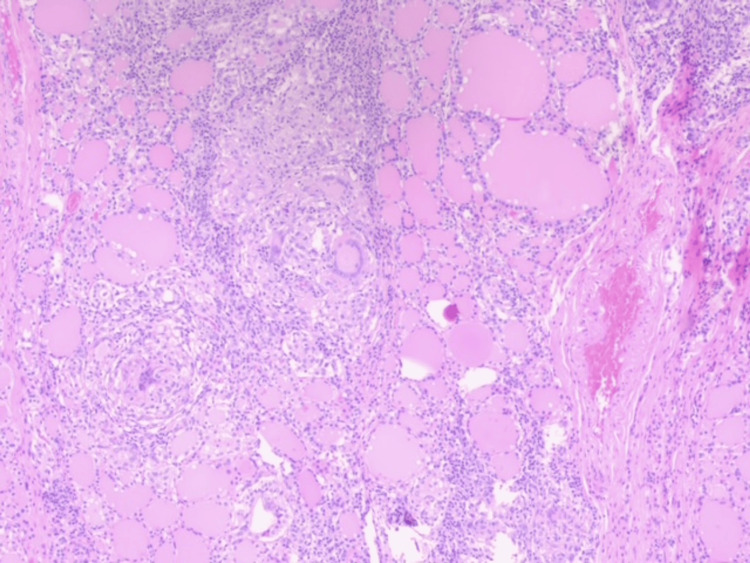 Figure 3
Figure 3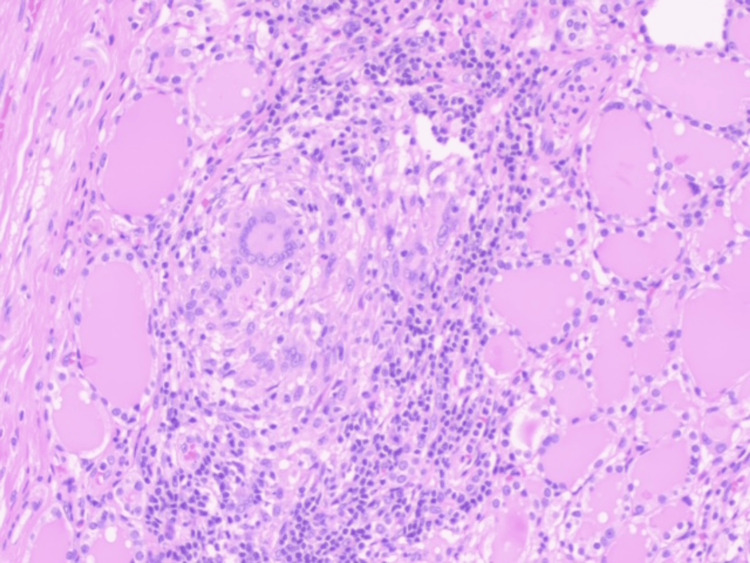 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Anomalies · Thyroid and Parathyroid Surgery · Myasthenia Gravis and Thymoma
Introduction
Extrapulmonary tuberculosis (EPTB) accounts for 15-20% of all tuberculosis cases worldwide, frequently affecting lymph nodes, pleura, bones, and genitourinary organs [1]. Thyroid involvement is extremely rare (<1%) even in tuberculosis-endemic regions [2-4], likely due to the gland’s high vascularity, iodine-rich colloid, and encapsulation, which provide resistance to mycobacterial infection [5-8].
Clinical presentations are variable, ranging from solitary nodules and multinodular goiters to diffuse enlargement or abscesses, sometimes causing compressive symptoms such as dysphagia, dyspnea, or stridor [9-13]. These features overlap with thyroid malignancy or benign nodular disease, making early diagnosis challenging. Due to similarities with malignancy, patients may undergo unnecessary surgery for an infection treatable with medication. Imaging with ultrasound or a CT scan is essential but nonspecific. Nodules may appear solid, cystic, or mixed, occasionally with calcifications [14,15]. Fine-needle aspiration cytology (FNAC) may be inconclusive due to sparse granulomas or the absence of acid-fast bacilli [16-19].
Case presentation
A 77-year-old female with prior subtotal gastrectomy for gastric adenocarcinoma, hypertension, and dyslipidemia (on valsartan and simvastatin) underwent routine surveillance. CT imaging revealed right-lobe-predominant thyroid enlargement causing tracheal compression and minor deviation (Figure 1). Thyroid function was normal.
Axial CT scan of the neckCT: computed tomography
Neck ultrasound revealed a multinodular goiter: right lobe: 4.1-cm mixed, predominantly solid nodule with macrocalcifications (Thyroid Imaging Reporting and Data System (TI-RADS) 3) - right lobe: 1.7-cm predominantly solid, mildly hypoechoic nodule (TI-RADS 4) (Figure 2) - multiple smaller nodules in the left lobe. No cervical lymphadenopathy was observed. While the larger nodule caused compression, the smaller one was biopsied due to higher suspicion features.
Nodules of the right thyroid lobe
FNAC of the 1.7-cm nodule suggested a follicular neoplasm (Bethesda IV). A right thyroid lobectomy was performed due to compressive symptoms and indeterminate cytology. Postoperative recovery was uneventful, apart from a minor seroma clinically detected and managed conservatively.
Histopathology revealed a follicular adenoma with epithelioid granulomas (Figures 3, 4). Ziehl-Neelsen staining was negative. Polymerase chain reaction (PCR) testing of FFPE (formalin-fixed, paraffin-embedded tissue) confirmed Mycobacterium tuberculosis (M. tuberculosis) complex DNA. The patient completed standard anti-tuberculosis therapy and remained asymptomatic with no recurrence at the eight-month follow-up.
Thyroid tissue with well-defined epithelioid granulomas
Epithelioid granuloma with giant multinucleic cells and inflamatory lymphocytic infiltration
Discussion
Thyroid TB is rare, accounting for <1% of thyroid surgical specimens [2-4,7]. Presentations are diverse, including nodules, multinodular goitre, abscess, or diffuse enlargement [14-16]. Compressive symptoms are uncommon but clinically significant, as in this case, in which a right-lobe-dominant nodule caused tracheal deviation. Ultrasound is essential for assessing nodule characteristics and mass effect, but cannot distinguish TB from malignancy [17,18]. FNAC may be limited by sparse granulomas and often negative acid-fast staining [19]. PCR enables definitive diagnosis from FNAC or surgical specimens, even in paucibacillary tissue. Previous reports support the utility of PCR in confirming TB when cytology is indeterminate [4,5].
Medical therapy with standard anti-TB regimens remains the first-line treatment [1,3,6]. Surgical intervention is reserved for cases of diagnostic uncertainty, compressive symptoms, or abscess drainage [7,15]. In this case, TB was not suspected preoperatively, and lobectomy was performed due to cytological suspicion and possible airway compromise. Histopathological examination combined with PCR confirmed TB, thereby preventing unnecessary extensive surgery.
Cases of thyroid TB causing compressive symptoms are rare. Fewer than 300 cases of thyroid TB have been reported in the global medical literature to date [20], making this condition extremely rare even in TB-endemic regions. Several reviews have emphasized this rarity: a 2006 review reported approximately 200 cases worldwide up to that time; a 2017 systematic review identified only seven cases reported in Western European countries since 2010; and a 2006 literature review found 76 cases that met its selection criteria. Teferi et al. reported a giant thyroid abscess causing airway obstruction [9], while Pachipala et al. described nodules larger than 3 cm managed surgically in combination with anti-TB therapy [4]. Many reports highlight the challenge of distinguishing TB from carcinoma, particularly with hypoechoic, solid, or calcified nodules.
The clinical lessons from this case are as follows: a high index of suspicion for TB should be maintained in patients with nodular thyroid disease accompanied by granulomatous inflammation or compressive symptoms, even among elderly or post-oncologic populations. PCR should be used to obtain a rapid and definitive diagnosis when cytology and conventional histology are inconclusive. Surgical intervention should be individualized for cases with diagnostic uncertainty or significant mass effect, while acknowledging that medical therapy remains the cornerstone of treatment.
Conclusions
This report describes thyroid TB presenting as a follicular lesion with tracheal compression, highlighting diagnostic challenges, molecular confirmation, and clinical management. Although rare, thyroid TB is an important differential diagnosis in nodular thyroid disease, as it can mimic follicular neoplasms and cause compressive symptoms, leading to potential misdiagnosis when relying on cytology and imaging alone. PCR testing on FNAC or surgical specimens enables definitive diagnosis and timely anti-TB therapy, though its role in preventing unnecessary surgery should be interpreted cautiously in this case, as PCR was performed postoperatively. Clinicians, particularly in TB-endemic regions, should maintain a high index of suspicion for this entity to facilitate prompt recognition and multidisciplinary management. Reporting such rare cases contributes to improved understanding of clinical presentations, diagnostic approaches, and management strategies, while broader recommendations regarding routine molecular testing or future research should be framed cautiously.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnostic and management guidelines of thyroid tuberculosis: our experience and systematic review Indian J Otolaryngol Head Neck Surg Chaudhary P Bhadana U Anand A Kapur N 130213107520233727509410.1007/s 12070-022-03275-y PMC 10235232 · doi ↗ · pubmed ↗
- 2Thyroid tuberculosis: a case series and a review of the literature J Thyroid Res Majid U Islam N 359864201120112160316410.4061/2011/359864 PMC 3095885 · doi ↗ · pubmed ↗
- 3Thyroid tuberculosis Indian J Tuberc Bansal LK Gupta S Gupta AK Chaudhary P 2722786820213384596410.1016/j.ijtb.2020.09.006 · doi ↗ · pubmed ↗
- 4Two interesting cases of thyroid gland tuberculosis Cureus Pachipala MS Aiyappan SK 016202410.7759/cureus.68733 PMC 1145328639371708 · doi ↗ · pubmed ↗
- 5A case of miliary tuberculosis complicated by thyroid involvement: managing rifampicin-induced thrombocytopenia with rifabutin Cureus Nagashima A Kobori T Hattori M Imura S Okochi Y 016202410.7759/cureus.57876 PMC 1108141038725736 · doi ↗ · pubmed ↗
- 6Incidental finding of thyroid tuberculosis by operation for Graves’ disease: a rare case presentation Case Rep Endocrinol El Azime Z Handa S Bourkadi G Aynaou H Salhi H El Ouahabi H 3865608202420243848161210.1155/2024/3865608 PMC 10937076 · doi ↗ · pubmed ↗
- 7Primary thyroid tuberculosis mimicking papillary carcinoma of thyroid: a rare case report Ann Med Surg (Lond) Banmala S K CS Raut M Poudel R Karki S Maharjan S 215521588520233722891110.1097/MS 9.0000000000000648 PMC 10205275 · doi ↗ · pubmed ↗
- 8Primary tuberculosis of the thyroid gland Hormones (Athens) Zendah I Daghfous H Ben Mrad S Tritar F 330333720081912199510.14310/horm.2002.1215 · doi ↗ · pubmed ↗