Neurocognitive risk markers in first-episode major depressive disorder with positive family history: a large-scale case–control study
Zhiyong Li, Min Pan, Xulai Zhang, Anzhen Wang, Wenmei Fang, Jianjun Guan, Boyu Zhang, Xialong Cheng

TL;DR
This study identifies language and cognitive impairments as potential risk markers for first-time depression in individuals with a family history of the condition.
Contribution
The study reveals that language function and total cognitive scores are independent neurocognitive markers for first-episode MDD with a positive family history.
Findings
PFH-MDD patients showed worse language function and total cognitive scores compared to NFH-MDD patients.
Language function and total score independently predicted PFH-MDD with high discriminative accuracy (AUC > 0.96).
Cognitive impairments were more strongly associated with depression severity in PFH-MDD than in NFH-MDD.
Abstract
To identify specific neurocognitive risk markers in first-episode major depressive disorder (MDD) patients with positive family history (PFH). Antipsychotic-naive adults aged 18–60 were recruited across three groups: major depressive disorder patients with positive family history (PFH-MDD, n = 171), major depressive disorder patients with negative family history (NFH-MDD, n = 185), and healthy controls (HCs, n = 180). All patients met the DSM-5 criteria for first-episode MDD (HAMD-24 ≥ 17). Neurocognition was assessed with the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). Group differences were examined using the Kruskal–Wallis test and ANCOVA. Logistic regressions identified independent cognitive predictors; ROC curves evaluated discriminative validity. The RBANS total and domain scores differed across the groups (p < 0.001). PFH-MDD performed worse than…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
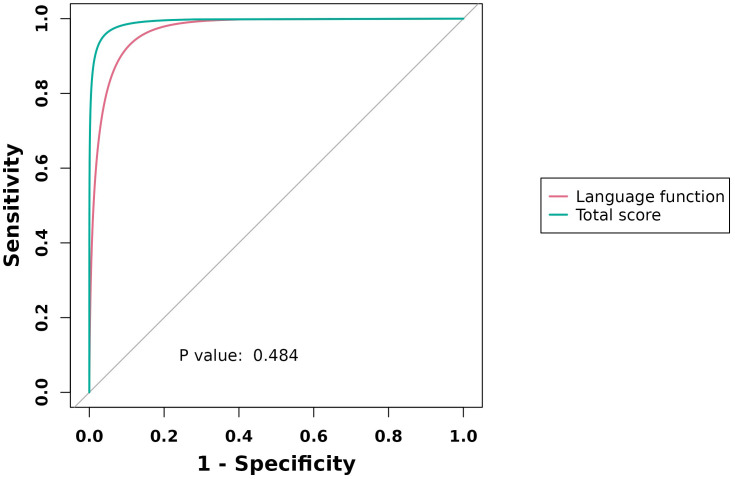 Figure 1
Figure 1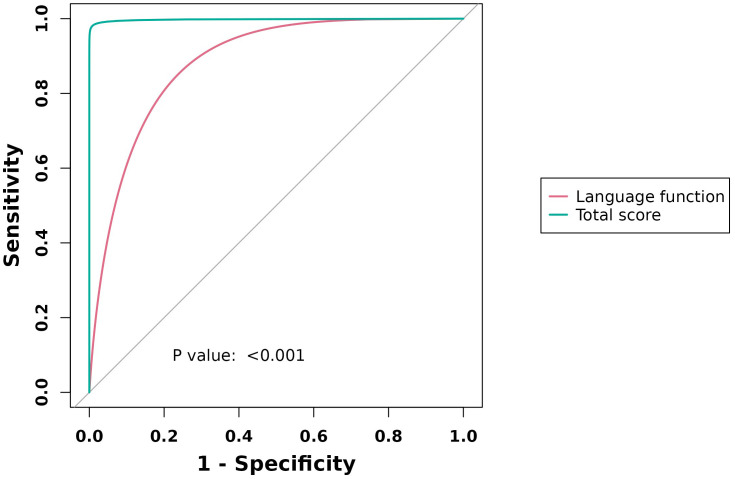 Figure 2
Figure 2| Group | n | Age (years) | Gender ( | Years of education (years) | Average duration (weeks) | HAMA (points) | HAMD (points) | |
|---|---|---|---|---|---|---|---|---|
| Male | Female | |||||||
| PFH-MDD | 171 | 31.8 ± 7.9 | 56 | 115 | 12.4 ± 1.7 | 18.5 ± 12.1 | 18.24 ± 5.13 | 26.5 ± 4.7 |
| NFH-MDD | 185 | 32.8 ± 8.6 | 60 | 125 | 12.7 ± 2.5 | 16.4 ± 11.7 | 16.94 ± 4.73 | 28.4 ± 4.4 |
| HCs | 180 | 34.6 ± 9.5 | 62 | 118 | 13.5 ± 3.3 | |||
| Neuropsychological status battery (RBANS) | PFH-MDD | NFH-MDD | HCs | |
|---|---|---|---|---|
| ( | ( | ( | ||
| Immediate memory | 35 (19, 45) | 34 (28, 40) | 52 (48, 56) | <0.001** |
| Visual span | 36 (33, 37) | 35 (34, 37) | 44 (39, 55) | <0.001** |
| Language function | 25 (17, 28) | 32 (29, 34) | 39 (36, 44) | <0.001** |
| Attention | 48 (18, 58) | 51 (48, 53) | 73 (67, 77) | <0.001** |
| Delayed memory | 42 (40, 48) | 39 (32, 53) | 57 (54, 60) | <0.001** |
| Total score | 174 (157, 199) | 192 (179, 201) | 276 (261, 283) | <0.001** |
| Neuropsychological status battery (RBANS) | PFH-MDD vs. NFH-MDD | PFH-MDD vs. HCs | NFH-MDD vs. HCs | |||
|---|---|---|---|---|---|---|
|
|
|
|
|
|
| |
| Immediate memory | 1.084 | 0.835 | −13.883 | <0.001** | −15.259 | <0.001** |
| Visual span | 1.375 | 0.508 | −13.749 | <0.001** | −15.417 | <0.001** |
| Language function | −8.233 | <0.001** | −10.292 | <0.001** | −18.269 | <0.001** |
| Attention | −1.349 | 0.177 | −14.375 | <0.001** | −15.434 | <0.001** |
| Delayed memory | 1.172 | 0.723 | −12.535 | <0.001** | −13.973 | <0.001** |
| Total score | −3.805 | <0.001** | −14.574 | <0.001** | −18.068 | <0.001** |
| Scale scores | PFH-MDD | NFH-MDD | ||||||
|---|---|---|---|---|---|---|---|---|
| Language function | Total score | Language function | Total score | |||||
|
|
|
|
|
|
|
|
| |
| HAMA | 0.107 | 0.164 | −0.04 | 0.607 | 0.402 | <0.001** | −0.143 | 0.052 |
| HAMD | −0.184 | 0.016* | −0.027 | 0.728 | −0.364 | <0.001** | −0.158 | 0.032* |
| RBANS scores | PFH-MDD and HCs | NFH-MDD and HCs | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI |
| OR | 95% CI |
| |||
| Language function | −0.82 | 0.676 | 0.993 | 0.042* | −0.93 | 0.716 | 1.214 | 0.604 |
| Total score | −0.90 | 0.853 | 0.942 | <0.001** | −0.77 | 0.675 | 0.867 | <0.001** |
| Group | Neuropsychological status battery (RBANS) | AUC (95% CI) | Sensitivity (%) | Specificity (%) | Cut-point |
|---|---|---|---|---|---|
| PFH-MDD | Language function | 0.967 (0.837, 0.982) | 98.80 | 87.80 | 34 |
| Total score | 0.991 (0.967, 0.997) | 96.50 | 98.90 | 224 | |
| NFH-MDD | Language function | 0.883 (0.846, 0.917) | 77.80 | 87.80 | 34 |
| Total score | 0.997 (0.983, 0.998) | 99.50 | 98.90 | 229 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTreatment of Major Depression · Anxiety, Depression, Psychometrics, Treatment, Cognitive Processes · Tryptophan and brain disorders
Introduction
Major depressive disorder is highly heritable (h² ≈ 40%–70%) (1). Meta-analyses of never-depressed first-degree relatives demonstrate small to medium deficits in intelligence, memory, and language (2, 3). Whether these deficits represent premorbid vulnerability markers or epiphenomena remains unresolved (4). We hypothesized that antipsychotic-naive first-episode major depressive disorder (MDD) patients with positive family history (PFH) would display a distinct cognitive signature predictive of disorder onset (5).
Methods
Participants
A large-scale case–control study was conducted in August 2020 and June 2023 at Hefei Fourth People’s Hospital. The inclusion criteria were as follows: 1) age 18–60 years, 2) DSM-5 first-episode MDD (SCID-5), 3) HAMD-24 ≥17, 4) PFH defined as ≥1 first-degree relative with DSM-5 MDD confirmed by hospital records, 5) no psychotropic medication, and 6) signed informed consent. The exclusion criteria include recurrent depression, other axis I disorders, ADHD, neurological illness, and substance dependence. Healthy controls (HCs) were community volunteers matched for age, gender, parental education, and estimated IQ (WASI-2). This study was approved by the Ethics Committee of the Fourth People’s Hospital of Hefei (No. HFSY-IRB-YJ-KYXM-CL.2024-064-001).
Clinical assessments
HAMD-24 (cutoff ≥ 17) and HAMA (cutoff ≥ 14) were validated in China. RBANS includes five index scores + total score (normative Chinese version; higher scores = better performance). Interrater ICC was >0.90.
Statistical analysis
SPSS 22.0 software was used for the statistical analysis. PASS 11.0 software was used to calculate the sample size. The measurement data conforming to the normal distribution are represented as mean ± SD. Count data conforming to a non-normal distribution were expressed as [M (P25, P75)]. Power analysis (GPower 3.1) indicated n = 171 per group to detect d = 0.30 at 90% power. Demographics were compared using one-way ANOVA or χ²; post hoc comparisons employed Tukey’s test. For RBANS, group differences were assessed using the Kruskal–Wallis test with Bonferroni post hoc corrections when appropriate. ANCOVA was used to compare groups controlling for gender, parental education, and IQ. Associations between variables were evaluated by Spearman’s ρ with FDR correction (q < 0.05). The Spearman’s correlation test was used to examine the correlation between the neurocognitive function in five dimensions (immediate memory, visual span, language function, attention, and delayed memory) with psychiatric symptoms (HAMA and HAMD scores). Logistic regression (enter) was adjusted for the above covariates; the Hosmer–Lemeshow value was >0.05, indicating a good fit. ROC analysis was used to establish optimal cut-points based on the Youden index. Significance was defined as two-tailed p < 0.05 (FDR-corrected for 20 primary tests).
Results
Sample characteristics
There were no significant differences in age, gender, years of education, or symptom severity among the groups (Table 1).
RBANS performance
PFH-MDD < NFH-MDD < HCs across all domains (p < 0.001). NFH was significantly higher than PFH on language function score and total score (p < 0.001). Effect sizes remained significant after covariate adjustment. Gender × group interactions were non-significant for all domains (p > 0.05) (Tables 2, 3).
Correlation analysis between RBANS scores (language function, total score) and HAMA and HAMD scores in PFH-MDD and NFH-MDD
In the PFH group, language function score was negatively correlated with HAMD score (r = −0.184, p = 0.016). In the NFH group, language function score was positively correlated with HAMA score (r = 0.402, p < 0.001) and negatively correlated with HAMD score (r = −0.364, p < 0.001). Total score was negatively correlated with HAMD score (r = −0.158, p = 0.032) (Table 4).
Cognitive predictors of group membership
Language function and total score independently predicted PFH-MDD vs. HCs (OR = −0.82 and −0.90); only total score predicted NFH-MDD vs. HCs (OR = −0.77). The results were corrected by FDR (Table 5).
ROC analysis
The AUC values for PFH-MDD were as follows: language = 0.967 (95% CI: 0.837–0.982) and total score = 0.991 (95% CI: 0.967–0.997). For NFH-MDD, the AUC values were as follows: language = 0.883 (95% CI: 0.846–0.917) and total score = 0.997 (95% CI: 0.983–0.998) (Table 6; Figures 1, 2).
ROC curve analysis of RBANS (language function, total score) in PFHG vs. HCs.
ROC curve analysis of RBANS (language function, total score) in NFHG vs. HCs.
Discussion
We examined neurocognitive profiles in 536 antipsychotic-naive adults experiencing their first major depressive episode. Patients with a positive family history of MDD (PFH-MDD, n = 171) showed significantly lower language and global RBANS scores than family-history-negative patients (NFH-MDD, n = 185) and HCs (n = 180) (6). Language and total scores survived adjustment for gender, parental education, and estimated IQ; predicted PFH-MDD vs. HCs with excellent discrimination (AUC ≥ 0.96); and were selectively correlated with symptom severity in PFH-MDD (7). These data indicate that language dysfunction is a robust, independent marker of familial risk for depression and may represent a target for early identification and preventive intervention (8).
The heritability of MDD is 40%–70% (1). By restricting the sample to first-episode, medication-free patients, we removed confounds of illness chronicity and treatment, allowing purer estimation of genetic load (9). The effect size for language impairment in PFH-MDD (Cohen’s d = 0.48) was more than twice that in NFH-MDD (d = 0.22), supporting a quantitative gene–cognition pathway rather than a simple “exposed vs. non-exposed” dichotomy (10). This gradient is consistent with recent polygenic-risk studies demonstrating that greater MDD polygenic scores are associated with reduced verbal fluency in the general population (11). Language tasks simultaneously recruit left inferior frontal gyrus, temporal pole, and inferior parietal lobule—regions showing hypoactivation during verbal fluency in drug-naive MDD (12), reduced cortical thickness in high-risk offspring (13), and oligodendrocyte-related gene downregulation in postmortem MDD (14). Thus, language dysfunction may mirror early neurodevelopmental alterations driven by oligodendroglial–synaptic genes implicated in MDD heritability (15).
From a practical standpoint, the RBANS language subtest requires <5 min, can be administered on paper or digitally, and is culture-fair in Chinese populations (16).A cutoff ≤28 yielded 96% sensitivity and 88% specificity for PFH-MDD in our ROC analysis. Embedding this brief screen in university or primary care mental health checkups could flag high-risk young adults before syndromal onset (17). Secondly, language-based cognitive training (e.g., semantic category generation, phonemic switching) has improved executive functions and functional outcome in established MDD (18); our findings justify testing such interventions in the prodromal phase (19). Negative studies often included recurrent cases, used coarse instruments (MMSE), or failed to control for IQ and parental education (20). We minimized these biases by recruiting only first-episode, medication-free participants, adjusting for estimated IQ and parental education, and correcting for 20 primary cognitive comparisons with FDR (21). The absence of gender × group interactions further suggests that our results are generalizable across sexes (22).
Limitations and future directions
The cross-sectional design precludes causal inferences; a 24-month follow-up of the present cohort is underway to determine whether language deficits predict conversion to MDD in high-risk relatives (23). RBANS is a screening battery; future work should incorporate comprehensive executive function and social cognition tasks (e.g., D-KEFS, hinting task) and digital phenotyping (24). Polygenic risk scores and epigenetic markers will be integrated to dissect gene–environment interactions underlying cognitive vulnerability (25). Replication in multi-ethnic samples is needed to confirm culture generalizability (26).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sullivan PF Neale MC Kendler KS . Genetic epidemiology of major depression: review and meta-analysis. Am J Psychiatry. (2000) 157:1552–62. doi: 10.1176/appi.ajp.157.10.1552, PMID: 11007705 · doi ↗ · pubmed ↗
- 2Mac Kenzie LE Uher R Pavlova B . Cognitive performance in first-degree relatives of individuals with vs without major depressive disorder: a meta-analysis. JAMA Psychiatry. (2019) 76:297–305. doi: 10.1001/jamapsychiatry.2018.3672, PMID: 30586133 PMC 6439825 · doi ↗ · pubmed ↗
- 3Cullen B Gameroff MJ Ward J Bailey MES Lyall DM Lyall LM . Cognitive function in people with familial risk of depression. JAMA Psychiatry. (2023) 80:610–20. doi: 10.1001/jamapsychiatry.2023.0716, PMID: 37074691 PMC 10116387 · doi ↗ · pubmed ↗
- 4Shen X Howard DM Adams MJ . A polygenic risk score for MDD associates with cognitive function in the general population. Psychol Med. (2022) 52:1–9.
- 5Van Dijk MT Murphy E Posner JE Talati A Weissman MM . Association of multigenerational family history of depression with lifetime depressive and other psychiatric disorders in children: results from the ABCD study. JAMA Psychiatry. (2021) 78:778–87. doi: 10.1001/jamapsychiatry.2021.0350, PMID: 33881474 PMC 8060885 · doi ↗ · pubmed ↗
- 6Kakeda S Watanabe K Katsuki A . Language-related brain abnormalities in drug-naïve major depressive disorder: a multimodal MRI study. J Affect Disord. (2021) 295:1104–11.
- 7Singh MK Kelley RG Chang KD . Gray matter structural alterations in pediatric offspring of patients with major depressive disorder. Psychiatry Res Neuroimag. (2022) 327:111532.
- 8Kim S Webster MJ . Correlation of GABA-related gene expression with oligodendrocyte markers in postmortem depression. Neuropsychopharmacology. (2020) 45:2053–61.