Large and giant intracranial aneurysms: outcomes from the multicenter prospective SMART coils registry
Yazan Ashouri, Alexandra R. Paul, Mohammad AlMajali, Amit Chaudhari, Eugene Lin, Min S. Park, Richard J. Bellon, Bradley N. Bohnstedt, Albert J. Yoo, Clemens M. Schirmer, Reade A. DeLeacy, David J. Fiorella, Keith Woodward, Harris E. Hawk, Ashish Nanda, Peter J. Sunenshine

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
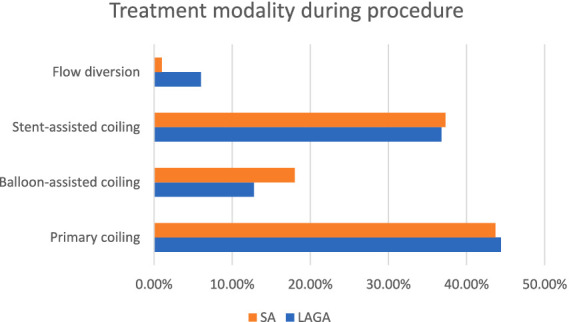 Figure 1
Figure 1| Baseline characteristics | Small aneurysms ≤10 mm ( | Large and giant aneurysms >10 mm ( | Difference SA-LAGA (95% CI) | |
|---|---|---|---|---|
| Age (mean, SD), years | 59.4 (12.47) | 62.0 (13.39) | −2.6 (−4.9, −0.3) | 0.0299 |
| Age, range (min, max) | 17.0, 93.0 | 20.0, 87.0 | NA | NA |
| Race | ||||
| American Indian or Alaska Native | 0.4% (3/772) | 0.0% | 0.4% (−0.1, 0.8%) | 1.0000 |
| Asian | 0.8% (6/772) | 0.0% | 0.8% (0.2, 1.4%) | 0.6003 |
| Black or African American | 4.4% (34/772) | 3.0% (4/133) | 1.4% (−1.8, 4.6%) | 0.6396 |
| White | 26.4% (204/772) | 23.3% (31/133) | 3.1% (−4.7, 10.9%) | 0.5207 |
| Native Hawaiian or Other Pacific Islander | 0.0% | 0.0% | NA | NA |
| Other | 1.3% (10/772) | 5.3% (7/133) | −4.0% (−7.8, −0.1%) | 0.0068 |
| Ethnicity | ||||
| Hispanic or Latino | 3.4% (26/772) | 3.8% (5/133) | −0.4% (−3.9, 3.1%) | 0.7963 |
| Not Hispanic or Latino | 29.9% (231/772) | 27.8% (37/133) | 2.1% (−6.2, 10.4%) | 0.6813 |
| Female | 75.4% (582/772) | 70.7% (94/133) | 4.7% (−3.6, 13.0%) | 0.2800 |
| Comorbidities | ||||
| Hypertension | 62.4% (482/772) | 57.9% (77/133) | 4.5% (−4.5, 13.6%) | 0.3348 |
| Diabetes mellitus | 14.4% (111/772) | 16.5% (22/133) | −2.2% (−8.9, 4.6%) | 0.5086 |
| Smoking | 63.2% (488/772) | 61.7% (82/133) | 1.6% (−7.4, 10.5%) | 0.7707 |
| Former | 28.8% (222/772) | 27.8% (37/133) | 0.9% (−7.3, 9.2%) | 0.9173 |
| Current | 33.5% (259/772) | 33.1% (44/133) | 0.5% (−8.2, 9.1%) | 1.0000 |
| Unknown | 0.9% (7/772) | 0.8% (1/133) | 0.2% (−1.5, 1.8%) | 1.0000 |
| Coronary artery disease | 4.0% (31/772) | 8.3% (11/133) | −4.3% (−9.1, 0.6%) | 0.0424 |
| Peripheral artery disease | 1.3% (10/772) | 2.3% (3/133) | −1.0% (−3.6, 1.7%) | 0.4208 |
| Hyperlipidemia | 12.8% (99/772) | 10.5% (14/133) | 2.3% (−3.4, 8.0%) | 0.5698 |
| Aneurysm size, mean (SD), mm | 5.8 (1.95) | 13.7 (3.59) | −8.0 (−8.4, −7.6) | <0.0001 |
| Size range (min, max), mm | 1.0, 10.0 | 10.1, 29.0 | NA | NA |
| Aneurysm location | ||||
| MCA | 12.7% (98/772) | 11.3% (15/133) | 1.4% (−4.5, 7.3%) | 0.7764 |
| ACom | 28.0% (216/772) | 10.5% (14/133) | 17.5% (11.4, 23.6%) | <0.0001 |
| ICA terminus | 3.1% (24/772) | 3.0% (4/133) | 0.1% (−3.0, 3.3%) | 1.0000 |
| Basilar tip | 0.8% (6/772) | 3.8% (5/133) | −3.0% (−6.3, 0.3%) | 0.0140 |
| PCom | 17.5% (135/772) | 20.3% (27/133) | −2.8% (−10.2, 4.5%) | 0.4624 |
| Pericallosal | 3.0% (23/772) | 0.8% (1/133) | 2.2% (0.3, 4.1%) | 0.2367 |
| Cavernous | 0.6% (5/772) | 4.5% (6/133) | −3.9% (−7.4, −0.3%) | 0.0022 |
| Aneurysm shape | ||||
| Saccular | 87.7% (677/772) | 75.9% (101/133) | 11.8% (4.1, 19.4%) | 0.0007 |
| Fusiform | 1.4% (11/772) | 8.3% (11/133) | −6.8% (−11.6, −2.1%) | <0.0001 |
| Dissecting | 2.3% (18/772) | 3.8% (5/133) | −1.4% (−4.8, 2.0%) | 0.3652 |
| Other | 8.0% (62/772) | 12.0% (16/133) | −4.0% (−9.9, 1.9%) | 0.1332 |
| Wide neck | 59.7% (461/772) | 69.9% (93/133) | −10.2% (−18.7, −1.7%) | 0.0268 |
| Small neck | 37.0% (286/772) | 24.1% (32/133) | 13.0% (5.0, 21.0%) | 0.0042 |
| Aneurysm status | ||||
| Ruptured | 31.7% (245/772) | 32.3% (43/133) | −0.6% (−9.2, 8.0%) | 0.9198 |
| Unruptured | 68.3% (527/772) | 67.7% (90/133) | 0.6% (−8.0, 9.2%) | 0.9198 |
| Treatment outcomes | Small aneurysms ≤10 mm ( | Large and giant aneurysms >10–25 mm ( | Difference SA-LAGA (95% CI) | |
|---|---|---|---|---|
| Efficacy | ||||
| Packing density (calculated), mean (SD)% | 34.1 (18.28) | 21.1 (13.06) | 13.0 (10.3, 15.8) | <0.0001 |
| Raymond-Roy occlusion classification (postprocedure) %, ( | <0.0001 | |||
| Class I | 43.8% (338/771) | 23.3% (30/129) | 20.6% (12.5, 28.7%) | |
| Class II | 39.4% (304/771) | 34.9% (45/129) | 4.5% (−4.4, 13.5%) | |
| Class III | 16.7% (129/771) | 41.9% (54/129) | −25.1% (−34.0, −16.2%) | |
| Class I to II | 83.3% (642/771) | 58.1% (75/129) | 25.1% (16.2, 34.0%) | <0.0001 |
| Raymond-Roy occlusion classification (1-year follow-up) | 0.0041 | |||
| Class I | 66.6% (409/614) | 53.1% (52/98) | 13.6% (3.0, 24.1%) | |
| Class II | 24.6% (151/614) | 29.6% (29/98) | −5.0% (−14.7, 4.7%) | |
| Class III | 8.8% (54/614) | 17.3% (17/98) | −8.6% (−16.4, −0.7%) | |
| Class I to II | 91.2% (560/614) | 82.7% (81/98) | 8.6% (0.7, 16.4%) | 0.0166 |
| Aneurysm lesion occlusion % ( | ||||
| Better (progressive occlusion) | 37.6% (231/614) | 50.0% (47/94) | −12.4% (−23.2, −1.6%) | 0.0237 |
| Stable | 49.7% (305/614) | 36.2% (34/94) | 13.5% (3.0, 24.0%) | 0.0150 |
| Worse (recanalization) | 12.7% (78/614) | 13.8% (13/94) | −1.1% (−8.6, 6.3%) | 0.7417 |
| Safety, % ( | ||||
| Retreatment through follow-up% ( | 6.4% (40/627) | 11.5% (12/104) | −5.2% (−11.6, 1.3%) | 0.0648 |
| Mortality, % ( | ||||
| Within 24 h of procedure | 0.1% (1/772) | 0.0% | 0.1% (−0.1, 0.4%) | 1.0000 |
| After 24 h from procedure | 4.5% (35/772) | 9.8% (13/133) | −5.2% (−10.5, 0.0%) | 0.0197 |
| Mortality at 1-year follow up | 4.7% (36/772) | 9.8% (13/133) | −5.1% (−10.4, 0.2%) | 0.0222 |
| Device-related mortality | 0.1% (1/772) | 0.0% | 0.1% (−0.1, 0.4%) | 1.0000 |
| Procedure-related mortality | 0.3% (2/772) | 0.0% | 0.3% (−0.1, 0.6%) | 1.0000 |
| Mortality after 365 days | 0.3% (2/772) | 1.5% (2/133) | −1.2% (−3.3, 0.9%) | 0.1052 |
| Serious adverse events, % ( | ||||
| Device-related | 4.1% (32/772) | 4.5% (6/133) | −0.4% (−4.2, 3.4%) | 0.8153 |
| Procedure-related | 8.7% (67/772) | 9.8% (13/133) | −1.1% (6.5, 4.3%) | 0.6236 |
| Functional outcome | ||||
| mRS 0–2 at 1-year, % ( | 86.4% (376/435) | 72.6% (53/73) | 13.8% (3.1, 24.6%) | 0.0047 |
| Raymond-Roy occlusion | Wide neck ≤10 mm ( | Wide neck >10 mm ( | Difference SA-LAGA (95% CI) | |
|---|---|---|---|---|
| Postprocedure | <0.0001 | |||
| Class I | 39.9% (184/461) | 22.0% (20/91) | 17.9% (8.3, 27.5%) | |
| Class II | 40.8% (188/461) | 31.9% (29/91) | 8.9% (−1.7, 19.5%) | |
| Class III | 19.3% (89/461) | 46.2% (42/91) | −26.8% (−37.7%, −16.0%) | |
| Class I to II | 80.7% (372/461) | 53.8% (49/91) | 26.8% (16.0, 37.7%) | <0.0001 |
| Final follow-up | 0.0002 | |||
| Class I | 69.6% (263/378) | 47.8% (32/67) | 21.8% (9.0, 34.6%) | |
| Class II | 24.1% (91/378) | 34.3% (23/67) | −10.3% (−22.4, 1.9%) | |
| Class III | 6.3% (24/378) | 17.9% (12/67) | −11.6% (−21.1%, −2.1%) | |
| Class I to II | 93.7% (354/378) | 82.1% (55/67) | 11.6% (2.1, 21.1%) | 0.0055 |
| Raymond-Roy occlusion | Primary coiling | Balloon-assisted coiling | Stent-assisted coiling | Flow diversion | |
|---|---|---|---|---|---|
| Postprocedure | 0.112 | ||||
| Class I | 17 (39.4%) | 6(35.3%) | 7(14.6%) | 0 | |
| Class II | 18(31%) | 7(41.2%) | 19(39.6%) | 1(16.7%) | |
| Class III | 23(39.7%) | 4(23.5%) | 22(45.8%) | 5(83.3%) | |
| Class I-II | 35(60.3%) | 11(76.5%) | 26(54.2%) | 1(16.7%) | 0.071 |
| Final follow-up | |||||
| Class I | 23 (51.1%) | 7 (58.3%) | 18 (52.9%) | 4 (57.1%) | 1.00 |
| Class II | 14 (31.1%) | 3 (25%) | 19 (29.4%) | 2 (28.6%) | |
| Class III | 8 (17.8%) | 2 (16.7%) | 6 (17.6%) | 1 (14.3%) | |
| Class I-II | 37 (82.2%) | 10 (83.3%) | 28 (82.4%) | 6 (85.7%) | 0.966 |
| Baseline characteristics | aOR | 95% CI | |
|---|---|---|---|
| Age | 0.95 | 0.90–1.01 | 0.077 |
| Packing density | 1.00 | 0.99–1.01 | 0.249 |
| Primary coiling | Ref | – | – |
| BAC | 1.05 | 0.15–7.29 | 0.96 |
| SAC | 1.87 | 0.38–9.21 | 0.44 |
| FD | 11.2 | 0.5–253 | 0.13 |
| Wide-neck aneurysm | 2.31 | 0.54–9.94 | 0.260 |
| Aneurysm type | |||
| Saccular | Ref | – | – |
| Other | 1.21 | 0.08–20.14 | 0.894 |
| Fusiform | 0.16 | 0.02–1.21 | 0.077 |
| Dissecting | 1.95 | 0.25–15.0 | 9,521 |
| Aneurysm size (mm) | 0.95 | 0.92–0.99 | 0.005 |
| Ruptured aneurysm | 1.08 | 0.26–4.40 | 0.918 |
| Baseline characteristics | aOR | 95% CI | |
|---|---|---|---|
| Age | 0.979 | 0.91–1.05 | 0.572 |
| Packing density | 1.04 | 0.99–1.01 | 0.149 |
| Primary coiling | Ref | – | – |
| BAC | 0.06 | 0.02–1.64 | 0.100 |
| SAC | 0.12 | 0.01–2.04 | 0.144 |
| Wide-neck aneurysm | 2.07 | 0.39–10.8 | 0.38 |
| Aneurysm type | |||
| Saccular | Ref | – | – |
| Fusiform | 2.04 | 0.1–94.5 | 0.72 |
| Dissecting | 0.054 | 0.9–86.9 | 0.06 |
| Aneurysm size (mm) | 0.94 | 0.90–0.98 | 0.004 |
| Ruptured aneurysm | 0.029 | 0.01–0.414 | 0.009 |
| Wide neck aneurysm | 1.617 | 0.35–7.56 | 0.541 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Vascular Malformations Diagnosis and Treatment · Meningioma and schwannoma management
Introduction
1
Large and giant aneurysms (LAGA) are defined as aneurysms with at least one dimension measuring (>10–25 mm) and (>25 mm), respectively. These relatively uncommon lesions, representing about 7% of unruptured intracranial aneurysms (1), are characterized by progressive growth, thrombosis, and a high risk of rupture (2–4), and mortality (5). LAGA pose a significant challenge for treatment due to their size, association with wide neck morphology, and proximity to cranial nerves and the brain stem.
Active treatment aiming for LAGA occlusion, prevention of the aneurysmal rebleeding, relief of mass effect, and reduction of embolic complications is commonly pursued. Endovascular coiling for the treatment of cerebral aneurysms has been evolving since the results of the International Subarachnoid Aneurysm Trial (ISAT) and the BRAT (Barrow Ruptured Aneurysm Trial) were published (6, 7). Despite improving treatment strategies, the efficacy and safety of endovascular coiling of LAGA are still debated, with a high risk of recurrence and the necessity of further treatment commonly cited (4, 8–11).
The results of the SMART Registry were recently published (12). In this article, we describe a subgroup analysis comparing outcomes for LAGA and small aneurysms (SA) treated with the Penumbra SMART COIL (SMART) System, which includes SMART COIL, Penumbra Coil 400 (PC400), and Penumbra Occlusive Device (POD) indicated for endovascular embolization in the peripheral and cerebral vasculature.
Methods
2
Design
2.1
The SMART Study was a prospective, single-arm, post-market, multicenter registry of the SMART System (Penumbra, Inc.; ClinicalTrials.gov Identifier: NCT02729740). The registry was approved by the local Institutional Review Board (IRB) and Ethics Committee (EC) and conducted in accordance with relevant clinical research regulations. Written informed consent was provided by the study participant or their legally authorized representative (LAR). Emergent patients were enrolled after signing the consent within one calendar day after the procedure or if a LAR signed on their behalf. Penumbra, Inc., provided sponsor oversight of this trial.
Eligibility criteria, outcomes and data collection
2.2
Eligibility criteria, outcomes, and data collection have been described previously (12). Patients were excluded if SMART, PC400, or POD coils accounted for <75% of the total number of coils implanted, if their life expectancy was <1 year, if they were already enrolled in the SMART Registry, or if they were participating in other investigations that could confound results. All study procedures were completed per site’s standard of care. Adjunctive techniques and devices were permitted per study inclusion criteria. The aneurysm occlusion status was determined from cerebral angiograms obtained immediately and 1 year (± 6 months) postprocedure according to Raymond–Roy occlusion classification (RROC, class I: complete obliteration, class II: residual neck, class III: residual aneurysm) (13). For ruptured aneurysms, clinical grading of SAH was determined at admission, with no restriction on grade for enrollment, using the Hunt and Hess scale (14). Coil packing density was calculated by using either software calculators or by calculating aneurysm volume assuming an ellipsoid model and coil volume [V = π (p/2)^2^ × L], where p represents primary coil diameter, and L represents coil length. Packing density was not calculated for patients with deconstructive treatment, fusiform or dissecting aneurysms (12). Wide-necked aneurysms were defined as follows: a dome-to-neck ratio <2 or a neck width ≥4 mm.
The retreatment rate at 1 year and device-related serious adverse events (SAEs) within 24 h of the procedure were the primary efficacy and primary safety outcomes. The secondary outcome was the immediate adequate occlusion, defined as RR occlusion Class I or II. Other short-term follow-up outcomes included all periprocedural SAEs (SAEs within 24 h of the procedure), SAEs 24 h after the procedure, and all-cause mortality within 24 h. One-year outcomes included adequate occlusion, recanalization, modified Rankin Scale (mRS) 0 to 2, all-cause mortality, and SAEs.
Statistical analysis
2.3
We reported two-sided a 95% t confidence intervals (continuous data) or Wald asymptotic intervals (categorical data) were presented. Continuous variables were summarized with descriptive statistics [n, mean, standard deviation, median, and interquartile range (IQR)]. Frequency counts and percentages of subjects within each category were included for categorical data. A subgroup analysis was conducted on aneurysm size in the overall population and the wide-neck aneurysm subset. Two-sided 95% Wald asymptotic intervals for the difference in binomial proportions and two-sided p values based on Fisher’s Exact Test for categorical data, the t-test for continuous data, and the Wilcoxon rank-sum test using normal approximations for ordinal data were reported for the subgroup comparison. SAS 9.4 (SAS Institute) was used for statistical programming.
Results
3
Demographics
3.1
The SMART registry included 905 patients with intracranial aneurysms treated at 67 North American sites between June 2016 and August 2018. Of these, 14.7% (N = 133) had LAGA (Table 1). Patients with LAGA were older [mean (SD), 62.0 (13.4) vs. 59.4 (12.5), p = 0.0299] compared to patients with SA. Female patients were predominant, comprising 70.7% of LAGA and 75.4% of SA patients (p = 0.28). In both groups, more than half of the patients were hypertensive (57.9% vs. 62.4%, p = 0.3348) and one-third were current smokers (33.1% vs. 33.5%, p = 1.0) for LAGA and SA, respectively.
Aneurysm characteristics
3.2
Aneurysm characteristics for LAGA and SA are outlined in Table 1. The mean (SD) aneurysm size was 13.7 (3.59) mm for LAGA and 5.8 (1.95) mm for SA (p value <0.0001). Almost one-third of all aneurysms were ruptured (32.3% for LAGA and 31.7% for SA; p = 0.9198). Of these, 36.6% LAGA and 44.6% SA had Hunt and Hess ≥3 (p = 0.3958). The most common location for LAGA was the posterior communicating artery (PCom) (20.3%), while the most common location for SA was the anterior communicating artery (ACom) (28%). LAGA were more likely to present at the basilar tip (3.8% vs. 0.8%, p = 0.0140) and the cavernous segment (4.5% vs. 0.6%, p = 0.0022) and less likely to present in the ACom (10.5% vs. 28.0%, p < 0.0001) compared to SA. In terms of morphological characteristics, LAGA were less likely to be saccular (75.9% vs. 87.7%, p = 0.0007), more likely to be fusiform (8.3% vs. 1.4%, p < 0.0001), and wide-necked (69.9% vs. 59.7%, p = 0.0268) compared to SA.
Aneurysm treatment
3.3
LAGA and SA were similar in the utilization of primary, unassisted coiling (43.6% vs. 43.3%), stent-assisted coiling (SAC, 36.8% vs. 37.3%), and balloon-assisted coiling (15.8% vs. 21.1%) (all p > 0.1) (Figure 1). However, LAGA were more likely to be treated with adjunctive flow diversion (6.0% vs. 1.0%, p = 0.0008) compared to SA. Within the LAGA group, a larger aneurysm sac was associated with lower rates of primary coiling (52.7% vs. 21.2% vs. 28.6%, p = 0.0028) and higher rates of flow diversion (2.2% vs. 12.1% vs. 28.6%, p = 0.0075) for aneurysms (10–15 mm), (15–20 mm) and (>20 mm), respectively. This trend was not seen in aneurysms <10 mm.
Endovascular treatment strategies employed in patients with small aneurysms (SA) vs. large and giant aneurysms (LAGA).
Treatment outcomes
3.4
Treatment outcomes for LAGA and SA are outlined in Table 2. Across the entire study cohort, the mean clinical and radiological follow-up period was 9.5 months (range: from 42 to 850 days). Packing density was significantly lower in LAGA, compared to SA [mean (SD) = 21.1(13.06) vs. 34.1(18.3), p < 0.001]. There was a trend toward lower packing density as aneurysmal size increase [Mean(SD) 23.5(18) vs. 17.9(10.6) vs. 13.3(8), p = 0.08] for aneurysm 10–15 mm vs. 15–20 vs. > 20. Adequate occlusion postprocedure (RROC I-II) was achieved in 58.1% of LAGA compared to 83.3% of SA, p < 0.0001.
Angiographic data at 1-year follow-up was available for 98 (73.7%) patients with LAGA and 614 (79.5%) patients with SA. Adequate occlusion (RROC I-II) on follow-up was lower in LAGA compared to SA (82.7% vs. 91.2%, p = 0.0166). However, the recanalization rates were similar between the two groups (13.8% vs. 12.7%, p = 0.7417 for LAGA and SA, respectively). Progressive occlusion of aneurysms on follow-up was more likely in patients with LAGA compared to SA (50.0% vs. 37.6%, p = 0.0237). Further, the retreatment rates through follow-up were similar between LAGA and SA (11.5% vs. 6.4%; p = 0.0648).
In terms of good functional outcome, LAGA patients were less likely to achieve mRS 0–2 at 1-year follow-up compared to SA patients (72.6% vs. 86.4%, p = 0.0047; Table 2). There was no device- or procedure-related periprocedural mortality in the LAGA cohort, while device- or procedure-related mortality was 0.3% in the SA cohort (p = 1.0). However, all-cause mortality >24 h postprocedure was significantly higher in LAGA (9.8% vs. 4.5%, p = 0.0197) compared to SA. Similar was true for all-cause mortality at 1-year follow-up (9.8% vs. 4.7% for LAGA and SA, respectively; p = 0.0222).
A subgroup analysis was performed to compare the treatment outcomes of patients with wide-neck LAGA and SA (Table 3). We noted that patients with wide-neck LAGA were less likely to achieve adequate occlusion postprocedure (RROC I-II: 53.8% vs. 80.7%, p < 0.0001) and at 1-year follow-up (82.1% vs. 93.7%, p = 0.0055) compared to wide-neck SA.
Further analysis on adequate occlusion post-procedure and on follow-up revealed that BAC treatment showed a trend towards better adequate occlusion rates post-procedure(76.5%) with p = 0.07 compared to 60.3, 54.2 and 16.7% for primary coiling, SAC and flow diversion, respectively (Table 4). There was no statistical difference in terms of adequate occlusion on follow-up between different treatment techniques.
A multivariate logistic regression model exploring predictive factors for 1-year adequate occlusion demonstrated that aneurysm size (aOR: 0.95, CI: 0.92–0.99, p: 0.005) was a significant predictor of achieving adequate occlusion on follow-up imaging. (Table 5).
Moreover, a multivariate analysis exploring factors associated with good functional outcome in patients with LAGA who had 1 year follow-up. After adjusting for possible confounders, aneurysm size and rupture status were associated with lower odds of achieving good functional outcome (Table 6). Dissecting aneurysms showed a trend towards worse functional outcome but did not reach statistical significance.
Discussion
4
Multiple series have reported safe outcomes in intracranial aneurysms treated using the SMART Coil system (15–18). The current subgroup analysis is the first to investigate the safety and efficacy of primary and assisted coiling in patients with LAGA treated with a single EVT coil family in an international, multicenter setting.
The stable embolization rate for LAGA using coils is typically lower than for SA (8). Patients in our series demonstrated similar occlusion rates and favorable outcomes to the previously published literature focused on endovascular coiling of LAGA. Immediate occlusion was found in 87.6% of aneurysms in the Chalouhi et al. (8), series and 58.1% in our series. At 1 year, an adequate occlusion was seen in 82.7% of cases, although our series had double the number of fusiform aneurysms (8.3% versus 4.1%).
Complication rates related to the target procedure were also similar; in our series 9.8% vs. 10.5% in Chalouhi et al. (8), and 10.2% in Wang et al. (19). Thirty-nine of aneurysms in the Chalouhi et al. (8) study demonstrated recanalization and 33% required further treatment by 25.4 months, compared to 13.8 and 11.5%, respectively, at 9.5 months in our series. This observation may (at least in part) be explained by a longer follow-up in the Chalouhi et al. (8) study compared to our series. Other groups have published recurrence rates as high as 57.9% with a retreatment rate of 25.5% (19).
The Chalouhi et al. (8) study also found that stent-assisted coiling was associated with lower recurrence rates and had 27.5% of cases in this category compared to 36.8% in our series. This aligns with the national trend moving away from primary coil embolization in more complex aneurysm cases (20).
Our all-cause mortality rate at 1 year (9.8%) was comparable to previous studies analyzing endovascularly treated large and giant aneurysms (19, 21, 22); importantly, none of the occurrences were device or procedure-related. One of the key findings of the study was the significant progression of occlusion in LAGA accompanied by a low recanalization rate. Notably, achieving RROC I-II in LAGA improved from 58.1% postprocedure to 82.7% on follow-up, and only 13.8% of aneurysms recanalized.
In summary, our series demonstrates that coil embolization of large and giant aneurysms with the SMART system yields occlusion rates and patient outcomes comparable to ones reported for other coiling technologies. These positive results may be partly due to the progressive coil softness and inner structural wire that might lead to less compartmentalization.
Limitations
4.1
This study followed an international, multicenter design that allowed for the evaluation of outcomes of the procedures conducted by different operators in various hospital care models. However, study limitations must be addressed to interpret our data fairly. The chief limitation is that data were provided by each study center without a core laboratory and blinded adjudication. As such, the physician-reported rates of aneurysm occlusion might have been subject to bias. The study was not powered for subgroup comparisons. Moreover, the utilization of dual antiplatelet agents was not collected and was at discretion of treating physician. Additionally, the primary intent of the study was to assess the outcomes of coiling technology. Alternative endovascular techniques, such as flow diverters, were out of scope for this analysis due to the limited data available. Finally, the study followed patients for 1 year only, and a longer-term follow-up would aid in understanding of post-treatment recurrence rates more accurately.
Conclusion
5
Despite the known challenges treating large and giant aneurysms, the SMART registry demonstrated high adequate aneurysm occlusion rates on follow-up imaging and good independent functional outcomes. This study provides further evidence for the efficiency and safety of the SMART System for the treatment of large and giant aneurysms in a real-world clinical setting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vlak MHM Algra A Brandenburg R Rinkel GJE. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. (2011) 10:626–36. doi: 10.1016/S 1474-4422(11)70109-0, 21641282 · doi ↗ · pubmed ↗
- 2Investigators TI So UIA. Unruptured intracranial aneurysms—risk of rupture and risks of surgical intervention. N Engl J Med. (1998) 339:1725–33. doi: 10.1056/NEJM 1998121033924019867550 · doi ↗ · pubmed ↗
- 3Brown RD Broderick JP. Unruptured intracranial aneurysms: epidemiology, natural history, management options, and familial screening. Lancet Neurol. (2014) 13:393–404. doi: 10.1016/S 1474-4422(14)70015-8, 24646873 · doi ↗ · pubmed ↗
- 4Murayama Y Takao H Ishibashi T Saguchi T Ebara M Yuki I . Risk analysis of unruptured intracranial aneurysms: prospective 10-year cohort study. Stroke. (2016) 47:365–71. doi: 10.1161/STROKEAHA.115.010698, 26742803 · doi ↗ · pubmed ↗
- 5Choi IS David C. Giant intracranial aneurysms: development, clinical presentation and treatment. Eur J Radiol. (2003) 46:178–94. doi: 10.1016/S 0720-048X(03)00090-112758113 · doi ↗ · pubmed ↗
- 6Molyneux A. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. (2002) 360:1267–74. doi: 10.1016/S 0140-6736(02)11314-6, 12414200 · doi ↗ · pubmed ↗
- 7Spetzler RF Mc Dougall CG Albuquerque FC Zabramski JM Hills NK Partovi S . The Barrow ruptured aneurysm trial: 3-year results: clinical article. J Neurosurg. (2013) 119:146–57. doi: 10.3171/2013.3.JNS 12683, 23621600 · doi ↗ · pubmed ↗
- 8Chalouhi N Tjoumakaris S Gonzalez LF Dumont AS Starke RM Hasan D . Coiling of large and giant aneurysms: complications and long-term results of 334 cases. AJNR Am J Neuroradiol. (2014) 35:546–52. doi: 10.3174/ajnr.A 3696, 23945229 PMC 7964717 · doi ↗ · pubmed ↗