Rarity of Acute Pancreatitis as an Initial Presentation of Lung Carcinoma
Navin Kumar, Nayana S. Kumar, Prasoon Saxena, Ijan Dhamala, Nishit Jain, Karamveer Singh, Somprakas Basu

TL;DR
A rare case where a lung cancer diagnosis was first revealed through acute pancreatitis symptoms in a 75-year-old man.
Contribution
Highlights the rare occurrence of acute pancreatitis as the initial sign of lung carcinoma.
Findings
Acute pancreatitis can be a rare initial presentation of metastatic lung carcinoma.
The case involved a 75-year-old man diagnosed with lung cancer after presenting with pancreatitis.
Abstract
Gallstones and alcohol consumption are the most common causes of acute pancreatitis. Lung carcinoma typically presents with respiratory symptoms, and in some cases, locoregional or distant metastases. However, acute pancreatitis as the initial manifestation of lung carcinoma is rare. Herein, we report the case of a 75 year‐old man who presented with acute pancreatitis and was diagnosed with metastatic lung carcinoma upon evaluation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1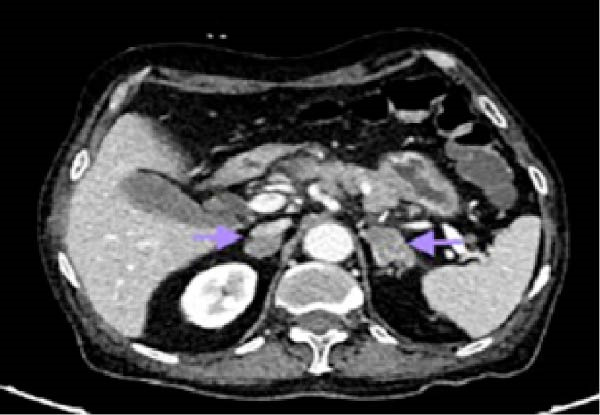 Figure 2
Figure 2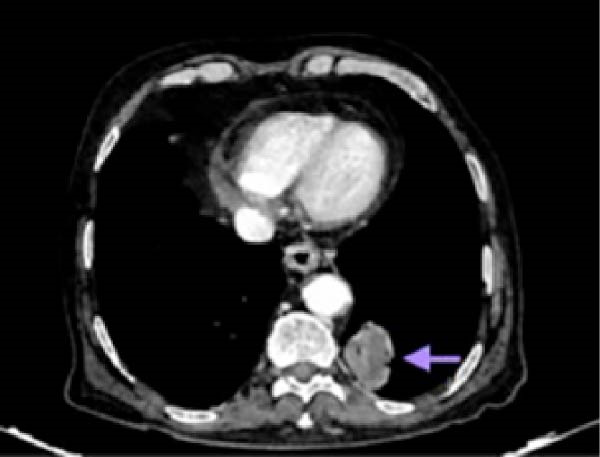 Figure 3
Figure 3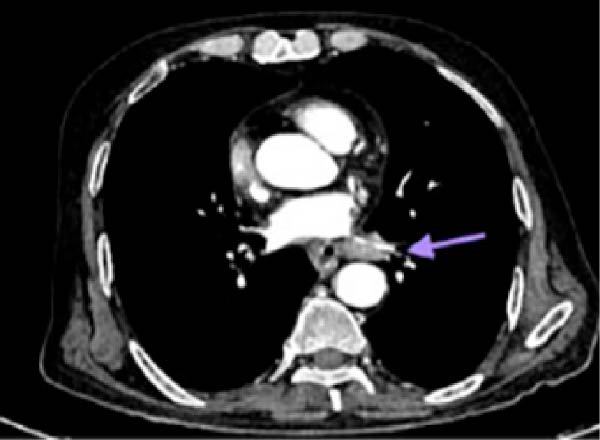 Figure 4
Figure 4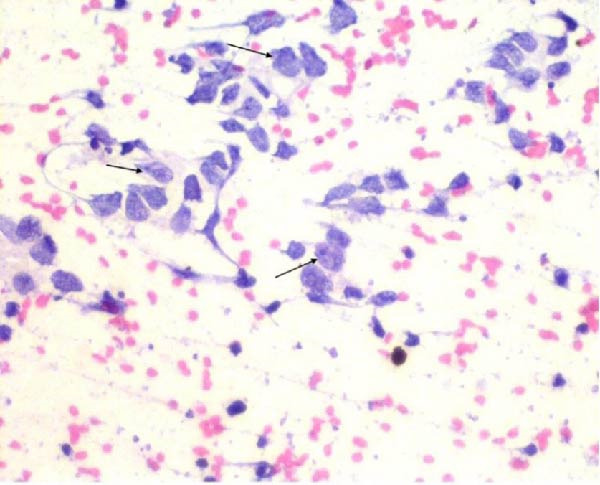 Figure 5
Figure 5| Investigation | Value | Reference |
|---|---|---|
| Hemoglobin | 10.2 | 11.0–13.0 g% |
| Total leucocyte count | 8700 | 4000–11,000/cc |
| Platelets | 110,000 | 150,000–450,000/cc |
| PT/INR | 12.1/0.97 | 11.8/1.03 |
| Bilirubin (total/direct) | 1.1./0.26 | 0.3–1.2 mg/dL |
| ALT | 79 | 0–35 IU |
| AST | 88 | 0–35 IU |
| ALP | 332 | 30–120 IU |
| Lipase | 1790 | 10–140 U/L |
| Amylase | 850 | 40–140 U/L |
| Calcium | 12.5 | 8.4–10.3 mg/dL |
| Albumin | 3.5 | 3.5–5.2 g/dL |
| Urea | 26 | 17–43 mg/dL |
| Creatinine | 1 | 0.55–1.02 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Pancreatic and Hepatic Oncology Research · Dermatological and COVID-19 studies
1. Introduction
Acute pancreatitis is common in surgical practice, and gallstones and alcohol consumption are its most common etiologies. Lung carcinoma is one of the rarest cause of acute pancreatitis, most commonly observed cases involving the small cell variant. Non‐small cell lung carcinoma (NSCLC) is an aggressive tumor with early metastatic potential and poor prognosis [1]. The probable causes of acute pancreatitis in lung carcinoma include hypercalcemia and pancreatic metastasis. Very few cases of small cell lung carcinoma have been described presenting as acute pancreatitis are reported in the literature.
2. Case Report
A male smoker aged 75 years presented to the emergency department with abdominal pain radiating to his back and multiple episodes of vomiting for 3 days prior to presentation. He also had a history of anorexia and weight loss of approximately 10 kg over the past 3 months. He had no history of alcohol consumption. He was afebrile with a heart rate of 88/min and blood pressure of 110/80 mmHg. Abdominal examination revealed tenderness in the epigastrium and a 3 cm × 3 cm hard nontender lymph node in the right inguinal region. The rest of the abdomen was unremarkable. The laboratory investigations revealed raised serum amylase, lipase, alkaline phosphatase, and calcium (Table 1). The rest of the blood investigations, including lipid profile, were unremarkable.
The Glasgow–Imrie score was two. The patient was clinically diagnosed with acute pancreatitis. Ultrasonography of abdomen revealed a single large stone in the gallbladder, and the common bile duct (CBD) was 5 mm in diameter without any stones. Hence, MRCP was not performed on the patient. Contrast‐enhanced computed tomography (CT) of the abdomen revealed Balthazar grade C acute pancreatitis with pancreatic gland abnormalities, and a peripancreatic inflammation suggesting a CT severity index of 4/10. Multiple enlarged mesenteric, peripancreatic, gastro‐hepatic, retroperitoneal, right external iliac, and right inguinal lymph nodes were noted (Figure 1). Metastatic bulky bilateral adrenal glands were also noted (Figure 2).
Contrast‐enhanced computed tomography of the abdomen showing acute interstitial pancreatitis (arrow) with multiple mesenteric, peripancreatic, gastro‐hepatic, and retroperitoneal lymph nodes.
Contrast‐enhanced computed tomography of the abdomen showing metastatic bulky bilateral adrenal glands (arrows).
CT of the chest revealed an enhancing lesion with soft tissue attenuation measuring 3.2 cm × 3.4 cm in the posterior–basal segment of the left lower lobe (Figure 3), and multiple conglomerated, heterogeneously enhancing lymph nodes in the mediastinal and bilateral hilar regions, with the largest measuring 2.8 cm × 1.8 cm (Figure 4). CECT of thorax (Figures 3 and 4) was suggestive of lung cancer.
Contrast‐enhanced computed tomography of the chest showing an enhancing lesion with soft tissue attenuation (arrow) in the left lower lobe suggestive of lung cancer.
Contrast enhanced computed tomography of thorax showing multiple conglomerated, heterogeneously enhancing mediastinal lymph nodes (arrow).
Fine‐needle aspiration cytology of the right inguinal lymph node was suggestive of lymph node metastasis (Figure 5). Together, these findings were suggestive of stage IV metastatic lung carcinoma initially presenting as acute pancreatitis.
Fine‐needle aspiration cytology of the inguinal lymph node showing atypical cells with large nucleus–cytoplasm ratio, irregular nuclei, vesicular‐to‐clumped chromatin, one to two nucleoli, and scanty cytoplasm, suggestive of lymph node metastasis (arrows). Pap stain, 40x magnification.
A histopathological diagnosis is mandatory if the clinicoradiological suspicion of malignancy is high. However, the patient’s family refused further investigation and management, and the patient was referred to palliative care.
3. Discussion
The two most common etiologies of acute pancreatitis are gallstones and alcohol consumption; however, hypercalcemia is a rare cause of acute pancreatitis. Acute pancreatitis is usually associated with low serum calcium levels; therefore, hypercalcemia may arise due to hyperparathyroidism or malignancy. Hypercalcemia causes pancreatic injury via secretory blockage, accumulation of secretory proteins, or activation of proteases. The cause of hypercalcemia should be accordingly managed along with the administration of intravenous fluids, ideal fluid of choice is 0.9% normal saline, initial 1–2 L of bolus followed by a maintenance rate of 200–500 mL/h according to patient’s cardiac and renal status, loop diuretics ideally furosemide (40–80 mg every 6–12 h), and bisphosphonates preferably zoledronic acid 4 mg IV over 15 min and routine management of pancreatitis and its complications. One possible cause of pancreatitis in our patient was hypercalcemia, which may be associated with a paraneoplastic syndrome of lung malignancy or metastasis [2–11]. NSCLC and small cell lung cancer account for 85%–90% and 10%–15% of lung cancers, respectively [12]. The most common extrapulmonary sites of distant metastases of lung cancer are the brain, bones, liver, and adrenal glands [13]. Approximately 20%–50% of patients with NSCLC present with metastatic disease. The prognosis of stage IV NSCLC is poor, with a median overall survival time of 7–11 months [14]. Previous autopsy studies have reported a 1.6%–5.9% incidence of metastasis to the pancreas from lung carcinoma [15]. Metastasis‐induced pancreatitis is caused by the obstruction of the pancreatic duct by metastatic deposits or pancreatic compression by the enlarged regional lymph nodes, which can cause autolysis via pancreatic enzyme activation. Vascular compromise due to the invasion of metastatic neoplastic cells is another suggested mechanism for acute pancreatitis [16]. Some case reports have described hypercalcemia as a causative mechanism for acute pancreatitis in patients with NSCLC [17–19]. On the contrary, in some cases of small cell lung cancer with acute pancreatitis, where no common causes of pancreatitis were identified, autopsy showing no evidence of pancreatic metastasis suggested paraneoplastic syndrome as a possible cause [20]. In our case, contrast‐enhanced CT of the abdomen revealed no pancreatic metastases. Gallstone‐induced pancreatitis was also a differential diagnosis because the patient had cholelithiasis. However, there was only one large stone in the gallbladder, the CBD diameter was within normal limits, there were no stones in the CBD or main pancreatic duct, and hypertriglyceridemia was ruled out. Therefore, paraneoplastic syndrome due to lung malignancy with hypercalcemia was thought to be the cause of the acute pancreatitis, which was the first and only manifestation of an underlying lung carcinoma. This is an infrequent presentation of lung carcinoma. There are very few case reports in the literature describing lung cancer presenting as acute pancreatitis due to hypercalcemia; among these, hypercalcemia was the initial and sole manifestation of lung cancer, with an often‐unknown underlying cause. Such presentations, typically, occur in the advanced stages of the malignancy [17–19]. Possible reasons for paraneoplastic hypercalcemia in lung carcinoma are the secretion of parathyroid hormone‐related protein [PTHrP] or osteolytic activity due to cytokine production, which stimulates osteoclasts and has a poor survival outcome [20, 21]. Chemotherapy is the first‐line of treatment for patients with stage IV NSCLC [14]. The NCCN Clinical Practice Guidelines recommend immunotherapy for locally advanced and metastatic lung cancer. Patients with stage III NSCLC treated with durvalumab (anti‐PD‐L1 monoclonal antibody) for upto 12 months did not progress after definitive chemoradiation therapy. Patients with NSCLC progressing with, or after, first‐line chemotherapy can be switched to nivolumab immunotherapy [22].
4. Conclusion
Paraneoplastic hypercalcemia due to carcinoma of the lung can present with acute pancreatitis and is usually present in the advanced stages of malignancy with poor outcomes. In the absence of common causes of pancreatitis, hypercalcemia should be appropriately investigated. Early diagnosis and management can increase the survival rates.
Funding
This study did not receive any funding.
Ethics Statement
This study was compliant to ethical requirement. Ethics clearance taken from the Institutional ethics committee with letter number AIIMS/IEC/24/127 dated March 15, 2024, from the All India Institute of Medical Sciences, Rishikesh.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Identifying details have been anonymized. Patient consented to this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khan M. A. , Luni F. K. , and Kamal S. , et al.Acute Pancreatitis: First and Sole Manifestation of Small Cell Carcinoma of Lung, Journal of Medical Cases. (2014) 5, no. 10, 525–528, 10.14740/jmc 1896 w. · doi ↗
- 2Schmitt J. K. , Pancreatitis and Diabetes Mellitus With Metastatic Pulmonary Oat-Cell Carcinoma, Annals of Internal Medicine. (1985) 103, no. 4, 638–639, 10.7326/0003-4819-103-4-638_2.2994535 · doi ↗ · pubmed ↗
- 3Hall M. , Bundred N. J. , and Hall A. W. , Oat Cell Carcinoma of the Bronchus and Acute Pancreatitis, European Journal of Surgical Oncology. (1987) 13, no. 4, 371–372.3040475 · pubmed ↗
- 4Noseda A. , Gangji D. , and Cremer M. , Acute Pancreatitis as Presenting Symptom and Sole Manifestation of Small Cell Lung Carcinoma, Digestive Diseases and Sciences. (1987) 32, no. 3, 327–331, 10.1007/BF 01297062, 2-s 2.0-0023113897.3028735 · doi ↗ · pubmed ↗
- 5Evans A. T. , Necrotising Pancreatitis and Diabetes Associated With Disseminated Small Cell Carcinoma of Lung, Scottish Medical Journal. (1988) 33, no. 6, 10.1177/003693308803300612, 2-s 2.0-0024270958, 377.2854301 · doi ↗ · pubmed ↗
- 6Chowhan N. M. and Madajewicz S. , Management of Metastases-Induced Acute Pancreatitis in Small Cell Carcinoma of the Lung, Cancer. (1990) 65, no. 6, 1445–1448.2155057 10.1002/1097-0142(19900315)65:6<1445::aid-cncr 2820650632>3.0.co;2-f · doi ↗ · pubmed ↗
- 7Maclennan A. C. and Macleod I. A. , Case Report: Small Cell Carcinoma Induced Acute Pancreatitis, The British Journal of Radiology. (1993) 66, no. 782, 161–162, 10.1259/0007-1285-66-782-161, 2-s 2.0-0027465407.8384507 · doi ↗ · pubmed ↗
- 8Huang Y. W. , Yang J. C. , Chang Y. L. , Tsang Y. M. , and Wang T. H. , Acute Pancreatitis Combined With Acute Budd-Chiari Syndrome as the Initial Manifestation of Small Cell Lung Cancer, Journal of the Formosan Medical Association. (2005) 104, no. 6, 431–435.16037834 · pubmed ↗