Paraneoplastic cerebellar degeneration from an isolated nodal clear cell carcinoma of suspected gynecologic origin: case report and literature review
Claire Rose Kissinger, Aashima Gupta, Mina Aiad, Zachary Rothkopf, Melissa Wilson

TL;DR
A rare case of paraneoplastic cerebellar degeneration linked to an undetected gynecologic cancer is reported, emphasizing the need for thorough evaluation in similar cases.
Contribution
This case highlights the rare occurrence of anti-Yo PCD associated with an isolated nodal gynecologic malignancy without a primary tumor.
Findings
Anti-Yo antibodies were detected in serum and CSF, indicating a paraneoplastic process.
FDG-PET/CT identified pelvic lymph node metastasis from a suspected gynecologic origin.
The patient showed partial improvement with immunotherapy and chemotherapy but remains non-ambulatory.
Abstract
Paraneoplastic cerebellar degeneration (PCD) is a rare neurologic syndrome that often presents before an underlying malignancy is diagnosed. Patients typically develop subacute cerebellar symptoms—such as vertigo, dysmetria, disconjugate gaze, and dysarthria—before any tumor is detected. Establishing the diagnosis involves ruling out metastatic disease, treatment toxicity, infection, and metabolic disturbances, and often hinges on finding antineuronal antibodies (most commonly anti-Yo, also called type-1 anti-Purkinje cell antibody or PCA-1) in blood or cerebrospinal fluid (CSF). Anti-Yo positivity is classically linked to breast or gynecologic cancers and carries a poor prognosis. We describe a 56-year-old woman with a remote history of parotid basal cell adenocarcinoma who developed gradually worsening cerebellar dysfunction over several months, despite negative initial imaging and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
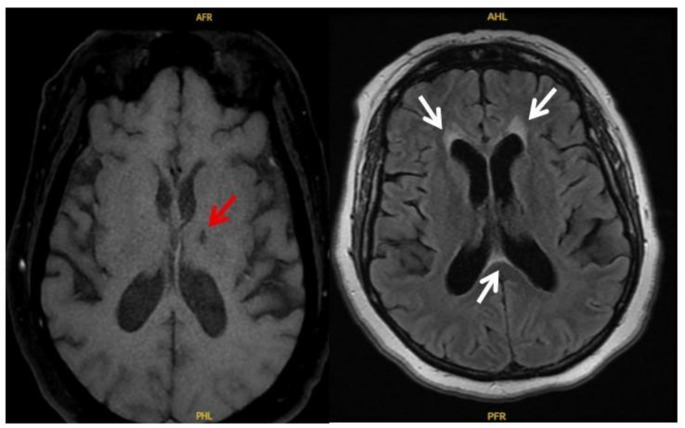 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Neurological Disorders and Treatments · Genetic Neurodegenerative Diseases · Brain Metastases and Treatment
Introduction
Paraneoplastic cerebellar degeneration (PCD) is an immune-mediated disorder in which autoantibodies target cerebellar Purkinje cells in the context of malignancy. Most often, it presents in women with breast or gynecologic cancers and may precede tumor detection by weeks or even months (Cao et al. 1999). Clinically, PCD typically manifests as subacute vertigo, nystagmus, gait instability, and dysarthria. Because these symptoms are nonspecific, they can mimic more common conditions, and brain imaging may be normal early on, a prompt diagnosis of PCD can be challenging (Leypoldt and Wandinger 2014). Detecting antineuronal antibodies, particularly anti-Yo (PCA-1), can confirm the suspected PCD diagnosis and guide the workup to undercover an underlying malignancy. Treatment must address both the malignancy and the autoimmune process, frequently combining immunosuppression, plasma exchange, and chemotherapy or surgery (Frings et al. 2005). Although most patients tend to stabilize rather than improve despite intensive treatment, those who show meaningful recovery often received earlier intervention—emphasizing the critical role of timely recognition and treatment.
Case presentation
A 56-year-old woman with a history of pT4aN0 basal cell adenocarcinoma arising from a pleomorphic adenoma of the left parotid gland (treated 7 months prior to presentation with surgical resection and adjuvant chemoradiation) first reported acute-onset vertigo. Over the following few weeks, she presented multiple times to the emergency department. Her neurologic examinations remained non-focal, brain MRI showed only chronic microvascular changes and a stable old thalamic lacunar infarct (Fig. 1), and she was discharged with symptomatic measures (meclizine, and scopolamine).Fig. 1MRI Brain (Axial T2/FLAIR) demonstrating an old left thalamic lacunar infarct (red arrow) and small scattered periventricular white matter hyperintensities consistent with chronic microvascular changes (white arrows)
One month after the time of presentation, she returned with persistent vertigo, nausea, and vomiting; evaluation revealed hypokalemia, which was corrected, and she was again discharged. However, later that same week, she developed bilateral lower extremity weakness and was admitted. Laboratory studies showed erythrocytosis (hemoglobin 18.3 g/dL, hematocrit 52.8% (reference: hemoglobin 12.0–16.0 g/dL, hematocrit 36–46% in females) and mild hyperbilirubinemia (total bilirubin 1.5 mg/dL (reference: 0.3–1.2 mg/dL); molecular testing for JAK2 V617F, CALR exon 9, and MPL exons 10–12 was negative. Otolaryngology noted left-sided hearing loss and nystagmus on Dix-Hallpike testing. CTA of the head and neck and repeat brain MRI ruled out local parotid adenocarcinoma recurrence. Hematology/oncology evaluation was unremarkable, and she underwent phlebotomy for presumed polycythemia. She was discharged with plans for outpatient neurology follow up and vestibular rehabilitation.
Three months after initial presentation, her cerebellar signs had progressed: she exhibited dysmetria, multidirectional nystagmus, and dysarthria. Concern for a paraneoplastic process prompted serum testing for autoimmune/paraneoplastic antibodies (Mayo Clinic MDS2 panel), which was initially negative. Given ongoing suspicion, an expanded paraneoplastic antibody panel (including CSF) was ordered. This revealed high-titer Purkinje cell cytoplasmic antibody type 1 (anti-Yo) in serum (1:3, 840) and CSF (1:64), strongly suggesting paraneoplastic cerebellar degeneration.
The patient subsequently received five sessions of plasma exchange (PLEX), five daily doses of IVIG at 400 mg/kg, and four days of high-dose IV methylprednisolone (1000 mg daily), with partial improvement in speech and upper-limb coordination.
To identify the occult malignancy, contrast-enhanced CT of the chest, abdomen, and pelvis five months after initial presentation revealed a 1.3 cm spiculated pulmonary nodule in the left upper lobe, a 1.3 cm left adrenal nodule, sclerotic lesions in the thoracolumbar spine, and endometrial thickening. Biopsies of the lung and adrenal lesions were benign. A nuclear medicine bone scan showed no osseous metastases. Endometrial curettage demonstrated benign inactive endometrium with focal non-atypical hyperplasia, without malignancy.
Seven months after initial presentation, the patient remained symptomatic with encephalopathy, dysarthria, nystagmus, and ataxia, but still no identifiable primary. An FDG-PET/CT scan then demonstrated FDG-avid lymphadenopathy along both iliac chains, enlarged compared to imaging two months earlier. Gynecologic oncology evaluation included pelvic washings, which revealed atypical cells positive for BerEp4 and pan-keratin (AE1/AE3) but negative for Napsin, P504S, WT-1, calretinin, and CK5/6 with background CD68-positive histiocytes—findings suspicious of malignancy.
Given these findings and her positive anti-Yo antibody status, surgical exploration was recommended. Because anti-Yo is strongly associated with gynecologic malignancy, and the location of the lymphadenopathy was not retroperitoneal or para-aortic, gynecologic oncology was favored over renal or urogenital.She underwent robotic total laparoscopic hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymphadenectomy. Grossly, the uterus, cervix, and adnexa appeared normal. Pathology confirmed that uterine, ovarian, and fallopian tube tissues were benign. Of the pelvic lymph nodes, three left external iliac nodes were negative, but one right and one left common iliac node each harbored large metastatic deposits of clear cell carcinoma. Immunohistochemistry showed the tumor cells were positive for pancytokeratin (AE1/AE3), PAX8, CK7, P504S/Racemase, and Napsin A, and negative for CK20, p40, S100, inhibin, RCC marker, CD10, carbonic anhydrase IX, OCT3/4, and estrogen receptor; p53 expression was wild type. These findings, combined with anti-Yo positivity, pointed to a gynecologic origin despite no primary lesion in the uterus or ovaries.
Postoperatively, she received five days oral methylprednisolone course for neurological symptoms and then treated with adjuvant carboplatin (AUC 5) and paclitaxel (135 mg/m^2^), total of five cycles. Unfortunately, treatment was complicated by grade 4 neutropenia, pleural empyema, and pericardial effusion requiring drainage about ten months after initial presentation.
Approximately one year after initial presentation (approximately six months after surgery), she demonstrated modest improvements in upper-limb coordination and speech but remained non-ambulatory with bilateral lower extremity paralysis, persistent dysarthria, and mild cognitive impairment that limited decision-making.
At recent follow-up visits, three years after initial presentation, she remains alive without evidence of recurrent carcinoma but continues to require supportive care, physical therapy, and intermittent steroid use only if her neurologic symptoms worsen.
Discussion
We reviewed 40 reported cases of anti-Yo-positive PCD, including our case (Tables 1, 2 and 3). The average age at diagnosis was 59.1 years (median 59.5; range 31–84), with a strong female predominance—37 patients (92.5%) were female and only 3 (7.5%) were male.Table 1. Summary of paraneoplastic anti–Yo-positive PCD cases with primary malignancies identifiedReferenceAge/ SexCancer diagnosis (stage)PCD onset before/after cancer diagnosisSerum Anti-YoCSF Anti-YoBrain ImagingCancer treatmentPCD treatmentPCD symptoms at presentationDuration of PCD symptoms before presentationOutcome of PCD treatment & SurvivalSurvival after PCD diagnosis Aparna et al. (2024)68 FHigh-grade serous ovarian carcinoma (clinically IIIC) PCD ~ 4 months before cancer diagnosis + Not Reported (NR)CT head: frontal & cerebellar atrophy in keeping with PNS, not age relatedDebulking surgery + carboplatin/paclitaxel chemoIVIG 1 g/kg with 1 g IV MP x total 5 dosesProgressive ataxia, dysarthria, falls, instability ~ 4 monthsSlight improvement of speech and coordination, then cerebellar symptoms gradually worsenedAlive at 2 yearsBaransi et al. (2022)52 Fhigh-grade serous ovarian carcinoma; FIGO IIIB PCD ~ 2 mo before cancer Dx + NRBrain MRI: normalDebulking surgery + adj Carbo/Taxol × 6, then niraparib 200 mg QD × 36 MoIV MP 1 g × 5 days, Cyclophosphamide 750 mg/m^2^ IV every 4–6 weeksGait ataxia, dysphagia, hand weakness & weight loss ~ 1 monthsslight improvement in speech & swallowing, but her gait ataxia & limb incoordination persisted ≥ 3 yearsBhargava et al. (2014)44 FBorderline serous papillary ovarian carcinoma (FIGO IIA) PCD ~ 8 months before tumor found + Negative (-)Brain MRI: Bilateral cerebellar atrophyAHBSOIV MP 1 g QD × 5 days, then IVIG course 2 g/kg over 5 daysVertigo, nausea, vomiting; dysarthria, ataxia, nystagmus8 monthsTwo weeks after AHBSO: marked improvement in dysarthria &vertigoBy 1 month: ambulate with supportBy 2 Mo: only minimal residual ataxia & ocular findings; independent in ADLsAlive &functionally independent at ~ 10 monthsBradley et al. (2008)56 FSerous ovarian carcinoma (III C) PCD ~ 2.5 years after cancer Dx + NRBrain MRI: normaldebulking surgery + Carbo/Taxol then more chemo for recurrencePLEX, IVIG, corticosteroids, & Tacrolimus (dose: NR)Difficulty walking, ataxia, dysarthria ~ 1 weekNo neurological improvementAlive at 24 monthsCao et al. (1999)65 FPoorly differentiated serous adenocarcinoma of the right ovary, FIGO IIIC PCD ~ 1 month before cancer Dx + NRBrain MRI: normalDebulking surgery onlyNone – no PLEX, IVIG, or steroidsDysarthria, gait ataxia, dysphagia, diplopia3–4 weeksNo improvement remained in bedriddenAlive at 6 monthsĆerimagić and Džananović (2020)61 FHER2 positive invasive breast carcinoma, Stage IIA PCD ~ 6 months before cancer diagnosis + NRInitial MRI normal; follow-up at 3 months: 5 mm cerebellar lesion (ischemic vs. PCDNeo chemo + HP, mastectomy, XRT & trastuzumab × 2 cyclesPLEX × 5, IV cyclophosphamide 1 g, azathioprine, IVIG 2 g/kg × 1 then 0.4 g/kx 13Sudden onset vertigo, nystagmus & nausea ~ 10 monthsMild improvement in limb coordination after PLEX but remained wheelchair-bound with persistent ataxia & dysarthriaAlive at ~ 2–3 yearsChatham and Niravath (2021)—Case 1 57 FHER2 positive invasive ductal carcinoma of breast, stage IIIA PCD ~ 6 months before cancer Dx + + Brain MRI: normalLeft mastectomy + trastuzumab plus pertuzumab × 17 cyclesIV MP + IVIG, PLEX × 2, & Rituximab over 7 Mo (dose: NR)Progressive ataxia and dysarthria ~ 3 monthsNo significant improvement – PCD stabilized with severe deficits (wheelchair-bound, dysarthria persists)Alive at 39 monthsChatham and Niravath (2021)—Case 261 FHER2 positive breast carcinoma PCD ~ 3 months before cancer Dx + NRBrain MRI: normalLeft mastectomy + trastuzumab plus pertuzumab × 17 cyclesPLEX over 7 Mo then Rituximab over 10 Mo (no doses, steroid or IVIG were reported)Vertigo, nausea, vomiting & ataxia ~ 3 monthsMinimal improvement – remains wheelchair-bound (able to take only a few assisted steps), with persistent dysarthria and poor coordinationAlive at 36 monthsCui et al. (2017)65 FSerous ovarian carcinoma (Stage III) PCD 1 year after cancer diagnosis + NRBrain MRI: normalCytoreductive surgery + adj cisplatin/paclitaxel × 7IVIG 1 g × 7 days + IV MP 0.4 g/kg/day × 5 daysRapidly progressive ataxia, vertigo & dysarthria ~ 5 monthsVertical nystagmus resolved, speech improved, & regained ability to sit/stand (with supervision) & to mobilize in bed ≥ 19 monthsDeac et al. (2021)59 FHigh grade serous ovarian carcinoma (Stage IV) ~ 4 months before cancer Dx + NRBrain MRI: cerebellar atrophy, enlargement of 4th ventricle, scattered T2-signal abnormalities in the frontal lobespaclitaxel–carboplatin x total of 6 cyclesIVIG 2 g/kg over 5 days + corticosteroid (dose: NR)Vertigo, imbalance, bilateral plantar paresthesia, hedahche, insomnia, sad mood, & weight loss ~ 4 monthsonly a slight transient improvement of diplopia & vomiting—but cerebellar dysfunction progressed ~ 7 monthsElomrani et al. (2014)80 FPoorly differentiated ovarian adenocarcinomaPCD and cancer diagnosed concurrently + NRBrain MRI: normalNo resection; received Carboplatin + paclitaxel (dose NR)Corticosteroids were given along with antiemetic with the chemo (Dose: NR)subacute vertigo, vomiting, spontaneous nystagmus and clinical ataxia (on exam)described as “subacute”Complete disappearance of the cerebellar syndrome after the first chemo cycle; however, following the second cycle the ataxia recurred with marked deterioration in general condition ~ 1 monthsFrings et al. (2005)– case 1 59 FAdenocarcinoma of the left fallopian tube, at least FIGO Stage IIB Several weeks + + Initial brain MRI: normalFollow-up MRI: marked cerebellar atrophy, sparing the brain stemCombined ovariectomy + adnexectomy, but no chemo was givenIV MP & Mitoxantrone (dose: NR)Nystagmus, dysarthria, and severe ataxiaWeeks to monthsNo clinical improvement; remained severely ataxic and bedriddenNRFrings et al. (2005)–case 257 FInvasive lobular breast cancer, ER/PR negative, HER2 positive, ≥ IIIB Few weeks + + Brain MRI: advanced cerebellar atrophy without brain-stem involvementNo resection or XRT; received 5-fluorouracil + epirubicin + cyclophosphamide (FEC regimen)anti-cancer chemo onlyNystagmus, dysarthria, and severe ataxiaWeeks to monthsNo clinical improvementNRGiucca et al. (2023) ~ 65 FHigh-grade serous ovarian adenocarcinoma, FIGO stage IV PCD ~ 16 months after cancer dx + NRBrain MRI: normalcarboplatin + paclitaxel, interval debulking surgery, Bevacizumab added at cycle 6 then as maintenancePLEX with IV MP 1 g/day × 5 &double vision, dizziness, nausea, headache, and poor coordination ~ 9 daysCerebellar syndrome continued to worsen despite treatment ~ 2 monthsHasadsri et al. (2013)49 MLarge cell, poorly differentiated adenocarcinoma of the lung, Stage IA1 found at autopsy ~ 8 weeks between PCD onset and postmortem cancer diagnosis on autopsyNR + Brain MRI: mild generalized cerebral and cerebellar atrophyNo oncologic therapy (cancer found post-mortem)IV MP (dose: NR)Vertigo, gait ataxia, slurred speech; falls and vomiting ~ 2 weeksInitial improvement but later worsened, progressive ataxia, became bedridden; fatal outcomeHasadsri et al. (2013)Imai et al. (2022)60 FLeft submandibular gland salivary duct carcinoma PCD onset led to workup revealing the cancer (5 days apart) + NRBrain MRI: normalTumor resection (submandibular glandectomy + neck dissection); no adjuvant therapy notedIV MP 1 g/d × 3, PLEX × 10, IVIG × 5 days, cyclophosphamide (dose: NR)Acute gait ataxia, limb and trunk dysmetria, truncal instability ~ 5 daysPartial improvement with Nausea, vertigo and nystagmus after tumor resection but persistent ataxiaNot Reported (alive at report, persistent PCD)İlhan et al. (2021)54 FOvarian cancer, recurrent after initial remission PCD ~ 3 years after cancer remission, and ~ 6 month before recurrence dx + + Brain MRI: normalCytoreductive surgery at initial diagnosis; after recurrence, received ed carboplatin + paclitaxel × 6 cyclesTingling & unsteadiness while walking, ataxia, dysarthriaPLEX × 5, each performed 2 days prior to the chemo ~ 6 monthsSignificant improvement in walking and balance noted by the start of cycle 2 of chemotherapyNRKato et al. (2017)42 FLeft breast microinvasive ductal carcinoma, ER/PR negative, HER2 positive, stage IA PCD ~ 2 months before cancer dx + + Initial Brain MRI: normal; 4-months post-surgery: cerebellar atrophyLeft mastectomy (no adjuvant therapy)IVIG, steroids, and PLEX (does/ number of treatments: NR)Dizziness, dysarthria, ataxia, slightly impaired orientation ~ 2 monthsInitially improved, then relapsed – residual ataxia despite immunotherapy ≥ 1 yearLe May and Dent (2018)53 Finvasive ductal carcinoma of the left breast, ER/PR negative, HER2 positive, stage IIBPCD ~ 4 months before cancer dx + NRBrain MRI: normalMastectomy, adjuvant Doxorubicin–cyclophosphamide × 4, Paclitaxel weekly × 12 cycles with trastuzumabIVIG × 2 doses & Physiotherapyataxia, dysarthria, emotional lability, diplopia & fine motor weakness ~ 4 monthsNo meaningful improvement after IVIG or chemotherapy; PCD deficits stabilized but persisted, with eventual wheelchair dependence and long-term care placement ≥ 9 monthsLiapi and Sarivalasis (2020)61 FHigh-grade serous ovarian cancer (FIGO IIIC) PCD at presentation – preceded cancer diagnosis + NRBrain MRI: diffuse cerebellar atrophy, predominant in vermiscarboplatin/ paclitaxel & maintenance Bevacizumab × 15 monthAnti-cancer chemogait ataxia, dysphonia, dysarthria, dysmetriaNRTransient improvement of ataxia during chemo ≥ 7 yearsLie et al. (2016)84 FHigh-grade serous endometrial adenocarcinoma (recurrence with LN metastasis) PCD onset ~ 1 year after initial cancer, and ~ 6 months before the recurrence dx + NRBrain MRI: normalAHBSO at initial cancer diagnosisHigh dose steroid (dose: NR)gait ataxia, dysarthria, tremors, nystagmus6 months history of fallsNO improvement; severe functional declineNRMartin et al. (2017)52 FBreast infiltrating ductal carcinoma (stage IIIA, HER2 positive) Breast cancer was uncovered on chest CT performed at her initial PCD presentation + NRBrain MRI: chronic microvascular changesNeo docetaxel + carboplatin + HP, mastectomy, adj XRT, adj HP. Later lapatinib + capecitabine; ado-trastuzumab (for recurrence)IVIG 2 g/kg total, given over 3 days, then maintenance monthlySubacute ataxia, dysarthria, diplopia, dysphagia, nystagmus; episodes of uncontrolled crying (pseudobulbar affect) ~ 1 monthTransient—but significant improvement in ataxia and pseudobulbar affect, slight dysarthria improvement, but later, she retained severe truncal and limb ataxia ≥ 3 yearsMirallas et al. (2020)44 FMultifocal invasive breast ductal carcinoma, HER2 positive, stage IA PCD ~ 5 months after breast cancer dx + + Brain MRI: normalNeo Doxorubicin + Cyclophosphamide × 4 – paclitaxel/HP × 11, mastectomy, adj trastuzumab/tamoxifenIVIG course over 5 daysGait instability, right upper extremity weakness, mild paresthesia × 4 extremities, discrete right diadochokinesia ~ 5 weekssignificant improvement, autonomous gait restored, able to sit/stand unaided but had persistent right-sided asymmetry and mild balance disorder ≥ 1 yearOthman et al. (2020)48 FSerous carcinoma arising from fallopian tube/peritoneum ~ 2 weeks before cancer dx + NRBrain MRI: normal1 cycle carboplatin alone; then 5 cycles carboplatin + paclitaxelAnti-cancer chemoFalls, ataxia, dysarthria, hyperreflexia, limb dysmetria ~ 2 weeksMild improvement: at 18 months follow-up able to move extremities and transfer with assistance ≥ 18 monthsRenjen et al. (2018)65 FHigh-grade serous ovarian carcinoma (FIGO IIIA1) PCD ~ 2 months before cancer dx + NRBrain MRI: diffuse cerebellar folial enhancement &mild atrophyDebulking surgery + adj carboplatin/paclitaxelIVIG × 5 daysSubacute‐onset imbalance/ataxia & sudden throbbing headaches ~ 2 monthsPartially regained ambulation but remained ataxic ≥ 6 monthsRusso et al. (2013)64 FHigh grade serous papillary ovarian cancer (FIGO IIIC) PCD 1 year after cancer diagnosis + + Brain MRI: normalReduction surgery + adj Carboplatin/Paclitaxel × 6 cyclesIVIG 400 mg/kg daily × 7 + corticosteroids + Cyclophosphamide 800 mg/m^2^/monthSubacute dysmetria, ataxia, dysgraphia, nystagmus, diplopia & mild dysphagia ~ 2 monthsStabilization only; no significant improvement; remained severely disabled ≥ 12 monthsTanaka et al. (1992)47 FFallopian tube adenocarcinoma, FIGO IA PCD ~ 3 months before cancer dx + + Brain MRI: small old cerebellar infarct, otherwise unremarkableTumor resection via test laparotomy + adj FCAP (cisplatin, Adriamycin, cyclophosphamide, 5-FU) × 3 cyclesAnti-cancer treatment onlyAcute diplopia, ataxia, vertigo, nausea, vomiting, ataxia, & upper limbs hyperreflexia ~ 3 months subacuteregained ability to sit unaided, improved speech; autoantibody titers fell ≥ 1 yearWang et al. (2022)51 FInvasive ductal breast adenocarcinoma, ER/PR negative, HER2 positive, stage IIIC PCD ~ 33 days before cancer dx + + Brain MRI: normalMastectomy + adj paclitaxel, carboplatin, HP × 2 cycles onlyIVIG 5 days (40 g Day 1, 25 g × 4) + high-dose IV MP then taper to oral prednisoneUnsteady gait, dizziness, dysarthria (explosive speech), vertigo; rapidly progressive cerebellar ataxia with pyramidal signs ~ 6 weeksNeurologic decline halted shortly after immunotherapy; at 1-year follow-up: no cancer recurrence, neurologic symptoms stable (persistent ataxia/dysarthria without further deterioration) ≥ 1 yearWesterlinck et al. (2022)31 FInvasive ductal breast carcinoma, triple positive, clinical stage IIB PCD ~ 1.5 months before cancer dx + NRBrain MRI: initially normal; repeat showed bilateral cerebellar T2 FLAIR hyperintensity without contrast enhancementNeo EC (epirubicin/ cyclophosphamide), mastectomy, adj EC × 2, then paclitaxel + HP × 13 cycles + XRTIVIG 400 mg/kg/day × 5, High-dose corticosteroids, Natalizumab monthly × 6 & Whole-brain RTheadache, dizziness, ataxia, dysmetria, nystagmus, diplopia, dysarthria / expressive aphasia ~ 1 monthRapid stabilization after whole-brain RT + tumor resection; over months: clear speech, improved motor skills & continued neurological recovery ≥ 33 monthsXia et al. (2003)55 MInvasive adenocarcinoma of distal esophagus, stage IIIB PCD ~ 6 weeks before cancer dx + + Brain MRI: large cisterna magna noted, otherwise unremarkableCisplatin + Irinotecan, palliative XRT, then esophagectomyEmpiric immunosuppressants (unspecified), IVIG and PLEX (unspecified)Progressive ataxia, dizziness, dysarthria, nystagmus, dysmetria of all extremities & weight loss ~ 6 weeksNo neurologic improvement; became wheelchair-bound & mute postoperatively ≥ 6 monthsYan et al. (2018)67 FInvasive ductal breast carcinoma, ER/PR negative, HER2 positive, stage IIA PCD ~ 6 months before cancer dx + NRBrain MRI: normalLeft breast lumpectomy; no adj therapyIVIG (unspecified)Dizziness, dysarthria, nausea, vomiting, diplopia& psych symptoms ~ 6 monthsMarked neurologic improvement after lumpectomy; at 12-month follow-up: resolution of ataxia, dysarthria, and gait instability ≥ 12 monthsYang et al. (2025)62 FSquamous cell lung carcinoma; stage IIIB PCD ~ 3 weeks before cancer dx + NRBrain MRI: normalCisplatin/etoposide × 3 + Concurrent thoracic radiotherapyIVIG 0.4 g/kg/d × 5 + IV MP 80 mg/day × 7 then po prednisone taper + Mycophenolate mofetilVertigo, nausea, vomiting, ataxia, nystagmus and diplopia ~ 3 weeksSignificant improvement of nausea, vomiting & vertigo; gained independent ambulation without gait support ≥ 6 monthsYasuda et al. (2024)77 FPeritoneal serous papillary carcinoma, FIGO IIB PCD ~ 5 months before cancer dx + NRBilateral cerebellar atrophy on MRI (with cerebellar hypoperfusion on SPECT)THBSO + adj paclitaxel/ carboplatin × 6 cyclesMonthly IVIG (0.4 g/kg/day × 5 days) concurrent with chemotherapy (6 courses)subacute dysarthria with scanning speech, Neck tremor, severe limb dysmetria & ataxia ~ 5 monthsDysarthria began improving after 3rd IVIG course but had Persistent limb ataxia & wheelchair dependence ≥ 6 monthsZhuang et al. (2024)57 FRemote history of breast cancer ER/PR negative HER2 positive s/p resection PCD occurred later, after cancer treatment (period: NR) + + Brain MRI: leptomeningeal enhancement prominently involving both cerebellar hemispheresNo active oncologic therapy reported (no recurrence or metastasis identified)PLEX + IV MP (dose: NR)Gait unsteadiness, receptive aphasia, insomnia, cerebellar ataxia with nystagmus and diplopia ~ 12 daysNo significant neurologic improvementPatient died during follow-up (exact period: NR)ADLs activities of daily living, AH-BSO Abdominal hysterectomy with bilateral salpingo-oophorectomy, Adj adjuvant, BID twice daily, Dx diagnosis, F female, HP trastuzumab-pertuzumab, IV intravenous, IVIG intravenous immunoglobulin, LN lymph node, M male, MP methylprednisolone, Mo months, NR not reported, Neo neoadjuvant, PCD paraneoplastic cerebellar degeneration, PNS paraneoplastic neurological syndrome, PO oral, QD once daily, SPECT Single-Photon Emission Computed Tomography, XRT radiation therapyTable 2Summary of paraneoplastic anti–Yo-positive PCD cases with no malignancy identified / occult malignancyReferencesAge/ SexPresumed occult malignancy (no tumor identified)Serum Anti-YoCSF Anti-YoBrain ImagingCancer treatmentPCD treatmentPCD symptoms at presentationDuration of PCD symptoms before presentationOutcome of PCD treatment & SurvivalSurvival after PCD diagnosisHu et al. (2020)64 MWorkup included Whole-body PET/CT, CT chest/abdomen/pelvis, targeted endoscopic biopsies (e.g., ileal ulcer) all negative + − MRI: normalNoneDexamethasone 10 mg QD × 10 days; Plasma exchange (4 courses); Prednisone 10 mg QD × 3 monthsProgressive ataxia, gait instability, dysuria, blurred vision, diplopia, blepharoptosis ~ 5 daysMarked improvement: independent ambulation; anti-Yo became undetectable; symptoms relieved at 6 months ≥ 6 monthsDou et al. (2024)63 FAn ultrasound examination revealed lymphadenopathy and left side breast nodules, but PET/CT did not identify any tumors + − MRI: initially normal; 5 months later cerebellar atrophyNot applicable (no tumor identified)IVIG 0.4 g/kg × 5 days; IV methylprednisolone 500 mg × 10 days; Ofatumumab 20 mg × 2 injectionsDizziness, vomiting, nystagmus, dysarthria, progressive ataxia ~ 1 monthPartial improvement: walker-dependent but able to stand; further symptomatic relief after second OFA dose ≥ 11 monthsTable 3Summary of paraneoplastic anti–Yo-positive PCD cases with isolated lymphadenopathy/ lymph node metastasesReferencesAge/ SexCancer diagnosis (stage)PCD onset before/after cancer diagnosisSerum Anti-YoCSF Anti-YoBrain ImagingCancer treatmentPCD treatmentPCD symptoms at presentationDuration of PCD symptoms before presentationOutcome of PCD treatment & SurvivalSurvival after PCD diagnosisAbdulaziz et al. (2018)68 FBiopsy of right axillary lymp nodes showed Poorly differentiated metastatic cancer cells but no primary foundPCD Dx led to finding LN cancer cells in LNPositive ( +) + Brain MRI: normalNoneIV methylprednisolone (MP) 500 mg × 5 days, then PO prednisone 60 mg QD × 3 MoVertigo, diplopia, nystagmus, severe ataxia ~ 6 monthsImproved: walking independently at 1 yearAlive at 1 yearChatham and Niravath (2021)—Case 379 FPara aortic lymphadenopathy on image (3 cm),, presumed ovarian cancer Presumed metastatic ovarian cancer but patient declined biopsyPCD ~ 4 months before cancer suspicion + NRNRRadiation therapy to the para-aortic/aortocaval LNPLEX + Steroid, then IVIG (dose: NR)Ataxia, blurry vision & fatigue ~ 4 monthsRapid neurologic deterioration – became completely unable to walk or speak by ~ 8 monthsNRLou et al. (2021)61 FBiopsy of retroperitoneal lymphnodes showed adenocarcinoma of pancreaticobiliary origin, no primary foundPCD onset ~ 10 days before cancer dx + + Brain MRI: normalAnlotinibIVIG 0.4 g/kg/day × 5, IV MP 160 mg/day × 3, then 80 mg/day × 3, then 40 mg/day × 7vertigo, nausea/vomiting, nystagmus & ataxia ~ 10 daysInitial transient symptoms improvement then remained bedridden ≥ 16 monthsOur case56 FIsolated clear cell carcinoma in two pelvic lymph nodes; presumed ovarian origin; primary not identifiedPCD onset ~ 7 months before cancer dx + + Brain MRI: chronic microvascular changes and stable thalamic lacunar infarct; no acute cerebellar lesionRobotic hysterectomy, BSO, pelvic lymphadenectomy + adj carboplatin/paclitaxel × 5 cyclesPLEX × 5, IVIG 400 mg/kg/day × 5, IV MP 1000 mg/day × 4 days, then po prednisone taperVertigo, ataxia, bilateral lower extremity weakness, vertical diplopia, nystagmus, dysmetria & dysarthria ~ 3 monthsmodest recovery of coordination and speech after PLEX, IVIG, steroids; remained non‐ambulatory with bilateral lower extremity paralysis, dysarthria, and cognitive limitations ≥ 3 years
Among the 40 cases, the most frequent malignancy was ovarian cancer (15 cases, 37.5%): 11 serous ovarian carcinoma, 2 ovarian carcinoma unspecified type, 1 clinically presumed but no biopsy was done, and our case with clear cell carcinoma in inguinal lymph node presumed ovarian origin but no primary identified in the uterus, fallopian tubes and ovaries pathology.
Breast cancer was the second most common, reported in 12 cases (30%), all of them were HER2-positive. Other confirmed gynecologic cancers included fallopian tube serous carcinoma in 3 cases, serous endometrial carcinoma in 1 case, and primary peritoneal serous carcinoma in 1 case, all sharing high-grade serous histologic features.
Non-gynecologic malignancies were also represented: lung carcinoma (squamous and large cell, 2 cases—the large cell found at autopsy), esophageal adenocarcinoma (1 case), and cholangiocarcinoma (1 case, presumed based on lymph node biopsy). Additionally, 1 case involved submandibular gland carcinoma. One case found to have poorly differentiated cancer cells in axillary lymph node, but no primary identified. Two cases had no malignancy detected despite extensive evaluation.
Most patients—33 out of 40—presented with subacute PCD symptoms, evolving over weeks to months, while only 6 patients had an acute onset with symptoms developing over a few days.
In 30 cases, PCD was diagnosed before the underlying malignancy, with reported intervals ranging from a few days to 8 months, and an average of approximately 5 months. Notably, only seven cases were diagnosed with cancer within the same week as PCD. This highlights the potential for a significant delay between neurologic and oncologic diagnoses, underscoring the importance of prolonged and repeated malignancy surveillance in patients with paraneoplastic cerebellar degeneration.
On the other hand, although less common, 8 cases had PCD onset after the cancer diagnosis, with reported intervals ranging from 5 months to 3 years. In several instances, PCD developed during remission or in the setting of recurrence—notably, in two patients who manifested PCD approximately 6 months before confirmed cancer recurrence, despite having completed initial treatment 1 to 3 years earlier (İlhan et al. 2021; Lie et al. 2016). These observations demonstrate that PCD can emerge well after an initial cancer diagnosis or period of remission, reinforcing the importance of continued neurologic surveillance in oncology patients, especially those at risk for recurrence.
Brain MRI findings were reported in all but one of the 40 patients with anti-Yo–associated PCD. Twenty-four patients (60%) had normal or unremarkable brain MRI at the time of presentation, reflecting the often non-specific or delayed imaging findings in early PCD. Eight patients (20%) demonstrated cerebellar atrophy on initial MRI, and an additional three patients initially had normal imaging but developed cerebellar atrophy on repeat MRI, highlighting the progressive nature of cerebellar degeneration (Frings et al. 2005; Kato et al. 2017; Dou et al. 2024). Isolated cases revealed other abnormalities: one patient had a focal cerebellar lesion (Ćerimagić and Džananović 2020), another had a cerebellar infarction (Tanaka et al. 1992), and one patient showed bilateral cerebellar T2 FLAIR hyperintensities without contrast enhancement (Westerlinck et al. 2022). Another had leptomeningeal enhancement prominently involving both cerebellar hemispheres (Zhuang et al. 2024). These findings show that while early brain MRI is often normal in PCD, serial imaging can reveal evolving cerebellar pathology, and occasional atypical findings may mimic other neurologic conditions, necessitating careful interpretation in the clinical context.
Among the 40 patients, anti-Yo antibodies were confirmed in serum only in 14 cases, CSF only in 2 cases, and in both serum and CSF in 20 cases, while 4 cases lacked documentation regarding the source of antibody detection. This highlights the diagnostic utility of testing both serum and CSF to increase the likelihood of detecting anti-Yo antibodies in suspected PCD.
Management generally combined definitive tumor therapy (often debulking surgery with platinum/taxane chemotherapy) and immunomodulatory treatments (high-dose steroids, IVIG, PLEX). Although most patients stabilized rather than experienced full neurologic recovery, a subset—8 of 38 cases (21%)—demonstrated significant neurologic improvement. For example, one patient regained independent ambulation at one year (Abdulaziz et al. 2018), another walked independently by two months with only minimal residual ataxia (Bhargava et al. 2014), and several others restored gait or showed marked improvement in coordination and balance (İlhan et al. 2021; Tanaka et al. 1992; Hu et al. 2020; Mirallas et al. 2020; Yan et al. 2018; Yang et al. 2025). These findings suggest that approximately 1 in 5 anti-Yo PCD patients may achieve functional recovery, notably higher than the < 10% recovery rate previously reported (Bradley et al. 2008).
Analyzing the eight cases with significant neurological recovery reveals a pattern: patients who improved tended to receive early intervention, targeting both the underlying malignancy and the immune process within a narrow window (ideally within 1–3 months) of symptom onset. Most had normal baseline MRIs (i.e., no cerebellar atrophy) and were treated with multimodal therapy, including surgery, chemotherapy, immunosuppressants (e.g., IVIG, steroids), and often structured rehabilitation. For example, in the case by Yang et al. (2025) a 62-year-old patient with lung cancer received prednisone and IVIG within 1–2 months of symptom onset, followed promptly by chemoradiation—resulting in resolution of her nystagmus and normalization of gait.
In contrast, patients who remained disabled generally experienced delays in diagnosis or incomplete treatment beyond this critical window, often accompanied by evidence of neuronal loss on imaging. For instance, Ćerimagić and Džananović (2020) describe a 61-year-old woman whose cerebellar symptoms persisted for approximately 10 months before receiving any tumor-directed or immunosuppressive therapy. Despite aggressive treatment with plasmapheresis, cyclophosphamide, azathioprine, and IVIG, she remained wheelchair-bound with severe ataxia and dysarthria.
Together, these examples suggest a clear pattern: once ataxia persists beyond approximately three to six months without definitive cancer-directed therapy and immunomodulation, irreversible Purkinje cell loss often ensues, and subsequent interventions fail to restore neurologic function. Clinicians should therefore recognize that initiating early, combined oncologic and PCD-specific therapy is crucial to maximize the chance of recovery.
Beyond conventional treatments such as tumor resection, chemotherapy, plasma exchange (PLEX), IVIG, steroids, and other immunosuppressive strategies, whole brain radiation therapy (WBRT) has been reported in a unique anti-Yo PCD case by Westerlinck et al. (2022). The patient—a 31-year-old woman with breast cancer-associated PCD—developed severe neurologic deficits, including expressive aphasia, paraparesis, and cerebellar tremor, despite tumor regression and standard immunosuppressive therapy. Concerned about irreversible damage, the clinical team proceeded with mastectomy followed by WBRT (10 Gy in 5 fractions), not for metastatic disease but rather to suppress the cerebellar autoimmune response. Following this combined approach, her neurologic decline stabilized, and she experienced gradual recovery of speech and motor function over the subsequent months (Westerlinck et al. 2022). This exceptional case raises the possibility that cranial irradiation may exert immune-modulating or neuroprotective effects in rapidly progressive anti-Yo PCD. While promising, the potential role of WBRT in this context remains speculative and warrants further clinical investigation.
Our patient’s presentation was typical in several ways: a middle-aged woman with subacute onset of vertigo, diplopia, and gait instability evolving over three months, accompanied by initially unremarkable imaging and a positive anti-Yo antibody result that prompted a thorough malignancy workup. Her treatment timeline and clinical course align with the patterns observed in prior cases. She first developed cerebellar symptoms preceding her initial presentation, but targeted immunotherapy—including five sessions of plasma exchange, IVIG, and high-dose steroids—was not initiated until approximately three months after symptom onset, when high-titer anti-Yo antibodies were confirmed. Definitive tumor-directed therapy, consisting of hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymphadenectomy followed by adjuvant carboplatin/paclitaxel, was further delayed until nearly seven months after initial neurologic symptoms emerged.
This delay beyond the critical 3-to-6-month window—associated with meaningful recovery in other anti-Yo PCD cases—likely contributed to her outcome: modest improvements in speech and coordination, but persistent non-ambulatory status. Her course reinforces the emerging observation that delays of six months or more often coincide with irreversible cerebellar injury, underscoring the importance of early recognition and dual-targeted treatment.
Our case is unique among reported anti-Yo PCD cases in that it is the first to document truly isolated nodal malignancy of presumed gynecologic origin confirmed through comprehensive surgical exploration, with no identifiable primary tumor. In Abdulaziz et al. (2018) a 68-year-old woman underwent axillary lymph node biopsy revealing metastatic carcinoma, and subsequent bilateral breast biopsies were negative; however, no pelvic or gynecologic exploration was performed to rule out an alternative primary source. Similarly, Chatham and Niravath (2021) reported a 61-year-old woman with isolated axillary node metastases who underwent mastectomy without detection of a breast tumor, and no further evaluation for a gynecologic origin was pursued. In the case by Elomrani et al. (2014) an 80-year-old woman underwent biopsy of an inguinal lymph node that revealed poorly differentiated adenocarcinoma with a gynecologic immunophenotype, yet she did not undergo hysterectomy or salpingo-oophorectomy, leaving the possibility of an occult ovarian primary unresolved. By contrast, our patient underwent robotic hysterectomy, bilateral salpingo-oophorectomy, and pelvic lymphadenectomy, with histopathology confirming clear cell carcinoma isolated to two common iliac lymph nodes and no malignancy found in the uterus, ovaries, or fallopian tubes. To the best of our knowledge, this represents the first anti-Yo PCD case with definitive exclusion of a gynecologic primary through complete surgical staging, supporting a diagnosis of isolated nodal metastases of presumed gynecologic origin.
The diagnostic challenge in such situations is profound. Even with serum and CSF anti-Yo positivity—strongly suggestive of breast or gynecologic malignancy—tumors may remain occult on routine imaging. In our patient, contrast CT and endometrial biopsy were unrevealing. Only FDG-PET/CT detected hypermetabolic iliac nodes. This highlights the value of FDG-PET/CT when standard imaging fails to localize a primary lesion in suspected PCD. If PET identifies isolated lymphadenopathy, empiric surgical exploration (e.g., lymphadenectomy plus removal of potential sites of origin) may be necessary to confirm the diagnosis and guide treatment. To the best of our knowledge, only two patients—Hu et al. (2020) and Dou et al. (2024)—with anti-Yo-positive PCD remained tumor-negative after exhaustive imaging and biopsy workups. Even in an exceptional report by Hasadsri et al. (2013), a 49-year-old man with anti-Yo PCD underwent extensive evaluation (including CT, MRI, and PET), yet no malignancy was identified ante mortem; only at autopsy was a 0.8 cm large-cell lung adenocarcinoma discovered, confirming an occult tumor hidden from clinical detection. Such “tumor-negative” cases therefore likely represent occult malignancies that either spontaneously regressed or remained below detection thresholds rather than true, permanent absence of cancer.
Our report expands the recognized spectrum of gynecologic malignancies associated with anti-Yo PCD by documenting a nodal clear cell carcinoma without an identifiable primary. When anti-Yo antibodies are detected but imaging is negative, clinicians should consider advanced metabolic imaging (FDG-PET/CT) and maintain a low threshold for surgical exploration of potential primary sites—even in the absence of radiographic or endometrial abnormalities. Early tumor localization and removal may limit irreversible Purkinje cell loss, although the overall prognosis for neurologic recovery remains guarded.
Conclusion
In conclusion, this case highlights the importance of maintaining a high index of suspicion for breast or gynecologic malignancies in patients presenting with subacute cerebellar dysfunction and anti-Yo antibodies, even when initial imaging studies are unrevealing. Advanced metabolic imaging such as FDG-PET/CT can uncover occult nodal disease that eludes conventional CT or MRI, and when PET identifies isolated lymphadenopathy without a clear primary, empiric surgical exploration—including hysterectomy, bilateral salpingo-oophorectomy, and lymphadenectomy—may be necessary to confirm the diagnosis. Although multimodal therapy (surgical resection, chemotherapy, plasma exchange, IVIG, and corticosteroids) can stabilize neurologic decline, irreversible Purkinje cell injury often leaves patients with significant residual deficits; therefore, early tumor localization and prompt treatment are crucial to optimizing neurologic outcomes, despite the overall guarded prognosis for full cerebellar recovery.