Pulmonary embolism complicating Mycoplasma pneumoniae pneumonia in children: a retrospective case series
Pei Tao, Zhigang Wang, Kaiyu Zhou, Ying Wu

TL;DR
This study reports on eight children with Mycoplasma pneumoniae pneumonia who developed pulmonary embolism and highlights the importance of early diagnosis and treatment.
Contribution
The paper presents a rare case series of pediatric Mycoplasma pneumoniae pneumonia complicated by pulmonary embolism, offering clinical insights and management strategies.
Findings
All eight children with MPP developed pulmonary embolism confirmed by CTPA.
Anticoagulation therapy with heparin and rivaroxaban led to favorable outcomes and resolution of emboli.
No recurrence was observed during follow-up, and thrombophilia markers normalized.
Abstract
To describe the clinical characteristics, management, and outcomes of children with Mycoplasma pneumoniae pneumonia (MPP) complicated by pulmonary embolism (PE). We conducted a retrospective review of eight children diagnosed with Mycoplasma pneumoniae pneumonia complicated by pulmonary embolism between January 2023 and December 2024 at our hospital. The diagnosis of pulmonary embolism was confirmed by computed tomography pulmonary angiography (CTPA). Demographic characteristics, clinical manifestations, laboratory findings, imaging features, treatment strategies, and outcomes were systematically collected. The cohort included six males and two females, with a mean age of 7.81 ± 3.64 years. The median interval from pneumonia onset to PE diagnosis was 14 days. All patients had severe or refractory MPP. Common symptoms included chest pain (n = 6), hemoptysis (n = 4), and dyspnea (n =…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
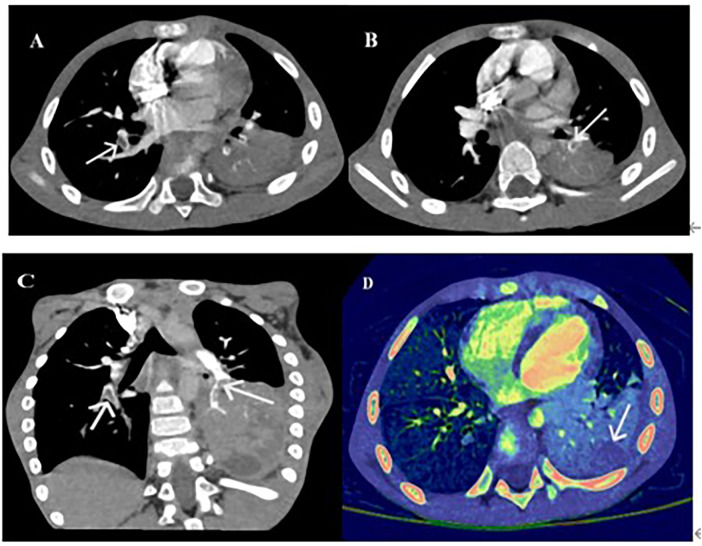 Figure 1
Figure 1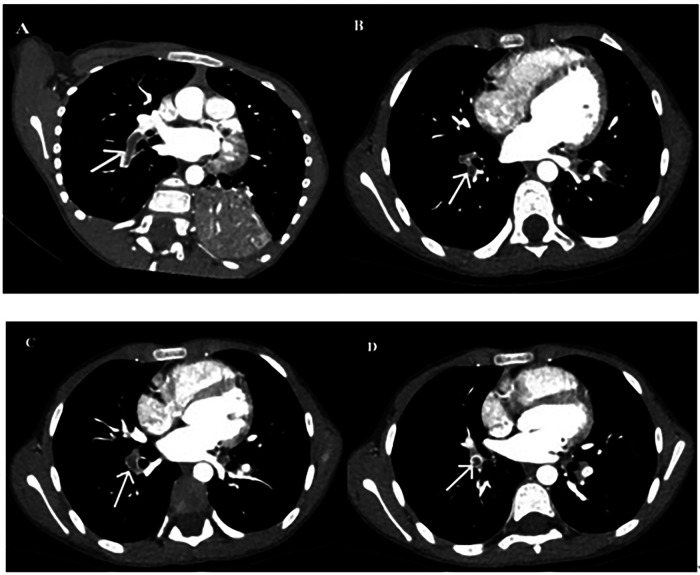 Figure 2
Figure 2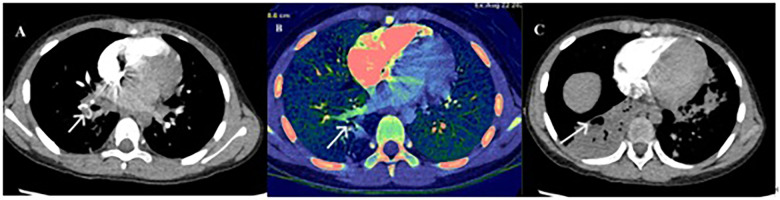 Figure 3
Figure 3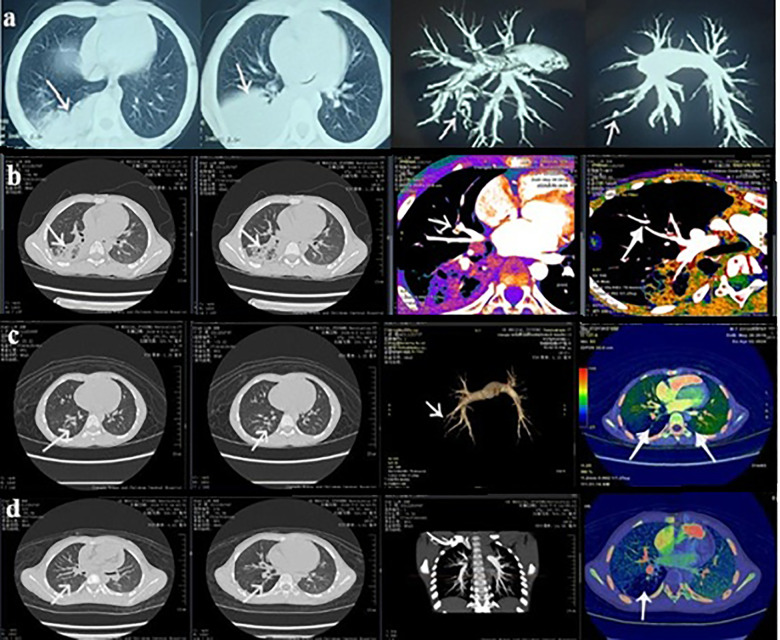 Figure 4
Figure 4| Case | Age (years) | Gender | Main symptoms | Etiology | Lung consolidation site | Embolic site | Complications |
|---|---|---|---|---|---|---|---|
| 1 | 2.75 | M | Cough, fever, dyspnea |
| Right upper and lower lobes | Right upper, middle, and lower lobes | Kawasaki disease; Necrotizing pneumonia |
| 2 | 4.75 | M | Cough, fever, dyspnea |
| Right upper lobe; left lower lobe | Both lower lobes | Necrotizing pneumonia |
| 3 | 8 | M | Cough, fever, chest pain, hemoptysis |
| Right lower lobe; left upper and lower lobes | Both lower lobes; left upper lobe | Necrotizing pneumonia |
| 4 | 9 | M | Cough, fever, chest pain, hemoptysis |
| Right lower lobe | Right lower lobe | Necrotizing pneumonia |
| 5 | 9 | M | Cough, fever, chest pain, hemoptysis |
| Right lower lobe | Right lower lobe | Necrotizing pneumonia |
| 6 | 6 | F | Cough, fever, chest pain |
| Bilateral lower lobes | Right lower pulmonary artery; anterior and posterior basal segments (right) | Necrotizing pneumonia |
| 7 | 8 | F | Cough, fever, chest pain |
| Right lower lobe | Right lower lobe | None |
| 8 | 15 | M | Cough, fever, chest pain, hemoptysis |
| Left lower lobe | Left lower lobe | Necrotizing pneumonia |
| Parameter | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | Case 8 | Median (IQR) |
|---|---|---|---|---|---|---|---|---|---|
| WBC (×10⁹/L) | 7.7 | 30.07 | 5.92 | 9.16 | 8.48 | 16.22 | 9.36 | 8.8 | 8.98 (8.09–12.79) |
| PLT (×10⁹/L) | 300 | 711 | 201 | 323 | 254 | 241 | 323 | 235 | 277 (238–323) |
| CRP (mg/L) | 27 | 18.5 | 157.6 | 24.5 | 7.8 | 17.8 | 42.8 | 8.9 | 21.5 (13.35–34.9) |
| PCT (ng/ml) | 0.127 | 0.107 | 0.412 | 0.047 | 0.100 | 0.115 | 0.550 | 0.170 | 0.121 (0.103–0.291) |
| D-dimer (mg/L) | 10.05 | 8.16 | 5.32 | 4.07 | 0.81 | 2.64 | 19.61 | 0.19 | 4.695 (1.725–9.105) |
| LDH (U/L) | 910.1 | 425.2 | 214 | 539.6 | 221 | 368.2 | 355.4 | 246.8 | 361.8 (233.9–482.4) |
| IgG (g/L) | 7.56 | 6.87 | 7.58 | 9.36 | 9.04 | 8.61 | 11.04 | 7.38 | 8.095 (7.425–9.280) |
| IgA (g/L) | 1.82 | 1.01 | 1.25 | 1.94 | 1.38 | 1.65 | 2.18 | 1.15 | 1.515 (1.175–1.910) |
| IgM (g/L) | 1.33 | 1.23 | 1.24 | 1.04 | 1.78 | 1.41 | 1.43 | 1.23 | 1.285 (1.230–1.425) |
| C3 (g/L) | 1.52 | 1.325 | 1.146 | 1.462 | 1.249 | 1.513 | 1.425 | 1.245 | 1.375 (1.246–1.500) |
| C4 (g/L) | 0.324 | 0.206 | 0.317 | 0.253 | 0.342 | 0.337 | 0.308 | 0.327 | 0.320 (0.266–0.334) |
| CD3+ (%) | 55.32 | 49.47 | 67.23 | 78.13 | 62.24 | 63.44 | 59.36 | 70.23 | 62.84 (56.33–69.48) |
| CD4+ (%) | 31.78 | 25.71 | 36.34 | 42.24 | 26.76 | 21.94 | 25.39 | 38.78 | 29.27 (25.47–38.17) |
| CD8+ (%) | 32.69 | 19.44 | 22.32 | 30.71 | 21.93 | 33.27 | 24.68 | 28.22 | 26.45 (22.03–32.20) |
| B cells (%) | 15.21 | 36.85 | 15.28 | 16.65 | 8.76 | 16.68 | 20.10 | 18.53 | 16.67 (15.23–19.71) |
| NK cells (%) | 8.66 | 13.16 | 15.35 | 4.57 | 26.28 | 19.10 | 15.40 | 19.34 | 15.38 (9.79–19.28) |
| Case | Antibiotics | Anticoagulant | Outcomes | ||
|---|---|---|---|---|---|
| Hospitalization | Outpatient | 3M | 6M | ||
| 1 | Erythromycin, Azithromycin | Enoxaparin for 7 d | Rivaroxaban for 3 m | Disappeared | – |
| 2 | Azithromycin, Cefotaxime | Enoxaparin for 7 d | Rivaroxaban for 3 m | Disappeared | – |
| 3 | Doxycycline, Cefotaxime | Enoxaparin for 7 d | Rivaroxaban for 3 m | Disappeared | – |
| 4 | Doxycycline | Enoxaparin for 7 d | Rivaroxaban for 3 m | Disappeared | – |
| 5 | Erythromycin | Enoxaparin for 7 d | – | Disappeared | – |
| 6 | Erythromycin | Enoxaparin for 7 d | Rivaroxaban for 6 m | – | Disappeared |
| 7 | Cefotaxime, Azithromycin | Enoxaparin for 10 d | Rivaroxaban for 6 m | – | Disappeared |
| 8 | Doxycycline, Peramivir | Enoxaparin for 7 d | – | Disappeared | – |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections · Infective Endocarditis Diagnosis and Management · Heparin-Induced Thrombocytopenia and Thrombosis
Introduction
1
Mycoplasma pneumoniae pneumonia (MPP) is the most common cause of community-acquired pneumonia in children aged 5 years and older in China (1). Severe M. pneumoniae pneumonia (SMPP) is defined as MPP meeting the criteria for severe community-acquired pneumonia and is often associated with significant intrapulmonary and extrapulmonary complications (2, 3). Common intrapulmonary complications include plastic bronchitis, moderate-to-large pleural effusion, extensive lung consolidation, pulmonary necrosis, and pulmonary embolism (PE) (4–6). Patients may present with clinical symptoms such as shortness of breath, chest pain, or hemoptysis (7, 8). In addition, extrapulmonary complications can involve multiple organ systems, including the liver, skin, nervous system, and hematologic system (1). PE, although relatively rare in children, can be life-threatening if not diagnosed and treated in a timely manner (9, 10).
Refractory M. pneumoniae pneumonia (RMPP) is diagnosed when children continue to experience persistent fever, progressive clinical deterioration, radiological worsening, or extrapulmonary complications despite receiving at least seven days of appropriate macrolide therapy. In recent years, the incidence of both SMPP and RMPP has increased, particularly during epidemic outbreaks, raising concerns regarding severe complications and atypical disease courses (11–15).
Beyond direct pulmonary involvement, M. pneumoniae infection can trigger a wide range of extrapulmonary complications through immune-mediated and vascular mechanisms, including autoimmunity, immune complex deposition, endothelial injury, and thrombosis (16–19). These mechanisms may contribute to thromboembolic events such as PE, highlighting the complex interplay between infection, inflammation, and coagulation. However, existing pediatric reports of PE complicating MPP are largely limited to isolated cases or small series, and systematic clinical descriptions remain scarce.
Comprehensive characterization based on structured clinical, laboratory, and imaging data may improve recognition of pulmonary embolism in children with severe or refractory Mycoplasma pneumoniae pneumonia. In this study, we retrospectively analyzed a series of pediatric patients with MPP complicated by PE, focusing on clinical presentation, diagnostic evaluation, treatment strategies, and outcomes. This clinically grounded overview may facilitate hypothesis generation and support future integrative research in pediatric thromboembolic disease.
Methods
2
Study design and participants
2.1
This was a retrospective observational study conducted at the Respiratory Department of Chengdu Women and Children's Central Hospital. Eight pediatric patients diagnosed with MPP complicated by PE were included. The study was conducted from January 2023 to December 2024. Eligible patients were identified by applying strict inclusion and exclusion criteria to the hospital's electronic medical records system.
Ethical statement
2.2
The study protocol was approved by the Ethics Committee of Chengdu Women and Children's Central Hospital {Approval No. [2024(95)]}. Written informed consent for computed tomography pulmonary angiography (CTPA) and data use for research purposes was obtained from the legal guardians of all patients. All clinical data were anonymized prior to analysis to ensure patient confidentiality.
Inclusion and exclusion criteria
2.3
Inclusion criteria for the PE group were as follows:
-
Diagnosis of MPP confirmed by: Positive M. pneumoniae-specific IgM (titer ≥ 1:160); and/or positive M. pneumoniae DNA detection via PCR from nasopharyngeal swabs.
-
Diagnosis of PE confirmed via CTPA showing embolic occlusion in the pulmonary vasculature.
-
Informed consent obtained for the CTPA procedure. The exclusion criteria included:
-
Alternative causes of PE, such as air embolism, congenital heart disease, central venous catheterization, nephrotic syndrome, surgery, malignancy, or use of hormonal contraceptives in adolescent females.
-
Incomplete clinical, laboratory, and imaging data.
Microbiological testing
2.4
Within 24 h of admission, all patients underwent comprehensive pathogen screening:
- M. pneumoniae DNA detection from nasopharyngeal swabs using a PCR kit (Tian Long Tech, China; detection limit: 100 copies/ml).
- A multiplex respiratory PCR panel targeting influenza A/B, respiratory syncytial virus, adenovirus, human metapneumovirus, and parainfluenza virus (Sansure Biotech Inc.).
- Serological IgM antibody testing against M. pneumoniae, Chlamydia pneumoniae, Legionello pneumophila, Rickettsia, and common respiratory viruses using ELISA kits (Mike Bio, China).
- Tuberculosis screening (T-SPOT.TB or PPD), and blood and sputum cultures for bacterial pathogens.
Laboratory and imaging data collection
2.5
Clinical and diagnostic data were extracted from electronic medical records and organized into a structured multi-dimensional dataset to enable potential future computational analyses.
Demographic and clinical characteristics
2.5.1
Data included patient age, sex, prior history of venous thromboembolism (VTE) or cardiovascular disease, duration from symptom onset to CTPA diagnosis, intensive care unit (ICU) admission, primary clinical manifestations, and anatomical distribution of PE.
Hematological and coagulation parameters
2.5.2
Complete blood counts and coagulation profiles were reviewed, including white blood cell (WBC) count, absolute neutrophil and lymphocyte counts, hemoglobin (Hb), platelet (PLT) count, plasma D-dimer levels.
Inflammatory and biochemical markers
2.5.3
Inflammatory indices such as C-reactive protein (CRP), procalcitonin (PCT) were recorded. Biochemical data included lactate dehydrogenase (LDH), alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin, albumin, serum creatinine, blood urea nitrogen (BUN), and serum electrolytes.
Immunological assessment
2.5.4
Serum immunoglobulin levels (IgA, IgG, and IgM), complement components (C3 and C4), and autoimmune markers [antinuclear antibodies (ANAs), extractable nuclear antigens (ENAs)] were analyzed. Lymphocyte subsets (CD3^+^, CD4^+^, CD8^+^, B cells, and NK cells) were evaluated using flow cytometry.
Imaging studies
2.5.5
Radiological investigations included CTPA to determine the presence and distribution of emboli, chest computed tomography or radiography to assess pulmonary involvement, and Doppler ultrasound of the lower extremities when clinically indicated.
Data presentation
2.6
Categorical variables were expressed as absolute numbers and proportions (%), while continuous variables were reported as medians and interquartile ranges (IQR) owing to their non-parametric distribution. No formal statistical analyses were performed, and all data are presented descriptively.
Results
3
Baseline characteristics
3.1
A total of eight children with severe or refractory M. pneumoniae pneumonia (SMPP/RMPP) complicated by pulmonary embolism (PE) were included. The cohort comprised six males and two females, aged 2–15 years (median 7.81 ± 3.64 years). Coinfections included Streptococcus pneumoniae (n = 2), Escherichia coli (n = 1), and influenza A virus (n = 1). The median interval from MPP onset to PE diagnosis was 14 days. No patients had a family history of thrombophilia or hereditary disease (Table 1). Fever and cough were observed in all eight patients. Additional symptoms included chest pain (n = 6), hemoptysis (n = 4), and dyspnea (n = 2). Heterogeneous pulmonary involvement and embolic distribution were noted, with a right-lung predominance (Table 1).
Laboratory, immunological, and coagulation profiles
3.2
Elevated D-dimer levels were observed in 7 of the 8 patients at the time of PE diagnosis, with a median of 4.695 mg/L (IQR 1.725–9.105 mg/L). One patient had a level within the normal range (0.19 mg/L). Median WBC was 8.98 × 10⁹/L (IQR 8.09–12.79), and median platelet count was 277 × 10⁹/L (IQR 238–323). Median CRP and procalcitonin levels were 21.5 mg/L (IQR 13.35–34.9) and 0.121 ng/ml (IQR 0.103–0.291), respectively. LDH was elevated in five patients (median 361.8 U/L, IQR 233.9–482.4). Immunologic evaluation showed IgG 8.095 g/L (IQR 7.425–9.280), IgA 1.515 g/L (IQR 1.175–1.910), IgM 1.285 g/L (IQR 1.230–1.425), complement C3 1.375 g/L (IQR 1.246–1.500), and C4 0.320 g/L (IQR 0.266–0.334). Lymphocyte subsets were within reference ranges: CD3 + 62.84% (IQR 56.33–69.48), CD4 + 29.27% (IQR 25.47–38.17), CD8 + 26.45% (IQR 22.03–32.20), B cells 16.67% (IQR 15.23–19.71), and NK cells 15.38% (IQR 9.79–19.28). No abnormalities were detected in thrombophilia-related tests, including antiphospholipid antibodies, protein C and S, coagulation factors, or inhibitors (Table 2).
The institutional reference ranges for all laboratory parameters are provided in the footnote of Table 2.
Imaging examination
3.3
Computed tomography pulmonary angiography (CTPA) confirmed PE in all eight cases. Emboli were located in the right lung (n = 5), left lung (n = 1), or both lungs (n = 2). PE-related vascular occlusion was associated with localized parenchymal necrosis in affected regions. Five patients developed necrotizing pneumonia, and one had Kawasaki disease (Figures 1–3).
Computed tomography pulmonary angiography (CTPA): (A) Right pulmonary artery embolism. (B) Left pulmonary embolism (PE). (C) Double PE coronal axis diagram. (D) Energy spectrum of double PE.
(A–D) Left PE observed at different time points.
CTPA: (A) pulmonary thrombosis. (B) Angiography and energy spectrum. (C) Corresponding necrotic areas after PE.
Treatment and follow-up
3.4
All patients received enoxaparin during hospitalization (7–10 days). Outpatient oral anticoagulation with rivaroxaban was administered in six cases (3–6 months). Anti-M. pneumoniae therapy included erythromycin, azithromycin, doxycycline, and/or cefotaxime. One patient received antiviral therapy (peramivir). All eight patients demonstrated complete thrombus resolution during follow-up (3–6 months), with no recurrence observed (Table 3, Figure 4).
CPTA (Case no. 7): (a) Baseline. (b) 1-month follow-up. (c) 3-month follow-up. (d) 6-month follow-up.
Discussion
4
Pulmonary embolism (PE) is a relatively rare but potentially life-threatening complication in children, especially when it occurs secondary to severe or refractory Mycoplasma pneumonia (MPP) (9, 20–26). The epidemiological data for the pediatric population in China is still limited, although recent reports indicate an upward trend. In our study cases, PE occurred within the median 14 days after the onset of MPP, highlighting the importance of early identification of severely or refractory diseases in children.
Previous studies have reported the positive rate of thrombotic autoantibodies in children with MPP-related embolic events (27). In contrast, our cohort did not demonstrate significant abnormalities in thrombosis-related autoantibodies, including antiphospholipid antibodies and antinuclear antibodies, suggesting heterogeneity in immune-mediated thrombotic mechanisms across pediatric populations.
M. pneumoniae infection activates B cell–mediated immune responses, leading to increased IgM and IgG production and alterations in IgA and IgE levels. Severe MPP has also been associated with pathological lymphocyte activation, elevated complement components C3 and C4, and dysregulated T cell subsets, including reduced CD3^+^/CD4^+^ and NK cells with increased CD8^+^ T cells (28–31). Although elevated IgA has been implicated in the progression of pediatric PE (32), such immune abnormalities were not observed in our cohort. These discrepancies may reflect population-specific immune characteristics, underlying genetic heterogeneity, or the limited sample size of the present study. Nevertheless, the systematic documentation of immune parameters alongside clinical and imaging findings in our series provides a clinically grounded framework for future studies exploring immune–thrombotic mechanisms in MPP-related PE.
The clinical manifestations of pediatric pulmonary embolism are diverse and often atypical. In our case series, 6 patients experienced chest pain, 4 had hemoptysis, and 2 had breathing difficulties. Laboratory results also showed heterogeneity: 7 patients had elevated D-dimer levels (≥0.5 mg/L), while platelet count, CRP, and LDH were elevated to varying degrees. However, D-dimer alone is insufficient to rule out PE in children, as normal values may be observed in confirmed cases. These indicators were associated with disease severity and necrotizing pneumonia (33–41). Taken together, these observations indicate the interaction between inflammation, coagulation, and pediatric MPP-related PE lung injury, and highlight the need for imaging evaluation, such as CTPA, in severe or refractory cases.
Computed tomography pulmonary angiography (CTPA) remains the diagnostic gold standard for pulmonary embolism (PE) (42). In pediatric patients, its use is often limited by concerns regarding radiation exposure, small vessel caliber, and nonspecific clinical presentations (43). Despite these challenges, CTPA played a central role in our cohort by confirming the diagnosis of PE in all eight patients and enabling dynamic assessment of thrombus resolution during follow-up. Notably, pulmonary necrotic changes were observed in the disease progression of several children, raising questions about persistent perfusion defects and potential microvascular damage. These imaging results provide in-depth insights into the evolution of pediatric PE under anticoagulation therapy and emphasize the importance of careful radiological assessment. Despite the limitations of sample size and follow-up time, our longitudinal imaging observations highlight the unresolved issues regarding vascular changes after thrombosis, and this requires further study in a larger pediatric cohort.
The management of thromboembolic diseases in children still mainly relies on consensus recommendations and inferences from adult studies (44–46). In our study cases, all patients initially received low-molecular-weight heparin anticoagulation therapy, and most patients subsequently switched to rivaroxaban for maintenance treatment. The clinical outcomes were good, and complete resolution of pulmonary embolism was observed during the follow-up period. It is notable that both patients who continued oral anticoagulation treatment and those who stopped treatment early showed improvement, highlighting the current uncertainty.
In summary, the case series we studied provided a rare and clinically detailed group sample for children with pulmonary embolism related to MPP. By highlighting new observations, including immune heterogeneity, atypical symptom manifestations, and differences in laboratory results, these findings complement the existing literature and point out the areas that require further research. Despite limitations such as the retrospective design, small sample size, and single-center setting, this dataset lays the foundation for prospective, multicenter studies to elucidate the natural course, risk factors, and long-term prognosis of pediatric pulmonary embolism, and may provide guidance for targeted clinical management strategies.
Conclusion
5
Pulmonary embolism (PE) complicating M. pneumoniae pneumonia (MPP) is an uncommon but clinically serious condition in children (47, 48). In this retrospective case series, we described eight pediatric patients with MPP-related PE, systematically summarizing their clinical presentation, laboratory and immunological findings, imaging characteristics, management strategies, and outcomes. Although the small sample size limits the generalizability of our observations, the rarity of this complication makes detailed case-based data clinically informative. Our findings highlight the diagnostic challenges of PE in pediatric MPP and underscore the importance of timely recognition and appropriate anticoagulant therapy. This structured clinical experience may serve as a reference for clinicians and provide a foundation for future studies aimed at improving risk assessment and management of pediatric thromboembolic disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Health Commission of the People’s Republic of China. Guidelines for the diagnosis and treatment of Mycoplasma pneumoniae pneumonia in children (2023 edition). Int J Epidemiol Infect Dis. (2023) 50(2):79–84. 10.3760/cma.j.cn 331340-20230217-00023 · doi ↗
- 2Respiratory Group, Pediatrics Branch of Chinese Medical Association, Editorial Committee of Chinese Journal of Pediatrics, Pediatric Specialty Committee of Chinese Medical Education Association. Guidelines for the management of community-acquired pneumonia in children (2024 revision). Zhonghua Er Ke Za Zhi. (2024) 62(10):920–30. 10.3760/cma.j.cn 112140-20240728-0052339327958 · doi ↗ · pubmed ↗
- 3Miyashita N Kawai Y Inamura N Tanaka T Akaike H Teranishi H Setting a standard for the initiation of steroid therapy in refractory or severe Mycoplasma pneumoniae pneumonia in adolescents and adults. J Infect Chemother. (2015) 21(3):153–60. 10.1016/j.jiac.2014.10.00825533771 · doi ↗ · pubmed ↗
- 4Gao HM Qian SY. Treatment of refractory, fulminant and macrolide-resistant Mycoplasma pneumoniae pneumonia. Chin Pediatr Emerg Med. (2021) 28(1):1–6. 10.3760/cma.j.issn.1673-4912.2021.01.001 · doi ↗
- 5Zhou Y Shan Y Cui Y Shi J Wang F Miao H Characteristics and outcome of severe Mycoplasma pneumoniae pneumonia admitted to PICU in Shanghai: a retrospective cohort study. Crit Care Explor. (2021) 3(3):e 0366. 10.1097/CCE.000000000000036633786442 PMC 7994047 · doi ↗ · pubmed ↗
- 6Zhang M. Clinical characteristics and imaging features of severe Mycoplasma pneumoniae pneumonia in children. Chin J CT MRI. (2020) 18(2):37–40. 10.3969/j.issn.1672-5131.2020.02.012 · doi ↗
- 7Hennelly KE Ellison AM Neuman MI Kline JA. Clinical variables that increase the probability of pulmonary embolism diagnosis in symptomatic children. Res Pract Thromb Haemost. (2019) 4(1):124–30. 10.1002/rth 2.1226531989094 PMC 6971320 · doi ↗ · pubmed ↗
- 8Liu FQ Zhang J Chen X Ding N Dai FF Wang K Clinical analysis and etiological investigation of 30 cases of pulmonary embolism in children. Chin J Appl Clin Pediatr. (2022) 37(18):1386–91. 10.3760/cma.j.cn 101070-20220126-00099 · doi ↗