Comparative effectiveness and safety of vonoprazan/amoxicillin-based dual therapy versus quadruple therapy as second-line treatment for Helicobacter pylori Infection: a retrospective cohort study
Ying-Ying Han, Ji-Yan Li, Ya-Ni Zhou, Lin Tuo, Ge Wang, Jing-Mei Liu, Zhen-Zhen Zhou, Mei Liu, Pei-Yuan Li

TL;DR
This study compares two second-line treatments for Helicobacter pylori infection and finds that a simpler dual therapy is as effective as a more complex one but with fewer side effects.
Contribution
The study introduces a simplified dual therapy as a viable second-line treatment for H. pylori with comparable efficacy and better safety than quadruple therapy.
Findings
VA dual therapy and VAMB quadruple therapy had comparable eradication rates in second-line treatment.
VA therapy had significantly fewer adverse events compared to VAMB therapy.
Both treatment groups showed excellent medication adherence.
Abstract
The introduction of vonoprazan has markedly enhanced the effectiveness of the first-line Helicobacter pylori (H. pylori) eradication regimens. This study aimed to compare the effectiveness of vonoprazan-amoxicillin based dual therapy with that of quadruple therapy as second-line treatments, while also investigating potential clinical predictors of therapeutic success. From January 2023 to June 2025, we retrospectively analyzed clinical data from H. pylori-infected patients who received second-line treatment with either: vonoprazan-amoxicillin dual therapy (VA) or VA based quadruple therapy (VAMB; vonoprazan, amoxicillin, minocycline, and colloidal bismuth pectin). The eradication status was evaluated by 13/14Curease breath test four weeks after treatment completion. Adverse events and medication compliance were systematically documented during follow-up. The study included 241…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
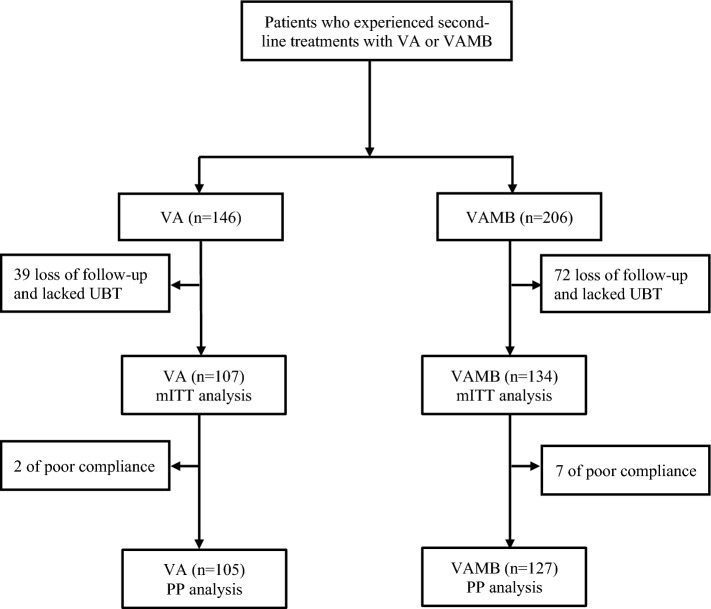 Figure 1
Figure 1- —Tongji Hospital Clinical Research Fund
- —https://doi.org/10.13039/501100004761Natural Science Foundation of Hainan Province
- —Hainan Province Science and Technology Special Fund
- —https://doi.org/10.13039/501100003819Natural Science Foundation of Hubei Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Clostridium difficile and Clostridium perfringens research · Gastric Cancer Management and Outcomes
Introduction
Helicobacter pylori (H. pylori) infection remains a serious global health challenge, leading to various gastric and extra-gastric complications [1]. Despite declining prevalence in certain regions, recent studies indicate that over 40% of adult worldwide remain infected, imposing a substantial burden on healthcare systems [2, 3]. Successful eradication of H. pylori infection can help to restore normal gastric mucosa, relieve symptoms, and reduce gastric cancer risk [4]. However, rising antibiotic resistance—particularly to clarithromycin, levofloxacin, and metronidazole—has significantly compromised eradication rates [5]. Reports indicate that 10–20% of H. pylori infection patients failed in initial treatment and required rescue therapy [6, 7]. Repeated eradication failures further promote the development of multidrug-resistant strains, posting major challenge for subsequent treatment strategies.
Although individual susceptibility testing (molecular or after culture) is recommended for rescue therapy, such protocols are not routinely implemented in clinical practice due to their cumbersome procedures and high costs [4, 8]. The Maastricht VI/Florence consensus recommended fluoroquinolonecontaining regimens as empiric second-line therapy when patients failed to first triple or nonbismuth quadruple therapies [4]. Given that the resistance rate of levofloxacin has reached 30% to 50% in China, fluoroquinolone-based regimens are not suitable as salvage treatment [5]. The 2022 Chinese guideline continued to recommend bismuth quadruple therapy (BQT) for empiric second-line treatment of H. pylori infection, utilizing antibiotic combinations with low resistance rates, such as amoxicillin, tetracycline, or furazolidone [8]. In contrast, minocycline—a tetracycline derivative with broad-spectrum antibacterial activity—has been used in H. pylori eradication for over two decades [9]. It exhibits a low resistance rate and is widely accessible in clinical settings [10]. Both minocycline and amoxicillin demonstrate high efficacy against H. pylori infection, and their combination offers several advantages, including simplified dosing, favorable safety, and good tolerability. As a result, this regimen has become a common empirical choice for rescue therapy [11].
Recent studies [12] have demonstrated that high-dose dual therapy (HDDT), consisting of esomeprazole or rabeprazole (double dose bid or standard dose qid) combined with amoxicillin (≥ 3 g/day, administered as 1 g tid or 0.75 g qid), has achieved satisfactory efficacy with fewer adverse reactions, making it a recommended option for both first- and second-line eradication treatments [8]. The introduction of vonoprazan, a reversible potassium-competitive acid blocker (P-CAB), has further enhanced H. pylori eradication rates due to its more potent and sustained acid suppression compared to proton pump inhibitors (PPIs) [13]. Our previous research established that a 10-day vonoprazan-amoxicillin (VA) dual therapy could achieve an eradication rate of over 90% in the first-line treatment [14]. Nevertheless, data supporting VA dual therapy as second-line regimen remain limited. Existing reports show considerable regional variation in outcomes, and few studies have systematically compared the efficacy and safety profiles between VA-based dual therapy and quadruple regimens in remedial settings.
To address these knowledge gaps, this study aimed to compare the efficacy and safety of VA dual therapy versus VAMB (vonoprazan-amoxicillin-minocycline-bismuth) quadruple therapy as second‑line treatments for H. pylori infection.
Methods
Study design and patients
This was a retrospective cohort study conducted at Division of Gastroenterology in Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. Data were retrieved from consecutive patients between January 2023 and June 2025. We enrolled H. pylori-infected patients who failed only one course of H. pylori eradication, and received VA or VAMB regimen as second-line treatment. In this study, the selection of VA or VAMB regimen as second-line treatment was made by the attending physician, taking into account the patient’s previous treatment history, compliance, potential adverse reaction risks, and through shared decision-making with the patient.
Exclusion criteria encompassed: (i) naive to H. pylori treatment; (ii) history of gastrectomy; (iii) intake of antibiotics, bismuth, Chinese traditional medicines with antibacterial effect within the preceding 4 weeks, or PPIs, P-CAB, H_2_ receptor antagonists within the previous 2 weeks. Medical information, such as demographic information, clinical characteristics, treatment outcome, adverse effects, and compliance were extracted from the electronic medical records and telephone/WeChat (a mobile messaging application) follow-up.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by the Institutional Ethics Board of Tongji Hospital, Wuhan, China (Approval Number: TJ-IRB202505047, dated May 30, 2025). All participants signed written informed consent forms before enrolment.
Diagnosis of H. pylori infection and treatment regimen
H. pylori infection was diagnosed by positive ^13/14^Curease breath test (^13/14^C-UBT), immuno-histochemical staining of biopsy samples, or stool antigen test (SAT). As to the outcome of treatment, the H. pylori status was assessed by ^13/14^C-UBT at least 4 weeks after completion of therapy.
The VA dual regimen consisted of VPZ (Takeda Pharmaceutical Co., Ltd., China) 20 mg twice daily and amoxicillin (Hainan General Sanyang Pharmaceutical Co., Ltd., China) 1000 mg three times daily (both after meals) for 14 days. The VAMB quadruple regimen consisted of VPZ (Takeda as above) 20 mg twice daily, amoxicillin (General Sanyang as above)1000 mg twice daily, minocycline (Hanhui Pharmaceutical Co., Ltd., China) 100 mg twice daily, and colloidal bismuth pectin (Heilongjiang Dilong Pharmaceutical Co., Ltd., China) 200 mg twice daily for 14 days. Patients were suggested to take vonoprazan and colloidal bismuth pectin half an hour before meals, while amoxicillin and minocycline taken immediately after meals.
Study outcomes
The primary outcome was the eradication rate. Patients who were lost to follow-up or lacked re-examination results were excluded before the modified intention-to-treat (mITT) analysis, and those with poor compliance were further excluded before the per-protocol (PP) analysis. The secondary outcomes included the incidence of adverse events, compliance, and related factors might affect the therapeutic effect. Adverse events were reported by participants as instructed according to the influence of adverse events on their daily activities. It was graded as “mild” (existing but transient, tolerable, and not affecting daily life), “moderate” (psychological or physical discomfort, partly affecting daily life), and “severe” (severe interruption of their daily activities). The frequency of adverse events was assessed by counting the number of patients with each event. Multiple adverse reactions may occur in one patient and should be counted separately. Compliance was considered as “poor”, if the patient had taken < 80% of the prescribed medications.
Statistical analysis
Continuous variables were expressed as median (interquartile range), and were compared through the Mann–Whitney test. Categorical variables were presented as numbers and percentages (%), and were compared through the Chi-square test or Fisher’s exact test, as appropriate. Univariate analysis was performed to explore significant predictive variables. All statistical calculations were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). P value with both-sided < 0.05 was regarded statistically significant.
Results
Baseline characteristics
As shown in Fig. 1, a total of 352 patients with first treatment failure of H. pylori infection received second-line treatment with either the VA or VAMB regimens. After excluding those lost to follow-up or lacking re-examination results, 107 subjects in the VA group and 134 in the VAMB group were included in the mITT analysis. Additionally, 2 patients in the VA group and 7 in the VAMB group were excluded from the PP analysis for poor compliance.Fig. 1. Flow diagram of this study. VA, dual therapy with vonoprazan and amoxicillin dual therapy; VAMB, bismuth quadruple therapy with vonoprazan, amoxicillin, and minocycline; mITT, modified intention-to-treat; PP, per-protocol; UBT, urea breath test
The demographic and clinical characteristics of the mITT population are summarized in Table 1. Baseline characteristics were comparable between the two groups, with the exception of previous treatment regimens. Specifically, the proportion of patients who had received dual therapy as first-line treatment was significantly higher in the VAMB group than in the VA group (10.4% vs. 2.8%, p = 0.021).Table 1. Baseline demographics and clinical data of patientsBaseline factorsVA (n = 107)VAMB (n = 134)P valueSex (male: female)47:6056:780.739Age (years)46.0 (34.0–56.0)48.5 (36.0–57.0)0.278BMI (kg/m^2^)22.7 (20.5–24.7)22.9 (21.4–24.2)0.674BSA (m^2^)1.63 (1.50–1.82)1.64 (1.54–1.78)0.702Family population (< 3: ≥ 3)17:9016:1180.376Style of dining (individual dining: gather dining)48:5951:830.286Smoking17(15.9%)22(16.4%)0.912Drinking23(21.5%)23(17.2%)0.395Time to rescue therapy0.252 < 6 months10(9.3%)19(14.2%) ≥ 6 months97(90.7%)115(85.8%)Previous therapy BQT73(68.2%)87(64.9%)0.590 Triple therapy18(16.8%)16(11.9%)0.279 Dual therapy3(2.8%)14(10.4%)0.021 Unknow13(12.1%)17(12.7%)0.900Amoxicillin used previously91(85.0%)104(77.6%)0.145Digestive Symptoms57(53.3%)64(47.8%)0.395 Abdominal distension24(22.4%)26(19.4%)0.565 Stomachache15(14.0%)16(11.9%)0.632 Belching19(17.8%)17(12.7%)0.273 Abdominal discomfort5(4.7%)7(5.2%)0.845 Acid reflux/Heartburn21(19.6%)18(13.4%)0.195 Nausea/Vomiting3(2.8%)3(2.2%)1.000 Others7(6.5%)4(3.0%)0.315Endoscopy diagnosis76(71.0%)95(70.9%)0.982 Non-atrophic gastritis36(33.6%)59(44.0%)0.101 Atrophic gastritis30(28.0%)30(22.4%)0.314 Peptic ulcer12(11.2%)17(12.7%)0.727 Reflux esophagitis4(3.7%)9(6.7%)0.309 Gastric polyp5(4.7%)3(2.2%)0.493 Gastric cancer1(0.9%)1(0.7%)1.000Family history of gastric carcinoma5(4.7%)2(1.5%)0.282BMI, body mass index; BSA, body surface area; BQT, bismuth quadruple therapy
H. pylori eradication rates
Eradication rates are presented in Table 2. In the mITT analysis, the eradication rates were 90.7% (97/107; 95% CI 85.0–96.3%) in the VA group and 92.5% (124/134; 95% CI 88.0–97.0%) in the VAMB group. Similarly, in the PP analysis, eradication rates were 91.4% (96/105; 95% CI 86.0–96.9%) and 93.7% (119/127; 95% CI 89.4–98.0%), respectively. No statistically significant differences were observed between the two groups in either analysis (mITT: p = 0.599; PP: p = 0.509).Table 2. Eradication rates of the two treatment groupsAnalysisVAVAMBP valuemITT90.7% (97/107)92.5% (124/134)0.59995% CI85.0%-96.3%88.0%-97.0%PP91.4% (96/105)93.7% (119/127)0.50995% CI86.0%-96.9%89.4%-98.0%CI, confidence interval; mITT, modified intention-to-treat; PP, per-protocol
Adverse events and compliance
Adverse events (AEs) observed during eradication therapy in both groups are detailed in Table 3. The overall incidence of AEs was significantly higher in the VAMB group (17.9%, 24/134) than in the VA group (8.4%, 9/107; p = 0.033). In the VA group, the most frequently reported AEs included nausea/vomiting, diarrhea, or abdominal distension. One patient experienced transient but notable abdominal pain, which resolved after treatment discontinuation. The VAMB group primarily reported dizziness, nausea/vomiting, or abdominal distension, with no treatment discontinuations due to AEs. Due to the retrospective design of this study, mild or transient AEs—such as amoxicillin-associated rashes—may not have been systematically documented. Importantly, all AEs were mild to moderate in severity and resolved spontaneously after treatment completion. Treatment compliance was excellent and comparable between groups: 98.1% (105/107) in the VA group versus 94.8% (127/134) in the VAMB group (p = 0.306).Table 3. Adverse events and compliance of the two treatment groupsAnalysisVA (n = 107)VAMB (n = 134)P valueAdverse effectsNo. of patients9 (8.4%)24 (17.9%)0.033Total No. of events12 (11.2%)30 (22.4%)0.023Nausea/Vomiting4 (3.7%)6 (4.5%)1.000Dizziness1 (0.9%)8 (6.0%)0.088Diarrhea4 (3.7%)3 (2.2%)0.762Abdominal distension2 (1.9%)4 (3.0%)0.892Poor appetite03 (2.2%)0.331Dry mouth03 (2.2%)0.331Abdominal pain1 (0.9%)2 (1.5%)1.000Black tongue01 (0.7%)1.000Discontinued drugs because of adverse events1 (0.9%)00.444Compliance98.1% (105/107)94.8% (127/134)0.306
Factors influencing eradication efficacy
The factors influencing the eradication efficacy were presented in the mITT population. As presented in Table 4, demographic and lifestyle factors including sex, age, body mass index (BMI), body surface area (BSA), smoking status, alcohol consumption, style of dining, family population, and presence of digestive symptoms showed no significant association. Additionally, treatment-related factors such as occurrence of side effects and medication compliance were similarly not correlated with treatment outcomes (all p > 0.05).Table 4. Univariate analysis of factors influencing eradication rates in the two treatment groupsVariablesVA (n = 107)VAMB (n = 134)Eradication rateP valueEradication rateP valueSex Male91.5% (43/47)1.00087.5% (49/56)0.122 Female90.0% (54/60)96.2% (75/78)Age, years < 3589.7% (26/29)0.70395.7% (22/23)0.087 35–5087.9% (29/33)98.0% (48/49) > 5093.3% (42/45)87.1% (54/62)BMI, kg/m^2^ < 2292.7% (38/41)0.84197.6% (41/42)0.312 22–2590.0% (36/40)89.6% (60/67) > 2588.5% (23/26)92.0% (23/25)BSA, m^2^ < 1.6589.5% (51/57)0.90895.9% (70/73)0.199 ≥ 1.6592.0% (46/50)88.5% (54/61)Smoking Yes100% (17/17)0.32381.8% (18/22)0.099 No88.9% (80/90)94.6% (106/112)Drinking Yes82.6% (19/23)0.27587.0% (20/23)0.495 No92.9% (78/84)93.7% (104/111)Style of dining Individual dining95.8% (46/48)0.18596.1% (49/51)0.377 Gather dining86.4% (51/59)90.4% (75/83)Family population < 394.1% (16/17)0.93681.3% (13/16)0.186 ≥ 390.0% (81/90)94.1% (111/118)Time to rescue therapy, month0.2351.000 < 680.0% (8/10)94.7% (18/19) ≥ 691.8% (89/97)92.2% (106/115)Amoxicillin used previously1.0000.560 Yes90.1% (82/91)91.3% (95/104) No93.8% (15/16)96.7% (29/30)Digestive symptoms Yes91.2% (52/57)1.00095.3% (61/64)0.401 No90.0% (45/50)90.0% (63/70)Side effects Yes88.9% (8/9)1.00091.7% (22/24)1.000 No90.8% (89/98)92.7% (102/110)Compliance Good91.4% (96/105)0.17993.7% (119/127)0.149 Poor50% (1/2)71.4% (5/7)
We further examined the potential impact of two specific clinical factors: the interval before rescue therapy and prior amoxicillin use in first-line treatment. The analysis revealed that neither the duration between treatments nor previous amoxicillin exposure significantly affected the eradication rate (all p > 0.05).
Discussion
We conducted a retrospective cohort study to evaluate the efficacy and safety of VA dual therapy and VAMB quadruple therapy as second-line treatments for H. pylori infection after first-line treatment failure. Although this study was conducted in a tertiary academic hospital, which may not fully represent the broader primary care settings, it represents routine practice within a specialized referral center. The treatment decisions, patient management, and outcome assessments reflect routine clinical care without experimental intervention, preserving the essence of an observational effectiveness study [15]. Both the mITT and PP analysis yielded eradication rates exceeding 90% for each regimen as second-line therapies. No statistically significant difference in efficacy was observed between the two groups. Moreover, the VA dual therapy showed a more favorable safety profile, with a significantly lower incidence of adverse events (8.4% vs. 17.9%, p < 0.05). Eradication success was unaffected by the interval time to rescue therapy, prior amoxicillin usage, or patient compliance. Given its comparable efficacy and superior tolerability, the VA dual therapy may be considered a preferred option for second-line H. pylori eradication.
The antibiotic resistance remains the primary challenge in the eradication of H. pylori infection. A recent meta-analysis [5] has revealed alarming resistance patterns in mainland China: the primary and secondary resistance rates were 30.72% and 75.53% for clarithromycin, 32.98% and 58.17% for levofloxacin, and 70.14% and 88.56% for metronidazole, respectively; while resistance rates remained relatively low for amoxicillin (2.41% and 3.43%), tetracycline (2.53% and 0.42%), and furazolidone (1.54% and 0.45%). Despite these favorable low resistance profiles for furazolidone, tetracycline, and amoxicillin, the clinical utility of furazolidone and tetracycline is constrained by safety concerns or limited availability compared to amoxicillin, rendering the selection of appropriate antibiotic combinations for rescue therapy particularly challenging [16]. Several studies highlighted promising results with amoxicillin and minocycline-based bismuth quadruple therapy (BQT). You et al. [17] reported 92% (66/72) and 100% (42/42) eradication rates in H. pylori first-line and rescue therapy, respectively. A Southwest China real-world study [18] achieved 91.3% (21/23) success in H. pylori treatment-experienced patients. While these studies yielded promising outcomes, their interpretation was limited by relatively small sample sizes and heterogeneous patient populations with varying treatment histories. Thereby, it precluded definitive conclusions regarding VAMB’s efficacy specifically in the second-line treatment. Our study included 134 patients with precisely one prior treatment failure, demonstrating that the VAMB regimen achieved eradication rates of 92.5% (mITT) and 93.7% (PP) as a second-line therapy. Such high efficacy may be attributed to the rapid and potent acid-suppressive effect of vonoprazan, and the high sensitivity of H. pylori to the amoxicillin-minocycline combination, additionally with the function of bismuth.
In 2020, Suzuki et al. [19] first established the clinical efficacy of VA dual therapy for treatment-naive patients with H. pylori infection. Recognized for its superior efficacy, simplified dosing regimen, and favorable tolerability profile, this approach has been endorsed as a first-line therapy in the current American College of Gastroenterology (ACG) Clinical Guideline [20]. Emerging evidence supports the application of VA dual therapy in rescue treatment settings. A retrospective study [21] demonstrated an overall eradication rate of 92.5% (172/186), with subgroup analysis revealing 92.9% (78/84), 96.3% (52/54), and 87.5% (42/48) success rates for patients with 1, 2, or ≥ 3 prior treatment failures, respectively. Liu et al. [22] conducted a randomized controlled trial comparing VA dual therapy with culture-guided therapy in treatment-experienced patients, finding comparable efficacy (87.5% vs. 83.3%) but superior tolerability with the VA regimen. However, another study [23] reported somewhat lower success rates (ITT: 73.8%; PP: 82.1%) using the same VA regimen, though their study lacked stratification by prior treatment attempts. These outcome variations likely reflected differences in study samples, regional resistance patterns, and inclusion criteria. Our results showed that the efficacy of the VA group exceeds 90% as a second-line treatment, probably attributable to several key factors: (1) rigorous patient selection limited to first-treatment failure; (2) persistently low secondary resistance to amoxicillin (3.43% in China) [5]; (3) potent acid-suppressive effect of vonoprazan; (4) A 14-day long course of treatment can ensure the efficacy of VA dual regimen.
It is noteworthy that the dosing schedule of amoxicillin differed between the two regimens: 1000 mg three times daily in the VA group versus 1000 mg twice daily in the VAMB group. This reflects the distinct rationales behind each regimen—maximizing the time above MIC for a single antibiotic in the dual therapy [12] versus employing a standard dose within a broader-spectrum combination in the quadruple therapy [8]. Our results showed comparable eradication rates between the two groups (mITT analysis: 90.7% vs. 92.5%, p > 0.05). This suggests that in the VA regimen, the strategy of intensifying amoxicillin dosing may effectively compensate for the synergistic antimicrobial effect offered by the addition of minocycline and bismuth in the quadruple regimen.
The VA regimen demonstrated significantly better tolerability, with an AEs incidence of 8.4% compared to 17.9% of VAMB regimen (p < 0.05). Nausea/Vomiting and diarrhea were common adverse reactions in VA group. Dizziness and Nausea/Vomiting were more common in VAMB group, consistent with previous findings from minocycline-containing regimens [10, 24]. Owing to the higher lipid solubility and being easier to across the blood–brain barrier than other tetracyclines, minocycline may cause more neurological-related side effects [25]. The standard dosage of minocycline was 200 mg/d for the eradication of H. pylori infection [10]. Huang et al. [26] pioneered an optimized quadruple regimen using reduced-dose minocycline (50 mg twice daily) combined with metronidazole (400 mg thrice daily). This modified bismuth quadruple therapy maintained high efficacy while demonstrating improved safety and compliance profiles compared to conventional dosing in refractory H. pylori patients. However, a meta-analysis [10] reported no significant difference in adverse events between quadruple therapies with or without minocycline (RR = 0.94, p = 0.63). Prospective and multicenter clinical trials are needed to fully establish the efficacy and safety of low-dose minocycline-containing regimens, especially in remedial treatment.
However, univariate analysis did not identify any risk factors associated with eradication failure. The optimal interval between rescue treatments has been a subject of ongoing debate. It’s reported that H. pylori might enter a non-replicative, non-culturable state with low metabolic activity after repeated eradication failures [27]. Some studies proposed that delaying retreatment for over 6 months might promote bacterial reversion to an active replicative state, potentially enhancing eradication efficacy [28]. However, our findings demonstrated no significant difference in treatment efficacy whether the interval was shorter or longer than 6 months. Recently, Lin et al. [29] investigated the association between eradication rate and treatment interval duration in a prospective observational study. Patients were stratified into four groups based on retreatment intervals (1–3 months, 3–6 months, 6–12 months, and > 12 months), yet no statistically significant differences in eradication rates were observed across groups. These findings collectively suggested that extending the interval between rescue treatments might offer no discernible clinical advantage.
The selection of sensitive antibiotics remains the most critical determinant of successful rescue treatment. Our analysis revealed that patients with prior amoxicillin exposure in both groups tended to have lower eradication rates. However, this observed difference lacked statistical significance, potentially attributable to subjects with only once treatment failure, or relatively less samples. Another notable observation is that the proportion of patients who had received dual therapy as first-line treatment was significantly higher in the VAMB group than VA group (10.4% vs. 2.8%, p = 0.021). This likely reflects a common "step-up" strategy in clinical practice, wherein patients who do not respond to first-line dual therapy are generally not retreated with the same regimen, but are instead switched to a more potent quadruple therapy as a second-line option [16]. Refractory H. pylori infection is clinically defined as persistent infection following ≥ 2 failed standard eradication attempts in China [8]. Of particular concern in this patient population is the emergence of amoxicillin resistance, with resistance rate exceeding 10% [24]. Xie et al. [30] documented particularly high secondary resistance to amoxicillin (40%, 4/10) in certain area, which significantly compromised the effectiveness of amoxicillin-based bismuth quadruple therapy. Current evidence supports two principal approaches for refractory H. pylori infection: (1) drug sensitivity-guided regimens, or (2) empirical bismuth quadruple regimens containing tetracycline, minocycline, or furazolidone.
Treatment compliance remains critical for successful eradication, with both groups in our study maintaining excellent adherence rates above 95%. Our previous research [14] demonstrated that poor compliance significantly diminished the effectiveness of a 10-day VA regimen. Consequently, in clinical practice, we strongly recommend adopting a 14-day treatment course of VA regimen to optimize therapeutic outcomes.
There were certain limitations existing in this work. First, as a retrospective investigation, the absence of long-term and frequent follow-up might introduce selection bias and potential data inconsistencies. For instance, mild or transient adverse events (such as mild rashes related to amoxicillin) may not have been systematically captured. Furthermore, the high rate of loss to follow-up (111/352, 31.5%) precluded a standard intention‑to‑treat (ITT) analysis and may compromise the completeness of safety data. A detailed review of medical records and final contact notes for these patients indicated that disengagement was primarily due to logistical and behavioral factors, including symptom resolution leading to perceived cure (> 50%), geographical or practical barriers to returning for re‑examination, and non-adherence unrelated to adverse events. Importantly, there were no documented contacts, emergency visits, or patient-reported discontinuations due to suspected adverse effects during treatment or at the final follow-up. In accordance with common practice in similar studies, the mITT population was used for the primary efficacy assessment [30, 31]. The primary purpose of ITT analysis is to preserve the comparability achieved through randomization. In this present study, however, treatment allocation was guided by clinical judgment and individual patient factors rather than randomization. Thus, the mITT approach may better approximate the true clinical effectiveness of the regimen in routine practice. Nevertheless, these constraints underscore the importance of implementing systematic, outcome‑driven follow‑up protocols in prospective studies to fully capture treatment outcomes and safety profiles [32]. Second, because the study was conducted in a tertiary referral center, the findings may be most applicable to institutions managing similarly complex patient populations; generalizability to primary care settings requires further validation. Nevertheless, treatment decisions, follow‑up, and outcome evaluation in this study all followed routine clinical pathways without research‑driven intervention, thereby preserving the study’s observational validity. Third, antibiotic susceptibility testing was not performed for those rescue patients. While current guidelines recommend tailored salvage therapies based on susceptibility results, such testing remains logistically and economically inaccessible in many clinical settings. Finally, the relatively small sample sizes in certain subgroups limited our ability to detect statistically significant differences between groups. Future large-scale, multicenter randomized controlled trials are warranted to further evaluate the efficacy and safety profiles of these regimens in second-line treatment.
In conclusion, the VA dual therapy has comparable eradication efficacy compared with the VAMB therapy in retreatment patients with H. pylori infection, and the former exhibiting a more favorable adverse event profile. Based on these results, VA dual therapy could be regarded as the preferred second-line treatment option for patients experiencing their first H. pylori treatment failure.