Intraperitoneal nivolumab for malignant ascites in patients with advanced gastrointestinal or pancreaticobiliary tract cancer
Hsiu-Tzu Wang, Yung-Luen Yu, Wen-Jyi Lo, Mei-Chen Lin, Chien-Lun Chu, Chia-Yu Chen, Sing-Ting Wang, Chang-Fang Chiu, En-Jia Bai, Li-Yuan Bai

TL;DR
This study shows that intraperitoneal nivolumab can effectively reduce malignant ascites in patients with advanced gastrointestinal or pancreaticobiliary cancer.
Contribution
The study introduces intraperitoneal nivolumab as a novel treatment for malignant ascites with minimal side effects.
Findings
Seven out of nine patients showed clinical improvement with reduced ascites and longer intervals between paracenteses.
Increased vascular endothelial growth factor A and decreased interleukin-1α levels were observed in responders.
The treatment was well-tolerated with only grade 1 tenderness at puncture sites reported.
Abstract
Malignant ascites occur in 10–15% of patients with gastrointestinal tract cancers. The abundance of immune cells in the peritoneum and ascitic fluid, along with the immunosuppressive environment created by cancer cells, suggests the potential utility of intraperitoneal (IP) immune checkpoint inhibitors for controlling malignant ascites. Patients with gastrointestinal or pancreaticobiliary tract cancer and cytologically confirmed malignant ascites received IP nivolumab. Twenty mg of nivolumab diluted in 100 mL of saline was infused into the peritoneal cavity over 10 min following paracentesis. IP treatment was repeated after each subsequent paracentesis until deemed ineffective by the treating physician, upon the occurrence of unacceptable toxicity, or discontinued at the patient’s request. This study was registered at ClinicalTrials.gov (NCT05745233). The median age of the nine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
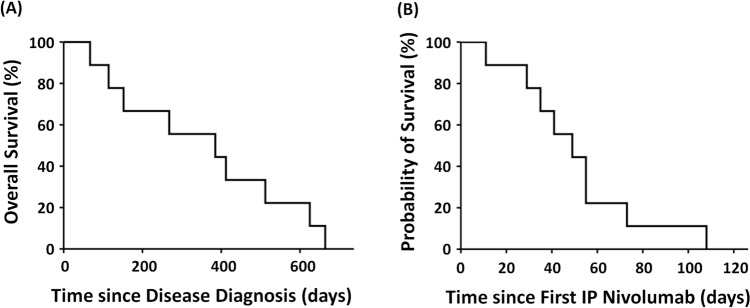 Figure 1
Figure 1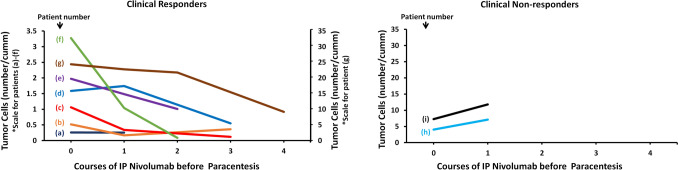 Figure 2
Figure 2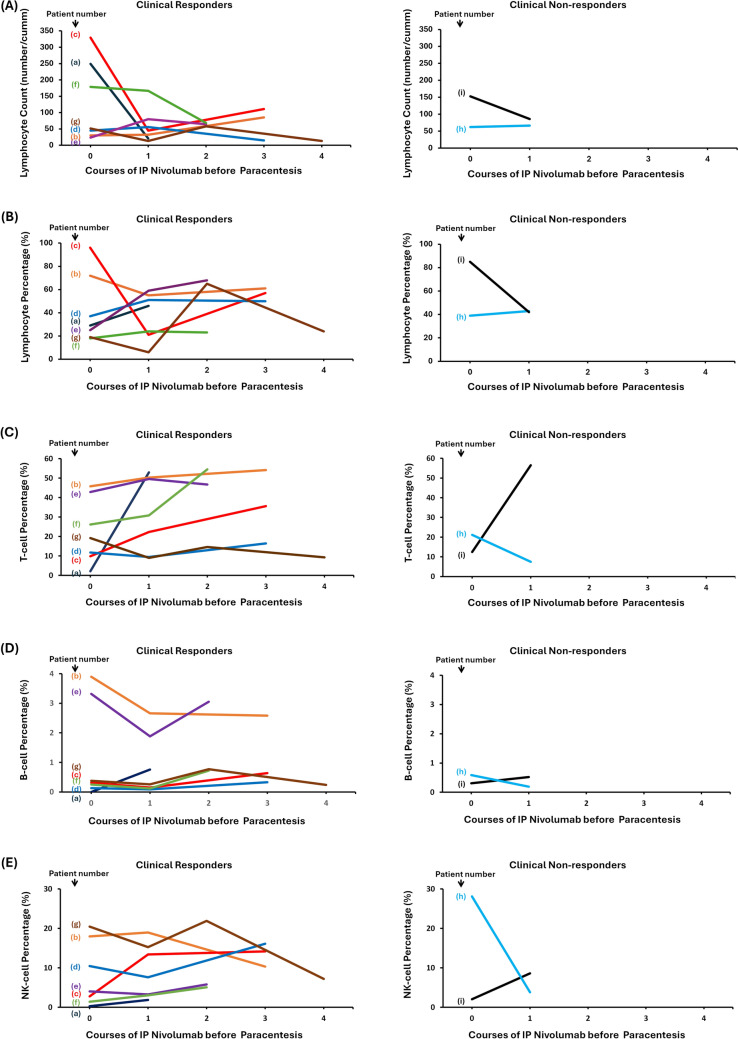 Figure 3
Figure 3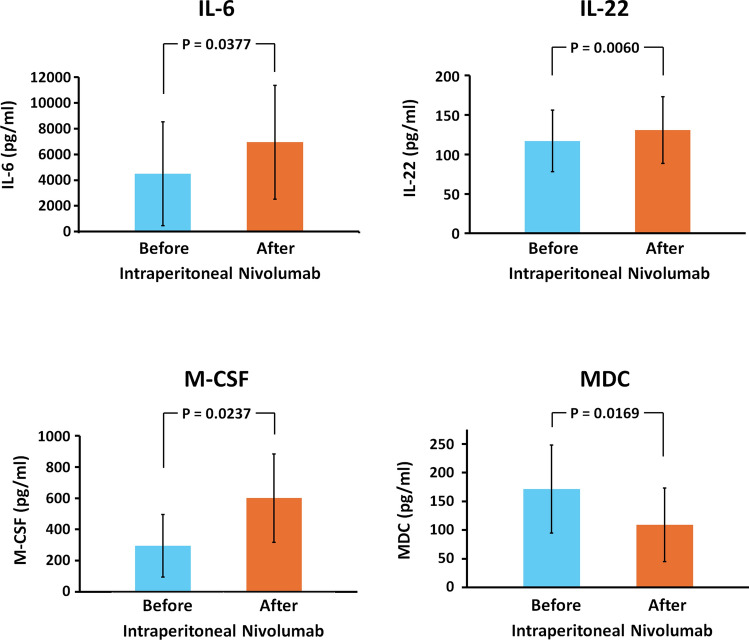 Figure 4
Figure 4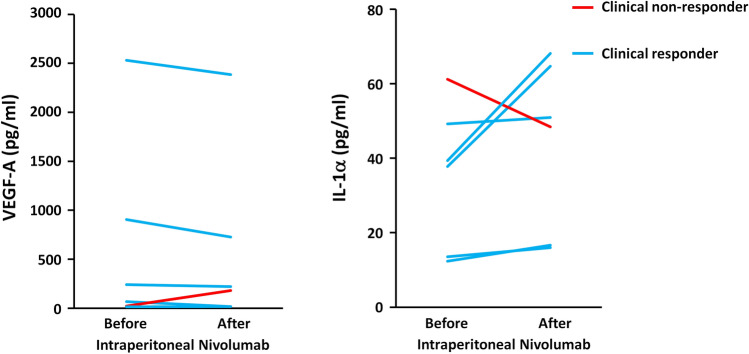 Figure 5
Figure 5- —National Health Research Institutes, Taiwan
- —China Medical University Hospital, Taiwan
- —http://dx.doi.org/10.13039/501100004663Ministry of Science and Technology, Taiwan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Pancreatic and Hepatic Oncology Research · IgG4-Related and Inflammatory Diseases
Introduction
Malignant ascites develop in 10–15% of patients with gastrointestinal cancers at some stage of the disease [1], including 8–18.3% of patients with gastric cancer [2, 3], 15–21% of those with advanced pancreaticobiliary cancers [3, 4], and approximately 4.0% of patients with esophageal cancer. Several factors contribute to the formation of malignant ascites, including obstruction of lymphatic drainage by tumor cells, altered vascular permeability, hormonal mechanisms, and sodium retention mediated by activation of the renin–angiotensin–aldosterone system [5]. Malignant ascites is associated with poor prognosis, with a median survival of 1–4 months [6]. Systemic chemotherapy is generally ineffective against malignant ascites, primarily because of inefficient intravenous drug delivery to peritoneal carcinomatosis deposits and low drug concentrations in the ascitic fluid. This unfavorable therapeutic gradient is largely attributable to high interstitial fluid pressure, caused by the dense extracellular matrix surrounding cancer cells and the disorganized vasculature resulting from tumor angiogenesis [7, 8]. These immature and hyperpermeable blood vessels not only promote ascites accumulation but also increase interstitial pressure, thereby impeding the penetration of anticancer drugs and immune cells into the tumor microenvironment [9, 10].
Management options for malignant ascites include dietary modifications, diuretics, on-demand paracentesis, drainage catheter implantation, peritoneovenous shunting, intraperitoneal (IP) chemotherapy [11, 12], IP administration of picibanil (OK-432) [13–15], cytoreductive surgery combined with hyperthermic IP chemotherapy [16, 17], and systemic anticancer therapies. IP therapy offers several advantages, including high local concentrations of anticancer drugs, direct exposure of free cancer cells and metastatic nodules on the peritoneal surface, and reduced systemic toxicity. However, the response rates are variable and often temporary. Additionally, some IP therapies are associated with significant adverse effects, such as bowel surface toxicity, abdominal pain, peritonitis, and catheter obstruction [13, 18].
The peritoneum is considered a lymphoid organ with distinct immunological characteristics [19], containing abundant dendritic cells (DCs), a predominance of CD8 + over CD4 + T cells, and various soluble immunomodulatory factors [20, 21]. However, in patients with malignant ascites, cancer cells disseminated across the peritoneum can inactivate DCs, induce T cell exhaustion, and overexpress programmed cell death ligand 1 (PD-L1), thereby evading cytotoxic T cell responses [20, 22, 23]. In addition, angiogenic factors promote the accumulation of regulatory T cells and suppress effector T cell functions [24]. Together, tumor-driven angiogenesis and the upregulation of immune checkpoints such as programmed cell death protein 1 (PD-1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) by cancer cells contribute to a highly angiogenic and immunosuppressive microenvironment [10]. These findings support the rationale for IP immunotherapy as a strategy to restore anticancer immune activity and overcome immune evasion. However, prior clinical studies of IP immunotherapy using agents such as tumor necrosis factor (TNF) or interferon have yielded inconsistent ourcomes [25]. Immune checkpoint inhibitors (ICIs) activate immune cells with anticancer properties, including cytotoxic T cells, natural killer cells, and macrophages. Theoretically, IP administration of ICIs represents an appealing strategy for treating malignant ascites, considering the distinct immunological features of the peritoneum and ascitic fluid.
We previously reported a case of a pancreatic cancer patient with refractory malignant ascites who responded favorably to IP nivolumab administration [26]. Building on this observation, we prospectively treated additional patients with malignant ascites and analyzed the ascitic fluid using flow cytometry to assess the immunological impact and clinical efficacy of IP ICIs. Here, we present the findings of nine patients treated with IP nivolumab.
Patients and methods
Patients
This prospective study was conducted at China Medical University Hospital between January 1, 2021, and January 31, 2023. Patients with gastrointestinal or pancreaticobiliary tract cancer and massive malignant ascites were eligible for screening. The presence of malignant ascites should be confirmed cytologically or pathologically. The study protocol was approved by the Research Ethics Committee of China Medical University and Hospital, Taichung, Taiwan (CMUH107-REC1-180). This study was registered at ClinicalTrials.gov (NCT05745233).
Treatments
Patients with symptomatic ascites who fulfilled the inclusion criteria underwent paracentesis as clinically indicated. During paracentesis, 20 mL of ascitic fluid was collected for flow cytometry and cytokine analysis. After paracentesis, patients were administered an IP infusion of nivolumab (20 mg diluted in 100 mL saline) over 10 min. The paracentesis catheter was removed immediately after nivolumab infusion was completed. After paracentesis, patients remained in bed with position changes every 20 min for 2 h: supine, on the right side, supine, on the left side, head high and feet low, and head low and feet high. Ascites was assessed by the treating physicians. Responders were defined as patients with increased paracentesis interval, whereas non-responders were patients were defined as patients with decreased paracentesis interval. IP treatment was repeated after each subsequent paracentesis until the treatment was deemed ineffective by the treating physician, unacceptable toxicity occurred, or stopped at the patient’s request.
Evaluation of toxicity
Physical examination, blood pressure, heart rate, and respiratory rate were recorded before and after each paracentesis and IP infusion of nivolumab. Any adverse events were documented and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 5.0.
Analysis of the cellular components of ascites
The cellular components of 20 mL of ascitic fluid, obtained during paracentesis, were analyzed using flow cytometry. Briefly, cells were concentrated by centrifuging the fluid at 2,000 rpm for 10 min. The resulting cell pellets were washed with 3 mL of phosphate-buffered saline (PBS) containing 0.2% bovine serum albumin (BSA) and centrifuged three times. The final pellet was resuspended in 100 µL of PBS with 0.2% BSA. The cells were stained with the following antibodies: CD45 (2D1, Horizon V500, BD Biosciences), CD44 (L178, fluorescein isothiocyanate [FITC], BD Biosciences), CD24 (ML5, APC-H7, BD Biosciences), CD71 (YDJ1.2.2, APC-A750, Beckman Coulter), CD200 (OX104, APC, Invitrogen), and CD326 (epithelial cell adhesion molecule [EpCAM], EBA-1, phycoerythrin [PE], BD Biosciences). The samples were incubated in the dark at 25 °C for 30 min. Erythrocytes were lysed using 2 mL of BD FACS™ Lysing Solution (BD Biosciences). For intracellular staining, cells were then fixed and permeabilized using the FIX & PERM™ Cell Permeabilization Kit (Invitrogen™), following the manufacturer’s instructions, and stained with anti-human cytokeratin-7/−8 antibody (CAM5.2, Brilliant Violet™ 421 [BV421], BD Biosciences). Finally, stained cells were washed once with PBS, resuspended in 200 µL of PBS containing 0.2% BSA, and analyzed using a BD FACSLyric™ cytometer (BD Biosciences, CA). Cancer cells were identified as CD45 −/EpCAM +/Cytokeratin +/CD44 +/CD24 +/CD71 +/CD200 −. Mesothelial cells were excluded based on CD200 expression.
Analysis of cytokines of ascites
Ascitic fluid samples from six patients (five clinical responders and one non-responder) were available for cytokine analysis both before and after IP administration of nivolumab. Paired ascites samples were analyzed for 19 cytokines, including: epidermal growth factor (EGF), fibroblast growth factor 2 (FGF-2), granulocyte colony-stimulating factor (G-CSF), interferon α 2 (IFNα2), interferonγ (IFNγ), interleukin 1α (IL-1α), interleukin 1β (IL-1β), interleukin 2 (IL-2), interleukin 6 (IL-6), interleukin 12p70 (IL-12p70), interleukin 22 (IL-22), monocyte chemoattractant protein-1 (MCP-1), monocyte chemoattractant protein-3 (MCP-3), macrophage colony-stimulating factor (M-CSF), macrophage-derived chemokine (MDC), macrophage inflammatory protein-1α (MIP-1α), macrophage inflammatory protein-1β (MIP-1β), vascular endothelial growth factor A (VEGF-A), and soluble CD40 ligand (sCD40L). Cytokine levels were measured using the Milliplex® Human Cytokine/Chemokine/Growth Factor Magnetic Bead Panel A/B (Merck KGaA, Darmstadt, Germany), according to the manufacturer’s protocol. All cytokines were measured in triplicate for each sample.
Statistical analysis
The outcome measure was the clinical response of ascites, defined as a reduction in ascitic fluid volume and a prolonged interval between paracenteses following IP nivolumab treatment. Duration of response was defined as the time interval from the initiation of IP nivolumab until it was deemed ineffective by the treating physician, upon the occurrence of unacceptable toxicity, or stopped at the patient’s request. All statistical analyses were performed using Statistical Product and Service Solutions version 26 for Windows (IBM Corporation, Armonk, NY, USA), with two-sided p-values < 0.05 considered statistically significant.
Results
Patient characteristics
Between January 1, 2021, and January 31, 2023, nine patients with malignant ascites secondary to gastrointestinal or pancreaticobiliary tract cancers received IP nivolumab therapy (Table 1). The underlying malignancies included pancreatic cancer in four patients, biliary tract cancer in three, and gastric cancer in two. All patients had previously received systemic therapy for their underlying disease, except for patient number (b). No patient had received any form of local therapy for ascites or pleural effusion. Table 1. Characteristics of patients and ascites contentPatientAge (years)SexUnderlying diseaseOther metastatic sitePrior systemic anticancer therapiesPrior local treatment for ascitesSystemic Tx prior to IP NivoSystemic Tx cocurrent IP NivoSystemic Tx post to IP NivoCancer cells in ascites before first IP (/cumm)Neutrophils in ascites before first IP (%)Lymphocytes in ascites before first IP (%)Lymphocytes in ascites before first IP (/cumm)a55MPC–2NoGem + Aliposomal irinotecan + 5-FU––0.2585929249.4b53FPCliver1NoDCV––0.51797230.2c52FPC–2NomFOLFIRINOXGem + Aliposomal irinotecan + 5-FU × 3–1.063296329.3d71MBTClymph nodes1NoGem + A + cisplatinliposomal irinotecan + 5-FU––1.58643745.1e53FPC–1NoGem + A + oxaliplatinliposomal irinotecan + 5-FU × 1–1.97612523.8f71FBTCliver3NoGem + cisplatinpembrolizumab + lenvatinibLOXO LY3410738––3.277718178.7g55MGC–3Nocapecitabine + oxaliplatindocetaxel + ramucirumabFOLFIRI––24.381281951.3h48FGC–1NoNivolumab + mFOLFOX7docetaxel + ramucirumab––4.016113962.4i69MBTC–1NoGem + TS-1––7.254785153PatientN/L in ascites before first IPCancer cells in ascites before first IP (/cumm)Neutrophils in ascites before first IP (%)Lymphocytes in ascites before first IP (%)Lymphocytes in ascites before first IP (/cumm)N/L in ascites before first IPClinical responseTotal cycles of IPDuration of treatment (days)Cause of terminationOS (diagnosis to death, days)OS (first IP to death, days)a2.00.2585929249.42.0Yes228Patient’s wish38535b0.10.51797230.20.1Yes448Expire due to disease11449c0.01.063296329.30.0Yes564Expire due to disease412108d0.11.58643745.10.1Yes338Patient’s wish62555e0.01.97612523.80.0Yes229Expire due to disease15255f0.43.277718178.70.4Yes340Expire due to disease51241g1.524.381281951.31.5Yes537Expire due to disease26829h0.34.016113962.40.3No219Uncontrolled ascites66473i0.17.2547851530.1No210Uncontrolled ascites6711A Nab-paclitaxel, BTC Biliary tract cancer, DCV Dendritic cell vaccine, F Female, 5-FU 5-Fluorouracil, GC Gastric cancer, Gem gemcitabine, IP Intraperitoneal, L Lymphocyte, M Male, N Neutrophil, PC Pancreatic cancer, Tx Treatment
The cellular components of ascitic fluid were analyzed by flow cytometry. At baseline, the median cancer cell count was 1.976 (range: 0.258–24.381) cells/µL. The median neutrophil proportion was 7% (range: 1–59%), while the median lymphocyte proportion was 37% (range: 18–96%) with an absolute lymphocyte count of 62.4 (range: 23.8–329.3) cells/µL. The median neutrophil-to-lymphocyte ratio in the ascitic fluid was 0.1 (range: 0–2.0) (Table 1).
Treatment
All patients received a second dose of IP nivolumab based on symptoms of abdominal fullness, which ranged from 3 to 21 days. The median number of treatment cycles was three (range: 2–5) (Table 1).
All patients tolerated IP nivolumab well. No cases of fever, abdominal cramping, nausea, vomiting, or allergic reactions were observed. The only adverse event was grade 1 tenderness at the puncture sites.
Therapeutic efficacy
Of the nine patients, seven achieved a clinical response, as evidenced by a reduction in ascites volume and a prolonged interval between paracentesis following IP nivolumab treatment [patients (a) to (g)]. In contrast, ascites in two patients did not respond, and IP therapy was discontinued after two treatment cycles in patients (h) and (I) (Table 1).
The median number of treatment cycles and duration of IP treatment were 3 and 37 days (range: 10–64 days), respectively. Among clinical responders, IP nivolumab was discontinued due to disease progression and death in five patients and upon patient request in two. The median overall survival from disease diagnosis and from the start of IP nivolumab was 385 days and 49 days, respectively (Fig. 1).Fig. 1. Kaplan–Meier curves for overall survival. A From the date of disease diagnosis. B From the date of the first intraperitoneal nivolumab
Tumor cells in ascites decreased in clinical responders
Tumor cell count, neutrophil count, lymphocyte count, and the neutrophil-to-lymphocyte ratio in ascites were analyzed in relation to clinical response. Tumor cell counts decreased in six of the seven clinical responders, except in patient (a). Conversely, increased tumor cell counts were observed in both non-responders (Fig. 2). Changes in total lymphocyte count (Fig. 3A), lymphocyte percentage (Fig. 3A), T cell percentage (Fig. 3C), B cell percentage (Fig. 3D), and natural killer cell percentage (Fig. 3E) in ascites did not correlate with the clinical response.Fig. 2. Time course of tumor cell counts in ascites before and after intraperitoneal administration of nivolumab. The left and right panels represent data from seven clinical responders and two clinical non-responders, respectively. Each line represents an individual patient. Tumor cells were analyzed using ascitic fluid collected prior to each administration of intraperitoneal nivolumabFig. 3Changes in lymphocyte count (A), lymphocyte percentage (B), T cell percentage (C), B cell percentage (D), and natural killer (NK) cell percentage (E) in ascites before and after intraperitoneal nivolumab administration. The left and right panels represent data from seven clinical responders and two clinical non-responders, respectively. Each line represents an individual patient. Immune cells were analyzed using ascitic fluid collected prior to each course of intraperitoneal nivolumab
Cytokine changes in ascites in clinical responders vs. non-responders
The concentrations of 19 cytokines in ascitic fluid before and after IP nivolumab administration were compared (Supplementary Fig. 1). Among these, IL-6, IL-22, and M-CSF showed significant increases following treatment, while MDC levels decreased (Fig. 4). However, notable interpatient variability was observed.Fig. 4. Levels of interleukin 6 (IL-6), interleukin 22 (IL-22), macrophage colony-stimulating factor (M-CSF), and macrophage-derived chemokine (MDC) in ascites before and after intraperitoneal nivolumab administration. Data represent the mean ± standard deviation of three independent experiments
Cytokine profiles were compared between responders and non-responders to assess the relationship between cytokine changes and the clinical response. VEGF-A and IL-1α exhibited consistent trends that distinguished clinical responders from the non-responder (Fig. 5). All five responders showed a decrease in VEGF-A levels, whereas non-responders exhibited an increase following IP nivolumab treatment. Conversely, IL-1α levels increased in the ascites of all clinical responders, in contrast to a decrease observed in the non-responder.Fig. 5. Levels of vascular endothelial growth factor A (VEGF-A) and interleukin 1α (IL-1α) in ascites before and after intraperitoneal nivolumab administration. Each line represents an individual patient
Discussion
This prospective analysis of nine patients with gastrointestinal or pancreaticobiliary tract cancer demonstrated for the first time that IP nivolumab is effective in controlling malignant ascites, with a clinical response rate of 77%. Notably, the treatment was well tolerated, with no reports of abdominal pain, fever, gastrointestinal upset, or allergic reactions, except mild local tenderness at the site of paracentesis catheter insertion. A reduction in the number of cancer cells in ascitic fluid correlated well with clinical response, underscoring the potential of IP immune checkpoint inhibitors.
Given the unique immune characteristics of the peritoneal cavity and the abundance of anticancer immune cells in ascites, IP immunotherapy has been actively explored since the 1980 s, with varying degrees of success. Agents previously investigated include the immune-stimulator picibanil [13–15], interferon [21, 27], TNF [25], and monoclonal antibodies such as mouse IgG1 targeting the EpCAM [28]. IP administration of picibanil, a penicillin-inactivated, heat-treated preparation of Streptococcus pyogenes A3 designed to stimulate NK and T cells, resulted in ascites reduction in 50–70% of patients [13–15]. However, its use is often limited by intolerable adverse effects, with over 90% of patients experiencing abdominal cramping, fever, chills, bowel distention, nausea, and vomiting.IP administration of TNF or interferon has been proposed to enhance the activity of cytotoxic immune cells within the peritoneal cavity. However, their clinical application remains controversial due to notable adverse effects [21, 25, 27].
ICIs have demonstrated anticancer activity against a broad range of malignancies. IP infusion of ICIs directly targets the peritoneal cavity and has the potential to enhance local immune responses. Both pembrolizumab and nivolumab have been administered intraperitoneally in murine tumor models without evident toxicity [29]. In particular, nivolumab was reported to be substantially more effective than dacarbazine in controlling peritoneal metastases of malignant melanoma in mouse models [30]. To date, the IP administration of ICIs for treating malignant ascites has not been established [26, 31, 32]. A phase I trial investigated the combination of IP ipilimumab and nivolumab in 23 patients with peritoneal carcinomatosis secondary to gynecological malignancies [31]. The overall response rate was 18.8% in 16 evaluable patients. Grade ≧3 immune-related adverse events occurred in 2 (8.7%) patients, and the recommended phase 2 dose was nivolumab at 3 mg/kg every 2 weeks plus ipilimumab at 1 mg/kg every 6 weeks. Another phase I/II trial assessed IP nivolumab after debulking surgery and hyperthermic IP chemotherapy in patients with advanced ovarian carcinoma [32]. Of the 17 patients who received treatment, no dose-limiting toxicity was observed in 9 evaluable patients. Therefore, IP nivolumab at 3 mg/kg should be investigated in future studies. The target population in our cohort was different from that of the two studies. In addition, we performed an analysis of ascitic fluid. Although preliminary, these two publications, along with our report, suggest the feasibility and promising role of IP ICIs in patients with cancer.
The VEGF-A levels in ascites were consistently lower in clinical responders than in the non-responder (Fig. 5). VEGF, released by tumor cells, is a well-recognized factor promoting ascites formation [33]. Consequently, several studies have explored the therapeutic potential of anti-VEGF antibodies in managing malignant ascites [33, 34]. Conversely, IL-1α levels in ascites consistently increased in clinical responders, in contrast to the non-responders. IL-1α, produced by epithelial cells, endothelial cells, activated macrophages, and neutrophils, plays a central role in inflammation. Its in vivo functions include promoting collagen synthesis, stimulating fibroblast proliferation, increasing neutrophil recruitment, activating lymphocytes, stimulating the immune system, and inducing fever [35]. Therefore, the observed increase in IL-1α among responders suggests an immune-activating environment induced by intraperitoneal nivolumab.
This study has several limitations. First, this was a small prospective analysis involving only nine patients. The limited cohort not only restricts the statistical power but also undermines the reliability of subgroup analyses, such as cytokine profiling and tumor cell quantification. In the future, the potential of IP ICIs should be validated in larger cohorts using a control arm. Second, there was no standardized interval for paracentesis and IP ICIs; instead, the treatment timing was based on patients’ symptoms. In our study, patients had advanced gastrointestinal or pancreaticobiliary tract cancer, developed symptomatic malignant ascites, and were refractory to or refused standard of systemic anticancer treatment. Our goal was to improve symptoms caused by malignant ascites in hospice care for which paracentesis/IP nivolumab was administered in a symptom-driven manner. However, we acknowledge that a study adopting a protocol-defined administration pattern would be more robust and is essential to determine the value of IP ICIs. Third, we did not analyze predictive biomarkers at baseline to identify patients most likely to benefit from this treatment owing to the limited number of patients. Fourth, the pharmacokinetic of nivolumab in systemic circulation were not assessed. Given the potential for systemic immune activation by absorbed nivolumab from ascites, the future studies should include pharmacokinetic analysis of nivolumab in the systemic circulation.
Conclusion
IP administration of ICIs appears to be a safe, effective, and quality-of-life-preserving approach for managing malignant ascites in patients with gastrointestinal or pancreaticobiliary tract cancers. Further studies involving larger patient cohorts, malignancies of diverse origins, and biomarker investigations are required to validate and expand upon these findings.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (TIF 789 KB)