Bridging the Knowledge and Training Gap Between Educational Needs and Practices of Orthodontists and General Dental Practitioners Towards Clear Aligner Therapy in India: A Cross-Sectional Survey Study
Greeshma Gothankar, Sunil Kumari, Jitender Machawal, Garima Arora, Shailendra Singh Rana

TL;DR
This study explores the knowledge and training gaps among Indian dental professionals regarding clear aligner therapy, highlighting the need for targeted education to improve adoption and patient care.
Contribution
The study identifies specific educational and practical barriers to clear aligner therapy adoption among orthodontists and general dentists in India.
Findings
41.1% of participants reported no clinical experience with clear aligner therapy despite having access to systems.
Cost and patient compliance were identified as the major barriers to adopting clear aligner therapy.
Most practitioners expressed willingness to pursue further training in clear aligner therapy.
Abstract
Background: Clear aligner therapy (CAT) has rapidly evolved as a preferred orthodontic treatment option due to its aesthetic appeal, comfort, and removability. Despite increasing availability, variability exists in practitioners' knowledge, attitudes, and practical application of CAT. Objective: This study aimed to determine the knowledge and demand for CAT education amongst practitioners so as to offer insights for future tailored curricula on CAT. Methods: A cross-sectional survey was conducted among 112 licensed orthodontists and general dentists. Data were collected using a validated, self-administered questionnaire that focused on CAT-related knowledge, attitudes, practices, and training needs. Descriptive and inferential statistics were analyzed using SPSS Version 26 (IBM Corp., Armonk, NY, USA), with significance set at p < 0.05. Results: Participants had a mean age of 33.97…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
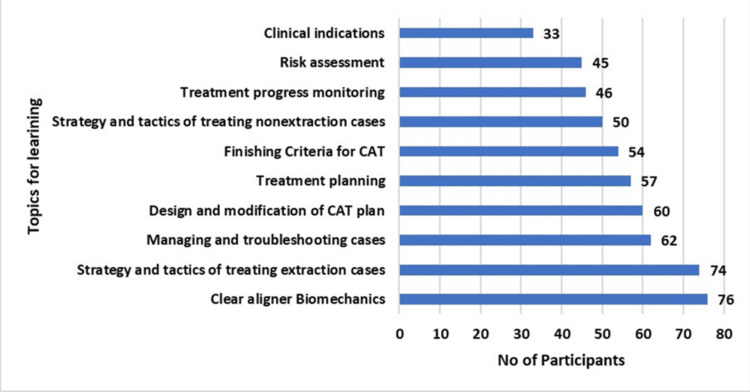 Figure 1
Figure 1| Variable | Frequency (n = 112) | Percentage (%) |
| Gender | ||
| Female | 50 | 44.64 |
| Male | 62 | 55.36 |
| Age | ||
| < 30 | 37 | 33.04 |
| 30 to 35 | 39 | 34.82 |
| > 35 | 36 | 32.14 |
| Occupation | ||
| Orthodontist | 89 | 79.46 |
| General Dentist | 23 | 20.54 |
| Working Sector | ||
| Private | 79 | 70.54 |
| Government | 23 | 20.54 |
| Semi-Government | 5 | 4.46 |
| PG Student | 5 | 4.46 |
| Experience (Years) | ||
| 0 to 1 | 20 | 17.86 |
| 2 to 5 | 51 | 45.54 |
| > 5 | 41 | 36.61 |
| Variable | Frequency (n = 112) | Percentage (%) |
| Experience using CAT (in years) | ||
| 0 | 46 | 41.07 |
| 1 to 2 | 38 | 33.93 |
| 2 to 4 | 18 | 16.07 |
| > 4 | 10 | 8.93 |
| Training in CAT | 68 | 60.71 |
| Access to a clear CAT in the Clinic | 64 | 57.14 |
| The CAT System used in the clinic. | ||
| Other | 70 | 62.50 |
| Invisalign | 50 | 44.64 |
| Clear Correct | 10 | 8.93 |
| Spark | 8 | 7.14 |
| Direct Printed CAT | 4 | 3.57 |
| Challenges faced in using CAT | ||
| Cost | 87 | 77.7 |
| Compliance | 52 | 46.4 |
| Training | 42 | 37.5 |
| Case Selection | 35 | 31.3 |
| Questions | Variables | Access to clear aligner systems | P Value | Chi-Square | Cramér’s V Effect Size | |
| Yes (n=64) | No (n=48) | |||||
| CAT is best suited for | Minor/Moderate Malocclusion | 63 | 45 | 0.186 | 4.813 (df=3) | 0.185 |
| None of the above | 0 | 2 | ||||
| Severe skeletal malocclusion | 1 | 0 | ||||
| TMD cases | 0 | 1 | ||||
| Material is commonly used in CAT | None of the above | 4 | 2 | 0.860 | 2.574 (df=3) | 0.152 |
| PMMA | 11 | 8 | ||||
| Polycarbonate | 6 | 4 | ||||
| Polyurethane | 43 | 34 | ||||
| Treatment with CAT requires fewer visits | No | 5 | 9 | 0.083 | 3.000 (df=1) | 0.163 |
| Yes | 59 | 39 | ||||
| NOT a clear CAT brand | Damon | 43 | 35 | 0.621 | 1.771 (df=3) | 0.125 |
| Demon | 18 | 12 | ||||
| Invisalign | 1 | 1 | ||||
| Spark | 2 | 0 | ||||
| Attachments or auxiliaries used with CAT | No | 2 | 1 | 0.399 | 1.838 (df=2) | 0.128 |
| Not Sure | 1 | 3 | ||||
| Yes | 61 | 44 | ||||
| I believe CAT are as effective as braces | Strongly Agree | 17 | 5 | 0.251 | 5.377 (df=4) | 0.155 |
| Agree | 24 | 19 | ||||
| Neutral | 13 | 12 | ||||
| Disagree | 9 | 10 | ||||
| Strongly Disagree | 1 | 2 | ||||
| CAT is important for modern dental practice | Strongly Agree | 29 | 17 | 0.096 | 4.686 (df=2) | 0.145 |
| Agree | 32 | 23 | ||||
| Neutral | 3 | 8 | ||||
| I feel confident explaining CAT to patients | No | 4 | 11 | 0.000 | 15.763 (df=2) | 0.266 |
| Sometimes | 9 | 16 | ||||
| Yes | 51 | 21 | ||||
| I am open to integrating CAT into my routine practice | Maybe | 5 | 8 | 0.340 | 2.159 (df=2) | 0.139 |
| No | 2 | 1 | ||||
| Yes | 57 | 39 | ||||
| Cost is a major barrier to adopting CAT | Strongly agree | 23 | 27 | 0.177 | 4.927 (df=3) | 0.149 |
| Agree | 32 | 17 | ||||
| Neutral | 6 | 2 | ||||
| Disagree | 3 | 2 | ||||
| I prefer fixed orthodontic appliances over CAT | Depends on the case | 43 | 22 | 0.034 | 6.777 (df=2) | 0.195 |
| No | 3 | 1 | ||||
| Yes | 18 | 25 | ||||
| I would attend training if offered locally or online | Maybe | 8 | 4 | 0.523 | 1.296 (df=2) | 0.108 |
| No | 1 | 0 | ||||
| Yes | 55 | 44 | ||||
| Learn treatment planning and biomechanics in CAT | Maybe | 3 | 3 | 0.914 | 0.179 (df=2) | 0.040 |
| No | 1 | 1 | ||||
| Yes | 60 | 44 | ||||
| CAT cases treated per month | 0 | 10 | 36 | 0.000 | 42.193 (df=3) | 0.434 |
| 1-2 | 35 | 11 | ||||
| 2-4 | 10 | 0 | ||||
| >4 | 9 | 1 | ||||
| Digital impressions for CAT cases | No | 5 | 19 | 0.000 | 26.675 (df=2) | 0.388 |
| Outsourced | 5 | 11 | ||||
| Yes | 54 | 18 | ||||
| Follow up every 4–6 weeks during CAT | No | 6 | 18 | 0.000 | 15.225 (df=2) | 0.262 |
| Occasionally | 9 | 9 | ||||
| Yes | 49 | 21 | ||||
| Educate patients about CAT options | Always | 47 | 18 | 0.000 | 16.257 (df=2) | 0.269 |
| Never | 0 | 3 | ||||
| Sometime | 17 | 27 | ||||
| Offer clear CAT therapy | No | 5 | 30 | 0.000 | 38.182 (df=1) | 0.583 |
| Amount is possible only with CAT | 0 mm | 1 to 2 mm | 2 to 4 mm | > 4 mm | Do not know |
| Intrusion | 1 (0.9) | 76 (67.9) | 31 (27.7) | 2 (1.8) | 9 (8.0) |
| Extrusion | 14 (12.5) | 70 (62.5) | 19 (17.0) | 3 (2.7) | 12 (10.7) |
| Molar distalization | 6 (5.4) | 48 (42.9) | 54 (48.2) | 5 (4.5) | 10 (8.9) |
| Molar mesialization | 17 (15.2) | 62 (55.4) | 23 (20.5) | 4 (3.6) | 13 (11.6) |
| Arch expansion | 2 (1.8) | 44 (39.3) | 47 (41.9) | 9 (8.1) | 10 (8.9) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Dental Education, Practice, Research · Dental Research and COVID-19
Introduction
Clear aligner therapy (CAT) is a removable and aesthetic alternative to conventional fixed appliances. It can treat a wider range of malocclusions due to continuous improvements in aligner materials, digital workflows, and three-dimensional treatment planning [1,2]. Despite this, acceptance of CAT varies and depends on practitioners’ knowledge, clinical training, and confidence in aligner systems. Although the brands such as Invisalign, Spark and Clear-Correct are easily available in the market, their successful utilization requires thorough knowledge of case selection, biomechanics, and patient management [3]. In India, undergraduate and postgraduate orthodontic curricula continue to focus on traditional fixed appliance therapy, with limited importance to aligner-based treatment modalities [4]. This educational limitation may contribute to inconsistent levels of knowledge and variable clinical utilization of CAT among practitioners. Some practitioners use aligners, whereas others still follow specifically conventional fixed braces due to the high cost of aligners, patient compliance issues, or a lack of experience [5]. Assessing these differences through a structured knowledge, attitude, and practice (KAP) framework provides valuable insights into practitioners’ preparedness and the barriers to broader adoption [6].
Although international studies have explored dental professionals’ perceptions of aligner therapy, there is limited evidence from India addressing these parameters. Therefore, this study aimed to determine the knowledge and demand for CAT education among orthodontists and general dental practitioners in India so as to offer insights for future tailored curricula on CAT. Identifying existing gaps will also help inform targeted continuing dental education programs and facilitate evidence-based integration of aligner therapy into modern orthodontic practice [7].
Materials and methods
Study design and participants
This study employed a cross-sectional, descriptive survey design to evaluate the knowledge, attitudes, practices, and educational demands of orthodontic practitioners regarding Clear Aligner Therapy (CAT). The survey was carried out using an online, closed-ended questionnaire, administered via Google Form for broad geographic coverage. The target population comprised licensed orthodontic practitioners and general dentists involved in orthodontic care. Ethical approval was obtained from the Institutional Review Board before study commencement. The ethical approval number was (MRIIRS/MRDC/SDS/IEC/2025/114). Informed consent was obtained from all participants, and confidentiality of responses was strictly maintained throughout the study.
Inclusion and exclusion criteria
Licensed orthodontists and postgraduate students or general dentists involved in orthodontic treatment who were willing to participate voluntarily and gave informed consent were included in the study. Undergraduate or interns and Incomplete survey responses were excluded from the study.
Sample size determination
The sample size was calculated using the formula for estimating proportions with a 95% confidence level, assuming a prevalence of 50% to maximize the sample size and a margin of error of 10%. This calculation yielded a minimum required sample size of 97 participants. To account for a potential 10% non-response rate, the sample size was increased to 107 participants to ensure adequate statistical power and representativeness. A convenience sampling method was employed, inviting orthodontic practitioners from various clinical settings, including private practices, government institutions, and academic centers, to participate in the study.
Survey instrument
A structured and validated questionnaire was developed for online distribution. It was divided into five sections:
Section A: Demographic and professional details (e.g., age, gender, years of experience, specialty, and practice setting).
Section B: Knowledge-based questions related to CAT, such as clinical indications, materials used, biomechanics, and treatment protocols.
Section C: Assessment of attitudes towards the adoption and effectiveness of CAT, using a five-point Likert scale.
Section D: Practice-oriented queries, including frequency of aligner usage, system preference, patient management, and challenges encountered.
Section E: Evaluation of learning needs related to CAT, including treatment planning, case selection, and interdisciplinary approaches.
The questionnaire was reviewed for content validity by three subject experts in orthodontics. A pilot test involving 10 respondents was conducted to assess clarity, relevance, and reliability, following which necessary modifications were made. The Item-level Content Validity Index (I-CVI) values ranged from 0.80 to 1.00, and the Scale-level CVI (S-CVI/Ave) was 0.93, indicating excellent content validity of the instrument.
Data collection and analysis
The finalized questionnaire was converted into an online format using Google Forms and disseminated through professional dental networks, email groups, and social media platforms like WhatsApp and LinkedIn. The survey link was accompanied by an introductory statement explaining the study’s purpose, voluntary participation, and confidentiality assurance. Participants provided informed consent before accessing the questionnaire. Measures were taken to prevent multiple submissions and maintain the anonymity of respondents.
Data were automatically recorded in Google Sheets and then exported to Microsoft Excel for cleaning and coding, and the analysis was conducted using SPSS Version 26 (IBM Corp., Armonk, NY, USA). The descriptive analysis was done, and the data were presented in terms of frequency and percentage. Wherever required, the mean and median were calculated. The comparison was done using the Chi-Square test, and a P-value of less than 0.05 was considered significant.
Results
The questionnaire was distributed to 125 practitioners via social media and email, of whom 112 participants responded. A total of 112 practitioners participated in the study. The demographic characteristics of the respondents are summarized in Table 1. Experience with clear aligner therapy, including training status, access to aligner systems, and challenges encountered in clinical use, is presented in Table 2. Responses related to practitioners’ knowledge, attitudes, and practices toward clear aligner therapy are detailed in Table 3. Practitioners’ understanding of the magnitude of tooth movements achievable using clear aligners is summarized in Table 4. Areas identified by participants for further learning and training are illustrated in Figure 1. All the participants (100%) agreed that patient compliance is essential for success in CAT therapy.
Topics for further learning and training
Discussion
This study offers a broad examination of orthodontists ' and dental practitioners' current knowledge, attitudes, behaviors, and educational needs, highlighting key gaps between awareness and clinical application. Although various unambiguous aligner systems are readily accessible, our data show that a substantial number of practitioners (41.1%; n = 46) acknowledged having no previous clinical experience with CAT, despite over 60% having attended training. This discrepancy underscores a disconnection between theoretical understanding and hands-on proficiency, an issue repeatedly noted in global literature [8,9].
In 75% respondents were orthodontists, and others were general practitioners. Given the expanding accessibility of aligner systems and company-led training programs, CAT is increasingly being practiced not only by orthodontists but also by general dental practitioners. In India, where many patients first consult general dentists for orthodontic concerns, their awareness and clinical readiness directly influence treatment uptake and outcomes. Therefore, including both orthodontists and dental practitioners provides a comprehensive assessment of current knowledge, attitudes, and practices related to aligner therapy across diverse clinical settings [9]. Two principal barriers, cost and patient compliance, emerged as the dominant constraints affecting aligner adoption. Nearly three-quarters of the participants cited cost as the main reason for the delayed adoption of aligners in both public and private clinical settings. Likewise, patient compliance remains pivotal given the removable nature of aligners, which, while enhancing comfort and hygiene, places treatment success heavily on patient adherence. These findings are similar to earlier studies emphasizing the behavioral and economic determinants of CAT uptake [10-12]. Clinically, most participants recognized CAT as best suited for mild to moderate malocclusions; these findings corroborate a systematic review that found aligners are less effective in complex cases requiring precise root control or extrusion [13]. From an educational perspective, the study reveals an urgent need for structured, skill-oriented training programs focusing on topics like appropriate case selection and treatment planning, clear aligner biomechanics and tooth movement predictability, digital workflow integration, and managing relapse and troubleshooting refinements. Most participants expressed a strong desire for additional CAT-related training [14-16].
An important dimension of CAT adoption in India is the growing influence of commercial aligner companies, particularly systems such as Invisalign and Clear-Correct, as well as emerging local brands. Aggressive marketing strategies and simplified certification programs have expanded general practitioners' access to aligners. Although it is easily available, it also has some drawbacks, namely uneven quality control, overreliance on specific software solutions, and limited application of sound biomechanical principles. Academic institutions and professional bodies must therefore ensure that clinical decision-making remains evidence-based and independent of commercial bias [14,15]. Introducing clear aligner therapy into the undergraduate and postgraduate dental curricula in India would be beneficial. Dedicated modules covering digital orthodontics, 3D printing, and aligner biomechanics would prepare future clinicians for the evolving landscape of orthodontic care [16].
Limitations
This study's cross-sectional design is limited to causal inference. The reliance on self-reported data may introduce recall and social desirability biases. The findings may not be generalizable due to the restricted geographic area. Additionally, the study did not evaluate treatment outcomes or objectively measure clinical proficiency. Future longitudinal studies with larger samples and objective performance metrics are recommended to validate and expand upon these findings.
Conclusions
The present study highlights a progressive yet uneven adoption of Clear Aligner Therapy among dental professionals in India. Although dental practitioners have theoretical knowledge, cost barriers, patient compliance issues, and limited hands-on training continue to hinder broader clinical integration. Structured, evidence-based educational initiatives focusing on case selection, biomechanics, and digital workflow are essential for improving competency. Incorporating clear aligner modules into dental curricula and standardized CDE programs will be key to fostering competent, ethically guided adoption of CAT in modern orthodontic practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Effectiveness of clear aligner therapy for orthodontic treatment: A systematic review Orthod Craniofac Res Robertson L Kaur H Fagundes NC Romanyk D Major P Flores Mir C 1331422320203165108210.1111/ocr.12353 · doi ↗ · pubmed ↗
- 2Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review Angle Orthod Rossini G Parrini S Castroflorio T Deregibus A Debernardi CL 8818898520152541226510.2319/061614-436.1PMC 8610387 · doi ↗ · pubmed ↗
- 3Clinical limitations of Invisalign J Can Dent Assoc Phan X Ling PH 263266732007 http://pubmed.ncbi.nlm.nih.gov/17439714/17439714 · pubmed ↗
- 4The pedagogical value of parallel charts for dental students in clinical education: A qualitative study Eur J Dent Educ Marty M Bédard U Gendron B Vergnes JN Valéra MC 100410102720233665168810.1111/eje.12892 · doi ↗ · pubmed ↗
- 5A comparison of treatment effectiveness between clear aligner and fixed appliance therapies BMC Oral Health Ke Y Zhu Y Zhu M 241920193067430710.1186/s 12903-018-0695-z PMC 6343314 · doi ↗ · pubmed ↗
- 6A survey on the knowledge and perception of orthodontic clear aligner systems among general dentists J Contemp Orthod Goswami DN Ansari N Arun AV Mahendra S Chandrashekar BS Raju AS Chikamagalur MM 18118982024
- 7Radiographic comparisons of crestal bone levels around implants placed with low-speed drilling and standard drilling protocols: Preliminary results Saudi Dent J Tabassum A 9659713320213493803910.1016/j.sdentj.2021.08.003PMC 8665170 · doi ↗ · pubmed ↗
- 8Nasolabial fold dynamics: Implications for facial paralysis and facial reanimation surgery Orthod Craniofac Res Dusseldorp JR Faraway J Razavi L Hadlock TA Trotman CA 62692420213254310010.1111/ocr.12400 PMC 11221366 · doi ↗ · pubmed ↗