Dual-Bone Grafting Technique of Neck Reconstruction in Non-union Neck Femur Fracture With Avascular Necrosis of the Femur Head
Somok Banerjee, Alok Rai, Nirmal Rathi, Suhas Mahendrakar, Rishabh Verma

TL;DR
A 36-year-old man with a non-healing hip fracture and bone death underwent a bone grafting surgery that successfully restored hip function and reduced pain.
Contribution
The paper presents a successful case of dual-bone grafting for non-union femoral neck fracture with avascular necrosis.
Findings
The patient achieved radiographic union and functional recovery three years post-surgery.
The Harris Hip Score improved from 38 to 85, indicating significant clinical success.
The dual-bone grafting technique preserved joint function and allowed return to manual labor.
Abstract
A 36-year-old male farmer with known sickle cell disease presented four months after a road traffic accident with right hip pain and difficulty walking. He had initially received conservative treatment with traction but discontinued it due to financial constraints. Clinical examination revealed signs of hip instability, a 3 cm true limb shortening, and a Harris Hip Score of 38. Imaging showed a Sandhu Stage 3 non-union of the femoral neck with >50% neck resorption and Ficat-Arlet Grade 2a avascular necrosis (AVN). Given the relatively favorable prognostic indicators, including a Kerboul angle of 100°, the patient opted for a joint-preserving procedure to retain his ability to squat and perform manual labor. The patient underwent osteosynthesis through a modified Heuter approach. A 3 cm tricortical iliac crest graft was used to bridge the fracture gap and restore neck length, supported…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
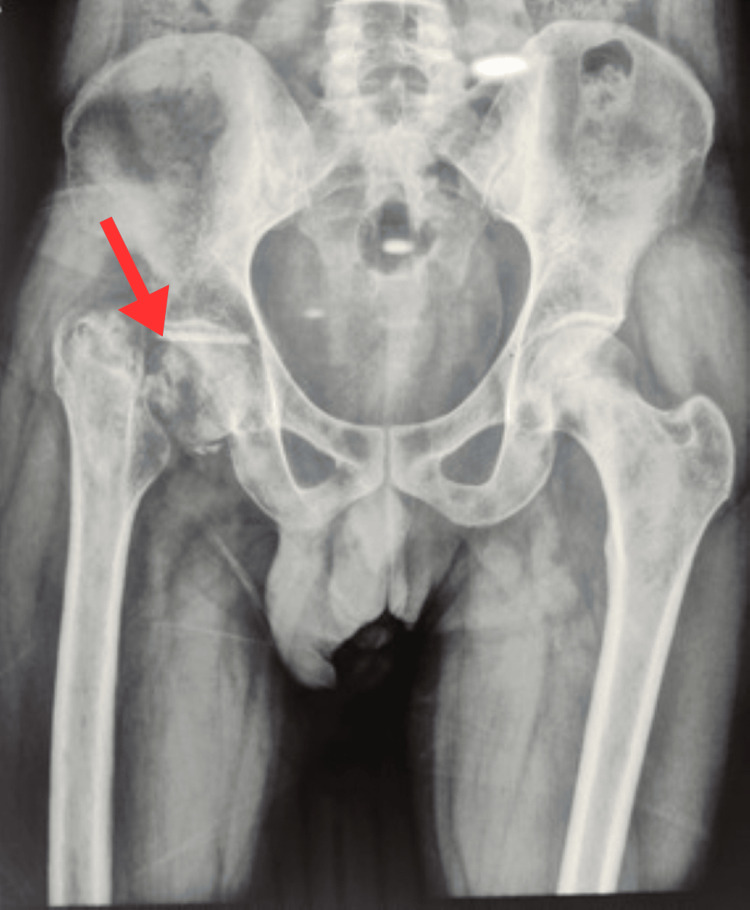 Figure 1
Figure 1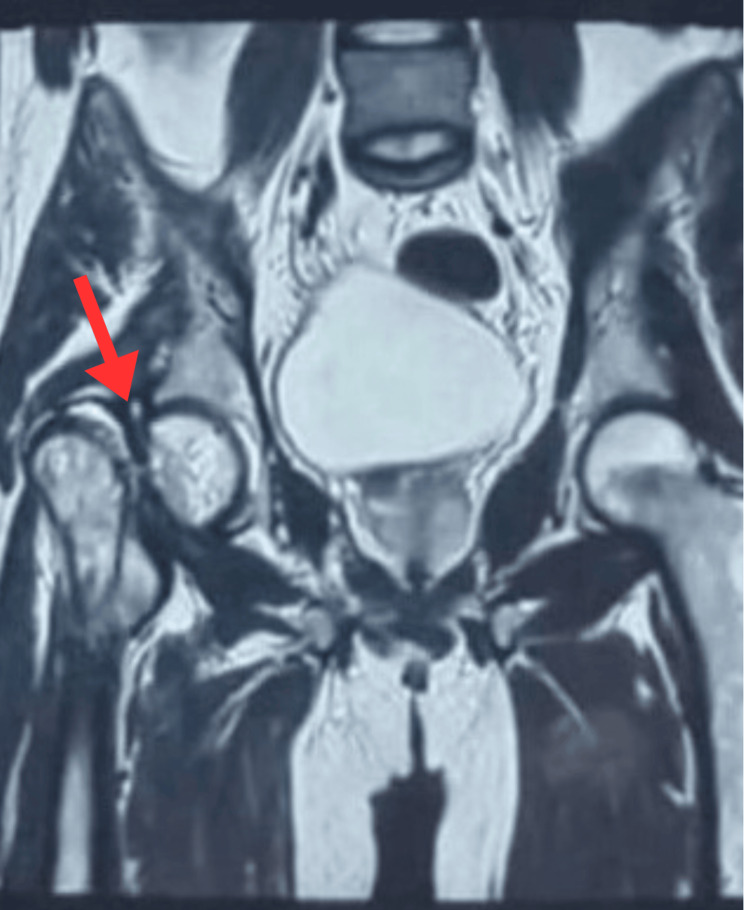 Figure 2
Figure 2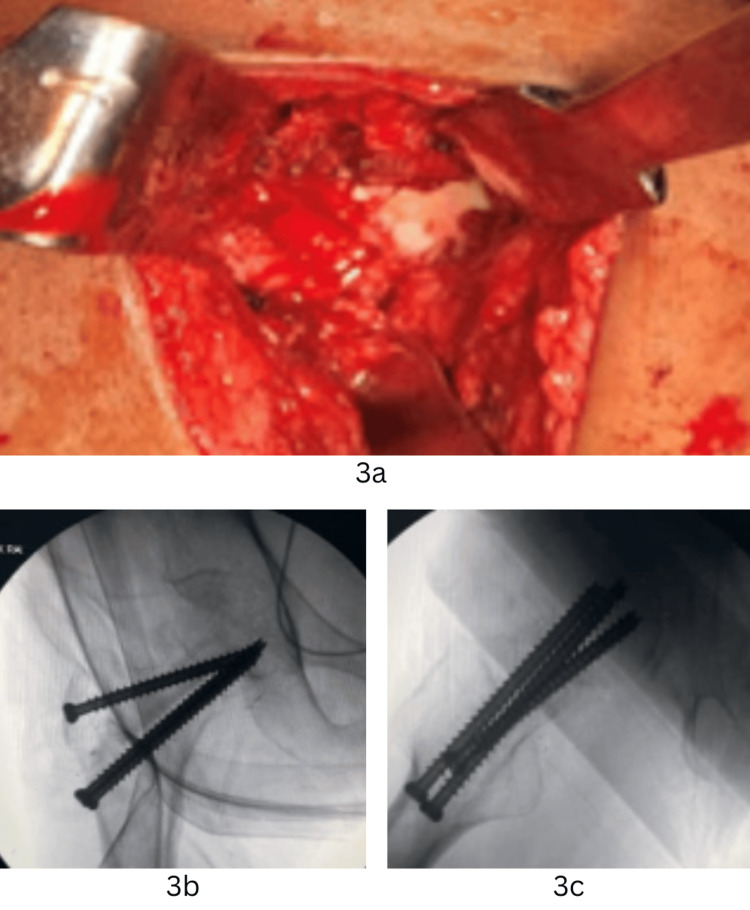 Figure 3
Figure 3 Figure 4
Figure 4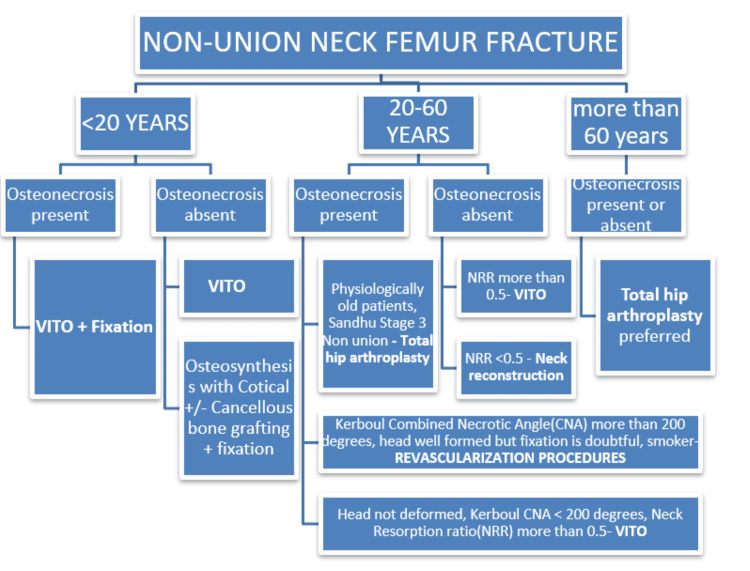 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Hip disorders and treatments · Bone and Joint Diseases
Introduction
Non-union of the femoral neck fractures with avascular necrosis (AVN) of the femoral head represents one of the most difficult scenarios in orthopaedic trauma surgery, particularly in young and active individuals [1]. These cases are further complicated in patients with underlying hematological disorders such as sickle cell disease, which independently contributes to the compromised vascularity of the femoral head. Management decisions in such situations require a nuanced approach to balance hip preservation and functional recovery. While total hip arthroplasty (THA) offers predictable results in older patients, it poses long-term challenges in young individuals due to increased mechanical demands and higher revision rates. Osteosynthesis with bone grafting remains a viable option in select young patients, aiming to preserve native anatomy and optimize biomechanics. We present a case of a young male manual laborer with sickle cell disease who sustained a femoral neck fracture, progressed to non-union with Ficat-Arlet Grade 2a AVN, and was successfully treated with open reduction and internal fixation (ORIF) combined with a dual-bone grafting technique, comprising autologous tricortical iliac crest graft and non-vascularized fibular strut graft, stabilized using cannulated cancellous screws (CC screws) and a Pauwels screw.
Case presentation
A 36-year-old male farmer presented four months after a road traffic accident, initially managed with skin traction at a district hospital. He had a known history of sickle cell disease and complained of intermittent right hip pain even before the trauma. Due to financial limitations, he delayed further intervention and presented with progressive pain, limp, and inability to bear weight.
On examination, he exhibited a 3-cm limb shortening, external rotation deformity of the lower limb, positive Trendelenburg and telescopy tests, and inability to perform a straight leg raise. No neurological deficits were noted. The Harris Hip Score at presentation was 38.
Radiographs demonstrated a non-union of the femoral neck with proximal migration of the greater trochanter and partial neck resorption (Figure 1). Magnetic resonance imaging revealed Grade 2a AVN changes in the antero-superior-medial femoral head and a Sandhu Stage 3 non-union (Figure 2). Given the patient’s occupation, functional demands, and desire to avoid the restrictions associated with total hip arthroplasty, he elected for a joint-preserving approach with ORIF and autologous bone grafting.
Preoperative radiographThe red arrow indicates non-union of the femoral neck with proximal migration of the greater trochanter.
Sagittal section of MRI showing non-union of neck of femur fracture The red arrow indicates non-union of the femoral neck and partial resorption of neck.
Surgical technique
After obtaining informed consent, the patient underwent surgery under combined spinal-epidural anaesthesia with prophylactic antibiotics. The patient was positioned supine on a fracture table with traction applied to the right lower limb and a modified Heuter approach was used. A 10-cm incision was made starting 2 cm distal and lateral to the anterior superior iliac spine and extended toward the lateral femoral condyle. The tensor fascia lata was dissected carefully to avoid damaging the lateral femoral cutaneous nerve. The ascending branches of the lateral circumflex femoral artery were ligated. The anterior hip capsule was exposed, and a T-shaped capsulotomy was performed.
On inspection, a 3-cm gap was found at the fracture site, with sclerosed margins. The fracture ends were curetted and freshened. A 3-cm wedge-shaped tricortical iliac crest graft was harvested and used to bridge the defect and restore neck length. The reduction was temporarily stabilized with three K-wires. A 6.5-mm fully threaded CC screw was inserted inferiorly through a separate lateral incision. A slot was created superior to this screw using a triple reamer, and a 7-cm non-vascularized fibular strut graft, harvested from the ipsilateral leg, was placed into the neck bridging the fracture site.
Additional fixation was achieved with a Pauwels screw and a posteriorly placed 6.5-mm CC screw (Figure 3). Haemostasis was secured, the capsule closed, and the wound closed in layers over a drain. Immediate postoperative X-rays confirmed anatomical reduction and stable fixation.
Intraoperative images(3a) Intraoperative clinical photo; (3b) antero-posterior image of final fixation; (3c) lateral image of final fixation.
Postoperative management and outcome
Postoperative rehabilitation included early passive mobilization and isometric exercises. Toe-touch weight-bearing began at six weeks, progressing to full weight-bearing at 6 months after radiographic evidence of union.
Follow-up radiographs (one-year follow-up) showed gradual graft incorporation and union across the fracture site. At three years follow-up, the patient demonstrated full union (Figure 4) with 1 cm residual shortening. He resumed agricultural activities and was able to squat, sit cross-legged, and ambulate without support. Harris Hip Score improved to 85 from 38, indicating significant functional recovery.
Follow-up orthogonal radiographs after three years The red arrow indicates union at fracture site after three years in antero-posterior (4a) and lateral (4b) radiographs.(4a) Antero-posterior view showing union at fracture site and rigid fixation; (4b) lateral view showing union at fracture site and rigid fixation,
Discussion
Femoral neck fractures in young adults are often termed “unsolved fractures” due to their tendency toward non-union and AVN. The femoral head’s limited blood supply, particularly from the retinacular vessels, predisposes it to necrosis following fracture. Factors like displacement, vertical fracture orientation (high Pauwels angle), posterior comminution, poor reduction, and delayed treatment contribute to adverse outcomes [2].
AVN further complicates management, especially in sickle cell disease, which impairs microvascular perfusion. Non-union with AVN can lead to mechanical failure, persistent pain, and disability [3]. Treatment choices must weigh preserving native joint anatomy versus the reliability of joint replacement (Figure 5) [4-6]. While THA and hemiarthroplasty offer predictable outcomes in elderly patients, young, active individuals benefit from preserving their biological hip structure [7].
Decision-making algorithm in the management of non-union neck femur fracturesRevascularization procedures: Vascularized fibula graftingKerboul combined necrotic angle: Sum of arc angles subtended by necrotic foci in head of the femur in antero-posterior and lateral views of MRI.Neck reconstruction: All India Institute of Medical Sciences (AIIMS) box technique, Modified AIIMS box technique, etc.Salvage options: Hip arthrodesis in young (not favored), total hip arthroplasty.VITO: Valgus intertrochanteric osteotomy; NRR: Size of femur head remnant/size of femur neck on the sound side (NRR<0.5 indicates high chance of failure from VITO).Credit: Algorithm created by Dr. Somok Banerjee.
Several surgical strategies exist for non-union femoral neck fractures with AVN, including valgus osteotomy, vascularized or non-vascularized bone grafting, and arthroplasty. Each carries specific indications and complications. ORIF with bone grafting, particularly when combined with strut grafts, offers biomechanical and biological advantages. The iliac crest graft provides osteogenic and osteoinductive potential, while the fibular strut acts as a mechanical buttress, resisting shear forces and facilitating revascularization of the femoral head [4,8].
In our case, the Kerboul angle was <100°, suggesting limited femoral head necrosis, which is associated with better outcomes. Studies suggest that necrotic angles <200° and neck resorption ratios >0.5 correlate with successful osteosynthesis. The dual grafting technique restored length and provided biological and mechanical support, contributing to union and functional success [9].
Literature indicates that ORIF in similar settings can achieve union rates of 60%-80% if anatomic reduction and stable fixation are obtained. Compared to THA, which carries long-term risks of wear, dislocation, and revision surgeries, ORIF enables young patients to maintain native biomechanics and return to high-demand activities [10].
Conclusions
Femoral neck non-union with AVN in young adults poses a significant challenge. This case demonstrates that ORIF with dual autologous bone grafting using tricortical iliac crest and non-vascularized fibula strut grafts can provide excellent outcomes in carefully selected patients. With proper technique, this hip-preserving method can yield a stable union and restore function in high-demand individuals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The relationship between femoral neck fracture in adult and avascular necrosis and nonunion: a retrospective study Ann Med Surg (Lond) Koaban S Alatassi R Alharbi S Alshehri M Alghamdi K 593920193073386310.1016/j.amsu.2019.01.002PMC 6357682 · doi ↗ · pubmed ↗
- 2Nonunion of the femoral neck: possibilities and limitations of the various treatment modalities Indian J Orthop Raaymakers EL Marti RK 13214220081982364910.4103/0019-5413.38575 PMC 2759582 · doi ↗ · pubmed ↗
- 3Treatment of neglected femoral neck fracture Indian J Orthop Jain AK Mukunth R Srivastava A 17274920152559335410.4103/0019-5413.143909 PMC 4292324 · doi ↗ · pubmed ↗
- 4Femoral neck nonunion treatment Clin Orthop Relat Res Mathews V Cabanela ME 5764200410.1097/00003086-200402000-0001015021132 · doi ↗ · pubmed ↗
- 5Triple attack technique for non-union of femoral neck fractures Int Orthop Abdelazeem H Abdelazeem A Al-Dars A Hegazy M Abdellatif N 8078124020162610576110.1007/s 00264-015-2808-5 · doi ↗ · pubmed ↗
- 6"Cage in box" - a modification of AIIMS BOX technique for large gap nonunion in young patients with neglected femur neck fractures Injury Garg B Vatsya P 119612015320223465775110.1016/j.injury.2021.09.046 · doi ↗ · pubmed ↗
- 7Hemiarthroplasty vs total hip arthroplasty for the management of displaced neck of femur fractures: a systematic review and meta-analysis J Arthroplasty Lewis DP Wæver D Thorninger R Donnelly WJ 183718433420193106091510.1016/j.arth.2019.03.070 · doi ↗ · pubmed ↗
- 8Indices affecting outcome of neglected femoral neck fractures after valgus intertrochanteric osteotomy J Orthop Trauma Varghese VD Boopalan PR Titus VT Oommen AT Jepegnanam TS 4104162820142416478710.1097/BOT.0000000000000030 · doi ↗ · pubmed ↗