Expert Elicitation on Exposure to Tick Bites and Tick-Borne Encephalitis Risk in Occupational and Recreational Forest Activities
Claude Saegerman, Elsa Quillery, Marc Leandri, Véronique Raimond, Pauline Kooh, Philippe Fravalo, Thierry Hoch, Yves Hansman, Nathalie Boulanger

TL;DR
Experts identified high-risk forest activities for tick bites, which can spread tick-borne encephalitis, to help target prevention efforts.
Contribution
The study uses expert opinions to rank forest activities by tick bite risk, filling a data gap for prevention strategies.
Findings
Forest monitoring, forestry, and scientific activities are top occupational risks for tick bites.
Recreational activities like mushroom picking and orienteering also pose high tick bite risks.
Targeted prevention messages can reduce TBE risk for people engaging in these high-risk activities.
Abstract
Background: Tick-borne encephalitis (TBE) virus is transmitted to humans via tick bites and occasionally via the consumption of unpasteurized milk products. According to the literature, the most important driver of TBE emergence and increase in incidence in humans is changes in human behaviour/activities. Method and principal findings: To compensate for the lack of data, expert opinions were gathered to identify the risk factors for exposure to tick bites linked to twenty-eight human activities (professional or recreational) in forests and to target prevention messages at the populations most at risk. Opinions were elicited from a total of twenty-five European experts. Seven criteria were included in the analysis for each activity: frequency, seasonality, duration of exposure, distance covered, degree of contact with vegetation, speed and average level of protection against tick bites.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1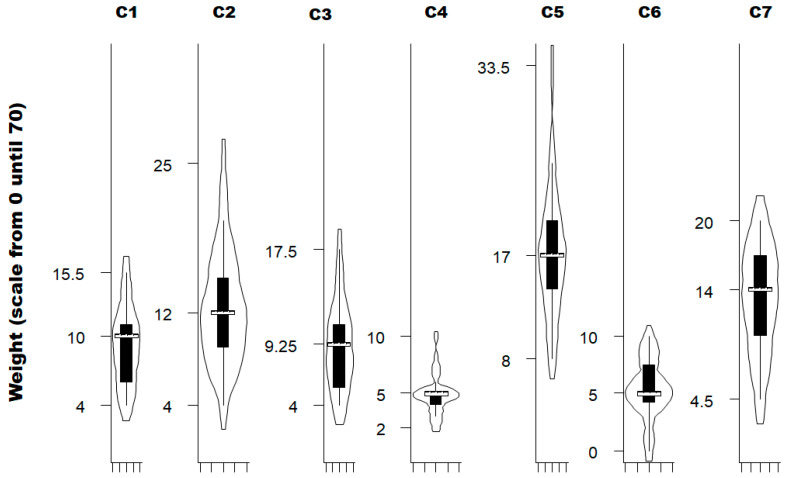 Figure 2
Figure 2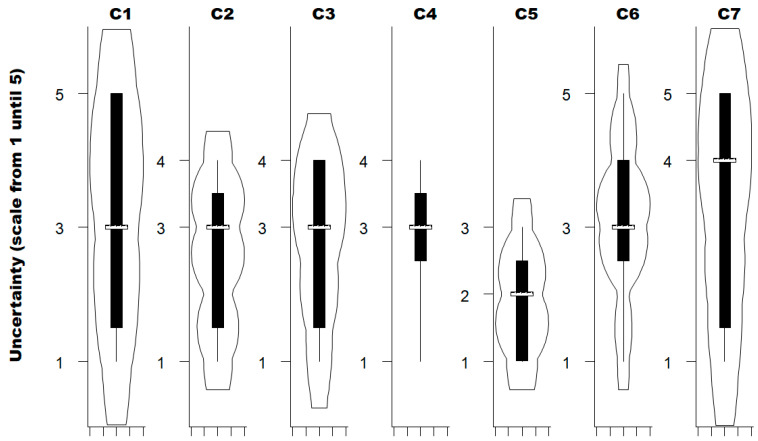 Figure 3
Figure 3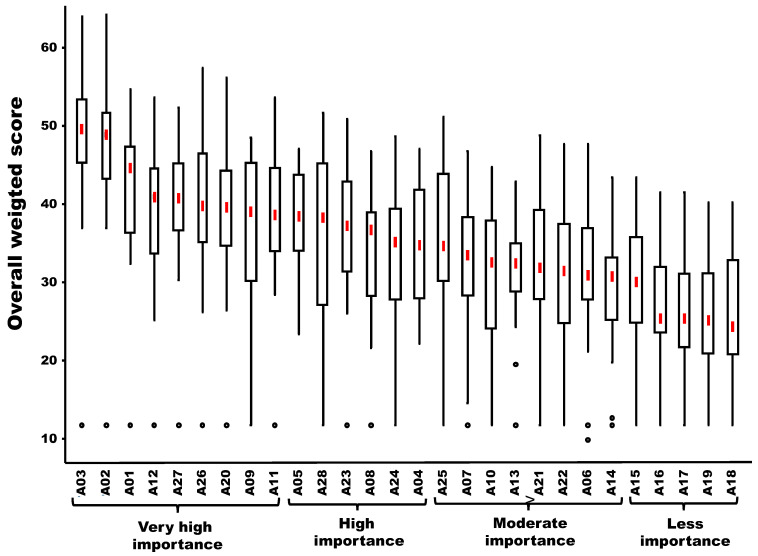 Figure 4
Figure 4- —TBEV risk assessment of a working group established by the French Agency for Food, Environmental and Occupational Health & Safety (Anses)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Herpesvirus Infections and Treatments · Viral Infections and Vectors
1. Introduction
Prevention against tick-borne diseases is an important public health issue. Lyme disease due to Borrelia is the most frequent worldwide tick-borne disease infection. However, the tick-borne encephalitis virus (TBEV) responsible for tick-borne encephalitis (TBE) is identified as a potential emerging pathogen in Western Europe. This virus is transmitted to humans by the bites of infected Ixodes ticks and, in rare cases, via the consumption of unpasteurized milk products [1]. The economic impact of the TBE in Europe is significant but highly variable, depending on the study [2,3,4,5]. TBE is endemic in parts of Asia and Europe, and according to the literature, the most important driver of TBE emergence and increase in incidence in humans is changes in human behaviour/activities [6]. For example, increasing leisure time spent outdoor activities and increasing travel and mobility within Europe are two drivers of TBE risk [7].
Forests are ideal locations for recreational activities (leisure, relaxation, tourism, discovering flora and fauna, hunting) as well as professional activities (professional activities in forest environments, including both forestry operations and knowledge-oriented work). Human forest visitation in Europe is trending upward, driven by a growing demand for recreation, well-being, and tourism, a trend significantly amplified by the COVID-19 pandemic [8,9]. In fact, COVID-19-related lockdowns significantly reduced the incidence of various infectious diseases by decreasing social contact. However, the incidence of TBE was not affected due to the pursuit of forest activities [10].
The risk of exposure to tick bites depends on several factors that favour tick-human encounters, such as certain leisure or professional activities [11,12]. For example, at the microhabitat level, exposure depends on the areas frequented by humans and the manner in which they are managed. More precisely, in forested areas, walking on maintained paths results in fewer tick bites than walking on grassy trails or off-trails. Vegetation maintenance therefore plays a role in exposure to tick bites [13]. Other exposure factors involve the relationship between seasons, weather conditions and human behaviour. For example, it has been hypothesised that tick bites are more frequent on weekends with good weather following a week of precipitation, which is a favourable time for mushroom picking [14]. Exposure to tick bites also depends on the density of Ixodes ricinus questing on vegetation and is therefore higher in mainland regions in spring and early summer, which also corresponds to the period of greatest human activity in forest areas.
In this context, identifying the activities that pose the greatest risk is a critical task in the development of awareness and information campaigns targeting people who practice these activities to reduce their exposure to tick bites. This paper aims to rank forest activities (professional or recreational) according to a series of criteria and European expert opinion.
2. Materials and Methods
2.1. Context and Expert-Opinion Elicitation
The following context was considered in the expert-opinion elicitation process: a forest in which all factors are present to favour the presence of ticks (presence of hosts, biotic and abiotic factors) and TBEV circulation. In this forest, all of the activities listed are possible, with consideration of the most frequently encountered situation for each type of activity (assignment of a score per criterion).
A questionnaire was prepared in the form of an Excel file consisting of various sheets:
- ▪Sheet entitled ‘Expert information’: this was intended to briefly describe the profile of the expert completing the questionnaire.
- ▪A set of seven sheets concerning the various criteria considered: (1) frequency of the activity; (2) seasonality; (3) duration of exposure; (4) distance covered; (5) degree of contact with vegetation; (6) speed; and (7) average level of protection against tick bites. These sheets were designed to gather the opinion of each expert by assigning a score for each of the criteria defined for each activity. Each sheet in the file provided the necessary instructions and details (e.g., definitions of activities and scores) (Table 1 and Table 2).
- ▪Sheet entitled ‘weighting of criteria’: this was intended to distribute a fixed number of points (n = 70) among the seven various criteria mentioned above. If the expert considered the criteria to be equivalent, he/she assigned the same number of points to each. Otherwise, he/she assigned the number of points in proportion to the relative importance of the criteria considered.
- ▪Sheet entitled ‘uncertainty’: for each criterion, they were also asked to give an uncertainty rating between 1 (minimum uncertainty) and 5 (maximum uncertainty).
Each tab in the Excel file explained the approach and details required to complete the task. The questionnaire was refined considering comments following a pre-test of the questionnaire with four experts from the Anses working group, each with a different area of expertise (political science, economics, ticks and tick-borne diseases, risk assessment). The questionnaire was then sent to a list of scientific experts compiled by the task force.
2.2. Scoring System and Clustering of Activities
Considering, on the one hand, the score assigned for each criterion and the number of possible options for each score and, on the other hand, the relative weight of each criterion, a weighted overall score (WOS) was calculated for each activity and for each expert using the following formula:
where Ci is a given criterion and M is the number of modalities per score for a given criterion (Table 2). As the number of modalities is not the same for each criterion, each score awarded was divided by the number of modalities for the criterion in question (standardization requirement).
The activities were then ranked in relation to each other based on the medians of the overall scores obtained for each activity by all experts. Finally, the activities were aggregated (clustered) into four groups using a regression tree analysis (activities classified as high risk, at risk, moderately at risk and low risk). Each group of activities was identified by a given average and by minimizing its standard deviation as much as possible.
2.3. Sensitivity Analysis
In order to ascertain whether the ranking of forest activities was influenced by the selection of experts, a sensitivity analysis was performed using a comparison of ten bootstraps each (random selection of fifteen experts amongst twenty-five) with the ranking of forest activities with all experts elicited as reference. The difference between the above ranking of forest activities (each bootstrap versus all experts as reference) was tested using the Pearson coefficient of correlation test [6]. Because of the overrepresentation of French experts in the European sample, a sensitivity analysis was also performed, excluding these experts. If this coefficient was close to 1 and the p-value was less than 0.05, the correlation between the two rankings of forest activities tested was considered significant.
2.4. Uncertainty Analysis and Additional Statistical Analysis
For each criterion, uncertainty was estimated using a rating between 1 (minimum uncertainty) and 5 (maximum uncertainty). A violin plot was used to depict the weight and the uncertainty about the seven criteria considered. It is a statistical visualization that combines a classical box plot (vertical axis) with a kernel density plot (horizontal axis) to show the distribution of numeric data across one or more groups [15].
3. Results
3.1. Number of Experts and Their Field of Expertise
Opinions were elicited from a total of twenty-five European experts. Their recruitment was done by the French Agency for Food, Environmental and Occupational Health and Safety using a list of experts in vectors and vectorial-borne diseases. These experts came from the following countries (in decreasing order): France (n = 14); Belgium (n = 3); Slovenia (n = 2); Sweden (n = 2); and Italy, Lithuania, the United Kingdom, and Switzerland (n = 1 each). The keywords characterising the expertise of these experts are depicted in Figure 1 and corroborate the multidisciplinary nature of the study. The top three keywords were epidemiology (13 occurrences), tick-borne diseases (7 occurrences), and vector-borne diseases (4 occurrences). The number of years of professional expertise in the field of tick-borne diseases followed a normal distribution (Shapiro–Wilk test, p-value = 0.68) with a mean of 21.1 years and a standard deviation of 9.1 years.
The panel of experts consisted of one research engineer, two with master’s degrees in science, twelve with PhDs, and ten others with PhDs who were professors. Four of them worked for an (inter)national agency, eight for a laboratory or research institution, two for a Ministry of Health, and eleven for a university.
3.2. Relative Importance of Criteria and Their Uncertainty
Not all criteria carry the same weight (Kruskal–Wallis test for equality of populations; Chi2 (6 degrees of freedom; α = 0.05) = 95.14; p-value = 0.0001) (Figure 2). Using quantile regression, the results show that the degree of contact with vegetation (criterion 5; p-value < 0.001) and the level of general protection against tick bites (criterion 7; p-value = 0.001) are more important than activity frequency, seasonality, and duration of exposure (criteria 1 to 3, respectively), while distance covered during activity (criterion 4) and speed during activity (criterion 6) are significantly less important (p-value < 0.001).
The uncertainty regarding the criteria to be considered when prioritising forestry activities was assessed by each expert on a scale ranging from 1 (minimal uncertainty) to 5 (maximum uncertainty) (Figure 3). The median uncertainty rating was 3 for the frequency of activity (C1), its seasonality (C2), the duration of exposure for one activity session (C3), the distance covered during the activity, and the speed during the activity (C6). For the contact with vegetation during the activity (C5) and the general protection against tick bites (C7), the median uncertainty was 2 and 4, respectively. No statistical difference in the median uncertainty was observed between criteria (Kruskal–Wallis test for equality of populations; Chi2 (6 degrees of freedom; α = 0.05) = 8.05; p-value = 0.23).
3.3. Ranking and Clustering of Forest Activities
The ranking and clustering (in four different groups) of forest activities in descending order of risk of exposure to tick bites is presented in Figure 4. The first group of activities with very high importance included nine forest activities (in decreasing order): forest protection activities (A03), forestry and wood industry activities (A02), scientific and/or analytical activities (A01), mushroom picking (A12), spending the night in the forest (A27), hunting as shooting and battue (A26), naturalist activities (A20), orienteering (A09), berry or fruit picking (A11). In addition, three other groups (high importance, moderate importance and less importance) were identified and included six, eight and five activities, respectively.
3.4. Sensitivity Analysis
The result of the sensitivity analysis indicated that, irrespective of the experts excluded, excluding some experts only had very limited or no significant effects on the ranking of forest activities compared to the reference (all experts elicited). Indeed, using ten bootstraps of fifteen experts amongst twenty-five, the Pearson correlation coefficient between each bootstrap against the ranking of twenty-five experts as a reference was very high (value between 0.97 and 0.99, with a p-value < 0.0001). The normality of p-value was also verified (Shapiro–Wilk test; p-value = 0.37) with a mean of 0.98 and a standard error of 0.007. Because of the overrepresentation of French experts in the European sample, a sensitivity analysis was also performed, excluding these experts, and limited effect on the ranking of forest activities was observed (value of the Pearson correlation coefficient 0.97 with a p-value < 0.0001).
4. Discussion
To the best of the author’s knowledge, no study was published before concerning the typology of forest activities based on weighted criteria related to the risk of human exposure to tick bites. The present study contributes to filling this gap.
Amongst twenty-eight forest activities included in this study, the first group of nine activities was more at risk of tick bites (in decreasing order): firstly three occupational activities (forest protection activities, forestry and wood industry activities and scientific and/or analytical activities) and secondly, five recreational activities and one hunting activity (mushroom picking, spending the night in the forest, hunting by shooting and beating, naturalist activities, orienteering, and berry or fruit picking).
This expert-opinion elicitation involved twenty-five experts with different fields of expertise and disciplines. It is legitimate to wonder whether the size of the expert panel is sufficient and whether its composition is appropriate to produce reliable results from the elicitation process. Currently, there is no standard method to calculate the required size of a panel of experts. However, ref. [16] summarized some trends. Indeed, a recommendation for panel size is five to twenty experts with diverse knowledge [17]. Moreover, under typical circumstances, the panel is usually between 10 and 30 experts [18,19,20,21,22,23,24,25,26,27,28,29]. However, the extent of expertise of the panel (partially and indirectly tested in the study using the sensitivity analysis) is far more important for decision-making effectiveness than the number of participants [30,31]. Finally, it is highly unlikely that another equally expert group will produce radically different results from a panel of fifteen experts [32]. Based on evidence (publications in international peer-reviewed journals), both the composition and the size of the expert panel (n = 25) involved in the present study are adequate and in accordance with the best practices in the field of expert-opinion elicitation. In addition, our sensitivity analysis demonstrates the robustness of the proposed expert-opinion elicitation, for which no important bias was observed.
Considering the seven criteria included in the analysis, one of them concerns the risk of tick bites associated with forest activities (i.e., the degree of contact with vegetation), and another concerns protective measures (i.e., the level of general protection against tick bites). The degree of contact with vegetation like sitting on grass during work or taking a break during an activity is most often associated with highest frequency of tick bites in the literature [33]. In general, prevention against tick bites relies mainly on mechanical and chemical prevention [34]. Preventive measures include wearing light-coloured clothing that covers the skin (long sleeves, long trousers) so that ticks can be easily detected and using skin repellents [35]. Suitable products include DEET (N,N-diethyl-3-methylbenzamide), IR3535 (synthetic ethyl butylacetylaminopropionate), picaridin, and oil of lemon eucalyptus or PMD (para-menthane-diol) [36]. Depending on the product used, some restrictions exist in case of pregnancy, breastfeeding, and for children [37]. Other preventive measures include regular checks of clothing and skin for ticks and careful removal of the ticks if found (if possible, with a tick remover or fine-tipped tweezers if the tick is already attached), and visits limitation to areas where ticks are abundant during the seasons when they are most active, especially by staying on paths. Despite the existence of marketing authorisation for clothing impregnated with pyrethroids, particularly permethrin, the risk-benefit balance of their use is now considered unfavourable for use by the general population and is therefore no longer recommended [38]. Prevention policies and information campaigns can improve awareness of the risk of tick bites and associated diseases, as well as the adoption of effective protective measures. Several studies support this view, particularly those relating to Lyme disease. For example, in this regard, between 2016 and 2019 in France, the rate of use of skin repellents and long clothing in situations of exposure increased by 2 and 7 percentage points, respectively, reaching 18% and 73% [39]. Given that the Lyme plan launched in France in 2016 aimed to raise awareness of these risks, it can be assumed that part of this change is due to information campaigns. Indeed, awareness of Lyme disease, which is better known than TBEV, remained at only 41% in 2019, compared with 29% in 2016 [39]. In the case of Lyme disease, a positive correlation was identified in France between protecting oneself and feeling well-informed [39]. This correlation has also been proven in the United Kingdom [40] and the Netherlands [41]. Information and prevention policies relating to protection against tick bites, such as those implemented in the Lyme plan since 2016 in France [34], are among the relevant courses of action recommended to limit human infections with TBEV. However, some of the protective measures generally recommended against Lyme disease are not effective against TBEV. Indeed, ‘ex-post’ measures such as body inspection or corrective measures such as the use of a tick remover to remove ticks as quickly as possible would not prevent TBEV transmission, which occurs immediately after the bite [42,43], unlike infection with the bacterium responsible for Lyme disease, which occurs later [44]. In this regard, continuing the information campaigns initiated in the Lyme plan can help to further increase individual protection, with an emphasis on those that also work for TBEV. More broadly, the implementation of prevention and information options regarding tick bites can build on existing tick-related initiatives like annual awareness day organised by the reference centres for tick-borne diseases or awareness-raising through citizen surveillance network on tick biting (e.g., CiTIQUE in France, TickNet in Belgium, TekenRadar in The Netherlands or the App Tick Prevention in Switzerland). Continued education must be tailored to the areas and target audiences (e.g., endemic versus emerging regions, children versus adults, urban areas versus forest areas). It can also take the form of dedicated signage, such as information boards in high-risk areas or messages in specific applications, to warn of the presence of ticks. Raising public awareness could also be achieved through better training for community pharmacists [45].
5. Conclusions
According to a systematic review and meta-analysis, it is important to note first that outdoor activities provide health benefits and promote well-being [46]. To compensate for the lack of data, expert-opinion elicitation was undertaken to identify the risk factors for exposure to tick bites linked to twenty-eight human activities in forests and to target prevention messages at the populations most at risk. Prevention messages regarding tick bites could be targeted at people who engage in activities considered in this analysis to be at the highest risk of exposure to ticks (in particular, mitigation measures should be presented in the following operational sequence for each user: what should I do before, during, and after each activity?). More observational studies are needed to gain more evidence-based information on tick bites related to forest activities, with the aim of improving risk assessment modelling. The implementation of a similar study is recommended in other continents, especially Asia where TBEV is more endemic and virulent [47], and for a broader number of forest activities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Süss J. Tick-borne encephalitis 2010: Epidemiology, risk areas, and virus strains in Europe and Asia-an overview Ticks Tick Borne Dis.2011221510.1016/j.ttbdis.2010.10.00721771531 · doi ↗ · pubmed ↗
- 2Cassini A. Colzani E. Pini A. Mangen M.J.J. Plass D. Mc Donald S.A. Maringhini G. van Lier A. Haagsma J.A. Havelaar A.H. Impact of infectious diseases on population health using incidence-based disability-adjusted life years (DAL Ys): Results from the Burden of Communicable Diseases in Europe study, European Union and European Economic Area countries, 2009 to 2013 Eurosurveillance 201823170045410.2807/1560-7917.ES.2018.23.16.17-00454 PMC 591597429692315 · doi ↗ · pubmed ↗
- 3Šmit R. Postma M.J. The Burden of Tick-Borne Encephalitis in Disability-Adjusted Life Years (DAL Ys) for Slovenia P Lo S ONE 201510 e 014498810.1371/journal.pone.014498826672751 PMC 4684505 · doi ↗ · pubmed ↗
- 4Scaggiante R. Guadagni L. Orso M. d’Angela D. Carrieri C. Polistena B. Spandonaro F. Bertoldi I. Pilz A. Schley K. Incidence, healthcare resource utilization and costs of hospitalized patients with tick-borne encephalitis (TBE) in Italy Ticks Tick. Borne Dis.20241510237210.1016/j.ttbdis.2024.10237238917767 · doi ↗ · pubmed ↗
- 5Slunge D. Boman A. Studahl M. Burden of Tick-Borne Encephalitis, Sweden Emerg. Infect. Dis.20222831432210.3201/eid 2802.20432435075997 PMC 8798699 · doi ↗ · pubmed ↗
- 6Saegerman C. Humblet M.-F. Leandri M. Gonzalez G. Heyman P. Sprong H. L’Hostis M. Moutailler S. Bonnet S.I. Haddad N. First Expert Elicitation of Knowledge on Possible Drivers of Observed Increasing Human Cases of Tick-Borne Encephalitis in Europe Viruses 20231579110.3390/v 1503079136992499 PMC 10054665 · doi ↗ · pubmed ↗
- 7Kunze U. The International Scientific Working Group on Tick-Borne Encephalitis (ISW TBE): Review of 17 years of activity and commitment Ticks Tick. Borne Dis.2016739940410.1016/j.ttbdis.2015.12.01826795231 · doi ↗ · pubmed ↗
- 8ŠodkováM. Purwestri R.C. Riedl M. JarskýV. Hájek M. Drivers and Frequency of Forest Visits: Results of a National Survey in the Czech Republic Forests 20201141410.3390/f 11040414 · doi ↗