HIV-1 Genetic Diversity and Drug Resistance Mutation Profiles in Donetsk, Luhansk and Zaporizhzhia Regions
Anastasiia Antonova, Anatolii Vinokurov, Daria Kustova, Andrei Pochtovyi, Daria Ogarkova, Anna Kuznetsova, Ruslan Adgamov, Elena Tsyganova, Inna Kulikova, Andrei Plutnitskii, Aleksandr Gintsburg, Vladimir Gushchin, Aleksei Mazus

TL;DR
This study examines HIV-1 genetic diversity and drug resistance in three Ukrainian regions, finding moderate resistance levels and highlighting the need for ongoing monitoring.
Contribution
The study provides new insights into HIV-1 resistance mutation profiles and genetic diversity in Donetsk, Luhansk, and Zaporizhzhia.
Findings
The overall prevalence of drug resistance mutations to INSTIs was 3.6%.
G140R and Y143R were the most common major drug resistance mutations.
High-level resistance was observed for RAL (57.1%) and CAB (42.9%).
Abstract
The first major HIV outbreak in the Eastern Europe and Central Asia (EECA) region was registered. Phylogeographic analysis revealed that the main exporters of the virus were Donetsk and Lugansk, from which most migration events occurred, and the predominant genetic variant in Donetsk was subtype A. However, despite a relatively high level of understanding of HIV genetic diversity, data on resistance mutations remain limited. The aim of this study is to assess HIV genetic diversity and drug resistance in Donetsk, Luhansk and Zaporizhzhia regions. A comprehensive examination was conducted, encompassing 392 sequences covering the integrase-coding region of the HIV-1 pol gene. Subtyping was achieved through various programs, including COMET, the Stanford Database, BLAST and REGA. The study also involved phylogenetic analysis to clarify HIV genovariants. The profiles and levels of drug…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
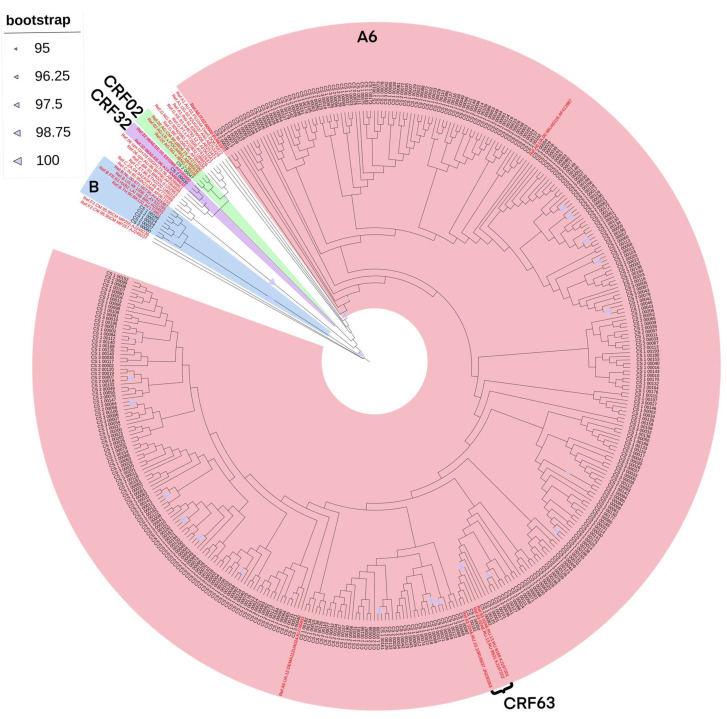 Figure 1
Figure 1- —Ministry of Health of the Russian Federation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS drug development and treatment · HIV Research and Treatment · HIV/AIDS Research and Interventions
1. Introduction
The first major HIV outbreak in the Eastern Europe and Central Asia (EECA) region was registered among injection drug users (IDUs) in the southern regions of Ukraine (Odessa and Nikolaev), from where the subtype A virus (currently classified as sub-subtype A6) rapidly spread through drug trafficking networks across the territory of the post-Soviet countries in the 1990s [1,2,3,4,5]. Subsequently, the route of transmission shifted from parenteral to sexual, mainly due to heterosexual contact [6].
One of the factors influencing the spread of HIV infection is population migration activity. Phylogeographic analysis revealed that the main exporters of the virus were Donetsk and Lugansk, from which most migration events occurred [7], and the predominant genetic variant in Donetsk was subtype A [2].
Currently, Europe is experiencing an increase in the number of HIV infections caused by migration flows from Ukraine and the A6 sub-subtype [8]. Also, the studies indicate that approximately 69% of refugees from Ukraine received a dolutegravir (DTG)-based regimen and 22% had received an efavirenz (EFV)-based ART. The other medications employed included lopinavir/ritonavir (LPV/r) at a rate of 6% and bictegravir (BIC) at a frequency of 2% [9].
However, despite a relatively high level of understanding of HIV genetic diversity, data on resistance mutations remain limited. At the same time, the “HIV Drug Resistance—Brief Report 2024” (the World Health Organization, WHO) noted that actual levels of drug resistance to dolutegravir (DTG), a promising second-generation antiretroviral drug from the integrase strand transfer inhibitors, were higher than those observed in clinical trials. In Ukraine, in the period of 2020–2021, the overall prevalence of HIV drug resistance to DTG was 3.7%, and among individuals already receiving dolutegravir-containing antiretroviral treatment (ART) regimens, it was 6.6% [10]. Thus, there is currently a risk of the spread of drug-resistant HIV-1 variants, particularly to DTG, from Donetsk to Europe and EECA countries, including the Russian Federation.
The aim of this study is to assess HIV genetic diversity and drug resistance in Donetsk, Luhansk and Zaporizhzhia regions. This study presents preliminary results that are part of a larger scientific study.
2. Materials and Methods
2.1. Study Participants and Data Collection
Plasma samples (n = 193) and whole blood samples (n = 199) collections were used as study material. We used a consecutive sampling method. The study included patients who visited regional AIDS centers as part of their routine follow-up and registration in 2025. These centers serve as the primary point of medical care and ART distribution for all registered HIV-positive individuals in these regions. Therefore, the vast majority of the regional patient population, regardless of their gender, age and route of infection, passes through these facilities. This makes our sample representative of the population.
These biological samples were obtained from unique patients with HIV (naive and ART-treated) from three medical institutions in the Donetsk, Luhansk and Zaporizhzhia regions in 2025. The HIV sequences obtained, along with the corresponding demographic, clinical, and epidemiological information, were analyzed. These sequences covered the integrase-coding region of the HIV-1 pol gene.
Adherence to the Declaration of Helsinki was ensured by obtaining informed consent from all HIV-positive individuals participating in this research. To protect patient privacy, all data were anonymized and assigned unique codes.
2.2. HIV-1 RNA/DNA Extraction and Sequencing
Blood collection and fractionation procedures to obtain blood plasma were carried out by employees of the medical institutions in the Donetsk, Luhansk and Zaporizhzhia regions.
Commercial genotyping kits (the HiPure Viral RNA Kit (Magen Biotechnology Co., Ltd., Guangzhou, China) and the HiPure Blood DNA Mini Kit (Magen Biotechnology Co., Ltd., Guangzhou, China) were used for HIV-1 RNA extraction from plasma samples and for HIV-1 DNA extraction from whole blood, respectively.
The AmpliSens^®^ HIV-Monitor-FRT Quantitive (Central Research Institute of Epidemiology, Moscow, Russia) commercial kit was used to determine viral load. In cases when the viral load was undetectable (<1000 copies/mL), further work was carried out with proviral DNA.
In-house methods were used for Sanger-based sequencing of the HIV-1 pol gene regions encoding the INT (4230–5096 bp, according to the HXB2 strain, GenBank accession number K03455).
2.3. Determination of the HIV-1 Genetic Variants
Firstly, multiple sequence alignments were generated using the ClustalW module integrated into the AliView v.1.27 software package [11]. In case of detection of problematic regions in the resulting alignments, additional manual alignments were performed. The final alignment covered a minimum of 696 nucleotides in length (4230–5096 bp, according to the HXB2 strain, GenBank accession number K03455).
Initial identification of HIV-1 genetic variants was carried out using the following online tools: COMET HIV-1 (https://comet.lih.lu/, accessed on 26 December 2025), the HIVdb Program Sequence Analysis (available via the Stanford University website), HIV BLAST (version 2.2.30) (https://www.hiv.lanl.gov/content/sequence/BASIC_BLAST/basic_blast.html, accessed on 26 December 2025) and the REGA HIV-1 Subtyping Tool (version 3.46), following the protocol described in a previous study [12].
To validate the genotyping results, phylogenetic analysis was conducted. Reference sequences for HIV-1 genetic variants were downloaded from the Los Alamos National Laboratory HIV Sequence Database (https://www.hiv.lanl.gov/content/sequence/NEWALIGN/align.html, accessed on 26 December 2025) and incorporated into the analysis.
The phylogenetic analysis was performed by the maximum likelihood method using IQ-TREE (version 2.0.3) [13] with the following command-line arguments: iqtree-s [sequence alignment file]-m MFP-bb 1000-alrt 1000. The analysis incorporated 1000 bootstrap replicates alongside the Shimodaira–Hasegawa approximate likelihood ratio test (SH-aLRT). Clusters with SH-aLRT support values above 0.9 were considered statistically significant. The best-fit nucleotide substitution model was degermed automatically
The resulting phylogenetic tree was visualized and annotated using iTOL (Interactive Tree of Life) software (version 7) [14].
2.4. Analysis of Drug Resistance Mutations
Drug resistance mutation analysis (determination of the integrase strand transfer inhibitors (INSTIs) was performed using the Sierra algorithm implemented in the HIVdb Program: Mutations Analysis Tool version 9.7 (Stanford University HIV Drug Resistance Database; https://hivdb.stanford.edu/hivdb/by-sequences/, accessed on 26 December 2025).
The Calibrated Population Resistance Tool (CPR) was used to perform drug resistance analysis among patients with HIV not on ART (PrimDR).
The Stanford HIV Drug Resistance Database (including the HIVdb Program, version 9.8, and the Calibrated Population Resistance Tool (CPR)) was used to characterize and interpret HIV drug resistance (DR) levels and drug-resistance mutations (DRMs), including surveillance drug-resistance mutations (SDRMs) [15].
DR levels were categorized into five tiers according to the Stanford penalty score: susceptible (score 0–9); potential low-level resistance (score 10–14); low-level resistance (score 15–29); intermediate resistance (score 30–59); and high-level resistance (score ≥ 60). This classification was applied for the following INSTIs: bictegravir (BIC), cabotegravir (CAB), dolutegravir (DTG), elvitegravir (EVG) and raltegravir (RAL). Sequences with a Stanford penalty score of 15 or higher were considered resistant to these drugs.
2.5. Statistical Analysis
The analysis was carried out using the R programming language (R version 4.2.2, RStudio version 2023.03.0 + 386, Inc. Software, Boston, MA, USA), as well as STATISTICA software (version 6.0, StatSoft, Tulsa, OK, USA).
Categorical data evaluated in the study were presented as proportions and frequencies and their comparisons were carried out using the chi-square test (χ^2^); if unstable, Yates’ correction or Fisher’s two-tailed exact test was applied. Differences were considered statistically significant at p-value < 0.05. Data visualization was performed using the R programming language.
3. Results
3.1. Profile of the Study Cohort
A total of 392 unique HIV-1 sequences were analyzed, obtained from patients with HIV in the Donetsk, Luhansk and Zaporizhzhia regions in 2025. Of these, 352 patients were receiving ART at the time of sampling, while 5 patients were not receiving ART, and information about the ART status for 35 other patients was not available. The most commonly used ART regimens in the study cohort of patients were TDF/3TC/DTG, TDF/3TC/EFV, TDF/FTC/ESV. The study cohort’s average duration time on ART was 101 (from 59 to 141) months, equivalent to 8 (from 4 to 11) years.
The median age of the participants (age data was available for 372 patients) was 43 years, ranging from 2 to 68 (Q1 = 36, Q3 = 49 years). Among the cohort, 204 (52.2%) individuals were male, and 187 (47.8%) individuals were female (gender data was available for 391 patients).
The main risk factor was sexual contact (265, 67.6%), followed by intravenous drug use (78, 19.9%). In the structure of sexual transmission, the heterosexual contact were most common (98.9%), followed by homosexual contact (0.7%) and unspecified (0.4%).
Data on the median (IQR) CD4 cell counts and median (IQR) HIV RNA for treated and untreated patients are presented in Table 1.
3.2. Phylogenetic Analysis
The combined refined results of the initial identification of HIV-1 genetic variants and phylogenetic analysis showed the following ratios: A6—382 of sequences (97.45%), B—5 (1.28%), CRF63_02A6—3 (0.77%), CRF02_AG—1 (0.25%) and CRF32_06A6—1 (0.25%) of sequence (Figure 1).
3.3. Analysis of Drug Resistance Mutations
To assess the prevalence of key DRMs, we analyzed the INT sequences (n = 392) targeting resistance to INSTIs.
In four patients without a history of ART, no resistance mutations were detected. The overall prevalence of drug resistance mutations to the integrase strand transfer inhibitors (INSTIs) among the studied patients was 3.6% (95% CI, 1.7–5.4%) (Table 2).
The most commonly detected major DRMs for INSTIs were G140R (4, 28.6%) and Y143R (3, 21.4%), followed by R263K (2, 14.3%), G140RG (2, 14.3%), Y143YS (2, 14.3%), Y143YC (1, 7.1%) and Q148QR (1, 7.1%). Considering the different lengths of the sequences, it is possible that the frequency of mutation R263K may even be higher. One patient exhibited a combination of these mutations: G140R + R263K (major) and G163R (accessory); a further four patients had both major and accessory mutations: for two patients—Y143R + T97A, and for two patients—G140R + G163R (Table 2).
A high-level resistance to INSTIs was observed for RAL—8/14 (57.1%), CAB—6/14 (42.9%), and EVG—2/14 (14.3%). Intermediate resistance was observed to vary across all the drugs presented: EVG—8/14 (57.1%), RAL—5/14 (35.7%), BIC and DTG—3/14 (21.4%) for each drug and CAB—2/14 (14.3%) (Table 2).
Among other mutations, the most common was the L74I polymorphism, which was presented in 370 patients (94.6%, 95% CI, 92.1–96.7%).
4. Discussion
Overall, the results obtained reflect the current trends in HIV infection in the EECA region, within the context of demographic and epidemiological indicators [16,17]. It is noteworthy that approximately 19% of HIV transmission cases were among IDUs, which aligns with the overall results for Russia. This indicates a definite shift in transmission routes in the region, with HIV infection spreading predominantly through heterosexual contact.
In terms of HIV-1 genetic diversity, the region maintains the historically justified absolute dominance of HIV-1 sub-subtype A6 [1,2,3,4,5]. However, even within this context, the study cohort exhibits a high genetic diversity of the virus, potentially resulting from active migration processes. Additionally, the recombinant form CRF32_06A6 was identified in the study area for the first time. This recombinant form was initially identified and described in Estonia in the mid-2000s as the dominant genetic variant among IDUs [18]. According to clinical and epidemiological data, the patient with this recombinant form of HIV-1 was infected through heterosexual contact. This discovery necessitates further monitoring due to the potential for continued transmission and spread of CRF32_06A6 in the region.
Given the significant genetic fragment of the A6 genovariant the integrase-coding region of the HIV-1 pol gene within CRF32_06A6, it is possible that this recombinant form also carries the L74I polymorphism. This polymorphism has been shown to significantly increase the risk of virological failure when using long-acting injectable antiretroviral drugs, CAB/RPV, which are commonly used in Europe and are now included in clinical guidelines for treatment in Russia since 2024 [19,20].
Despite the low percentage (3.6%) of patients with major drug resistance mutations to INSTIs, the results obtained warrant attention and further monitoring. Notably, the most common mutation in the study cohort was G140R, a rare non-polymorphic mutation that reduces the susceptibility to CAB [21]. It can be assumed that this mutation is locally distributed among certain groups. Additionally, a specific mutational background may be required for G140R to reduce the susceptibility to CAB, as three out of four patients (75%) with this mutation also had additional major (R263K) and accessory (G163R) mutations, which may also potentially reduce the virus’s sensitivity to other antiretroviral drugs: EVG, DTG, BIC, and CAB [22,23].
The second most common mutation was Y143R, which reduces the susceptibility to RAL by approximately 20-fold. In combination with T97A, which was observed in 75% of patients with the Y143R mutation, it reduces the susceptibility by 100-fold [24,25,26,27]. It is worth noting that among patients with major DRMs, only one patient had a history of RAL use. This may indicate cases of transmitted HIV-1 drug resistance in the region. Similarly, among patients with intermediate-level resistance to DTG, none had a history of using DTG.
5. Conclusions
The results presented in this study are part of a further larger research project and should be considered preliminary. The results of this study indicated a moderate HIV-1 resistance situation in the Donetsk, Luhansk and Zaporizhzhia regions. However, considering several limitations of the study, including the lack of a representative sample of treatment-naive patients, further expansion of this research is necessary. Therefore, ongoing monitoring of HIV infections in these areas is essential.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bobkov A. Cheingsong-Popov R. Selimova L. Ladnaya N. Kazennova E. Kravchenko A. Fedotov E. Saukhat S. Zverev S. Pokrovsky V. An HIV type 1 epidemic among injecting drug users in the former Soviet Union caused by a homogeneous subtype A strain AIDS Res. Hum. Retroviruses 1997131195120110.1089/aid.1997.13.11959310286 · doi ↗ · pubmed ↗
- 2Saad M.D. Shcherbinskaya A.M. Nadai Y. Kruglov Y.V. Antonenko S.V. Lyullchuk M.G. Kravchenko O.N. Earhart K.C. Sanchez J.L. Birx D.L. Molecular epidemiology of HIV Type 1 in Ukraine: Birthplace of an epidemic AIDS Res. Hum. Retroviruses 20062270971410.1089/aid.2006.22.70916910825 · doi ↗ · pubmed ↗
- 3Booth R.E. Kwiatkowski C.F. Mikulich-Gilbertson S.K. Brewster J.T. Salomonsen-Sautel S. Corsi K.F. Sinitsyna L. Predictors of risky needle use following interventions with injection drug users in Ukraine Drug Alcohol. Depend.200682 S 49S 5510.1016/S 0376-8716(06)80009-816769446 · doi ↗ · pubmed ↗
- 4Dehne K.L. Grund J.P.C. Khodakevich L. Kobyshcha Y. The HIV/AIDS epidemic among drug injectors in Eastern Europe: Patterns, trends and determinants J. Drug Issues 19992972977610.1177/002204269902900402 · doi ↗
- 5Sarang A. Stuikyte R. Bykov R. Implementation of harm reduction in Central and Eastern Europe and Central Asia Int. J. Drug Policy 20071812913510.1016/j.drugpo.2006.11.00717689355 · doi ↗ · pubmed ↗
- 6Vitek C.R. Čakalo J.I. Kruglov Y.V. Dumchev K.V. Salyuk T.O. BožičevićI. Baughman A.L. Spindler H.H. Martsynovska V.A. Kobyshcha Y.V. Slowing of the HIV epidemic in Ukraine: Evidence from case reporting and key population surveys, 2005–2012 P Lo S ONE 20149 e 10365710.1371/journal.pone.010365725251080 PMC 4174506 · doi ↗ · pubmed ↗
- 7Vasylyeva T.I. Liulchuk M. Friedman S.R. Sazonova I. Faria N.R. Katzourakis A. Babii N. Scherbinska A. ThézéJ. Pybus O.G. Molecular epidemiology reveals the role of war in the spread of HIV in Ukraine Proc. Natl. Acad. Sci. USA 20181151051105610.1073/pnas.170144711529339468 PMC 5798316 · doi ↗ · pubmed ↗
- 8Serwin K. Mielczak K. Urbańska A. Aksak-Wąs B. Karasińska-Cieślak M. Ząbek P. Siwak E. Cielniak I. Jabłonowska E. Jakubowski P. Comparison of HIV-1 A 6 dispersal dynamics in Poland before and after the war in Ukraine P Lo S Pathog.202521 e 101336910.1371/journal.ppat.101336940768555 PMC 12342253 · doi ↗ · pubmed ↗