Mpox Clade IIb Virus Introduction into Kinshasa, Democratic Republic of the Congo, July 2025
Tony Wawina-Bokalanga, Eddy Kinganda-Lusamaki, Christian Ngandu, Prince Akil-Bandali, Jérémie Kundey-Mafu, Nadege Ngombe, Laurens Liesenborghs, Princesse Paku-Tshambu, Lorenzo Subissi, Pauline-Chloé Muswamba-Kayembe, Samy Tessi-Mvutukulu, Jacques Santini-Mafuta

TL;DR
This paper reports the first cases of a new mpox virus lineage in Kinshasa, imported from West Africa and locally transmitted.
Contribution
The study identifies and genetically characterizes the first Clade IIb/sh2017 mpox virus cases in the DRC.
Findings
Two cases of Clade IIb/sh2017 MPXV were identified in Kinshasa, DRC.
The virus was imported from West Africa and later transmitted locally.
Genomic analysis placed the virus in lineage G.1, identified in Sierra Leone in January 2025.
Abstract
Clade I mpox virus (MPXV) is endemic in the Democratic Republic of the Congo (DRC). Recent studies have described the changing epidemiology of mpox in the country, which has been mainly characterized by the emergence of new MPXV lineages, Clade Ib/sh2023 and Ia/sh2024, associated with sustained human-to-human transmission. Both Clade Ib/sh2023 and Ia/sh2024 are co-circulating in Kinshasa, the capital city of the DRC. Here, we report the first two cases of Clade IIb/sh2017 identified in Kinshasa, DRC, imported from West Africa and locally transmitted. Clinical specimens were collected and tested by PCR. We performed whole genome sequencing using a tiled-amplicon sequencing approach with Clade IIb MPXV-specific primers. The phylogenetic tree shows that Kinshasa Clade IIb MPXV is assigned to Clade IIb/sh2017 within the newly designated lineage G.1, as identified in January 2025 in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
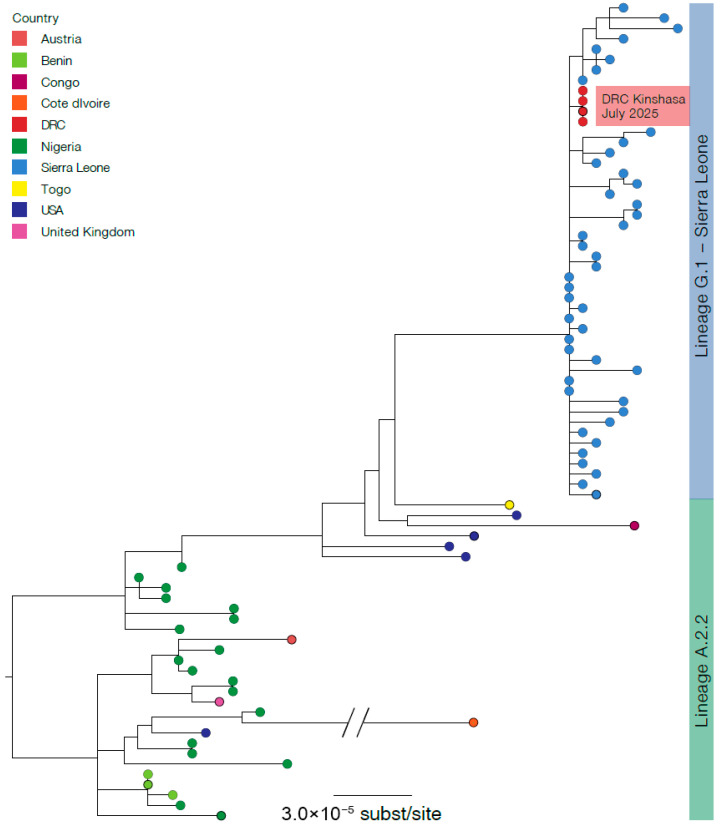 Figure 1
Figure 1- —Belgian Directorate-General for Development Cooperation and Humanitarian Aid
- —Research Foundation Flanders (“Fonds voor Wetenschappelijk Onderzoek–Vlaanderen”
- —Institute of Tropical Medicine Structurele Onderzoeksfinanciering (Flemish Government; Science, Technology, and Innovation)
- —Africa CDC
- —Global Health European and Developing Countries Clinical Trials Partnership 3 (EDCTP3) Joint Undertaking
- —US Department of Defense Threat Reduction Agency
- —US Department for Agriculture Research Service
- —Canadian Institutes of Health Research
- —International Mpox Research Consortium (IMReC)
- —Canadian Institutes of Health Research
- —International Development Research Centre
- —US NIAID/NIH
- —Center for Research in Emerging Infectious Disease-East and Central Africa (CREID-ECA)
- —Agence Française de Développement
- —US Department of Defense Threat Reduction Agency
- —US Department for Agriculture Research Service
- —Wellcome Trust
- —European Union
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPoxvirus research and outbreaks · vaccines and immunoinformatics approaches · HIV Research and Treatment
1. Introduction
Mpox is a zoonotic disease caused by two distinct clades of mpox virus (MPXV); Clade I and Clade II, each divided into two clades, a and b [1,2]. Although the virus can be transmitted through zoonotic spillover, in recent years, at least three different lineages have emerged and spread through sustained human-to-human transmission: Clade IIb/sh2017, Clade Ib/sh2023, and Clade Ia/sh2024 [2,3,4].
The Democratic Republic of the Congo (DRC) has traditionally been the epicenter of Clade I MPXV. For several decades, the country has seen an increasing number of outbreaks caused by zoonotic spillover of Clade Ia [5,6]. In 2024, Clade Ib/sh2023 emerged, prompting the World Health Organization to declare mpox for the second time a public health emergency of international concern [7]. Shortly thereafter, Clade Ia/sh2024 was detected in the capital Kinshasa, where both lineages continue to co-circulate [3,8]. Despite efforts to curb the epidemic, the DRC continues to report the highest number of overall suspected and confirmed mpox cases worldwide [9]. Between 1 January and 20 July 2025, the Ministry of Public Health of DRC, through the Institut National de Santé Publique, reported 61,532 suspected cases of mpox (14,351 PCR confirmed) across all 26 provinces.
On the other hand, human cases of MPXV Clade II were first observed in West Africa [10]. Following the emergence of Clade IIb/sh2017 in Nigeria in 2017 [11], the virus spread internationally and caused the global 2022 mpox outbreak that affected more than 100 countries [12,13]. Although global case numbers have since subsided, Sierra Leone is currently experiencing a large Clade IIb/sh2017 outbreak [14]. In contrast, throughout the global epidemic, the DRC had not reported any cases of Clade IIb/sh2017 to date.
Here, we report the first two Clade IIb/sh2017 mpox cases identified in the DRC, imported from West Africa by the index case and locally transmitted to his wife, with phylogenetic linkage to the ongoing outbreak in Sierra Leone.
2. Case Investigations
Between 21 and 26 July 2025, a 45–49-year-old man presented himself to the General Referral Hospital of Kinkole (HGRK—Nsele Health Zone) in Kinshasa, DRC with vesicle lesions. The patient self-reported symptom onset two days before the medical examination, with fever and headache, followed by the appearance of vesicle lesions on the face, palms, and penis, as well as inguinal lymphadenopathy. He had self-medicated for the fever with acetaminophen. He reported no contact or exposure to animals during the preceding three weeks, nor any sexual activities or known contact with MPXV-infected individuals. He also reported a prior history of smallpox vaccination and had a smallpox vaccination scar. He had recently traveled from the Ivory Coast to Togo, and finally to DRC, via transit through Jomo Kenyatta International Airport, Kenya.
Suspecting mpox, the physician immediately transferred the patient to isolation at the mpox treatment unit. Blood and vesicle swab specimens were collected for laboratory analysis. The dual HIV/syphilis Combo rapid diagnostic test (SD Biosensor, Suwon-si, Republic of Korea) was negative for both infections. Initial testing with the Xpert Mpox assay on the GeneXpert system (Cepheid, Sunnyvale, CA, USA), which detects Clade II and non-variola Orthopoxviruses, including Clade I MPXV, at HGRK-detected MPXV Clade II in the vesicle swab sample. Subsequently, vesicle and blood specimens were shipped to the Institut National de Recherche Biomédicale (INRB), Kinshasa, for diagnostic confirmation and whole-genome sequencing of MPXV.
As part of routine contact tracing, nine individuals were identified as high-risk contacts, including the patient’s wife and their three children, one uncle, one nephew, one hairdresser, one renter, and one healthcare worker. Because of sexual contact with the index case, a nasopharyngeal swab was collected from the patient’s wife—aged 35–39 years old—on day 2 after her last exposure to the patient. PCR testing performed at HGRK with the Xpert Mpox assay (Cepheid, Sunnyvale, CA, USA) confirmed the presence of Clade II MPXV DNA in the sample. Consequently, she was immediately admitted to the mpox treatment unit and reported having a fever, swelling of the vulva, and itching. She had vesicle lesions on the face, palms, vulva, and trunk. Vesicle and nasopharyngeal swabs were collected and shipped to INRB, Kinshasa. A follow-up among the other contacts for 21 days is still ongoing.
At INRB, vesicle swab samples of both patients were re-tested with the RADI RP022 mpox detection kit (KH Medical, Pyeongtaek-si, Republic of Korea) on the RADIONE system (KH Medical, Pyeongtaek-si, Republic of Korea), a fully automated point-of-care molecular diagnostic device. In addition, real-time PCR was performed in triplicate on each specimen from both patients (vesicle and blood from the index case, and vesicle and nasopharyngeal swab from his wife) using the RADI FAST RV015R mpox detection kit (KH Medical, Republic of Korea), also following the manufacturer’s instructions.
Following PCR confirmation, multiplex tiling PCR was performed using the Clade IIb MPXV primer pools designed by Chen et al. [15]. The library was also prepared in triplicate using the rapid sequencing DNA V14 barcoding kit (SQK-RBK114.96; Oxford Nanopore Technologies (ONT), Oxford, UK), following the manufacturer’s instructions. The sequencing library was loaded on a R10.4.1 flow cell and run on the GridION sequencer.
MPXV consensus genomes were generated by processing concatenated FASTQ files using the artic-mpxv-nf workflow v2.1.0 (https://github.com/artic-network/artic-mpxv-nf, accessed on 27 July 2025), and the Clade II MPXV genome (GenBank ID: NC_063383.1) was used as a reference. The Nextclade online tool (https://clades.nextstrain.org/, accessed on 27 July 2025) was used to assign the clade of MPXV genomes. Multiple sequence alignment against the Clade II MPXV reference genome (GenBank ID: NC_063383.1) and APOBEC3 mutation analysis were performed using SQUIRREL (https://github.com/aineniamh/squirrel, accessed on 27 July 2025). A phylogenetic tree was inferred using IQ-TREE v2.1.4 [16] with the HKY substitution model [17].
PCR results obtained from the RADIONE indicated amplification cycle threshold (Ct) values of 19.09 and 19.03 for Clade II MPXV in vesicle samples from the index case and his wife, respectively. The RADI FAST real-time PCR assay showed mean Ct values for Clade II of 21.47 and 28.62 in the vesicle and blood specimen triplicates from the first patient, and mean Ct of 21.23 and 34.68 in the vesicle and nasopharyngeal specimen triplicates from the patient’s wife (Table 1).
Of the index patient, MPXV genomes were generated from the vesicle swab and blood sample with horizontal genome coverages of 94.19% and 93.39%, respectively. Of the index patient’s wife, the vesicle and nasopharyngeal swabs generated MPXV genomes with horizontal genome coverages of 93.90% and 81.85%, respectively. The four MPXV genomes were similar, assigned to Clade IIb/sh2017 within the newly designated lineage G.1, and clustered with MPXV Clade IIb/sh2017 sequences recently identified in Sierra-Leone (https://virological.org/t/genomic-epidemiology-of-mpox-virus-in-sierra-leone/995, accessed on 5 August 2025) (Figure 1).
Although MPXV Clade IIb/sh2017 sequences obtained from two cases identified in July 2025 in Kinshasa, DRC, are genetically identical and cluster with sequences from the 2025 Sierra Leone mpox outbreak, they differ by two APOBEC3-like mutations (C92702T and C182135T) and one non-APOBEC3 mutation (C161570A), when compared with reference genomes PP_00341CY.3 and PP_00341DW.3 (Pathoplexus accession numbers). In addition, Clade IIb/sh2017 sequences from this study exhibit APOBEC3 mutation enrichment, with approximately 69% (67/97) of reconstructed SNPs consistent with APOBEC3 editing (Table 2). Together, this study indicates that transmission of MPXV Clade IIb/sh2017 in Kinshasa, DRC, resulted from human-to-human transmission.
A recent analysis by Campbell AKO et al. on the genomic epidemiology of Clade IIb circulation in Sierra Leone provided additional insights into the linkages between ongoing circulation in West Africa and the public health impacts of Clade IIb in Sierra Leone in 2025 [18]. This investigation identified linkages between Clade IIb circulation in Sierra Leone with a common ancestor from Nigeria, and linkages to additional regions in West Africa, including Togo. These observations, as well as the continued reporting of infections in multiple West African countries, highlights the ongoing circulation of Clade IIb MPXV more broadly in this region of the continent, the risks for cryptic circulation and ongoing expansion of the virus to new non-endemic regions of the continent, and the need for increased healthcare access and resilience, as well as community engagement regarding mpox.
3. Conclusions
The co-circulation of Clade Ib/sh2023 and Clade Ia/sh2024, with the novel importation of Clade IIb/sh2017 and its potential spread in Kinshasa -the largest metropolitan area of the DRC, with international and national connections- warrants enhanced genomic and epidemiological surveillance in the region. This finding underscores the urgent need to improve rapid detection and isolation of mpox cases, and enhance contact-tracing efforts, as well as strengthen genomic surveillance and implement vaccine strategies to mitigate the risk of widespread dissemination of Clade IIb/sh2017 and other MPXV variants in general across DRC provinces.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO) Monkeypox: Experts Give Virus Variants New Names 2022 Available online: https://www.who.int/news/item/12-08-2022-monkeypox--experts-give-virus-variants-new-names(accessed on 20 September 2024)
- 2Vakaniaki E.H. Kacita C. Kinganda-Lusamaki E. O’Toole A. Wawina-Bokalanga T. Mukadi-Bamuleka D. Amuri-Aziza A. Malyamungu-Bubala N. Mweshi-Kumbana F. Mutimbwa-Mambo L. Sustained human outbreak of a new MPXV clade I lineage in eastern Democratic Republic of the Congo Nat. Med.2024302791279510.1038/s 41591-024-03130-338871006 PMC 11485229 · doi ↗ · pubmed ↗
- 3Wawina-Bokalanga T. Merritt S. Kinganda-Lusamaki E. Jansen D. Halbrook M. O’Toole A. Pukuta-Simbu E. Vakaniaki E.H. Ola-Mpumbe R. Kwete-Mbokama P. Epidemiology and phylogenomic characterisation of two distinct mpox outbreaks in Kinshasa, DR Congo, involving a new subclade Ia lineage: A retrospective, observational study Lancet 2025406637510.1016/S 0140-6736(25)00294-640617661 · doi ↗ · pubmed ↗
- 4Ruis C. Lusamaki E. O’Toole A. Otieno J.R. Colquhoun R. Roemer C. Wawina-Bokalanga T. Tshiani-Mbaya O. Jansen D. Makangara J.C. A systematic nomenclature for mpox viruses causing outbreaks with sustained human-to-human transmission Nat. Med.2025312854285810.1038/s 41591-025-03820-640731088 · doi ↗ · pubmed ↗
- 5Bangwen E. Diavita R. De Vos E. Vakaniaki E.H. Nundu S.S. Mutombo A. Mulangu F. Abedi A.A. Malembi E. Kalonji T. Suspected and confirmed mpox cases in DR Congo: A retrospective analysis of national epidemiological and laboratory surveillance data, 2010–2023 Lancet 202540540841910.1016/S 0140-6736(24)02669-239892912 PMC 7618260 · doi ↗ · pubmed ↗
- 6Kinganda-Lusamaki E. Amuri-Aziza A. Fernandez-Nunez N. Makangara-Cigolo J.C. Pratt C. Vakaniaki E.H. Hoff N.A. Luakanda-Ndelemo G. Akil-Bandali P. Nundu S.S. Clade I mpox virus genomic diversity in the Democratic Republic of the Congo, 2018-2024: Predominance of zoonotic transmission Cell 20251884143945457310.1016/j.cell.2024.10.017 · doi ↗ · pubmed ↗
- 7World Health Organization (WHO) WHO Director-General Declares Mpox Outbreak a Public Health Emergency of International Concern 2024 Available online: https://www.who.int/news/item/14-08-2024-who-director-general-declares-mpox-outbreak-a-public-health-emergency-of-international-concern(accessed on 21 August 2024)
- 8Wawina-Bokalanga T. Akil-Bandali P. Kinganda-Lusamaki E. Lokilo E. Jansen D. Amuri-Aziza A. Makangara-Cigolo J.C. Pukuta-Simbu E. Ola-Mpumbe R. Muyembe M. Co-circulation of monkeypox virus subclades Ia and Ib in Kinshasa Province, Democratic Republic of the Congo, July to August 2024 Eurosurveillance 202429240059210.2807/1560-7917.ES.2024.29.38.240059239301745 PMC 11484285 · doi ↗ · pubmed ↗