Human Papillomavirus Genotype Landscape Across Cervical Cytology Grades and Impact of HIV Among Women of Eastern Cape Province, South Africa
Sinazo Kondlo, Nwabisa Giyose, Charles B. Businge, Zizipho Z. A. Mbulawa

TL;DR
This study examines HPV genotype distribution across cervical cytology grades and HIV status in South African women, revealing high HPV prevalence and differences in genotype patterns.
Contribution
The study provides new insights into HPV genotype distribution and its association with HIV status in cervical cancer prevention.
Findings
HPV prevalence increases with abnormal cervical cytology, reaching 93.8% in ASC-US and 100% in LSIL.
Non-HPV vaccine types dominate in HSIL and cervical cancer, highlighting gaps in current prevention strategies.
HIV status influences HPV genotype patterns, though overall prevalence does not significantly increase with HIV co-infection.
Abstract
Continuous surveillance of human papillomavirus (HPV) prevalence and genotype distribution in different cervical cytology grades is necessary for cervical cancer prevention and monitoring. This study investigated the distribution of HPV genotypes and associated factors, stratified by cervical cytology grades and human immunodeficiency (HIV) status, among women in the Eastern Cape Province, South Africa. A total of 540 women were recruited from a community health facility and a referral hospital in the OR Tambo District Municipality in Eastern Cape Province. HPV detection and genotyping in cervical cells were performed using the Seegene AllplexTM and AnyplexTM II HPV28 assays. HPV prevalence was 60.6% among women with normal cervical cytology, 93.8% among atypical squamous cells of undetermined significance (ASC-US), 100.0% among low-grade squamous intraepithelial lesions (LSILs), 95.2%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
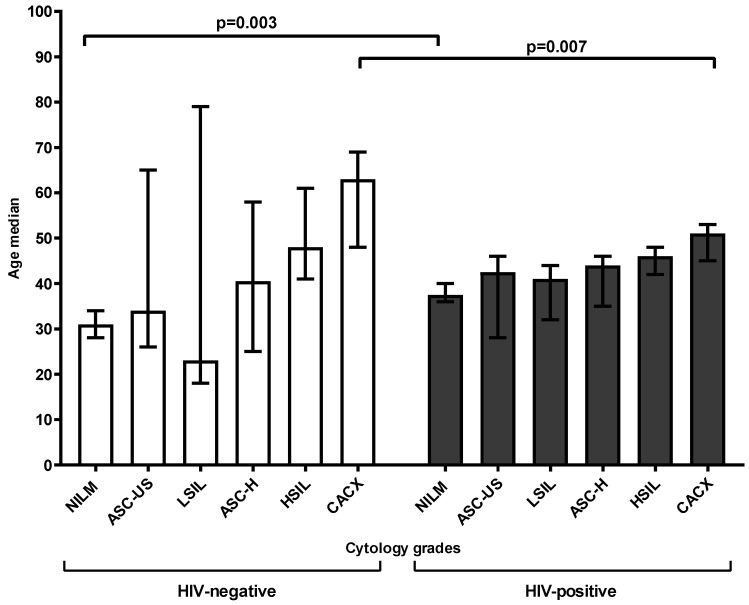 Figure 1
Figure 1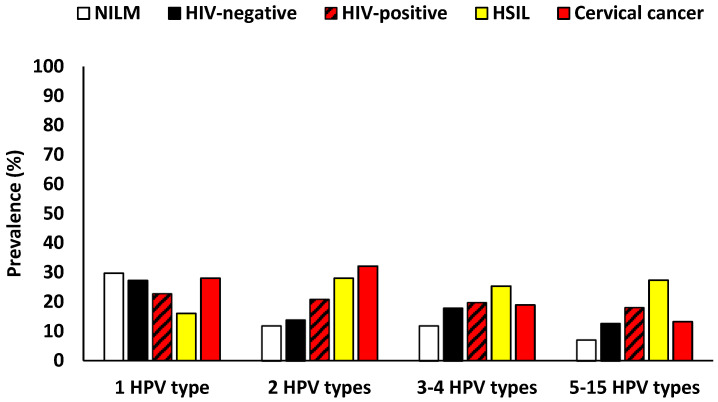 Figure 2
Figure 2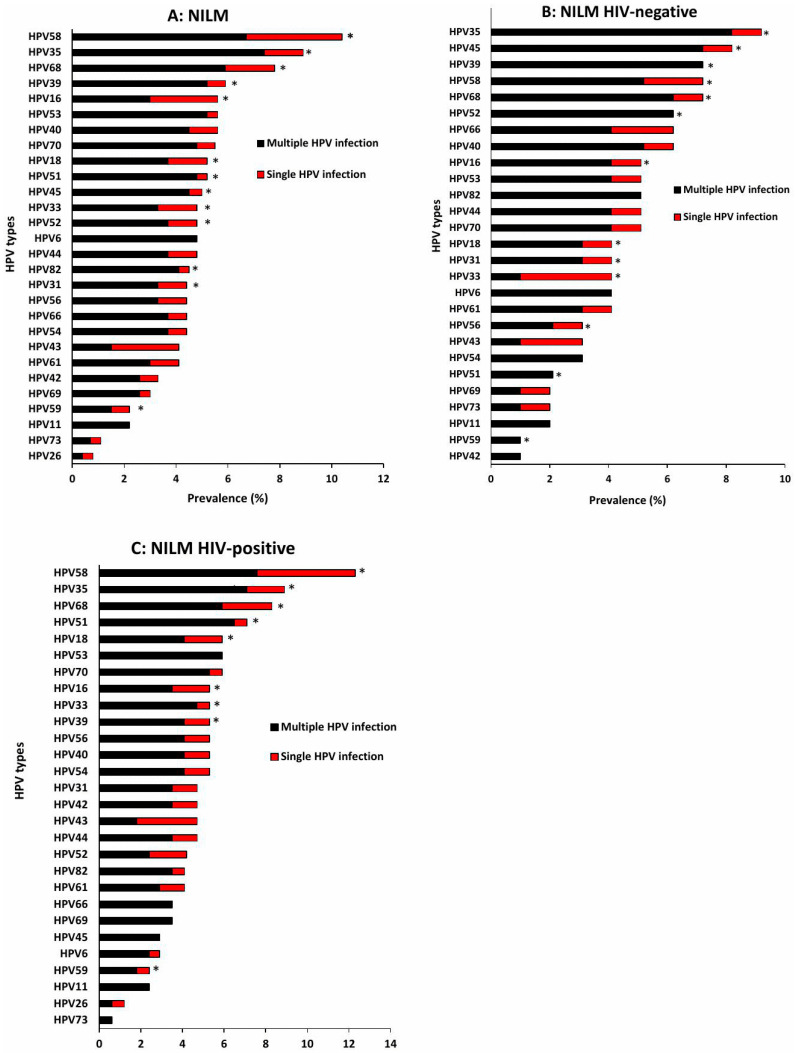 Figure 3
Figure 3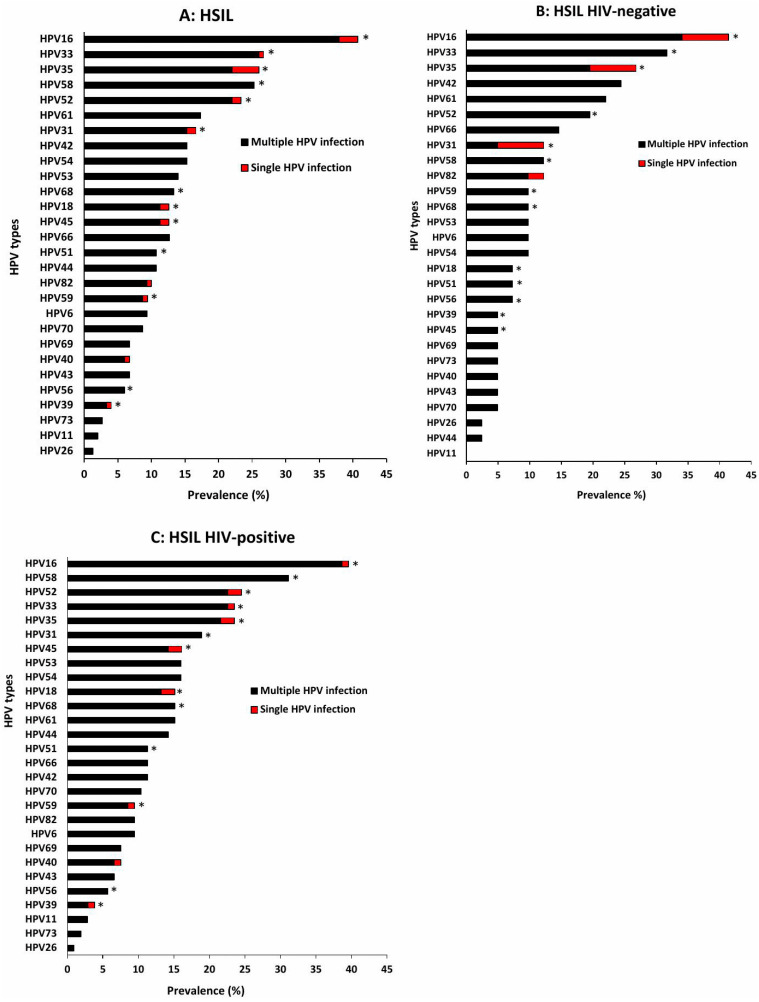 Figure 4
Figure 4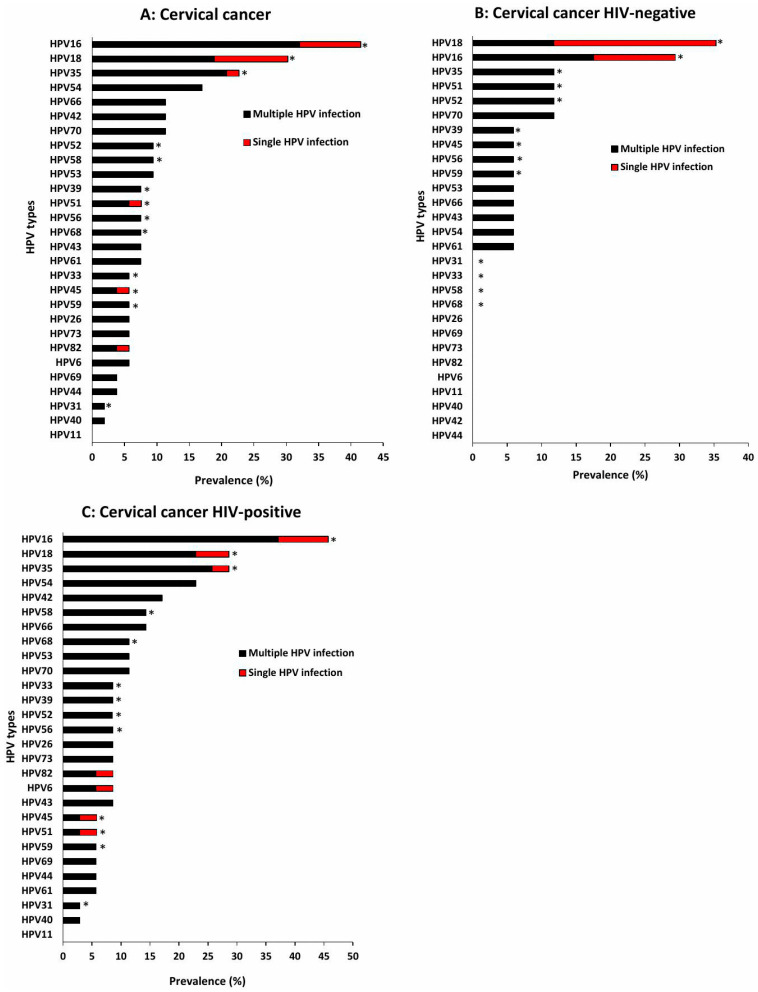 Figure 5
Figure 5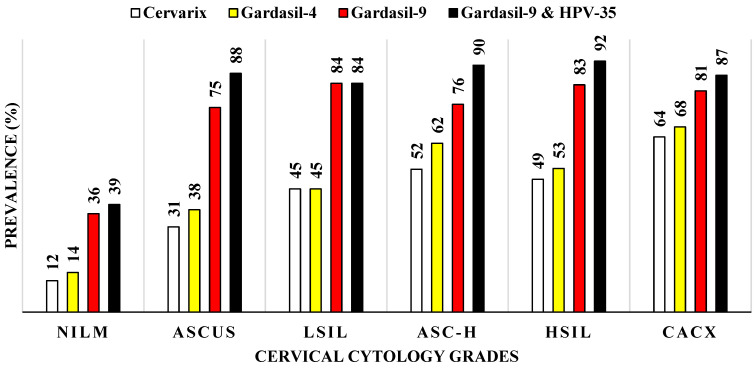 Figure 6
Figure 6- —South African Medical Research Council (SAMRC)
- —South African National Treasury
- —South African National Research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Reproductive tract infections research · Head and Neck Cancer Studies
1. Introduction
Globally, cervical cancer remains a leading cause of cancer-related morbidity and mortality, with low-resource settings being highly affected. In South Africa, cervical cancer is the second most common cancer among women, with an estimated 11,000 new cases and over 5900 deaths annually [1,2]. In the Eastern Cape Province, prevalence and mortality remain elevated despite ongoing public health efforts [1,3]. Persistent infection with high-risk human papillomavirus (HR-HPV) genotypes is the primary cause of cervical precancerous lesions and cervical cancer [4]. Globally, HPV16 and 18 account for approximately 70% of cervical cancer cases [5]; however, HPV genotype distribution varies geographically, influencing both disease progression and vaccine efficacy [4,6].
Alphapapillomavirus are classified as either HR-HPV or low-risk HPV (LR-HPV) based on their oncogenic potential [7,8,9]. While HPV16 and 18 dominate globally in high-grade squamous intraepithelial lesion (HSIL) and cervical cancer cases, African studies report a higher burden of other HR-HPV genotypes, including HPV35, 52, 39, and 56 [10,11,12,13]. Notably, HPV35 has a high prevalence among African women, being detected in approximately 10% of cervical cancer cases in the region, compared with around 2% worldwide, which may limit the effectiveness of current HPV vaccines in Africa [12,14,15].
South Africa has implemented active cervical cancer screening and HPV vaccination programs. A national school-based HPV vaccination program was introduced in 2014, targeting girls around aged nine years in Grade 4 [16]. This program primarily delivers the Cervarix^®^ HPV vaccine, which protects against HPV16 and 18 [17,18]. However, vaccine coverage has declined since its introduction, with initial dose coverage dropping from 86% in 2014 to 37% in 2021, and second dose from 65% to 34%, partially due to the coronavirus disease 2019 (COVID-19) pandemic [19]. Commercial HPV vaccines are also available in the private sector [16]. Cervical cancer screening policy has been in place for decades, recently incorporating HR-HPV testing to triage women for liquid-based cytology. Screening officially begins at 30, except for high-risk women, such as those with HIV, who are screened at diagnosis [20,21].
The high prevalence of HIV in South Africa, affecting over 7 million people, intersects significantly with HPV-related cervical disease [22]. HIV-positive women have a higher prevalence of HPV infection, often with multiple HPV genotypes, and face increased risk of persistent HPV infection and rapid progression to invasive carcinoma compared to HIV-negative women [23,24]. HIV-induced immunosuppression impairs HPV clearance, reduces CD4+ counts, and increases viral loads, contributing to HPV persistence and lesion progression [25]. While antiretroviral therapy (ART) improves immune function, the risk of HPV-associated cervical disease remains elevated, underscoring the need for focused prevention strategies [26].
Despite the known impact of HIV on HPV infection and cervical carcinogenesis, recent data on HPV genotype distribution among South African women, particularly in rural settings, remain limited. Such data are essential to optimize screening, vaccination, and clinical management in populations with high HIV prevalence. Therefore, this study aimed to investigate the distribution of HPV genotypes and associated factors among women in the Eastern Cape Province across different cervical cytology grades and to assess the effect of HIV infection on HPV prevalence, genotype distribution, and cervical lesion severity.
2. Materials and Methods
2.1. Study Setting and Population
This cross-sectional study was conducted at a primary health facility and at Nelson Mandela Academic Hospital, both situated in the King Sabata Dalindyebo (KSD) under the OR Tambo District Municipality, in the Eastern Cape Province of South Africa. The health facility offers primary healthcare services to a diverse population residing in the surrounding areas. Nelson Mandela Academic Hospital is a large provincial, government-funded tertiary teaching hospital that serves as a regional referral center providing specialized medical services. The study population comprised women aged ≥18 years who were referred to the hospital due to abnormal cervical cytology, atypical squamous cells of undetermined significance (ASC-USs), atypical squamous cells, cannot exclude high-grade lesions (ASC-Hs), low-grade squamous intraepithelial lesions (LSILs), HSILs, and cervical cancer, and those that were attending health facility with normal cervical cytology (N = 269). Participants were recruited between June 2023 and June 2025.
The inclusion criteria included women attending the community health facility for any health-related service or referred to Nelson Mandela Academic Hospital (NMAH) for gynaecological concerns or cervical cytology results (ASCUS, ASC-H, LSIL, HSIL, or cervical cancer). Women aged 18 years and above who had previously engaged in sexual activity or were sexually active at the time of recruitment. While, exclusion criteria consisted of pregnant women, those who had never engaged in sexual activity, menstruating or bleeding due to other reasons on the day of recruitment.
2.2. Data Collection
Data collection involved the use of structured questionnaires to gather information on various risk factors. Participants with negative or unknown HIV status were offered an HIV rapid test. Pre and post counselling sessions were done, and a Rapid HIV test (Rapid Anti-HIV 1&2; InTec PRODUCTS, INC; Xiamen, China) was conducted by a qualified health professional. Clinical examinations of participants were conducted by an experienced medical practitioner prior to sample collection. Cervical lesion diagnoses were based on routine cytology and pathology reports; no independent morphological review was conducted for this study. Cervical specimens were collected from all participants using a Digene cervical sampler brush (Qiagen Inc., Gaithersburg, MD, USA) and immediately stored in Digene specimen transport medium (Qiagen Inc., Gaithersburg, MD, USA) and transported to Nelson Mandela Academic Hospital NHLS/WSU virology laboratory for molecular analysis. In the laboratory, cervical specimens were stored at −20 °C until the extraction of nucleic acids.
2.3. Laboratory Investigations
Nucleic acid extraction from cervical specimens was conducted using an automated procedure with the Seegene NIMBUS and STARMag universal extraction system, both developed by Seegene Inc. based in Seoul, Republic of Korea. The extracted nucleic acid was used for both the detection and genotyping of HPV. The Seegene Allplex^TM^ and Anyplex^TM^ II HPV28 (Seegene Inc. Seoul, Republic of Korea) multiplexed real-time type-specific polymerase chain reaction (PCR) assays were used. These assays detected, differentiated, and quantified 28 different HPV genotypes, including 13 high-risks HPV types (HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68), 9 low-risks HPV types (HPV6, 11, 40, 42, 43, 44, 54, 61, 70), and 6 probable high-risks HPV types (HPV26, 53, 66, 69, 73, 82). Specimens from primary health facility participants were tested using the Anyplex^TM^ II HPV28 assay. While specimens from Nelson Mandela Academic Hospital-referred participants were tested using the Allplex^TM^ HPV28 assay. The current study did not compare the performance of the two assays; however, good agreement has been reported elsewhere [27,28]. The PCR assays were performed on a Bio-Rad CFX96 real-time thermocycler (Bio-Rad, Hercules, CA, USA) in accordance with the manufacturer’s instructions. The Allplex^TM^ and Anyplex^TM^ II HPV28 assays specifically targets the L1 one major capsid gene of the HPV types. Additionally, the human housekeeping (β-globin) was used as an internal control, being simultaneously with the L1 gene. Data analysis was automated and interpreted using the Seegene Viewer Software v3.31.000.006 (Seegene Inc., Seoul, Republic of Korea). The Allplex^TM^ and Anyplex^TM^ II HPV28 assays employed Seegene’s proprietary dual priming oligonucleotide and tagging oligonucleotide cleavage and extension technology in a multiplexed real-time PCR format to detect and semi-quantify HPV DNA. Viral load was categorized as high (+++; positive signal before 31 PCR cycles), medium (++; positive signal between 31 and 39 PCR cycles), or low (+; positive signal after 40 PCR cycles), with an endogenous internal control included. These viral load data are reported for completeness but were not analyzed in this study. If a sample yields a negative internal control and a negative HPV result was re-analyzed. If the re-analysis remains negative, the sample was deemed invalid. Conversely, if the internal control was negative but the HPV result was positive, the test result was considered valid. Negative HPV tests with a positive internal control were deemed negative for the 28 HPV types tested. To monitor for contamination, a negative control was included for every 20 samples and subjected to the same extraction and HPV genotyping processes.
2.4. Statistical Analysis
All variables from the questionnaires and laboratory investigation were captured and coded in Microsoft Excel 2016 (Microsoft Corporation, Seattle, WA, USA). GraphPad Prism v8.0.1.244 statistical software was used to perform all statistical analyses. Non-normally distributed data were summarized using the median and interquartile range (IQR). Categorical variables were presented using frequency tables, percentages, and graphs. The two-sample test of proportions was used to compare demographic characteristics between groups or categories. The association of two categorical variables was assessed using the Chi-squared test and Fisher’s exact test, depending on the expected frequencies. If 20% or more of the cells have expected frequencies of <5 or any one cell has an expected frequency of 0, Fisher’s exact test was used; otherwise, the Chi-squared test was used. The 95% Confidence Interval (CI) was used to estimate the precision of the estimate. The level of significance was set at 5% (p-value ≤ 0.05) for statistical significance. Risk ratios were calculated using contingency table analysis. Single HPV infection was defined as infection with one HPV type, and multiple infection was defined as infection with two or more HPV types.
2.5. Ethics Considerations
The study was conducted in accordance with ethical approvals granted by the Walter Sisulu University Health Research Ethics Committee (HREC: 004/2022; 037/2023; 258/2024) and the Eastern Cape Department of Health (EC_202203_011; EC_202309; EC_202502_012). Written informed consent was obtained from all participants prior to data collection, and participation was voluntary.
3. Results
3.1. Study Population Description
A total of 540 participants were included in the study, 269 had normal cytology, 16 had ASC-US, 31 had LSIL, 21 had ASC-H, 150 had HSIL and 53 had cervical cancer. The median age of overall study participants was 41 years, with an interquartile range (IQR) of 32–50 years. Among women with normal cervical cytology, most participants were aged 30–39 years (31.3%, 84/268) and were single (73.0%, 195/267). A large proportion reported no smoking (78.7%, 210/267), initiated sexual activity at 17–18 years (39.3%, 105/267), and a majority were HIV-positive (63.7%, 170/267). Among HSIL cases, the 40–49-year age group was most common (36.7%, 55/150), and about half of the participants were single (54.7%, 81/147). Most had initiated sexual activity at ≤16 years (37.7%, 55/146), and a substantial proportion were HIV-positive (72.1%, 106/147). Among women with cervical cancer, most were aged 50–98 years (60.4%, 32/53), and half were single (50.0%, 26/52). Additionally, 80.8% (42/52) reported no smoking, 67.3% (35/52) were HIV-positive, and 44.2% (23/52) had 3–4 lifetime sexual partners (Table 1).
Among both HIV-negative and HIV-positive women, the median age increased significantly as the cytology grades worsened (p for trend < 0.0001, p for trend < 0.001, respectively). HIV-negative women with negative intraepithelial lesions or malignancy (NILM) (median: 31 years) were younger than those with cervical cancer (median: 63 years, p < 0.0001). A similar age trend was observed among the HIV-positive women (p < 0.0001). HIV-negative women were younger in the NILM group than HIV-positive women (p = 0.003), while HIV-negative women were older in the cervical cancer group than HIV-positive women (p = 0.007, Figure 1).
3.2. Prevalence of HPV Infection According to Cervical Cytology and HIV Status Among Eastern Cape Women
Among women with NILM cytology, the prevalence of HPV infection was 60.6% (163/269), with multiple infections (30.9%, 83/269) being slightly more common than single infections (29.7%, 80/269). HR-HPV types (47.2%, 127/269) were also more common than LR-HPV types (27.9%, 75/269, Table 2). In contrast, women with HSIL had higher rates, with 93.7% (145/150) positive for any HPV type, 80.7% (121/150) having multiple HPV infections and 95.3% (143/150) positive for HR-HPV types. Among cervical cancer cases, these rates remained high, with 92.5% (49/53) positive for HPV infection, 64.2% (34/53) having multiple infections and 90.6% (48/53) positive for HR-HPV (Table 2). The overall HPV prevalence in different cervical cytology groups was not significantly influenced by HIV coinfection except in HSIL group (99.1%, 105/106 compared to 90.2%, 37/41; RR: 1.10, 0.99–1.22, p = 0.022).
Among women with NILM cytology, infection with one HPV type (29.7%, 80/269) was more common than infection with five to fifteen HPV types (7.1%, 19/269). In HSIL cases, infection with two HPV types (28.0%, 42/150) and with five to fifteen HPV types (27.3%, 41/150) were more prevalent than infection with one HPV type (16.0%, 24/150). Among cervical cancer cases, infection with one or two HPV types (28.3%, 15/52 and 32.1%, 17/53, respectively) was more common than infection with five to fifteen HPV types (13.2%, 7/53). In HIV-negative women, infection with one HPV type (27.2%, 47/173) was more common than infection with five to fifteen HPV types (12.7%, 22/173). Similarly, in HIV-positive women, infection with one HPV type (22.7%, 82/361) was more prevalent than infection with five to fifteen HPV types (18.0%, 65/361, Figure 2).
3.3. Distribution of HPV Genotypes Among Women with Different Cervical Cytology Grades in Single and Multiple Infections According to HIV Status
Among women with NILM cytology, the five most prevalent HPV types overall were HPV58 (10.4%), HPV35 (8.9%), HPV68 (7.8%), HPV39 (5.9%), and HPV16 and 53 (5.6%). For most types, multiple infections occurred more frequently than single infections (Figure 3A). When stratified by HIV status, HPV35 (9.3%), HPV45 (8.2%), and HPV39, 58, and 68 (7.2%) were the most common HPV types among HIV-negative, with multiple infections again exceeding single infections (Figure 3B). In contrast, HIV-positive women showed higher prevalence of HPV58 (12.4%), HPV35 (8.8%), and HPV68 (8.2%), and similarly demonstrate a predominance of multiple over single HPV infections (Figure 3C). Among women with ASC-US cytology, HPV68 was the most dominant type, and multiple infections were more common than single infections. In LSIL, HPV16 predominated, with the same pattern of multiple infections being more frequent. ASC-H cases were also dominated by HPV16, with multiple infections more common overall; however, HPV16 was the most frequent single-type infection specifically among HIV-negative women. In HSIL, HPV16 (40.7%), HPV33 (26.7%), HPV35 (26.0%), HPV58 (25.3%), and HPV52 (23.3%) were the most prevalent HPV types, and all were detected more frequently in multiple infections than as single types (Figure 4A). Among HIV-negative HSIL cases, HPV16 (41.5%), HPV33 (31.7%), and HPV35 (26.8%) were the dominant types, with multiple infections again more common (Figure 4B). Among HIV-positive HSIL cases, HPV16 (39.6%), HPV58 (31.1%), and HPV52 (24.5%) were most prevalent, reflecting the same pattern of higher multiple-infection burden in HIV-positive women (Figure 4C).
In contrast, among cervical cancer cases, the most prevalent HPV types overall were HPV16 (41.5%), HPV18 (30.2%), HPV35 (22.6%), HPV54 (17.0%), and HPV66 (11.3%). Multiple infections remained more common than single-type infections across all HPV types (Figure 5A). Among HIV-negative women with cervical cancer, the most dominant HPV types were HPV18 (35.3%), HPV16 (29.4%), and HPV35, 51, 52, and 70 (11.8%). Although multiple infections were still more frequent than single infections, HPV18 appeared more commonly as a single-type infection (Figure 5B). Among HIV-positive women, HPV16 (45.7%) was the most prevalent type, followed by HPV18 and 35 (28.6%), and HPV54 (22.9%). Consistent with patterns observed in other cytology grades, multiple infections remained more common than single infections (Figure 5C).
3.4. Prevalence of HPV Types Targeted by Current Commercial HPV Vaccines According to Different Cervical Cytology Grades
HPV types targeted by Cervarix^®^ HPV vaccine were detected in 12.0% (31/269) of NILM cases, 31.0% (5/16) of ASC-US, 45.0% (14/31) of LSIL, 52.0% (11/21) of ASC-H, 49.0% (73/150) of HSIL, and 64.0% (34/53) of cervical cancer cases. HPV types targeted by Gardasil-4^®^ HPV vaccine were detected in 14.0% (39/269) of NILM, 38.0% (6/16) of ASC-US, 45.0% (14/31) of LSIL, 62.0% (13/21) of ASC-H, 53.0% (79/150) of HSIL, and 68.0% (36/53) of cervical cancer cases. HPV types targeted by Gardasil-9^®^ HPV vaccine were detected in 36.0% (97/269) of NILM, 75.0% (12/16) of ASC-US, 84.0% (26/31) of LSIL, 76.0% (16/21) of ASC-H, 83.0% (125/150) of HSIL, and 81.0% (43/53) of cervical cancer cases. When HPV35 was added to the Gardasil-9^®^ HPV vaccine, prevalence increased to 39.0% (106/269) for NILM, 88.0% (14/16) for ASC-US, 84.0% (26/31) for LSIL, 90.0% (19/21) for ASC-H, 92.0% (138/150) for HSIL, and 87.0% (46/53) for cervical cancer. Notably, no additional increase was observed in LSIL, where the proportion remained unchanged following the inclusion of HPV35 (Figure 6). HPV35 was included due to its disproportionately high prevalence among African women, despite not being covered by existing vaccines. Incorporating HPV35 may therefore help close an important protection gap for populations with a higher HPV35-associated cervical cancer burden.
3.5. Factors Associated with HPV Infection Among Women with Normal Cervical Cytology in the Eastern Cape Province
Among women with normal cervical cytology, age was strongly associated with HPV infection. Participants aged 18–29 years had the highest prevalence, which declined significantly among those aged 40–49 years and 50–60 years (RR: 0.59, 95% CI: 0.40–0.81, p = 0.001; RR: 0.61, 95% CI: 0.45–0.80, p < 0.001, respectively). Current or past alcohol consumption was associated with a higher prevalence of HPV infection compared with non-drinkers (RR: 1.43, p = 0.029 and RR: 1.44, p = 0.021, respectively). Past smokers were also at significantly higher risk than non-smokers (RR: 1.43, 95% CI: 1.09–1.71, p = 0.020). HPV prevalence was higher among single women compared with those who were married or cohabiting (RR: 0.68, 95% CI:0.49–0.89, p = 0.004) and those who were separated or widowed (RR:0.34, 95% CI: 0.12–0.75, p = 0.002). Having one sexual partner in the past year compared to no partner was associated with increased HPV prevalence (RR: 1.39, 95% CI: 1.04–1.98, p = 0.031, Table 3).
Women with five or more children had significantly lower HPV infection risk (RR: 0.45, 95% CI: 0.29–0.70, p = 0.002). Use of condoms as their primary contraceptive method was associated with higher HPV prevalence compared to no contraceptive use (RR: 1.43, 95% CI: 1.05–1.87, p = 0.028). Participants reporting vaginal discharge also had a significantly higher prevalence of HPV infection (RR: 1.40, 95% CI: 1.15–1.72, p = 0.0001). Early sexual debut, HIV status, level of education, and other investigated factors were not significantly associated with HPV infection (p > 0.05). Among women with HSIL and cervical cancer, none of the assessed behavioral or demographic factors were significantly associated with HPV infection except for HIV status. HIV-positive women had an increased risk of HPV infection compared to HIV-negative women (RR: 1.09, CI: 1.02–1.24, p = 0.019, Table 3).
4. Discussion
This study examined the distribution of HPV genotypes and associated risk factors among women in the Eastern Cape Province across varying cervical cytology grades, with additional stratification by HIV status. Women with high-grade lesions or cervical cancer tended to be older, whereas those with normal cytology were generally younger. The progressive increase in median age with worsening cytological abnormalities suggest that cervical cancer development is more strongly linked to chronic, persistent HPV infection rather than recent exposure [29]. The age differences observed between HIV-negative and HIV-positive women further indicate that HIV-related immune impairment may reduce HPV clearance, thereby increasing viral persistence [25,30]. HPV prevalence was high across all cervical cytology grades, consistent with findings from other studies reporting elevated HPV infection rates; particularly in women with HSIL and cervical cancer [10,31,32]. However, a study from KwaZulu-Natal, South Africa, reported lower HPV prevalence across these grades [33]. Collectively, these findings reinforced the central role of HPV in cervical carcinogenesis.
Multiple infections were more common among women with severe lesions and cervical cancer, aligning with earlier studies demonstrating that multiple infections are associated with higher viral loads and increased risk of progression [34,35,36]. This pattern underscores the complexity of HPV epidemiology in this high-risk population. Similarly to reports from other African settings, high-risk HPV types predominated across the cytological spectrum [36,37], while low-risk types were frequently detected in combination with high-risk types, particularly among HIV-positive women. This co-occurrence has been documented in other African cohorts, where high-risk and low-risk types commonly coexist within the same infections [38].
Genotype-specific analyses showed that women with normal cytology were most frequently infected with HPV58, 35, 68, 39, and 53, whereas women with HSIL were more likely to have HPV16, 33, 35, 58, and 52. These patterns align with previous studies that similarly reported HPV58 as one of the dominant types in women with normal cervical cytology [39,40] and HPV16 as the predominant type among women with HSIL [32,36,37]. In cervical cancer cases, HPV16 and HPV18 remained the most prevalent types, consistent with global evidence identifying these two genotypes as the primary oncogenic drivers of cervical cancer [41,42]. Notably, HPV35 was also common in cervical cancer, ranking immediately after HPV16 and HPV18, underscoring its epidemiological importance in Africa. The recurrent detection of HPV35 across all cytology categories underscores the need to consider expanding vaccine coverage to include this type, which is not protected by current Gardasil-9^®^ vaccine [15].
HIV-positive women showed a wide variety of HPV types and multiple infections, confirming that immune suppression facilitates persistent infections and viral spread [43], and emphasizing the importance of integrated HPV and HIV management in affected populations [43]. Interestingly, HPV54, a low-risk type, appeared in some cervical cancers among HIV-positive women, suggesting that certain low-risk types may behave differently in the context of HIV co-infection. Cervarix^®^ and Gardasil-4^®^ prevented only 12.0–14.0% of infections in women with normal cervical cytology but prevented 60.0% of infections in cervical cancer cases, indicating vaccine-targeted high-risk types primarily drive severe disease. Approximately 80.0% of infections in women with HSIL and cervical cancer were preventable through Gardasil-9^®^’s broader coverage. Protection increased further when HPV35 was included in the vaccine. This highlights the significance of HPV35 in Africa and demonstrates why its inclusion in future vaccines would be beneficial [15].
Behavioral factors associated with HPV infection in women with normal cervical cytology included being younger, single, a former smoker, an alcohol consumer, and reporting vaginal discharge. These findings are consistent with other African studies that have linked such factors to increased HPV risk [44,45]. The association between HPV and vaginal discharge may reflect recently acquired HPV infection occurring alongside other genital infections that cause inflammation and mucosal disruption, thereby facilitating HPV transmission [46,47]. In contrast to studies reporting high parity as a risk for HPV infection [48,49], women with more children in this study had a lower prevalence of HPV infection. This may be explained by the tendency for higher-parity women to be older, as HPV acquisition generally decreases with age. Condom users were more likely to contract HPV, likely due to inconsistent [50] and higher rates of other risk factors, such as earlier sexual debut and multiple partners. The observed association between reporting one sexual partner in the past year and increased HPV prevalence is likely due to cumulative lifetime exposure and viral persistence rather than recent acquisition. HPV prevalence is strongly influenced by prior sexual history, and persistent HPV DNA may still be detected even when recent new partners are excluded in cross-sectional studies [51]. HIV infection was a significant risk factor among women with HSIL and cervical cancer [26], but it was not linked to HPV infection in women with normal cervical cytology.
The study’s HPV genotyping, distinguishing single and multiple infections, provides detailed insight into HPV genotype distribution, including high-risk and probable high-risk types, beyond the most prevalent strains. Stratification by cervical cytology and HIV status enabled assessment of the impact of immune status on HPV diversity and disease severity, which is particularly relevant in high HIV prevalence settings such as the Eastern Cape. The relatively large sample size supports robust statistical analyses and enhances the representativeness of the findings. However, the cross-sectional design limits causal links regarding HPV persistence or progression. The small sample size of cervical cancer, ASC-US, LSIL and ASC-H cases restricted subgroup analyses and limits generalizability. Although HPV genotype coverage relative to vaccine types was evaluated, actual vaccination uptake, history, and effectiveness in the cohort, particularly since public vaccination began in 2014 targeting girls now aged 19–22 years, were not assessed, which may influence genotype prevalence. Participants’ prior treatment history for cervical lesions or cervical cancer was not collected, which could potentially influence HPV prevalence estimates, and cervical lesion diagnoses were derived from routine clinical reports and were not independently morphologically verified, which may introduce diagnostic variability. Additionally, analyses of self-reported behavioral variables, such as condom use and sexual history, may be subject to recall or social desirability bias, potentially affecting accuracy.
5. Conclusions
This study highlights the high overall HPV prevalence, which further increased among women with abnormal cervical cytology in the Eastern Cape Province, South Africa. While overall HPV prevalence was not strongly influenced by HIV co-infection, distinct differences were observed in the HPV genotype patterns when stratified by HIV status. A significant proportion of HSIL and cervical cancer cases were attributed to types covered by the Gardasil-9^®^, but the dominance of non-vaccine types, especially HPV35, underscores a critical gap in current prevention strategies relevant to this specific population. The substantial increase in potential vaccine coverage achieved by including HPV35 highlights the necessity of regionally tailored vaccine formulations or expanded coverage to effectively reduce the burden of cervical cancer in the Eastern Cape. Data generated from this study further encourages the use of the Gardasil-9^®^ HPV vaccine in the South African national screening programme. In evaluating regional HPV epidemiology, integrated strategies that combine HPV vaccination, HIV care, and targeted cervical cancer screening should be prioritized in regional prevention programs. Public health education should also address behavioral risk factors to reduce the acquisition of HPV. Larger-scale, longitudinal studies are essential for monitoring the effects of HPV vaccination, assessing HPV persistence, and informing regional vaccine policy and cervical cancer prevention initiatives.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maswanganye C.K. Mkhize P.P. Matume N.D. Mapping the HPV Landscape in South African Women: A Systematic Review and Meta-Analysis of Viral Genotypes, Microbiota, and Immune Signals Viruses 202416189310.3390/v 1612189339772200 PMC 11680443 · doi ↗ · pubmed ↗
- 2Bolon J. Samson A. Irwin N. Murray L. Mbodi L. Stacey S. Aikman N. Moonsamy L. Zamparini J. An audit of adherence to cervical cancer screening guidelines in a tertiary-level HIV clinic South. Afr. J. HIV Med.202324149010.4102/sajhivmed.v 24i 1.149037293604 PMC 10244942 · doi ↗ · pubmed ↗
- 3Somdyala N.I.M. Bradshaw D. Dhansay M. Stefan D.C. Increasing Cervical Cancer Incidence in Rural Eastern Cape Province of South Africa from 1998 to 2012: A Population-Based Cancer Registry Study JCO Glob. Oncol.20206810.1200/JGO.19.00198 PMC 700022832031436 · doi ↗ · pubmed ↗
- 4Moosa-Battey R.M. Masuku P. Mayimele N. Human papillomavirus (HPV) as the main cause of cervical cancer and other related cancers: A review SA Pharm. J.202592586210.36303/SAPJ.1164 · doi ↗
- 5Tesfaye E. Kumbi B. Mandefro B. Prevalence of human papillomavirus infection and associated factors among women attending cervical cancer screening in setting of Addis Ababa, Ethiopia Sci. Rep.202414405310.1038/s 41598-024-54754-x 38374354 PMC 10876560 · doi ↗ · pubmed ↗
- 6Fitzpatric M.B. Hahn Z. Mandishora R.S.D. Dao J. Weber J. Haung C. Whole-genome analysis of cervical human papillomavirus type 35 from Zimbabwean women Sci. Rep.202010700110.1038/s 41598-020-63882-z 32332798 PMC 7181610 · doi ↗ · pubmed ↗
- 7Okunade K.S. Human papillomavirus and cervical cancer J. Obs. Gynaecol.20204060260810.1080/01443615.2019.163403031500479 PMC 7062568 · doi ↗ · pubmed ↗
- 8Skelin J. Tomaic V. Comparative Analysis of Alpha and Beta HPV E 6 Oncoproteins: Insights into Functional Distinctions and Divergent Mechanisms of Pathogenesis Viruses 202315225310.3390/v 1511225338005929 PMC 10674601 · doi ↗ · pubmed ↗