The Relationship Between Emotion Processing and Flexor Afferent Responses in Upper Limbs
Gianluca Isoardo, Rita B. Ardito, Stefano Ciullo, Elena Fontana, Ilaria Stura, Giuseppe Migliaretti, Paolo Titolo, Enrico Matteoni, Andrea Calvo, Valeria Fonzo, Federica Laino, Mauro Adenzato

TL;DR
This study shows that emotions affect reflex responses in people with chronic upper limb pain, linking emotional and motor processes.
Contribution
The paper reveals how emotional processing modulates spinal reflexes in chronic neuropathic pain patients.
Findings
Patients with chronic pain showed longer and stronger reflex responses compared to healthy controls.
Reflex durations correlated with anxiety, depression, and poor emotion recognition.
Tactile and pain perception thresholds mediated the relationship between emotions and reflexes.
Abstract
Background: This study investigates the influence of emotional processing on flexor reflex responses in the upper limbs, focusing on cutaneomuscular reflexes (CMRs) and the cutaneous silent period (CSP) in patients with chronic neuropathic pain. The modulation of motor reflexes by emotions remains unclear. Methods: Fifty-one patients with chronic upper limb neuropathic pain (carpal tunnel syndrome, other neuropathies, post-burn hypertrophic scars) and twenty healthy controls underwent standardized electrodiagnostic signal acquisition. Neurophysiological assessments (CMRs, CSP, standard nerve conduction tests) and psychological evaluations (anxiety, depression, emotion processing) were conducted. Neurophysiological signal acquisition included median and ulnar nerve conduction studies recorded with an electrodiagnostic system (48 kHz sampling rate; 30–3000 Hz bandpass). CSP and CMRs were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
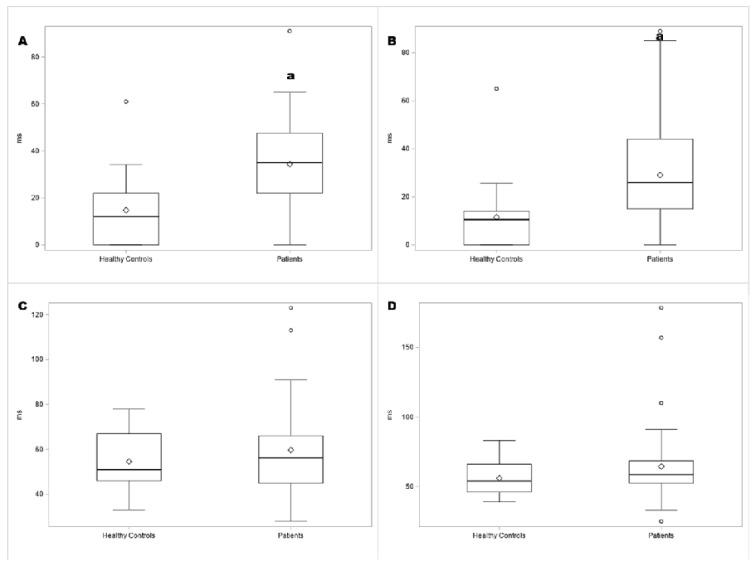 Figure 1
Figure 1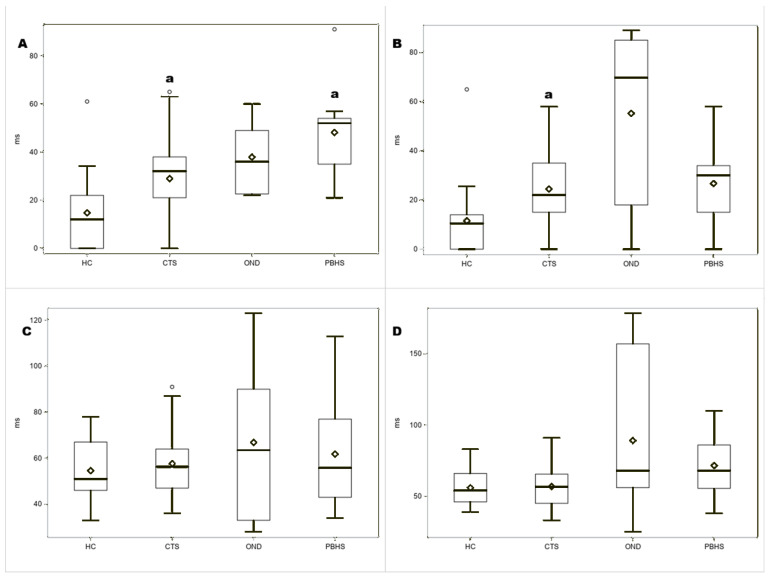 Figure 2
Figure 2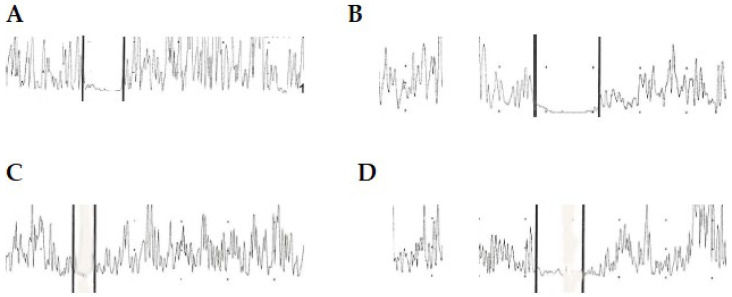 Figure 3
Figure 3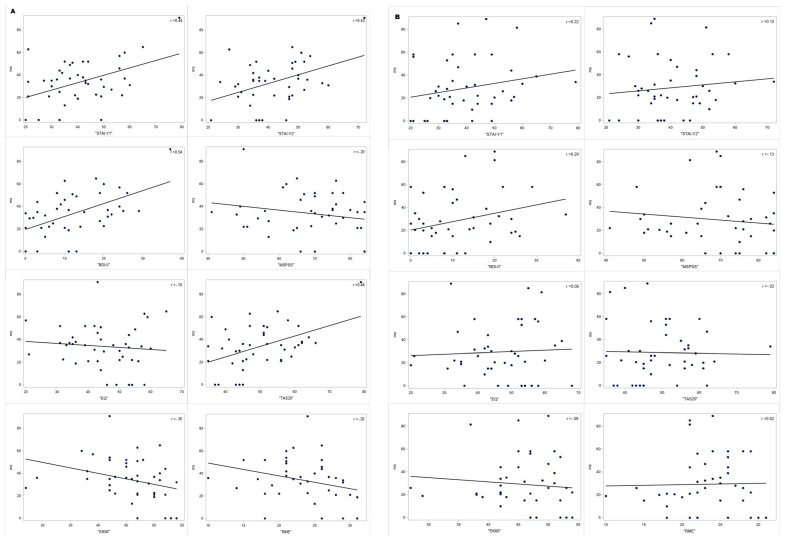 Figure 4
Figure 4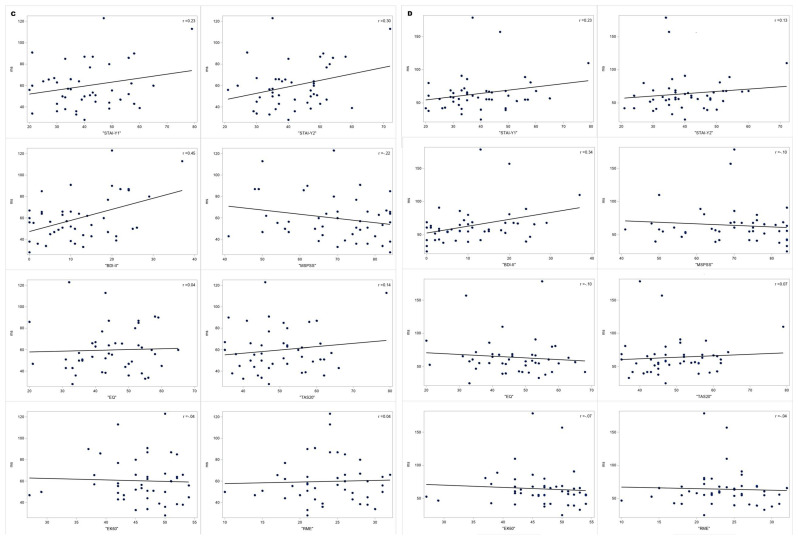 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPain Mechanisms and Treatments · Pain Management and Treatment · Musculoskeletal pain and rehabilitation
1. Introduction
Sherrington, in his 1910 pivotal work on the flexion reflex of the limb, defined the protective nature of the flexion reflex and its stereotypical pattern of muscle activation in response to a stimulus applied to a receptive field. Notably, he described a combination of vocalization, retracting the lips, opening the mouth, and turning of the head sideways and backward, together with flexion of the limb in the decerebrate cat, and coined the term “pseudoaffective reflex” to define a combination of reflex movements in preparation for defence [1]. Sherrington’s view that reflexes are stereotyped and fixed motor responses to a stimulus applied to a receptive field has changed, and reflexes are now regarded as flexible responses integrated by centrally generated motor commands to produce movements suitable for an ever-changing environment [2].
Within the group of reflex responses mediated by the so-called flexor reflex afferents, withdrawal reflexes are considered nociceptive responses [3,4], while cutaneomuscular reflexes (CMRs) are regarded as responses elicited by non-nociceptive stimuli and involved in fine motor control [3,4,5,6]. Although withdrawal reflexes are considered spinal circuitry-mediated and stereotyped responses [3], their amplitude can be modulated by emotional stimuli depending on the positive or negative valence of these stimuli [7,8,9]; for instance, amplitude of the withdrawal reflex recorded from the biceps femoris can be increased after phobic stimulation [7]. In the upper limb, the withdrawal response to noxious stimuli differs in the arm, forearm, and intrinsic hand muscles: in the hand muscles, a suppression of ongoing electromyographic activity, known as the cutaneous silent period (CSP), is prominent, whereas in the arm and forearm, there is a contraction of relaxed muscles [10]. Consistent with previous reports correlating withdrawal reflexes and emotions, CSP has been found to be related to anxiety scores on the Hospital Anxiety and Depression Scale [11]. Observation of another individual’s painful stimulation of the dorsum of the hand negatively modulates motor-evoked potentials recorded from the first dorsal interosseus in the observer [12]. This provides a clue to the link between unconscious modulation of motor output and conscious feelings.
CMRs coexist with CSP during high-intensity electrical stimulation of the fingers, and both CMRs and CSP are topographically organized. In thenar muscles, CMR may include a late inhibitory component (I2), sometimes preceded by an excitatory component (E2) [3,4,6,13,14]. Both E2 and probably I2 are mediated by a transcortical circuitry [13,14]. The amplitude of the E2 component superimposed on CSP is modulated by the proximity of the stimulated hand to the face, that is, the peripersonal space [14]. The increase in E2 with the hand near the face parallels that of the somatosensory blink reflex, which is modulated by empathy, anxiety, and the organization of the mental representation of attachment in childhood [15]. Thus, it is conceivable that flexor reflex afferent responses, including both withdrawal responses and CMRs, may be modulated by higher-order cognitive and emotional processes to better shape behaviour in response to the environment. In the present study, we correlated the metrics of intrapersonal and interpersonal emotion regulation, mood, and anxiety with both CMRs and CSP recorded from the abductor pollicis brevis in patients with neuropathic pain in the upper limb and healthy controls. To better define the mediators of possible correlations between CMR/CSP and psychological findings, we also took into account the psychophysical evaluation of Aβ and Aδ sensory fibres involved in CMR and CSP generation [3,4,5,6,12].
2. Materials and Methods
2.1. Patients
The study was approved by the Ethics Committee of the Città della Salute e della Scienza di Torino Hospital. Patients and controls provided informed consent to participate in the study. We enrolled patients with chronic (lasting more than 3 months) peripheral neuropathic pain [16,17,18] involving at least one hand. The patients cohort included individuals with carpal tunnel syndrome (CTS), brachial plexopathy, painful cervical radiculopathy, ulnar neuropathy at the elbow, or post-burn hypertrophic scars (PBHSs), and the diagnosis of each disease was made as previously described [19,20,21]. All patients underwent a full clinical evaluation as described [6,19,20,21], including pinprick, touch, and position sense assessments of both upper limbs. In addition to evaluating pinprick and touch sense, the pain sites were also assessed for signs of allodynia in response to brushing, as part of the DN4 questionnaire [22]. Self-reported mean pain intensity in the week before examination was graded on an 11-point numerical rating scale (NRS), with scores ranging from 0 (no pain) to 10 (worst possible pain) [23].
2.2. Neurophysiological and Psychophysiological Evaluation
Sensory and motor nerve conduction studies of the median and ulnar nerves were performed as described [6,19,20,21], using a commercially available electrodiagnostic equipment (Viking Quest, Carefusion, Middleton, WI, USA). The sampling rate was 48 kHz, with a bandpass of 30 to 3000 Hz. CSP and CMRs of the abductor pollicis brevis (APB) were recorded with surface electrodes in a bipolar belly–tendon montage. To elicit both CSP and CMRs in patients and controls, electric shocks were delivered to the index finger while subjects performed an isometric contraction at maximum force against a resistance [6,19]. To maintain constant contraction strength, audio feedback was provided to patients and controls. CSP and CMRs obtained during maximal contraction tend to be shorter in duration [5]; nonetheless, we performed CSP and CMR evaluation during maximal strength contraction to avoid eliciting the late excitatory component of CMRs in APB [5]. Stimulation was delivered through ring electrodes (Carefusion, Middleton, WI, USA), with the cathode placed at the index proximal interphalangeal joint. CSP was obtained after stimulation at an intensity eight times the perceptual threshold for an electric shock, while CMR was obtained at an intensity twice the perceptual threshold [6]. This threshold was determined separately for each hand by slowly increasing the intensity of stimulation delivered at 1 Hz until the patients perceived a sensation of a non-painful electric shock. To evaluate CSP, off-line rectified electromyographic activity was averaged over eight trials for each hand. To evaluate CMR, electromyographic activity was off-line rectified, and each of the ten traces that showed suppression of activity lasting more than 10 ms was included for analysis. To avoid habituation, each trial was performed at least 60 s after the previous trial. Onset and offset of CSP and CMRs were defined by the same author (G.I.) by visual inspection as the beginning of an abrupt decrease and recovery of electromyographic activity, as previously described [6,19]. This method of detection has been used in previous studies [6,19]. Before performing these studies, two experienced neurophysiologists separately evaluated the onset and offset of CSP and CMRs in patients and controls, with fair agreement between evaluations (k: 0.8, unpublished data).
All patients and controls underwent quantitative sensory testing (QST) evaluation of cold detection threshold (CDT) and heat pain detection threshold (HDT) at the dorsum of the hand and the palmar surface of the index and little fingers, and of vibration detection threshold (VDT) at the index and little fingers. Details on the QST procedure are provided elsewhere [6,19,20,21].
Psychological, Health Quality, and Social Support Evaluation
The following psychological evaluations were performed in all patients and controls: Toronto Alexithymia Scale (TAS-20) [24,25] for alexithymia, Beck Depression Inventory-II (BDI-II) [26] for depression, the Y form of the State-Trait Anxiety Inventory (STAI-Y) for anxiety symptoms [27], the Reading the Mind in the Eyes task (RME) [28] for affective theory of mind, the Ekman 60 Faces Test (EK-60) [29] for facial emotion recognition, and the Empathy Quotient [30] for empathy.
The 12-item General Health Questionnaire (GHQ-12) [31] was used to assess levels of psychological distress, and the Multidimensional Scale of Perceived Social Support (MSPSS) [32] was used to assess social support.
2.3. Statistical Analysis
The results are presented as mean ± standard deviation (SD) for continuous variables, and as absolute and relative frequencies for categorical variables. The normality of the distribution of continuous parameters was assessed using the Kolmogorov–Smirnov test. QST parameters that were not normally distributed were log-transformed for analysis with parametric inferential methods [20]. The z-scores of the patients at each site were calculated as follows:
Comparisons were performed using the t-test and ANOVA for normally distributed variables, or the Wilcoxon and Kruskal–Wallis tests for non-normally distributed variables.
Correlations were analyzed by estimating the parametric Pearson correlation coefficient (r). General Linear Models (GLMs) were used to test the dependence of CMRs and CSP on psychological evaluations, QST, and other parameters. Group, educational age, and achievements were considered as possible confounding factors; if significant, analyses are presented divided by these variables. Multiple comparison adjustments were made where necessary.
In all analyses, p-values < 0.05 were considered statistically significant. Statistical analysis was carried out using SAS^®^ Statistics Software v. 9.4.
3. Results
3.1. Demographic, Neurophysiological, and Psychophysical Findings
We enrolled 51 patients and 20 healthy controls. Data from all patients and controls were included in previously published studies [6,20,21]. In the patient group, 34 had CTS, 10 had PBHS, and 7 had other peripheral neurological diseases (ONDs) causing upper limb pain. Demographic data are shown in Table 1.
As previously reported [20,21], there was no difference in sex or age distribution between patients and controls, but patients had fewer years of education than controls. Findings from nerve conduction studies and QST evaluations are shown in Table A1 and Table A2 (Appendix A). CSP and CMR findings are shown in Table 2. Box plots showing the duration of CMRs and CSP in patients and healthy controls, as well as among CTS, OND, and PBHS, are provided in Figure 1 and Figure 2. Examples of CMRs and CSP in patients and healthy controls are shown in Figure 3.
Median nerve sensory conduction velocity and median and ulnar amplitudes of sensory action potentials were lower in patients than in controls. A significant difference between patients and controls was evident for ln-transformed VDT at all evaluated sites and for log-transformed CDT at all sites, except the right dorsum and right little finger. No significant differences were observed in sensory and motor nerve conduction or QST findings, among CTS, PBHSs, and ONDs.
Bilaterally, CMR duration and the intensity of electric shock required to elicit CMRs and CSP were significantly higher in patients than in healthy controls, as shown in Figures. No significant differences in CSP and CMR parameters were found among CTS, PBHSs, and ONDs. CMR duration was higher than in healthy controls and on the right hand in PBHSs, as shown in Figure 2A,B.
3.2. Psychological Findings
Results of psychological evaluations are summarized in Table 3. Patients had higher BDI-II, TAS-20 overall score, TAS-20 F1 score, TAS-20 F3 score, and lower overall EK-60 and EK-60 subscore for fear than healthy controls. No differences were observed in psychological metrics among CTS, ONDs, and PBHSs, as previously described [20,21].
3.3. Correlation Between CSP, CMR, and Psychological Findings
Duration of right CMR correlated with STAI-Y1 (r = 0.44, p = 0.001), STAI-Y2 (r = 0.43, p = 0.03), TAS-20 overall (r = 0.46, p = 0.001), TAS-20 F1 subscore (r = 0.53, p < 0.0001), EK-60 overall score (r = −0.30, p = 0.005), and EK-60 subscore for sadness (r = −0.41, p = 0.01). Bilaterally, duration of CMR correlated with BDI-II (right r = 0.54, p < 0.0001; left r = 0.29, p = 0.01), and EK-60 subscore for sadness (right r = −0.38, p = 0.002; left r = −0.3, p = 0.01).
Duration of CSP correlated bilaterally with BDI-II (right r = 0.34, p = 0.002; left r = 0.45, p = 0.008), and on the right side with TAS-20 F1 score (right r = 0.31, p = 0.01). Scatterplots showing the relationship between psychological findings and the duration of CMA and CSP are shown in the Figure A1.
3.4. General Linear Model (GLM)
When GLM analysis was performed to investigate the interaction among psychological findings and CMR and CSP parameters, the relationship between left CMR and CSP duration and BDI-II was mediated by STAI-Y1 (CMR: b = 0.6, standard error = 0.02, p = 0.02; CSP: b = 0.06, standard error = 0.02, p = 0.02) and STAI-Y2 (CMR: b = −0.09, standard error = 0.03, p = 0.01; CSP: b = −0.09, standard error = 0.03, p = 0.01). Right-hand CSP duration was also related to years of education (b = 1.5, standard error = 0.52, p = 0.005).
When GLM analysis of the relationship between CMR and CSP parameters with psychological findings was performed including QST results, the correlation between the duration of left CMR and BDI-II was entirely mediated by VDT z-score at the index finger (b = −0.6, standard error = 0.18, p = 0.0007) and little finger (b = 0.99, standard error = 0.38, p = 0.01). In contrast, the relationship between right CMR duration and STAI-Y2 was mediated by HPT z-score at the index finger (b = 0.1, standard error = 0.05, p = 0.02). Right-hand CSP duration is affected by the interaction between BDI-II and years of education (b = 1.7, standard error = 0.47, p < 0.001). The GLM did not identify other factors influencing the relationship between psychological findings and CMR/CSP parameters.
4. Discussion
The results reported here demonstrated a relationship between the duration of CMR and CSP and metrics of state and trait anxiety, depression, emotion recognition (EK-60), and emotion regulation (TAS-20). GLM showed that the relationship between left CMR and depression depends on VDT z-scores at the index and little fingers, and that the relationship between right CMR and trait anxiety is mediated by the HPT z-score at the index finger. Years of education only affected the relationship between right CSP and BDI-II.
The relationship between left CMR duration and depression is mediated by vibratory perception in the left index and little fingers. These results are consistent with our previous findings on the relationship between vibration perception in the left index finger and alexithymia, which in turn is a risk factor for the development of major depression [33]. In fact, CMR is mediated by Aß sensory fibres [3,4,5,6,13]; therefore, the relationship between left CMR duration and depression appears to be related to the function of Aß afferents from the left-hand fingers. The relationship between right CMR duration and trait anxiety is also consistent with the relationship between right-hand HPT z-scores and state anxiety observed in our previous study [20]. In contrast, GLM did not show any influence of QST findings on the relationship between right CMR duration and EK-60 total score, nor any influence of years of education on the relationship between CMR duration and psychological features. It is noteworthy that in our previous study [21], only the EK-60 score for surprise correlated with vibration perception at the left index, while neither the overall EK-60 score nor its subscores correlated with QST parameters or QST findings on the right hand. To our knowledge, this is the first study to comprehensively evaluate the relationship among CMRs/withdrawal reflexes and intrapersonal and interpersonal emotion processing. The correlation between CSP and anxiety [11], modulation of withdrawal reflex amplitude in response to phobic stimulation [7], and inhibition of intrinsic hand muscle motor-evoked potentials after cortical stimulation by observation of another person’s pain [12] further support a relationship among mood, anxiety, emotion processing, and motor control. These findings, along with our observations, appear to contrast with other animal model studies describing two different pathways for reflexive and affective behaviour after noxious stimulation [34]. However, Mas-related G protein-coupled receptor D-positive spinal neurons are involved in reflexive responses in healthy mice, but their activation elicits affective behaviour in mice with chronic pain [34]. This observation suggests that pain may modulate the activity of spinal neurons, thus allowing the expression of either simple reflexive or more complex affective behaviour. The so-called “emotional motor system”, responsible for behaviour in response to emotion-inducing stimuli [35,36], encompasses the periaqueductal grey and the locus coeruleus (LC). The LC can modulate withdrawal reflexes in rats [37] via its spinally projecting neurons [38]. Furthermore, the LC firing pattern (tonic or phasic) can modulate behavioural modes ranging from distractibility to task-oriented behaviour elicited by decision processing and salient sensory stimuli [39]. LC cortical projections include the anterior cingulate cortex and motor cortex [39]. Emotion-regulating neural circuits, including the amygdala and anterior cingulate cortex, can modulate the brainstem nuclei involved in the emotional motor system. Layer 5 neurons in the prelimbic area in mice (corresponding to area 32 in humans [40]) project to the ventrolateral periaqueductal grey, which in turn projects to the LC [41]. This circuit is inhibited by projections from the basolateral amygdala. Therefore, activation of the basolateral amygdala influences avoidance behaviour by modulating the prelimbic cortex/ventrolateral periaqueductal grey circuit, thus reducing noradrenergic e serotoninergic inputs to the spinal cord [41]. These observations further suggest that forelimb and brainstem structures controlling withdrawal reflexes also control more complex behaviour; therefore, it is conceivable that modulation of both withdrawal reflexes and CMRs is part of the response to emotion-inducing stimuli, particularly in the presence of chronic pain. Our study highlighted the correlations between both CMRs and withdrawal reflexes in the upper limbs and metrics of intrapersonal and interpersonal emotion regulation. Only some of the correlations were influenced by sensory perception or years of education; thus, the correlation of right-hand CMR (a component of optimal motor control [6]) with alexithymia and emotion recognition in others (evaluated by EK-60) seems to suggest a direct interaction between emotion recognition and motor control.
Eliciting withdrawal reflexes in humans activates of the anterior cingulate cortex and deactivates the posterior cingulate cortex [42]. As these cortical areas are also strongly involved in emotion processing, a functional overlap between nocifensive reflex circuits and emotional regulation is plausible. Furthermore, various aspects of social cognition [43], and emotions in particular, are considered primary reinforcers that guide goal-directed actions in the environment [44]. Within this framework, it is therefore conceivable that components of the motor infrastructure, such as CMR, which is involved in fine hand movements [3,5,6], as well as withdrawal nocifensive reflexes [3,4], may be modulated by emotion-regulation processes and mood.
Limitations of the Study
This study includes patients with neuropathic pain involving the upper limb, so the relationship between emotion regulation, CMRs, and withdrawal reflexes could be influenced by pain itself. Further studies on different neurological and psychiatric patient groups could elucidate whether CMRs and withdrawal reflexes are related to emotion processing independently. In addition, studies on patients with non-neuropathic pain (nociceptive and primary chronic pain) could clarify the effect of pain itself versus its pathophysiology on the relationship between CMRs/withdrawal reflexes and emotion processing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sherrington C.S. Flexion-reflex of the limb, crossed extension-reflex, and reflex stepping and standing J. Physiol.1910402812110.1113/jphysiol.1910.sp 00136216993027 PMC 1533734 · doi ↗ · pubmed ↗
- 2Kandel E.R. Schwartz J.H. Jessel T.M. Siegelbaum S.A. Hudspeth A.J. Spinal Reflexes Principles of Neural Sciences 4th ed.Mc Graw-Hill Companies Columbus, OH, USA 2000790811
- 3Pierrot-Deseillighy E. Burke D. Cutaneomuscular, withdrawal and flexor reflex afferent responses The Circuitry of the Human Spinal Cord Pierrot-Deseillighy E. Cambridge University Press Cambridge, UK 2005384451
- 4Floeter M.K. Cutaneous silent periods Muscle Nerve 20032839140110.1002/mus.1044714506711 · doi ↗ · pubmed ↗
- 5Caccia M.R. Mc Comas A.J. Upton A.R. Blogg T. Cutaneous Reflexes in Small Muscles of the Hand J. Neurol. Neurosurg. Psychiatry 19733696097710.1136/jnnp.36.6.9604272546 PMC 1083596 · doi ↗ · pubmed ↗
- 6Isoardo G. Rota E. Ciullo S. Titolo P. Matteoni E. Stura I. Calvo A. Fontana E. Battiston B. Migliaretti G. Psychophysiological and Neurophysiological Correlates of Dropping Objects from Hands in Carpal Tunnel Syndrome Brain Sci.202313157610.3390/brainsci 1311157638002536 PMC 10670400 · doi ↗ · pubmed ↗
- 7Fragiotta G. Pierelli F. Coppola G. Conte C. Perrotta A. Serrao M. Effect of phobic visual stimulation on spinal nociception Physiol. Behav.2019206222710.1016/j.physbeh.2019.03.02130902634 · doi ↗ · pubmed ↗
- 8Terry E.L. Thompson K.A. Rhudy J.L. Does pain catastrophizing contribute to threat-evoked amplification of pain and spinal nociception?Pain 201615745646510.1097/j.pain.000000000000039230888338 · doi ↗ · pubmed ↗