Pharmacological Management of Cancer Pain: Advances in Treatment Strategies and Drug Delivery Systems
Xueying Yang, Rong Zhang, Aijia Wang, Dan Zhang, Jiangxue Cheng, Bingtao Zhai, Dongyan Guo

TL;DR
This paper reviews new strategies and drug delivery systems for managing cancer pain, emphasizing the benefits of combining traditional Chinese and Western medicine.
Contribution
The paper introduces a novel integration of traditional Chinese and Western medicine and evaluates new drug delivery systems for cancer pain.
Findings
Integrated traditional Chinese and Western medicine reduces adverse reactions and enhances synergy in cancer pain management.
New drug delivery systems like microneedles and nano-drug delivery systems show promise for more effective cancer pain treatment.
Multi-target analgesic mechanisms involving inflammatory factors and glial cells are key to improving pain control.
Abstract
Cancer pain seriously damages the quality of life of patients, and its management urgently needs new strategies with both efficacy and safety. This review deeply analyzes the clinical limitations of WHO’s third-order analgesic strategy in cancer pain management, especially emphasizes the unique value of integrated traditional Chinese and Western medicine in synergy and reduction in adverse reactions, and summarizes the network interaction of related drugs through the regulation of multi-target analgesic mechanisms such as inflammatory factors, ion channels, neurotransmitters, and even glial cells and osteoclast activity in the tumor microenvironment. Building on this foundation, the article systematically analyzed the clinical advantages and limitations of drug delivery systems (DDS): oral sustained and controlled drug delivery system, mucosal drug delivery system (MDDS), transdermal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
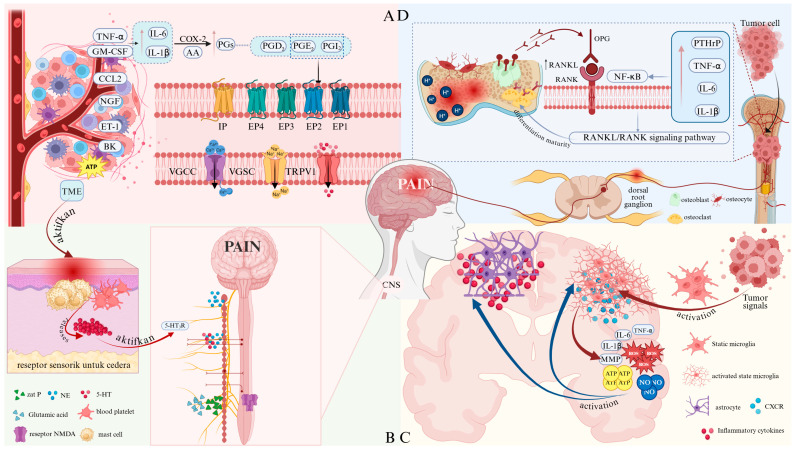 Figure 1
Figure 1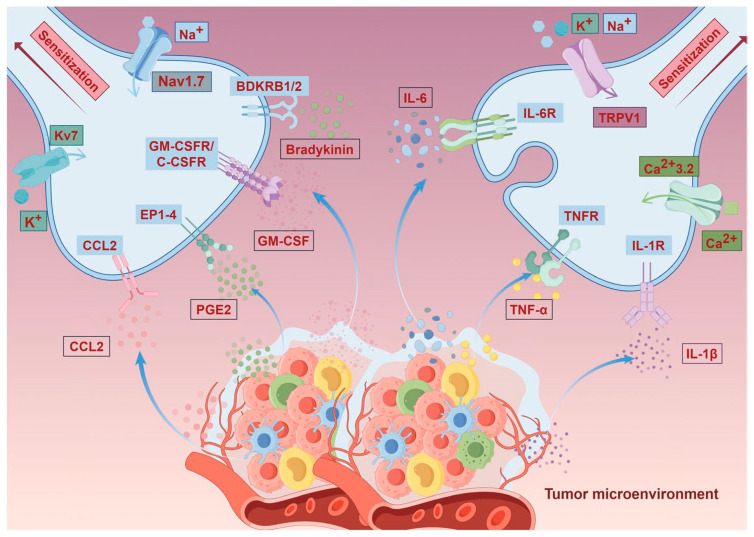 Figure 2
Figure 2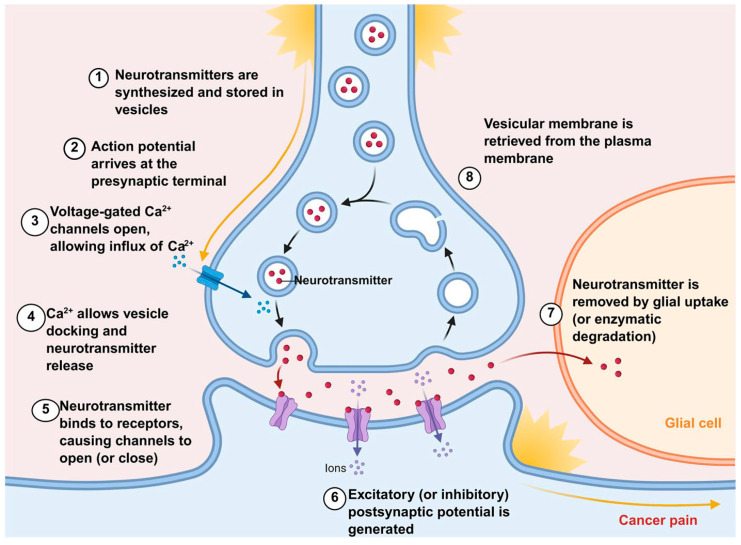 Figure 3
Figure 3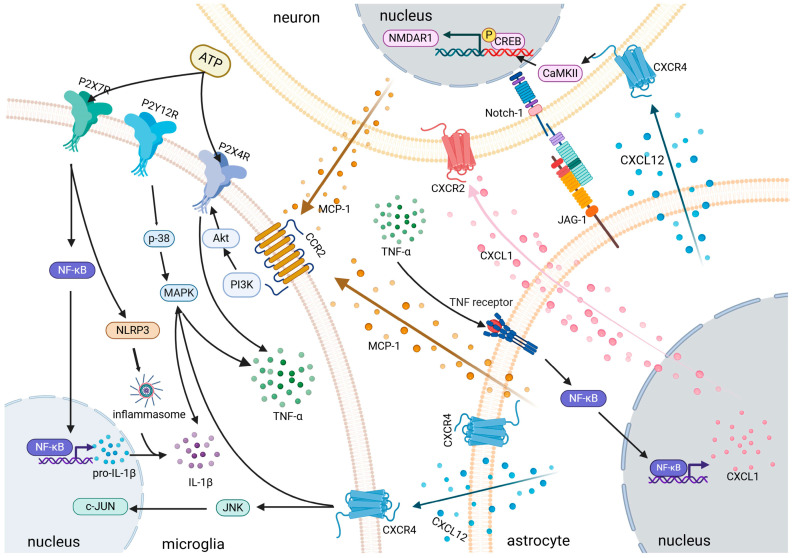 Figure 4
Figure 4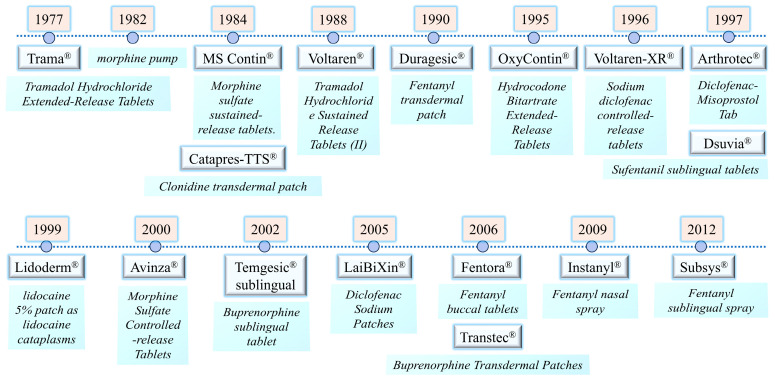 Figure 5
Figure 5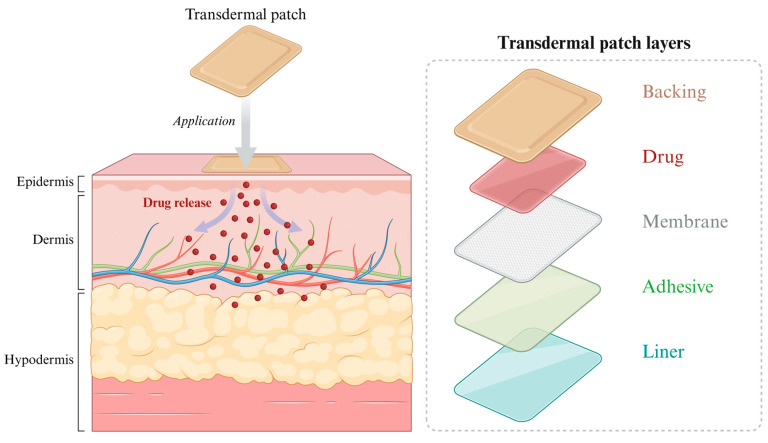 Figure 6
Figure 6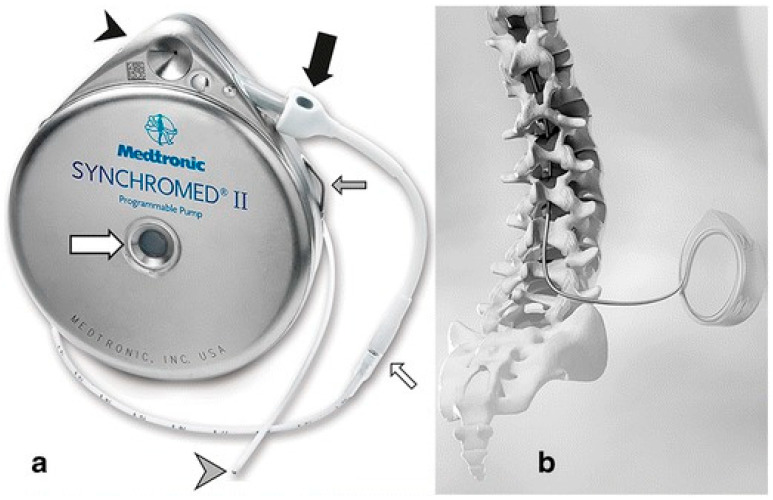 Figure 7
Figure 7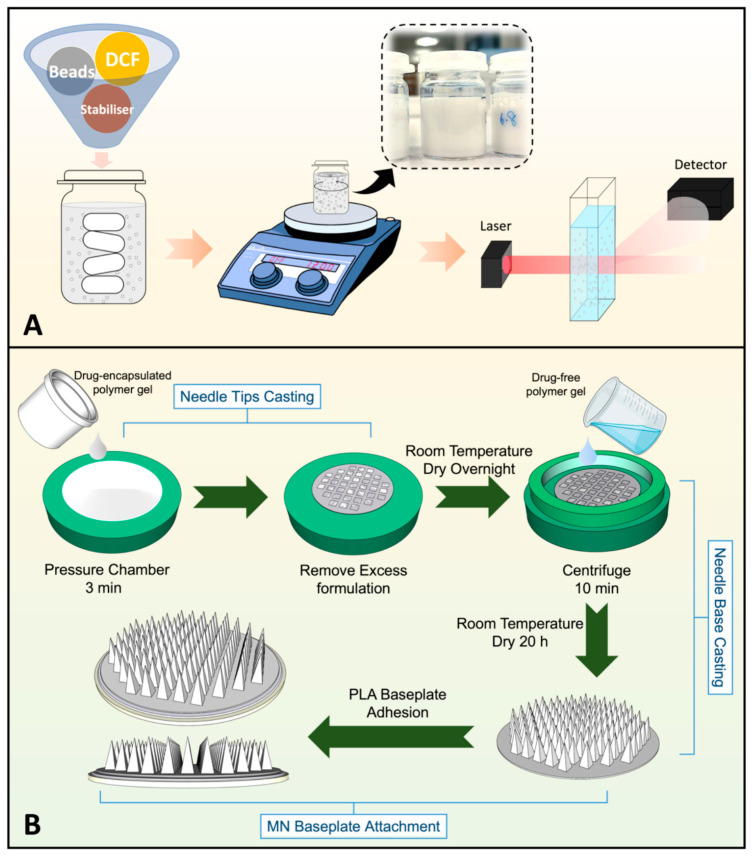 Figure 8
Figure 8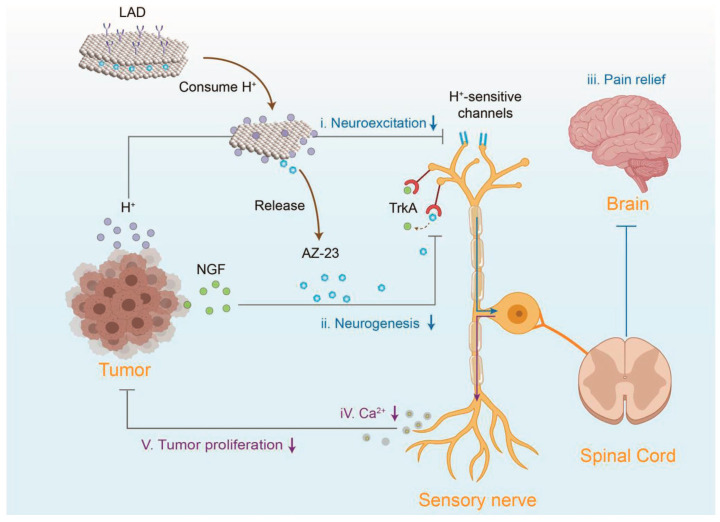 Figure 9
Figure 9 Figure 10
Figure 10| Classification of Drugs | Marketed Drugs | Initial Time to Market | Clinical Use for Cancer pain | Common Medication Dosage Forms and Dosages | Short-Term Side Effects | Long-Term Side Effects |
|---|---|---|---|---|---|---|
| APAP | Paracetamol tablets [ | 1955 (US) | Mild pain | Tablets, Capsules, Suppositories, Suspensions; 650 mg/4 h or 1 g/6 h; ≤4 g/d | Overdose may cause acute liver toxicity | Hepatotoxic |
| NSAIDs | Ibuprofen [ | 1969 (UK) | Mild to moderate cancer pain with inflammation | Tablets, Granules; ≤3200 mg/d | GI irritation, nausea, abdominal pain | GI irritation; liver, kidney damage |
| Diclofenac sodium tablets [ | 1988 (US) | Bone metastasis pain, Postoperative mild to moderate pain, Cancerous arthritis pain | Tablets, Suppositories, Topical Emulsions, Transdermal Patches; ≤150 mg/qd | GI discomfort, headache; local skin reactions (topical use) | GI tract; kidneys, cardiovascular risks | |
| Aspirin enteric-coated tablets [ | 1889 (Germany) | Mild pain accompanied by fever and bone metastases | Tablets, Suppositories; 30–60 mg/tid | GI irritation, tinnitus, bleeding tendency | GI bleeding; Reye’s syndrome risk (children/adolescents); Salicylate poisoning | |
| Naproxen tablets [ | 1976 (US) | Chronic and acute pain | Tablets, Suspensions; ≤1500 mg/d | GI discomfort, dizziness, drowsiness | Risk of cardiovascular thrombosis; GI ulcers, and bleeding | |
| Celecoxib [ | 1998 (US) | Osteoarthritis/RA Pain, Visceral Pain | Capsules; ≤200 mg/bid | Cardiovascular and GI risks | Cardiovascular thrombosis; renal impairment | |
| Meloxicam tablets [ | 1996 (European) | Bone metastasis pain, Chronic cancer pain from soft tissue tumors | Tablets, Suppositories; 7.5 mg/qd | Indigestion, nausea, abdominal pain | Risk of nephrotoxicity and bone marrow suppression | |
| Indomethacin tablets [ | 1965 (US) | Moderate cancer pain | Tablets, Suppositories; 25 mg/bid | Significant GI reactions, headache, dizziness | GI ulcers, central nervous system toxicity, bone marrow suppression | |
| Ketorolac injection [ | 1990 (Italy) | Moderate to severe acute cancer pain, Preferred for short-term control | Injections, Tablets; 15–30 mg/6 h, ≤5 d | High risk of GI bleeding; injection site pain; renal impairment | Long-term use can easily lead to severe gastrointestinal bleeding and acute renal failure. | |
| Weak opioids | Tramadol [ | 1977 (Germany) | Moderate to severe acute and chronic pain | Tablets, Capsules, Injections; ≤400 mg/d | Nausea, vomiting, dizziness, drowsiness | Tolerance and Dependence |
| Buprenorphine injection [ | 1981 (US) | Chronic Cancer Pain | Injections, Oral Dispersible Tablets, Transdermal patch; ≤900 μg/d | Nausea, drowsiness, constipation; risk of respiratory depression | Physical dependence; withdrawal symptoms occurring after discontinuation | |
| Strong opioids | Morphine tablets [ | 1827 (Germany) | Moderate to severe cancer pain, Breakthrough Pain, Postoperative Pain | Tablets 15–60 mg/d, Injections 15–40 mg/d | Nausea, vomiting, constipation, drowsiness, respiratory depression | Tolerance, physical and psychological dependence |
| Oxycodone extended-release tablets [ | 1995 (US) | Moderate to severe cancer pain, Neuropathic pain | Tablets; ≤40 mg/d | Constipation, nausea, dizziness | Tolerance, Dependence | |
| Fentanyl injections [ | 1968 (US) | Persistent cancer pain, Breakthrough pain | Transdermal Patches 12–100 mg/q 72 h, Injections 0.05–0.1 mg/dose, Lozenges, Nasal Sprays; - | Dizziness, blurred vision, nausea, vomiting, hypotension | Respiratory depression, asphyxia, muscle rigidity, and tachycardia | |
| Hydromorphone hydrochloride injection [ | 1972 (US) | Moderate to severe cancer pain | Injection, Tablet, Capsule; ≥8 mg/d | Dizziness, nausea, sweating | Respiratory depression and apnea | |
| Methadone tablets [ | 1947 (Germany) | Refractory Cancer Pain | Tablets, Injections; ≤45 mg/d | Risk of QT interval prolongation, complex drug interactions, accumulation and toxicity risks | Long half-life, respiratory depression, complex long-term management, high potential for addiction | |
| Anticonvulsants | Gabapentin capsules [ | 1993 (US) | Neuropathic Cancer Pain | Capsule, Tablet, Oral Liquid; 900–3600 mg/d | Dizziness, drowsiness, fatigue, ataxia | Weight gain, peripheral edema |
| Pregabalin capsules [ | 2004 (US) | Neuropathic Cancer Pain | Capsules, Oral Liquid; ≤600 mg/d | Dizziness, drowsiness, blurred vision | Weight gain, peripheral edema | |
| tricyclic antidepressants | Duloxetine capsules [ | 2004 (US) | Neuropathic cancer pain with depression | Enteric-coated capsules; ≤120 mg/d | Nausea, dry mouth, insomnia, constipation; may increase suicide risk in the early stages | Liver and kidney damage, discontinuation syndrome |
| Amitriptyline tablets [ | 1961 (US) | Neuropathic cancer pain | Tablets; 50–150 mg/qn | Dry mouth, constipation, blurred vision, drowsiness | Cardiac toxicity, weight gain, cognitive effects | |
| Local anesthetic | Lidocaine injection [ | 1948 (US) | Localized cancer pain | Injections, Patches, Gels; ≤200 mg/dose | Local skin reactions, systemic toxicity | Skin allergy or intolerance, systemic toxicity |
| Ropivacaine injection [ | 1996 (US) | Acute pain | Injections; 20–40 mg/d | Hypotension, nausea, vomiting, bradycardia, abnormal sensations | Risk of localized tissue toxicity or nerve damage | |
| Bisphosphonates | Zoledronic acid powder injection [ | 2001 (US) | Bone Metastasis Cancer Pain | Injections; 4 mg, IV ≥15 min, 3–4 dose/weeks | Fever, bone pain, hypocalcemia, nephrotoxicity | Mandibular necrosis, atypical femoral fracture |
| The glucocorticoid hormone | Dexamethasone tablets [ | 1958 (US) | Acute nerve compression pain, intracranial hypertension pain | Tablets 0.75–3 mg/bid, Injections IV 2–20 mg/dose | Mood swings, elevated blood sugar, insomnia, indigestion | Cushing’s syndrome, osteoporosis, immunosuppression, muscle atrophy, cataracts |
| Prednisone tablets [ | 1955 (US) | Chronic cancer pain with inflammation | Tablets 10–60 mg/d | Fluid retention, hypertension, and hyperglycemia are more pronounced | Adrenal cortex suppression | |
| α-2 adrenergic agonists | Clonidine tablets [ | 1974 (US) | Adjuvant Therapy for Refractory Cancer Pain | Tablets 0.1–0.3 mg/bid, Transdermal Patches 0.1–0.3 mg/d | Dry mouth, drowsiness, dizziness, hypotension, bradycardia | Long-term use leads to tolerance |
| Dexmedetomidine injection [ | 1999 (US) | Sedation and Analgesia for Cancer Pain in the Intensive Care Unit | Injections 0.2–0.7 μg/kg/h | Hypotension, bradycardia | Tolerance | |
| Tizanidine tablets [ | 1996 (US) | Spasmodic cancer pain | Tablets 2–4 mg/tid, ≤36 mg/d | Drowsiness, dry mouth, dizziness, low blood pressure, risk of liver toxicity | Hepatotoxicity and nephrotoxicity, tolerability | |
| NMDA receptor antagonist | Ketamine injection [ | 1970 (US) | Refractory cancer pain | Injections, Nasal Sprays; | Psychiatric symptoms, hypertension, tachycardia, nausea | Neurotoxicity, cognitive impairment |
- —National Natural Science Foundation of China
- —Qinchuangyuan Traditional Chinese Medicine Industry Innovation Aggregation Zone Project
- —Key Research and Development Programme of Shaanxi Province
- —Shaanxi University of Traditional Chinese Medicine Discipline Innovation Team Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPain Management and Opioid Use · Cancer, Stress, Anesthesia, and Immune Response · Pharmacological Effects of Natural Compounds
1. Introduction
Cancer pain is one of the most common and distressing symptoms experienced by cancer patients, presenting a significant clinical challenge in management. Statistics indicate that 60% of patients undergoing anticancer treatment will experience pain, with 50% suffering moderate to severe pain and 30% enduring excruciating, unbearable pain [1]. Furthermore, 33% to 40% of survivors who completed curative treatment continue to experience chronic pain [2]. The etiology of cancer pain is complex and multifactorial, encompassing pain directly caused by the tumor, pain resulting from tumor infiltration and vascular obstruction, pain arising from tumor obstruction of hollow or solid organ lumens, and pain triggered by mucosal ulceration and infection [3]. Pain may also occur during diagnostic procedures such as gastroscopy, colonoscopy, or esophagoscopy, when instruments damage peripheral receptors. Additionally, pain associated with cancer treatments-including postoperative pain, chemotherapy-induced pain, drug tolerance, and post-radiotherapy pain-presents significant challenges. Pain unrelated to the cancer itself or its diagnosis/treatment, as well as psychologically induced pain, also holds considerable importance [4]. Consequently, cancer pain remains a major clinical challenge. Its high prevalence, complexity, and profound impact on patients’ quality of life make effective management particularly difficult [5].
The World Health Organization (WHO) three-step ladder approach to cancer pain management has established the foundation for standardized global cancer pain care. For patients with mild cancer pain, non-opioid medications are prioritized, while weak opioids are initiated for moderate cancer pain, escalating to strong opioids as pain worsens [6]. For neuropathic cancer pain, adjunctive medications such as antiepileptics, tricyclic antidepressants (TCAs), and N-methyl-D-aspartate (NMDA) antagonists are required [7]. However, these approaches may be accompanied by numerous adverse reactions [8] and ofen demonstrate poor efficacy in advanced stages. In recent years, traditional Chinese medicine (TCM) has demonstrated unique advantages in treating cancer pain [9]. Formulas such as Peony and Licorice Decoction, Huachansu Capsules, Xihuang Pills, and Compound Kushen Injection can be combined with Western analgesics for cancer pain management. These combinations reduce adverse reactions while enhancing pain relief [10], offering novel approaches and combination strategies for cancer pain management. Ultimately, the efficacy of these interventions depends on precise targeting of the complex mechanisms underlying cancer pain.
Research indicates that the pathophysiological mechanisms of cancer pain involve multiple parallel and interacting pathways, including the release of inflammatory mediators, abnormal activation of ion channels, bone destruction, central sensitization, and glial cell activation [11]. Accordingly, existing drugs exert their effects through various mechanisms, such as inhibiting inflammatory factors, regulating ion channels, suppressing osteoclast activity, or modulating central sensitization. For example, nonsteroidal anti-inflammatory drugs (NSAIDs) [12], corticosteroids [13], and many traditional Chinese medicines suppress inflammatory factors [14]; anticonvulsants, local anesthetics, and Peony and Licorice Decoction modulate ion channels; bisphosphonates [15] and Huachansu inhibit osteoclast activation; while NMDA receptor antagonists like ketamine and TCAs target central sensitization [16]. Additionally, drugs such as Huachansu suppress glial cell activation [17]. These findings provide valuable insights for developing more synergistic treatment strategies.
Beyond this, drug delivery systems (DDS) have demonstrated significant potential in managing cancer pain. Oral controlled-release DDS enable prolonged, controlled analgesic effects while reducing dosing frequency [18]. Mucosal DDS provide rapid pain relief, making them particularly suitable for breakthrough cancer pain (BTP) [19]. Transdermal DDS maintain sustained drug release, offering long-lasting and consistent efficacy [20]. Intrathecal DDS minimize systemic side effects and provide a rapid onset of action [21]. Furthermore, the emergence of novel DDS—including implantable devices, targeted small molecules, nanoparticles (NPs), microspheres, and liposomes—has opened new avenues for cancer pain management.
Given the complex pathophysiological mechanisms underlying cancer pain, existing three-tier pain management guidelines fail to meet clinical demands. Current research predominantly focuses on the pathogenesis of cancer pain, the role of individual targets in cancer pain, and the clinical application of analgesics within the three-tier framework. However, no systematic review has yet been conducted on the development of integrated Chinese and Western medicine approaches or DDS in cancer pain management. Therefore, this paper searched databases including the Cochrane Library, PubMed, SCI, CNKI, and X-MOL using keywords such as “cancer pain,” “cancer pain treatment drugs,” “combination of Chinese and Western medicine,” “cancer pain mechanisms,” and “DDS.” It reviews advances in the three-step analgesic approach for cancer pain treatment, identifies the unique advantages of integrated Chinese and Western medicine therapy, and summarizes the mechanisms of action of the aforementioned drugs in cancer pain management. Furthermore, the potential of DDS in cancer pain management is emphasized, and the application prospects of novel DDS in cancer pain are discussed. This aims to provide new strategies and insights with clear guidance for future research and clinical practice in cancer pain treatment.
2. Drug Management of Cancer Pain
2.1. WHO Three-Step Pain Management
In 1986, the WHO published the Pain Management Guidelines for Cancer and recommended the global implementation of this protocol. Clinical practice has demonstrated that standardized application of the three-step approach can effectively control 80% to 90% of cancer-related pain, significantly improving patients’ quality of life [22]. See Table 1 for details.
The core of pharmacological treatment involves escalating medication based on pain intensity. The first step employs non-opioid medications for mild cancer pain, including acetaminophen (APAP) and NSAIDs. Since APAP alone has limited efficacy in relieving cancer pain [23], it is often combined with weak opioid medications. NSAIDs are the preferred treatment for mild pain. Commonly used NSAIDs include ibuprofen, diclofenac, celecoxib, etoricoxib, and loxoprofen. They are particularly effective in the presence of inflammation but carry long-term side effects such as gastrointestinal ulcers, gastrointestinal bleeding, platelet dysfunction, liver and kidney damage, and cardiac toxicity [24]. When NSAIDs or APAP reach their dosage limits or their adverse effects become intolerable, switching to other types of analgesics is recommended. Considering the potential risks of long-term use, cancer pain may be managed with either monotherapy or combination therapy with opioids based on individual circumstances [25].
The second step involves the use of weak opioids, such as tramadol and buprenorphine, for managing moderate pain; however, repeated or prolonged use may cause nausea, dizziness, respiratory depression, and mild dependence [26,27]. The third step prioritizes potent opioids, including morphine, oxycodone, fentanyl, hydromorphone, and methadone, which can be administered orally, intravenously, or subcutaneously for dose titration [28]. In palliative care, a direct transition from non-opioid analgesics to opioids is increasingly preferred. Additionally, opioid tolerance developed during long-term use reduces analgesic efficacy, necessitating dosage escalation by clinicians. This escalation can lead to addiction and physical dependence, representing a significant limitation to their sustained clinical use [29]. Moreover, prolonged opioid use may cause adverse reactions such as constipation, intractable vomiting, and respiratory depression. These side effects not only diminish patients’ quality of life but also compromise treatment efficacy. Therefore, developing strategies to reduce opioid dosages while maintaining effective pain management is crucial in clinical practice.
Additionally, adjunctive medications are often combined for patients with neuropathic cancer pain, including antiepileptic drugs (gabapentin, pregabalin), TCAs, local anesthetics (lidocaine, ropivacaine), bisphosphonates, corticosteroids (dexamethasone, prednisone), alpha-2 adrenergic agonists (clonidine, dexmedetomidine, tizanidine), and NMDA receptor antagonists (ketamine). These agents provide multimodal analgesia while reducing opioid dependence and adverse effects [30].
2.2. Clinical Application of Combined Chinese and Western Medicine in the Treatment of Cancer Pain
In standardized cancer pain management, while Western pharmaceutical analgesic regimens based on the WHO three-step ladder have significantly improved patient outcomes. However, patients with moderate to severe cancer pain often encounter challenges such as opioid dose dependence and adverse reactions. Therefore, it is crucial to identify proactive and effective cancer pain treatment strategies that minimize the side effects associated with Western medications. In recent years, the emergence of integrated Chinese and Western medicine therapies have emerged as effective options for relieving cancer pain. These approaches provide comprehensive benefits, including analgesia, anti-inflammation, antitumor activity, and immune modulation. Within comprehensive cancer pain management, they demonstrate long-term efficacy by enhancing therapeutic outcomes while reducing toxicity. Specific details are provided in Table 2.
Among these, the Kidney-Nourishing Bone-Strengthening Formula and Kidney-Nourishing Pain-Relieving Granules are derived from Liuwei Dihuang Wan, with modifications incorporating herbs that resolve stasis and detoxify. These formulas have the effects of nourishing the kidneys and replenishing marrow, strengthening tendons and bones, and resolving stasis and detoxifying. Clinically, they are frequently used to treat somatic cancer pain and bone metastasis-related cancer pain [84]. Song Hongli [60,61] found that combining the Yishen Gukang Formula with hydrocodone bitartrate extended-release tablets demonstrated superior efficacy in alleviating pain compared to Western medicine alone in patients with moderate-to-severe cancer-related somatic pain presenting with kidney deficiency and blood stasis syndrome. Furthermore, the Yishen Gukang Formula significantly reduced the frequency of breakthrough pain episodes and the required dosage of OxyContin, thereby mitigating adverse reactions such as dizziness, constipation, and nausea associated with high-dose opioid use. Zhang Qinglin [62] found that combining Yishen Qutong Granules with hydrocodone bitartrate extended-release tablets significantly reduced Numerical Rating Scale (NRS) scores, decreased the frequency of breakthrough pain episodes, and lowered OxyContin dosage in patients with moderate-to-severe kidney deficiency with toxin-stasis syndrome and bone metastasis cancer pain. The treatment demonstrated good safety.
Xuefu Zhuyu Tang, derived from Wang Qingren’s Medical Forest Corrections, is effective in promoting blood circulation, removing blood stasis, regulating qi, and alleviating pain. Xu Zhengyin [66] found that combining Xuefu Zhuyu Tang with hydrocodone bitartrate extended-release tablets significantly reduced NRS scores, cancer pain frequency, and adverse reactions (nausea, vomiting, constipation, anorexia) compared to the control group in patients with cancer pain caused by qi deficiency and blood stasis syndrome. Zheng Qiao [65] reported that combining Blood Residence Stasis-Resolving Decoction with standardized pain management reduced opioid consumption and improved clinical efficacy in patients with advanced lung cancer experiencing cancer pain caused by blood stasis obstructing the collaterals. Zhang Hongsheng [64] treated patients with liver cancer pain due to blood stasis obstruction syndrome using a combination of Blood Residence Stasis-Resolving Decoction and morphine hydrochloride sustained-release tablets. The treatment group demonstrated significantly higher overall pain relief rates and lower NRS scores compared to the control group. Levels of prostaglandin E2 (PGE2) and nitric oxide (NO) were significantly reduced, confirming the definite efficacy of this formula in treating cancer pain.
Yuanhu Zhitong Tablets are a commonly used oral analgesics in clinical practice, containing two Chinese herbal medicines with analgesic properties: Angelica dahurica and Corydalis yanhusuo. Although their analgesic potency is weaker than that of opioids, they offer convenient administration, fewer adverse reactions, and reliable safety [85]. Tan Dan [63] combined Yuanhu Zhitong Tablets with strong opioid medications to manage moderate-to-severe postoperative pain in lung cancer patients. The study demonstrated significant analgesic efficacy with fewer adverse reactions, enhancing patient tolerance and improving treatment compliance.
The bone pain patch has warming yang properties, dispels cold, unblocks meridians, and relieves pain. It is clinically used to treat cancer pain caused by bone metastases. Hou Zhaolin [67] combined the bone pain patch with oxycodone hydrochloride extended-release tablets to treat bone metastasis cancer pain characterized by a yin-cold stagnation pattern. This combination significantly reduced NRS scores, demonstrated superior efficacy compared to oxycodone hydrochloride alone, and showed no significant skin toxicity reactions, indicating a high level of safety.
The primary active ingredient in Aconitine Capsules is aconitine, which exhibits potent analgesic effects. Li Fang [83] demonstrated that combining Aconitine Capsules with morphine sulfate sustained-release tablets in patients with moderate-to-severe cancer pain reduced the required dosage of morphine sulfate sustained-release tablets and decreased the incidence of adverse reactions.
Yanghe Decoction, derived from the Complete Collection of Surgical Diagnosis and Treatment, has the effects of yang to stop bleeding and dispelling cold to unblock stagnation. It is commonly used clinically to treat lung cancer bone metastases. Zhang Chunmei [69] found that Yanghe Decoction synergistically enhances the efficacy of zoledronic acid, thereby more effectively alleviating pain caused by bone metastases. Feng Lei [68] demonstrated that combining Yanghe Decoction with zoledronic acid effectively reduces pain from bone metastases, improves clinical outcomes, enhances patients’ quality of life, and lowers TCM syndrome scores, while maintaining good safety. These findings suggest that Yanghe Decoction can serve as an adjunctive therapy for patients with bone metastases from breast cancer exhibiting the yang deficiency and cold stagnation pattern.
The Peony and Licorice Decoction, first documented in the Treatise on Cold Damage Diseases, plays a positive role in harmonizing qi and blood, soothing the liver, and relieving pain. Feng Xiaofei [70] demonstrated that combining Peony and Licorice Decoction with extended-release hydrocodone bitartrate tablets in patients with moderate-to-severe cancer pain improved pain relief rates, reduced pain intensity and breakthrough pain episodes, decreased adverse reactions, and enhanced patient prognosis. This combination may serve as a standard regimen for managing moderate-to-severe cancer pain. In particular, among patients with ovarian cancer pain, this combination therapy reduced the average daily hydrocodone dose by 24.69 mg, accelerated the average onset time by 13.26 min, prolonged analgesic duration by 2.11 h, and significantly lowered levels of pain-related factors, including serotonin (5-HT), PGE2, substance P, tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), and IL-6 [71].
Similarly, Xihuang Pills—a pure herbal anticancer medication derived from the ancient Xihuang formula—possess analgesic, antipyretic, detoxifying, blood-activating, stasis-resolving, and swelling-reducing properties. They are widely used to treat various mid-to-late-stage malignant tumors. Hong You [72] combined Xihuang Pills with extended-release hydrocodone hydrochloride tablets to treat 80 patients experiencing moderate-to-severe cancer pain from lung, esophageal, liver, and rectal cancers. This combined therapy increased the overall pain relief rate by 11.67% and reduced the incidence of adverse reactions by 27.15%. Among lung cancer pain patients, the treatment efficacy rate in the observation group was 14% higher than in the control group. At 1 h, 12 h, 1 week, and 2 weeks post-administration, the NRS scores in the observation group were consistently lower than those in the control group. The incidence rates of adverse reactions such as constipation, dizziness or drowsiness, nausea or vomiting, and urinary difficulty were comparable between the two groups [73]. Thus, combining Xihuang Pills with hydrocodone bitartrate extended-release tablets enhances analgesic efficacy and improves quality of life in patients with moderate-to-severe cancer pain. Yan Qingyuan’s [73] study demonstrates that this combination therapy in lung cancer pain patients achieves synergistic, rapid pain relief without increasing adverse reactions, advancing the development of integrated Chinese and Western medicine approaches for cancer pain management.
Additionally, huachansu, the primary active component extracted from the entire skin of the Chinese toad Bufo bufo gargarizans Cantor, has been widely used in patients with mid-to-late-stage cancer pain, demonstrating particularly pronounced efficacy for bone metastasis-related pain [86]. Yangsen [77] found that combining Huachansu capsules with fentanyl transdermal patches significantly alleviated pain in patients with moderate to severe bone metastases without increasing adverse reactions. Feng Zhang [78] observed that co-administering Huachansu capsules with zoledronic acid injections improved bone density and calcium and phosphorus metabolism, reduced pain symptoms, and enhanced safety in prostate cancer patients with bone metastases. Fang Yun [74] combined Huachansu capsules with hydrocodone bitartrate extended-release tablets for cancer pain management, observing enhanced efficacy, reduced adverse reactions, and improved quality of life. Zhang Yi [75] demonstrated that Huachansu capsules combined with hydrocodone bitartrate extended-release tablets alleviated pain severity and reduced adverse reaction rates in patients with moderate-to-severe cancer pain, indicating Huachansu as an effective adjunctive Chinese herbal medicine for improving cancer pain symptoms. Dong Xueshan [76] found that combining morphine sulfate sustained-release tablets with Huachansu capsules significantly improved pain management outcomes and quality of life while reducing the average daily dosage of morphine sulfate sustained-release tablets.
Compound Kushen Injection is a pure herbal preparation primarily derived from Sophora flavescens, known for its hemostatic and analgesic properties. Xiang Pei [79] demonstrated that combining Compound Kushen Injection with standardized pain management significantly enhanced analgesic efficacy in patients with severe cancer pain while reducing opioid analgesic dosage and adverse reactions. Zhou Li [80] showed that adding Compound Kushen Injection to hydrocodone bitartrate extended-release tablets and pregabalin for neuropathic cancer pain alleviated patient discomfort. The analgesic effect improved with combined therapy, and the addition of Compound Kushen Injection further controlled pain while decreasing adverse events. Miao Jidong [81] found that combining Compound Kushen Injection with sustained-release morphine hydrochloride tablets for moderate-to-severe cancer pain provided enhanced analgesia and reduced adverse event rates. Zhang Jingjing [82] reported that co-administering Compound Kushen Injection with fentanyl transdermal patches significantly decreased gastrointestinal reactions without causing hepatic or renal damage. This combination also reduced the release of inflammatory factors, effectively alleviating cancer pain.
3. Therapeutic Mechanisms of Drugs
Although the three-step analgesic ladder and integrated Chinese and Western medicine therapies have established well-defined application protocols in the clinical management of cancer pain, their efficacy fundamentally depends on intervening in the complex pathological mechanisms underlying this condition. Cancer pain, a multifaceted symptom associated with tumors, involves multiple pathways, including the release of inflammatory factors, regulation of ion channels, activation of osteoclasts, and release of pain mediators (Figure 1). Current pharmacological treatments achieve therapeutic effects by targeting these key pathways. For specific details, see Table 3.
3.1. Regulation Inflammatory Factors in the Tumor Microenvironment
3.1.1. Direct Inhibition of Inflammatory Factors
The origin of the cancer pain loop lies within the tumor tissue itself and its surrounding microenvironment (TME). Tumor cells, immune cells (such as macrophages and T cells), and tumor-associated fibroblasts continuously release large quantities of pro-pain mediators, including protons (H^+^), inflammatory cytokines, adenosine triphosphate (ATP), endothelin-1 (ET-1), and others. These substances persistently act on peripheral nociceptors, lowering their activation threshold and enhancing their responsiveness. This process leads to peripheral sensitization and the generation of cancer pain [112,113,114].
IL-6, a key member of the interleukin family, is secreted by macrophages, fibroblasts, T lymphocytes, and other cells, playing a crucial role in various inflammatory responses and diseases [115]. Evidence indicates that IL-6 enhances Toll-like receptor (TLR)-mediated cytokine production, suggesting its involvement in exacerbating inflammatory responses associated with cancer pain. IL-6 can also be self-induced in certain tumor cells, promoting their growth [116]. The release of IL-1β activates multiple signaling pathways, thereby enhancing pain perception. Furthermore, IL-1β upregulates macrophage expression of cyclooxygenase-2 (COX-2), amplifying prostaglandin (PG) synthesis [117] and inducing severe pain. Granulocyte-macrophage colony-stimulating factor (GM-CSF) contributes to increased IL-1β secretion [118]. TNF-α stimulates the release of IL-1β and IL-6, activates nociceptors, and exerts pro-nociceptive effects [119]. C-C chemokine ligand 2 (CCL2) promotes immune cell infiltration into the tumor microenvironment (TME), exacerbating inflammation and cancer pain perception [120]. The P2X3 receptor (purinergic receptor P2X, ligand-gated ion channel, 3) is highly and selectively expressed in small- and medium-diameter sensory neurons, mediating pain signal transmission [121]. Nerve growth factor (NGF) activates its high-affinity homologous receptor TrkA (tyrosine kinase receptor A), triggering intracellular signaling cascades that modulate the TME innervated by sensory and sympathetic nerve fibers, thereby inducing cancer pain [122]. ET-1 directly activates nociceptors and potentiates the pain-inducing effects of other noxious substances, including capsaicin, formaldehyde, and arachidonic acid (AA). Additionally, endothelial cells produce ATP, which sensitizes ET-1 receptors; released ATP activates P2X2/3 receptors on nociceptors, inducing pain generation [123]. Bradykinin (BK) increases nociceptor sensitivity, promotes cancer pain progression, and interacts with other inflammatory mediators to exacerbate pain [124].
In summary, the interactions among these inflammatory mediators—IL-6, IL-1β, TNF-α, CCL2, PGE2, GM-CSF, and BK—highlight their synergistic role in cancer pain mechanisms (Figure 2). Targeting these mediators may open new avenues for therapeutic interventions to alleviate pain in cancer patients. For instance, NSAIDs reduce inflammatory factors released by neutrophils and macrophages, such as IL-6 and TNF-α, thereby suppressing local inflammatory responses and alleviating inflammation-induced pain [88]. Hydrocodone decreases TNF-α and IL-1β levels, relieving cancer pain [125]. Amitriptyline reduces peripheral TNF-α production, mitigating inflammatory pain [96]. Lidocaine selectively inhibits P2X7 receptor expression to exert analgesic effects [126]. The Peony and Licorice Decoction may alleviate inflammatory pain by suppressing TNF-α expression and reducing leukocyte infiltration [127]. Huachansu inhibits the release of pro-pain mediators such as TNF-α, IL-1β, IL-6, and CCL2, thereby suppressing bone cancer pain (BCP) [128]. These findings demonstrate that direct inhibition of pain mediators effectively alleviates cancer pain.
3.1.2. Inhibition of COX Conversion to PGs
In anti-injury strategies, inhibiting COX reduces the conversion of its substrate, AA, into PGs. Inflammatory stimuli-induced overexpression of COX-2 leads to increased PGs in tumor regions. Among various PGs, PGE2, PGD2, and prostacyclin (PGI2) have been most extensively studied in nociception, with PGE2 typically associated with the induction of hyperalgesia. PGE2 and PGI2 activate EP and IP receptors on nociception, enhancing the activity of vanilloid transient receptor potential vanilloid 1 (TRPV1) channels and sodium channels (Nav1.9) through PKA-dependent phosphorylation, leading to mechanical and thermal hyperalgesia [88]. In contrast to PGE2 and PGI2, PGD2 modulates nociception through both peripheral and central mechanisms, either enhancing or reducing pain perception. Therefore, regulating the release of AA in the TME can effectively alleviate the onset of pain.
Among known therapeutic agents, APAP and NSAIDs reduce pain sensitization in inflammatory pain by inhibiting COX-1 and COX-2 in peripheral tissues, thereby decreasing the conversion of AA to PGs, thromboxanes, and PGI2. This occurs through reduced PGs synthesis [87]. Celecoxib, as a COX-2 inhibitor, exerts a direct targeted effect. APAP selectively inhibits COX-1 and COX-2 in the central nervous system (CNS), reducing central PGs synthesis and diminishing pain signal transmission [92]. Corticosteroids primarily suppress inflammation and edema by inhibiting phospholipase A2, reducing PGs and leukotrienes in peripheral tissues, thereby alleviating pain associated with tumor compression [93]. The boswellic acid components in Xihuangwan downregulate COX-2 expression, decreasing the conversion of AA to PGs [102], thereby exerting analgesic effects.
3.2. Regulation of Ion Channels
Ion channels are specialized proteins located on membranes or organelles that form highly selective pores in the phospholipid bilayer, allowing passively transported charged ions of appropriate size to pass through. Widely distributed across various tissues and organs, they participate in numerous physiological and pathological processes, serving as critical components for neuronal excitability and neural signal transmission. They have now emerged as potential therapeutic targets for treating multiple diseases, including tumors [130]. Dysfunction of voltage-gated ion channels frequently disrupts their function, leading to excessive activation of the nervous system and consequently causing persistent cancer pain.
3.2.1. Regulation of TRPV1
Somatic neurons involved in pain transmission reside in dorsal root ganglia (DRG), where TRPV1 is primarily expressed in nociceptors and sensory neurons. As a non-selective cation channel belonging to the transient receptor potential (TRP) family, TRPV1 functions as a nociceptor activated by noxious heat, protons, and capsaicin [131]. According to current research, TRPV1 plays a paradoxical role in the inflammatory process. Increased inflammatory mediators induce hyperalgesia to heat and abnormal mechanical pain while affecting TRPV1 [132]. Current research indicates that TRPV1 plays a paradoxical role in the inflammatory process. Elevated inflammatory mediators induce hyperalgesia and abnormal mechanical pain while simultaneously affecting TRPV1 [132]. Direct mechanisms include binding to the receptor to activate downstream kinases that phosphorylate TRPA1 or activating TRPA1 through the production of lipid mediators [133]. Consequently, persistent inflammation within the TME serves as a key driver for the generation and maintenance of TRPA1-dependent pain signaling. Furthermore, TRPA1 activation induces neuronal depolarization and promotes the release of pain-related signaling peptides like substance P and calcitonin gene-related peptide (CGRP). These substances not only transmit pain signals to the CNS but also exert paracrine effects on surrounding cells [134]. Research indicates that modulating the function of TRPA1 channels can prevent the onset of pain symptoms. For instance, opioids inhibit TRPV1-mediated signaling pathways, promote the nuclear translocation of β-inhibin 2, and exert analgesic effects [135]. The Peony and Licorice Decoction suppresses cancer pain by downregulating TRPV1 channels and reducing the expression levels of TNF-α and IL-1β [106]. Bulleyaconitine A inhibits TRPV1-mediated SNARE-dependent exocytosis on cell surfaces and reduces TRPV1 expression in peripheral nerve axons [109].
3.2.2. Regulation of Sodium Ion Channels
Pain signals are typically transmitted to the CNS via action potentials, whose rapid rise is mediated by voltage-gated sodium channels (VGSCs). Among the nine identified pore-forming α subunits (Nav1.1–1.9), the Nav1.7 and Nav1.8 subunits are key molecules involved in peripheral pain processing and increased pain sensitivity associated with inflammation and tissue injury [136]. Research indicates that, High concentrations of fluoxetine (SSRI) and venlafaxine (SNRI) in TCAs block Na^+^ channels, reducing abnormal neuronal discharge [96]. Anticonvulsants such as phenytoin, lamotrigine, carbamazepine, and oxcarbazepine also decrease ectopic nerve impulses by inhibiting Na^+^ channels. Local anesthetics block VGSCs to halt action potential conduction [99]. Lidocaine reduces the peak current of Na^+^ channels and accelerates the inactivation process, thereby decreasing neuronal excitability and preventing or alleviating pain perception [137]. Bulleyaconitine A can block VGSC-mediated ectopic discharges in neuropathic pain, exerting analgesic effects [110]. Compound Kushen injection alleviates cancer-related bone pain by reducing Nav1.7 expression in the spinal cord and DRG [107].
3.2.3. Regulation of Calcium Ion Channels
Voltage-gated calcium channels (VGCCs) play a pivotal role in pain signaling within the dorsal spinal cord. Calcium influx, primarily mediated by VGCCs in neuronal membranes, is crucial for pain signal transmission, with increased calcium currents enhancing excitability [138]. Research indicates that, gabapentin and pregabalin reduce α2-δ1 VGCC activity in the spinal cord and CNS [139]. They exert anti-hyperalgesic effects by binding to the Cavα2δ subunits of L-, N-, and P/Q-type VGCCs, thereby modulating presynaptic calcium influx and subsequent calcium-mediated glutamate release, which reduces neurotransmitters involved in pain processing [98]. Huachansu exerts analgesic effects by modulating L-VGCC current properties in rat DRG cells [128].
3.3. Regulation of Neurotransmitters
The importance of neurotransmitters in cancer pain is a complex field of research, playing a crucial role in regulating pain pathways. Various neurotransmitters, including 5-HT, dopamine, and glutamate, are implicated in modulating pain perception and the development of cancer-related pain syndromes (Figure 3).
3.3.1. Regulation of NMDA Receptors
Glutamate is the primary excitatory neurotransmitter in the CNS. Research indicates that elevated glutamate levels in the TME sensitize pain pathways, contributing to cancer-associated chronic pain conditions [140]. The NMDA receptor, a glutamate receptor, serves as the primary excitatory neurotransmitter in the human brain. Extensive research indicates that activation of NMDA receptors in the CNS plays a crucial role in the generation and maintenance of neuropathic pain, effectively alleviating pain. When tumor-related peripheral signals persistently input, synaptic efficacy in spinal dorsal horn neurons increases, sensitivity in superficial dorsal horn neurons rises, and the ratio between nociception-specific neurons and wide dynamic range (WDR) neurons shifts. This activates NMDA receptors, prolonging response time by 4–5 times [141]. It is evident that modulating NMDA receptors can alleviate pain. For example, Ketamine, as a non-competitive NMDA receptor antagonist, possesses the ability to block NMDA receptors. It reduces pain impulse transmission by decreasing central neuronal excitability, inhibits glial cell activation, and reduces neuroinflammation [94]. Opioid use alters neurotransmitter release, which helps alleviate cancer pain [129].
3.3.2. Regulation of 5-HT and NE
5-HT is a monoamine widely distributed throughout the nervous system. As a neurotransmitter, it participates in pain regulation and can influence the efficacy of analgesics. Upon peripheral tissue injury or inflammation, platelets and mast cells release 5-HT, which can either alleviate or exacerbate pain [142]. 5-HT release activates 5-HT_3_R, inducing descending facilitation in the rostral ventromedial nucleus (RVM) of the medulla, thereby transmitting nociceptive stimuli and promoting central sensitization and the formation of nociceptive stimuli [143]. Upregulation of 5-HT input into RVM maintains TRPV1 sensitization [144], leading to mechanical hypersensitivity. The interaction between 5-HT and norepinephrine (NE) further complicates cancer pain. NE may be involved in the intrinsic control of pain, with its main sources being the peripheral sympathetic nerves and the central NE brainstem nuclei A1-A7. In the spinal cord, NE released from descending pathways inhibits pain by suppressing α-2A adrenergic receptors at the central terminals of primary afferent nociceptors (presynaptic inhibition), directly acting on pain-transmitting neurons via α-2 adrenergic effects (postsynaptic inhibition), and activating inhibitory interneurons mediated by α-1 adrenergic receptors [145].
Research indicates that TCAs block presynaptic reuptake of 5-HT and NE, activating descending inhibitory pathways from the brainstem to the spinal dorsal horn to suppress pain signal transmission [95]. α-2 adrenergic agonists stimulate brainstem regions, enhance downward inhibitory pathways, inhibit the transmission of injurious signals by WDR neurons in the posterior horn of the spinal cord, promote endorphin release, inhibit substance P release, activate the 5-HT pathway, and promote the release of enkephalins, which directly inhibit pain signaling [97]. Opioids inhibit pain signal transmission by activating central and peripheral μ, κ, and δ receptors, suppressing substance P and glutamate release from primary afferent neurons in the dorsal spinal horn, reducing postsynaptic neuronal excitation, activating the periaqueductal gray (PAG) and RVM, promoting 5-HT and NE release, and inhibiting ascending pain signals [90]. Ketamine interrupts cholinergic transmission and inhibits 5-HT and NE uptake, exerting an analgesic effect [15]. Aconitine tablets activate descending pain inhibitory systems via 5-HT and NE. They also stimulate the release of enkephalins from spinal dorsal horn microglia through the Gs/cAMP/PKA/p28β/CREB signaling pathway. These enkephalins act on k-opioid receptors on postsynaptic membrane neurons to produce analgesic effects [146]. It is evident that inhibiting 5-HT and NE can significantly improve cancer pain.
3.4. Inhibition of Glial Cell Activation
The TME releases a large number of molecular signals that directly activate glial cells. Activated glial cells enhance nociception by releasing inflammatory mediators, which can either directly increase neuronal excitability or structurally alter pain transmission pathways (Figure 4).
Among these, microglia serve as crucial immune and defense cells within the nervous system. When tumor-associated biomolecules cause neuronal damage or inflammation, and microglia become activated, they release large quantities of neuroactive and inflammatory mediators. These substances include ROS, IL-1β, IL-6, TNF-α, MMPs, chemokines, ATP, and NO. On one hand, these active substances act on corresponding receptors on neurons, causing pain. On the other hand, they activate more microglia and astrocytes, creating a positive feedback loop and ultimately participating in the induction and maintenance of chronic pain [148]. By upregulating surface C-X chemokine receptors (CXCRs) such as CXCR3 and CXCR4, which mediate signaling between neurons and microglia via chemokines secreted by spinal neurons, the excitability and sensitivity of sensory neurons are enhanced [149]. This leads to the continuous synthesis of nociceptive proteins, maintaining the pain perception of nociceptors and sustaining cancer pain [150]. In BCP models, tumor-mediated bone destruction generates lactic acid, PGE2, extracellular ATP, and high-mobility group box 1 (HMGB1), which stimulate purinergic receptors (purinergic receptor p2x ligand-gated ion channel 4/purinergic receptor p2x ligand-gated ion channel 7, P2X4/P2X7) and Toll-like receptor 4 (TLR4) in microglia, inducing a proinflammatory M1 phenotype [151].
Astrocytes are the most abundant cells in the CNS. Their structure is closely associated with synaptic architecture, facilitating the formation of neuronal circuits and maintaining synaptic integrity [152]. Activation of astrocytes releases various inflammatory cytokines, inducing peripheral and central sensitization, thereby contributing to cancer pain. In the BCP model, neuronal chemokines (C-X3-C motif chemokine ligand 1, CX3CL1) or IL-1β and TNF-α activate astrocytes, leading to increased glial fibrillary acidic protein (GFAP) expression and cellular hypertrophy. Additionally, astrocytes participate in crosstalk with neurons by releasing Chemokine C-X-C Ligand 1 (CXCL1) and Chemokine C-X-C Ligand 12 (CXCL12), which act on the CXCR2 and CXCR4 receptors on neurons, respectively.
Research has found that the analgesic effect of morphine is associated with a reduction in pro-inflammatory factors such as IL-1β and TNF-α secreted by M1 microglia, along with an increase in the secretion of anti-inflammatory factors like IL-10 and TGF-β, thereby promoting the transition of M1 microglia to the M2 phenotype [91]. Hydrocodone maintains long-lasting and potent analgesic effects by inhibiting the activation of astrocytes and microglia in the spinal cord [153]. Huachansu alleviates pain by reducing inflammatory responses through suppression of astrocyte and microglial activation [104]. Peony and Licorice Decoction alleviates neuropathic pain by regulating the interaction between microglia and astrocytes via the HSP90AA1/HMGB1 pathway [154]. Thus, inhibiting glial cell activation significantly alleviates pain.
3.5. Inhibition of Osteoclast Activation
Osteoclasts are the only cells in the body capable of bone resorption. They degrade bone matrix by secreting acidic substances and proteases, thereby maintaining bone metabolic balance. When tumors metastasize to bone, osteoclast stimulatory factors secreted by the bone microenvironment—such as parathyroid hormone-related protein (PTHrP), TNF-α, IL-1β, IL-6, etc.—stimulate the synthesis of receptor activator of NF-κB ligand (RANKL). RANKL competitively binds to osteoprotegerin (OPG), activating the RANKL/RANK pathway to induce osteoclast differentiation and maturation, leading to bone destruction [155]. Under the influence of bone tumors, osteoblasts can induce inflammatory responses, thereby reducing OPG levels and enhancing osteoclast secretion of acidic substances and bone-dissolving enzymes. When the OPG/RANKL/RANK system is activated, osteoclasts significantly intensify their osteolytic destruction of the bone matrix, leading to the development of BCP. Bone-tissue immune cells within the bone microenvironment of metastatic tumors—such as monocytes, macrophages, dendritic cells (DCs), and myeloid-derived suppressor cells—can also differentiate into osteoclasts [156]. Upon activation, osteoclasts increase bone resorption, releasing large amounts of H^+^ that acidify the bone microenvironment, sensitizing and activating nociceptors in sensory neurons. When osteoclasts become excessively activated, spinal neurons become abnormally activated, and the inflammatory factors they secrete further exacerbate pain and bone destruction. Therefore, inhibiting osteoclast activation is an effective means of alleviating cancer pain.
In pharmacological treatment, bisphosphonates bind to calcium in bones, forming insoluble calcium salt precipitates that inhibit osteoclast activity. This reduces acid-induced activation of primary afferent nociceptors and suppresses phenyldiphasic phosphodiesterase synthase (FPPS), exerting anti-inflammatory and analgesic effects [101]. Quercetin in Peony and Licorice Decoction inhibits osteoclast activation and reduces pain by modulating the RANKL/RANK/OPG signaling pathway and inflammatory responses [105]. Huachansu alleviates bone metastatic cancer pain by inhibiting osteoclast formation through regulating the OPG/RANK/RANKL pathway [103]. Bulleyaconitine A inhibits osteoclast differentiation and mediates bone resorption by downregulating the transcription of osteoclast activation T cell nuclear factor 1 (NFATc1) during the differentiation of BMMs, exerting analgesic effects [108]. Yishen Gukang Formula inhibits osteoclast activation by regulating the OPG/RANK/RANKL pathway, thereby suppressing bone destruction in rats with osteosarcoma-induced pain and alleviating pain symptoms [111].
4. Application of Drug Delivery Systems in Cancer Pain Management
The complexity of cancer pain management stems from its diverse pathological mechanisms, varied sites of occurrence, and distinct drug targets. Traditional administration methods often result in inadequate analgesia, significant side effects, and poor patient compliance due to pharmacokinetic fluctuations, systemic exposure, and delayed effects. To overcome these limitations, DDS have emerged. By developing controlled-release formulations to achieve steady-state plasma concentrations, designing mucosal and transdermal delivery systems to enhance convenience and onset speed, and innovating intrathecal delivery pathways for central-targeted analgesia, these precise, controllable delivery strategies are driving cancer pain management from traditional models toward personalized, high-efficacy treatment paradigms. See Table 4 and Figure 5 for details.
4.1. Oral Controlled-Release Drug Delivery Systems
Cancer pain, as a persistent complication throughout cancer treatment, requires long-term, controllable therapeutic approaches. While conventional oral formulations offer rapid onset of action, they present issues such as significant fluctuations in blood drug concentrations and the need for frequent dosing. Oral sustained-release formulations achieve therapeutic effects by prolonging drug release, reducing dosing frequency, and maintaining stable plasma concentrations [157]. However, release rates are susceptible to gastrointestinal conditions and carry risks of interindividual variability. Oral controlled-release formulations further optimize this system by maintaining drug concentrations within the therapeutic window, offering the advantage of prolonged release while reducing dosage and improving patient compliance [158]. Clinically available oral sustained- and controlled-release formulations include tramadol sustained-release tablets, morphine sustained- and controlled-release tablets, and oxycodone sustained-release tablets.
In 1977, Germany’s Grünenthal GmbH Pharmaceutical Co., Ltd. first introduced tramadol hydrochloride sustained-release tablets (Trama^®^) [159]. Following a 100 mg dose, peak plasma concentration (C_max_) of 141 ± 40 ng/mL was reached after 4.9 h; after a 200 mg dose, C_max_ of 260 ± 62 ng/mL was achieved after 4.8 h. As a weak opioid analgesic, the introduction of tramadol sustained-release formulations extended the drug’s duration of action, demonstrating good efficacy in treating moderate to severe cancer pain. However, its relatively low peak concentration may also imply insufficient control for breakthrough pain. To improve the pharmacokinetic profile of oral tramadol, Nippon Zoki developed a novel formulation: a dual-layer sustained-release (SR) tablet. The upper layer delivers 35% of the immediate-release (IR) dose, while the lower layer provides 65%. As an SR formulation, it is administered twice daily (Twotram^®^ tablets; Nippon Zoki Pharmaceutical Co., Ltd.). To date, Phase III clinical studies have demonstrated the efficacy of the dual-layer tramadol tablet in treating cancer pain; however, current research limitations prevent assessment of tramadol’s long-term effectiveness [160].
On 18 September 1984, USA’s Hikma Pharmaceuticals Co., Ltd. first marketed morphine sulfate sustained-release tablets (MS Contin^®^) [161] utilizing the fully dispersed permeation dissolution sustained-release technology prevalent in the 1980s. In 1988, China Southwest Pharmaceutical Co., Ltd. developed China’s first 24-h long-acting analgesic, Tramadol Hydrochloride Sustained Release Tablets (II), by adopting the skeleton-film dual-controlled-release system, and in 1994, the company developed Morphine Hydrochloride Sustained-release Tablets by adopting the new technology of solid-dispersed fusion granulation, which could realize 12-h sustained analgesia through the principle of skeleton sustained-release [162]. Morphine sulfate extended-release tablets utilize salts with sulfate anions, while morphine hydrochloride extended-release tablets employ salts with hydrochloride anions. Compared to sulfate salts, hydrochloride salts exhibit faster dissolution rates. Compared to conventional morphine tablets, morphine sustained-release tablets typically reach peak plasma concentrations 2–3 h post-administration with slightly lower peak levels. Steady-state plasma concentrations exhibit minimal fluctuation, making both formulations suitable for managing severe cancer pain. In 1995, USA’s Purdue Pharmaceuticals Co., Ltd. first launched the extended-release hydrocodone bitartrate tablet (OxyContin^®^) [163], which provides sustained release for 12 h. It has an oral bioavailability of 6087%, is well absorbed, and reaches steady-state plasma concentrations within 2436 h. It is indicated for the relief of persistent moderate to severe cancer pain. However, it was precisely its highly efficient controlled-release technology and potent analgesic effects that laid the groundwork for the severe abuse and addiction crisis it would later trigger in the United States and other regions.
In 2000, the USA FDA approved controlled-release morphine sulfate tablets (Avinza^®^). Based on slow release, they maintain stable blood concentrations and reduce gastrointestinal irritation. Twice-daily dosing provided excellent pain control with minimal need for rescue medication [164]. This formulation enabled a reduction of over 20% in daily morphine dosage for advanced cancer patients. Most patients reported that controlled-release formulations offered superior convenience and adequacy of relief compared to standard oral morphine tablets [165]. They provide more sustained and stable analgesic effects, allowing adjustment of release rates and doses to individual patient needs. This approach reduced the risk of addiction and enabled personalized treatment regimens.
4.2. Mucosal Drug Delivery System
MDDS is a novel drug delivery system that primarily involves applying drugs with suitable carrier materials to mucosal surfaces to achieve localized effects or systemic absorption into the bloodstream for systemic therapeutic action [166]. Mucosal tissues possess a rich network of capillaries and lymphatic vessels. Certain mucosal sites, such as the nasal cavity and oral cavity, can bypass the first-pass effect, enhancing drug bioavailability. Furthermore, the limited variety and quantity of enzymes within mucosal tissues result in relatively low enzymatic degradation of drugs. Local administration thus improves bioavailability and patient compliance [167].
4.2.1. Oral Mucosal Drug Delivery
Oral mucosal DDS refer to a method where drugs are absorbed through the oral mucosa and enter the systemic circulation to exert their therapeutic effects. Compared to traditional oral administration, the oral mucosal delivery system allows drugs of specific molecular sizes to pass through the oral mucosa, directly entering the jugular vein via oral veins before entering systemic circulation. This bypasses degradation by gastrointestinal pH and enzyme systems and avoids hepatic first-pass metabolism, significantly enhancing drug bioavailability [168]. Clinically available formulations for oral mucosal administration include fentanyl sublingual tablets, orally disintegrating films, and sublingual sprays.
Fentanyl (SFC), a highly lipophilic opioid, exhibits rapid mucosal absorption with high bioavailability. The sublingual tablet and orally disintegrating film developed by Cephalon Co., Ltd., received FDA approval in 1997 and 2006, respectively. The fentanyl sublingual tablet is particularly indicated for BTP. Jordi [169] treated 127 elderly BtCP cancer patients with sublingual fentanyl, which significantly reduced VAS scores at 30 min after administration, with effectiveness in terms of overall and maximal pain relief of 34.7% and 30.6%, respectively. Fentanyl Buccal Soluble Film (FBSF) consists of a double-layer polymer membrane comprising an adhesive layer containing fentanyl and an inactive layer that prevents the diffusion of fentanyl. The adhesive layer can adhere to moist mucosal surfaces within seconds. When placed in the oral cavity, the drug is absorbed through the oral mucosa into the bloodstream, representing a novel delivery form for rapid relief of BtCP [170]. Yi-Hao Chiang [171] conducted a 14-day observation using FBSF. Among 63 BtCP episodes, 47.6%, 73.0%, 84.1%, and 92.0% of BtCP episodes showed significant relief within 5, 10, 15, and 30 min after FBSF administration, respectively. with BtCP intensity reduced by 37.8%, 47.6%, 73.0%, and 84.1%, respectively, and pain scores decreased by 2.3 points, 3.3 points, 4.1 points, and 4.9 points, respectively, demonstrating rapid and effective reduction in BtCP pain intensity. Fentanyl sublingual spray (Subsys^®^), marketed in the United States in 2012 for improving the rate and extent of fentanyl absorption through the sublingual mucosa [172], provides rapid pain relief for opioid-tolerant cancer patients and helps with acute or postoperative pain relief [173]. It reduces pain intensity within 4 min after administration and lasts up to 60 min, with significant efficacy in BtCP treatment [174].
4.2.2. Nasal Mucosal Drug Delivery
Nasal mucosal drug delivery refers to a noninvasive drug delivery method where medications are absorbed through the nasal mucosa, characterized by rapid absorption, fast onset of action, and high drug concentration, enabling both local and systemic therapeutic effects [175]. Opioid drugs administered nasally exert rapid effects on the CNS, providing swift analgesia. Fentanyl nasal spray (Instanyl^®^), developed by Nycomed in 2009 and approved by the European Medicines Agency, is indicated for BTP [176]. The nasal spray delivery device atomizes fentanyl into a fine mist that forms a gel on the mucosa, allowing the active ingredient to be absorbed through the mucosa into the bloodstream. Compared to oral morphine or oral fentanyl formulations, it provides more effective pain relief lasting 15~45 min [177]. Plasma concentrations are significantly higher than with oral mucosal administration, achieving a bioavailability of up to 89%, with analgesic effects occurring within approximately 5 min [178]. Not only does it provide rapid analgesic effects, but it also avoids the gastrointestinal side effects associated with oral administration, making it another effective option for treating BTP.
4.3. Transdermal Drug Delivery System
TDDS represents an innovative drug delivery method that administers medications at a constant rate through the skin into the systemic circulation, enabling targeted effects for local or systemic therapy. This approach offers advantages such as circumventing the first-pass effect of oral medications, enhancing and sustaining blood drug concentrations, preserving drug potency, and improving patient compliance [179]. Therapeutic agents accumulate in specific skin layers where they permeate and enter the bloodstream during absorption. Compared to traditional systems, this approach permits the storage of small quantities of nanotechnology-developed drugs within transport and delivery structures [20].
Transdermal patches (Figure 6) serve as the preferred treatment for patients unable to swallow or those with poor tolerance or compliance to oral medications. They offer advantages including avoidance of hepatic first-pass metabolism, bypassing gastrointestinal metabolism, prolonged duration of action, and stable blood drug concentrations [180]. In the field of cancer pain management, transdermal patches containing opioids (such as fentanyl, buprenorphine, diclofenac sodium, lidocaine, and clonidine) represent the most clinically mature and widely adopted technology.
As early as 1984, the Clonidine adhesive patch (Catapres-TTS^®^) was first launched in the United States. A randomized controlled trial confirmed its analgesic efficacy for cancer pain, though it is more suitable for specific patient populations [181]. Fentanyl-based drugs exhibit excellent membrane permeability due to their low molecular weight and high lipophilicity. In 1990, the U.S. FDA first approved the fentanyl transdermal patch (Duragesic^®^), with current technologies including reservoir-type and matrix-type formulations [182]. Yong Liu [183] treated 267 patients with moderate-to-severe cancer pain using a low-dose fentanyl transdermal patch (TDF) at 12.5 μg/h. The mean effective therapeutic dose was 6.3 ± 6.08 mg, achieving a total pain relief rate of 98.12% with mild adverse reactions. Shigeki Yamaguchi [184] found TDF achieved an 87.0% efficacy rate in opioid-naive cancer pain patients, with a mean VAS pain score change of −34.5 mm and no serious respiratory depression events.
The 5% lidocaine transdermal patch (Lidoderm^®^), developed and manufactured by the US subsidiary of Japan’s Imperial Pharmaceutical Co., Ltd. was launched in the U S in March 1999 for use in various forms of local anesthetic pain relief [185,186]. Jui-Hung Tsai [187] applied it to 96 advanced cancer patients already receiving opioid therapy. On the first and second days, 51 patients experienced reduced NRS pain intensity, indicating its efficacy in alleviating cancer-related local and superficial neuropathic pain. In 2005, China’s Bengbu Fengyuan Tushan Pharmaceutical Co., Ltd. launched a patch containing 50 mg of sodium diclofenac (Laixin^®^) for local pain relief [188] However, cancer pain management requires stable blood concentrations and systemic effects.
In 2006, Luye Pharma’s German subsidiary first launched the transdermal transect patch (Transtec^®^). As a potent opioid analgesic, it prolongs analgesic effects by activating μ-opioid receptors, with sustained release lasting up to 7 days. It is excreted via feces and exhibits no dose-dependent upper limit for analgesic efficacy, though respiratory depression has an upper limit. Its clinical use remains relatively limited.
4.4. Intrathecal Targeted Drug Delivery
ITDS proves effective for various neuropathic, nociceptive, and mixed pain conditions in cancer patients. By injecting analgesic drugs into the subarachnoid space via microcatheters, the cerebrospinal fluid circulation enables direct action of the medication on the CNS, treating chronic cancer pain and refractory cancer pain [189]. Compared to conventional administration methods, ITDD has been demonstrated to be superior to comprehensive medical management in pain control and reducing drug-related toxicity [190]. Intrathecal drug delivery system (IDDS) was employed as early as the 1980s for refractory pain management. Commonly used delivery devices include semi-implantable and fully implantable systems. Semi-implantable systems feature a catheter connected to an infusion port, with medication delivery controlled via a dedicated external medication reservoir and a patient-controlled analgesia (PCA) pump. Fully implantable systems connect catheters to programmable implantable pumps. The entire system is buried subcutaneously, with medication stored in the subcutaneous pump. Infusion parameters can be remotely adjusted via a programmer, making it the most rigorously tested and widely used implantable programmable device globally to date (Figure 7) [191].
Depending on the location and extent of the patient’s pain, the IDDS catheter can be placed within the spinal canal, the greater occipital cistern, or even the ventricles. Positioning the tip of the intrathecal morphine pump catheter in the anterior pontine cistern effectively relieves refractory head and facial cancer pain with extremely low morphine doses [192], reducing opioid usage in patients with refractory cancer pain [193]. Placing medication within the subarachnoid space allows for delivery near the trigeminal nerve, treating craniofacial cancer pain while reducing opioid intake and alleviating side effects [194].
Clinically, pain management often involves combining different medications such as morphine, hydromorphone, ropivacaine, fentanyl, and dexmedetomidine based on the patient’s analgesic goals. Among these, morphine is the preferred opioid for chronic pain IDDS. Its high hydrophilicity, slow onset, and prolonged duration of action allow it to diffuse more rapidly than other opioids after injection, providing broader analgesic coverage. It was the earliest IDDS drug clinically used for cancer pain management. Typically, 1 mg of morphine via IDDS is equivalent to 10 mg epidural, 100 mg intravenous, or 300 mg oral administration. Furthermore, different combination therapies can reduce morphine dosage while enhancing analgesic efficacy [195].
5. The Development Prospects of Drug Delivery Systems in Cancer Pain Management
5.1. Transdermal Drug Delivery System
5.1.1. New Transdermal Patch
Traditional transdermal patch delivery is limited by the barrier function of the skin’s stratum corneum, resulting in low transdermal absorption efficiency [196]. In the development of novel transdermal patches, research focuses on optimizing drug release and enhancing transdermal efficiency.
For example, in 2020, Chen Shen [197] developed a 5% lidocaine gel patch by uniformly mixing lidocaine with a hydrophilic polymer gel matrix and coating it onto a backing material. This formulation offers advantages including ease of use, rapid onset of action, and high safety.
In 2021, Japan’s Hisamitsu Pharmaceutical Co., Ltd. launched a novel diclofenac sodium patch (Zicthoru Tapes^®^) containing 75 mg of active ingredient, delivering systemic analgesia upon application [198]. In a phase III multicenter, randomized, double-blind, placebo-controlled comparative study, once-daily diclofenac sodium patches were initiated at 150 mg/day (2 patches) and could be increased to 225 mg/day (3 patches). At steady state, repeated administration of 225 mg yielded C_max_ and AUC values of 294.16 ng/mL and 3052.2 ng·h/mL, respectively, representing 76% of the relative bioavailability of oral diclofenac sodium 100 mg/day. This demonstrates sustained efficacy of the novel diclofenac sodium patch in cancer pain management. All adverse events were consistent with those observed with existing diclofenac sodium formulations during cancer treatment [199].
In 2024, Sourav Adhikary [200] developed a novel clonidine hydrochloride/montmorillonite sodium (CH/Na-MMT) composite patch. Na-MMT enables sustained drug release over four weeks, with clonidine achieving 82% release at pH 7.4. In rats, it demonstrated sustained analgesia. The CH/Na-MMT patch effectively penetrated skin, reaching effective blood concentrations of 100 mg/kg. Drug loading efficiency was 84.98 ± 0.31%, loading capacity was 6.78 ± 0.17%, and transdermal flux (Jss) was 0.76 ± 0.11 μg/cm^2^·h. CH/Na-MMT prolongs drug release duration, showing promise for cancer pain management by reducing dosing frequency, enhancing therapeutic efficacy, and improving patient compliance.
5.1.2. Microneedle
As a third-generation transdermal delivery system, microneedles (MNs) utilize micron-sized needles to penetrate the skin’s stratum corneum, creating microchannels that allow analgesic drugs to directly enter the epidermis or dermis. This bypasses the barrier function of the stratum corneum, delivering drugs directly to pain sites such as tumor peripheries or areas of nerve compression. By establishing high local drug concentrations, MNs achieve more effective analgesia [201]. Since the drug acts directly at the local site, it reduces systemic distribution, avoids first-pass hepatic metabolism and gastrointestinal side effects, and improves drug utilization.
For example, Mingshan Li [202] prepared diclofenac sodium (DCF) NPs with an average diameter of 202.63 ± 2.02 nm via wet milling. These were stabilized using polyvinyl alcohol (PVA) and polyvinylpyrrolidone (PVP) (35% w/w, PVA: PVP = 1:2) to stabilize the suspension. The nanoparticle suspension was then freeze-dried to ensure nanoparticle stability and high drug loading capacity. The MN patches were produced using a mold-casting method (Figure 8). Skin penetration capabilities of different MNs were validated through mechanical strength testing (compression experiments) and in vitro insertion experiments (Parafilm^®^ model). Results showed that the 600-needle array with longer needles achieved a drug loading capacity of 2.33 mg, demonstrated superior skin insertion depth, and significantly increased drug deposition. Finally, combined in vivo and in vitro evaluations demonstrated that DCF-NPs MNs exhibited a significantly longer in vivo half-life (T_1_/2 = 8.7 h) compared to oral administration (T_1_/2 = 1.9 h) with drug delivery efficiency (34%) superior to that of conventional transdermal DCF gel (6%). The current study showed that a single application of DCF-NP MNs could provide up to 48 h of systemic delivery and up to 72 h of localized and targeted drug concentrations. This fully demonstrates the tremendous potential of MNs, particularly those incorporating nanotechnology, in enhancing transdermal drug delivery efficiency and prolonging therapeutic duration.
Additionally, Ze Qiang Zhao [203] designed a hydrogel microneedle (MN) system made of gelatin-methacrylate (GelMA) for sustained delivery of lidocaine hydrochloride (LiH). The use of a backing layer reservoir significantly enhanced the drug loading capacity of GelMA MNs, increasing it substantially from 50–300 μg to 2927.168 ± 174.408 μg. In vivo and in vitro drug release experiments compared LiH/GelMA MNs with commercial LiH patches, demonstrating that MNs substantially enhanced drug absorption rates. Additionally, a rat SNI model was established to assess behavioral pain sensitivity to mechanical stimulation. Twenty-four hours post-treatment, rats exhibited a more than threefold increase in mechanical pain threshold compared to controls, indicating the excellent sustained analgesic efficacy of LiH/GelMA MNs. Furthermore, biosafety assessments in rats revealed that the MNs’ application site returned to normal appearance within hours post-treatment, with no dermatological side effects or behavioral abnormalities observed throughout the study. The findings demonstrate that MNs not only enhance the transdermal absorption efficiency of lidocaine but also enable sustained analgesia with high lidocaine loading, offering a convenient, safe, and effective novel approach for treating localized chronic pain.
5.2. Disposable Intrathecal Drug Delivery
Given the multifaceted mechanisms underlying cancer pain, there has been a surge in the development of intrathecal targeted drugs addressing multiple levels, including pain-related receptors, associated enzyme activities, chemokines in pain transmission, protein-coding genes, and targeted natural small molecules.
5.2.1. Targeting Relevant Receptors
These substances directly bind to specific receptors on cell membranes or nuclei, thereby activating or deactivating downstream signaling pathways to alleviate cancer pain. For example, the neuromediator U receptor 2 (NMUR2) is widely distributed throughout the CNS, with the highest concentrations in the cerebral cortex and hypothalamus, playing a crucial role in nociception and inflammation [204]. Intrathecal injection of si-NMUR2 significantly reduces the expression level of the target NMUR2, participating in pain regulation through the PKC/ERK and PI3K/AKT signaling pathways [205]. Peroxisome proliferator-activated receptor gamma (PPAR-γ) is a key receptor involved in regulating nuclear factor kappa-B (NFκB) [206]. Intrathecal injection of rosiglitazone (a PPAR-γ agonist) and GW9662 (a PPAR-γ antagonist) activates PPAR-γ to inhibit the NF-κB/NLRP3 inflammatory axis in spinal neurons, thereby alleviating cancer bone pain [207].
5.2.2. Targeted Enzymes
These agents modulate intracellular biochemical reactions and signaling pathways by enhancing or inhibiting specific enzyme activities, thereby alleviating cancer pain. For instance, histone deacetylases (HDACs) play a crucial role in regulating glial cell-mediated immune responses; suppressing HDAC expression in the spinal cord alleviates BCP. Intrathecal injection of the HDAC inhibitor SAHA suppresses HDAC and GSK3β activity, thereby alleviating BCP [208]. SIRT1, an NAD+-dependent HDAC, has been reported to play a key role in BCP and is important in neuropathic pain by regulating inflammatory responses, oxidative stress, the immune system, and epigenetic modifications [209]. Intrathecal injection of the SIRT1 activator SRT1720 suppresses mGluR1/5 expression and activates SIRT1 [210], thereby alleviating BCP via the CREB/CRTC1 signaling pathway [211].
5.2.3. Targeted Chemokines
These substances precisely regulate the migration and localization of immune cells within the body, representing a hotspot in immunology and cancer research. Monocyte chemotactic protein-1 (formerly MCP-1, now designated CCL2) and its primary receptor, C-C motif chemokine receptor 2 (CCR2), constitute one of the most characteristic neuroactive chemokine pairs regulating nociception. They have been demonstrated to play critical roles in nociceptive processing under chronic pain conditions, mediating neuroinflammation, neuron-glia interactions, and enhancing synaptic transmission in the dorsal spinal cord horn [212]. Intrathecal injection of the CCR2-selective agonist PP101 reduces T-cell infiltration and neuronal activation in DRG, effectively alleviating neuropathic pain and BCP by inhibiting the CCL2/CCR2 signaling pathway [213]. The chemokine C-X-C motif ligand 12 (CXCL12), belonging to the C-X-C subfamily, exerts its effects by binding its specific receptor, C-X-C motif receptor 4 (CXCR4) [214]. Increased expression of the CXCR4 signaling pathway in spinal neurons activates the RhoA/ROCK2 signaling pathway, promoting pain hypersensitivity. Intrathecal injection of the CXCR4 inhibitor Plerixafor (AMD3100) and the ROCK2 inhibitor Fasudil blocks the CXCR4-RhoA/ROCK2 pathway [215].
5.2.4. Targeted Protein-Coding Genes
MicroRNAs (miRNAs) play a crucial role in regulating the expression of pain-related mRNAs and proteins. Pain can induce the upregulation or downregulation of multiple miRNAs, participating in the regulatory mechanisms of chronic pain and the acute nociception process [216]. Among these, miR-195 is a key member of the microRNA-15/16/195/424/497 family [217]. Intrathecal injection of a miR-195 inhibitor reduces miR-195 expression while elevating MPT and cold stimulus thresholds, increasing expression of autophagy-related proteins in mice, suppressing neuroinflammation, and alleviating neuropathic pain [218]. In recent years, bone marrow-derived mesenchymal stem cells (BMSCs) have emerged as a promising cell therapy due to their well-established properties, including differentiation into neural cells, migration to injury sites, and immunosuppressive functions [219]. Studies indicate that genetically modified BMSCs significantly suppress pain perception [220]. Molecular alterations induced by miR-9-5p overexpression confer potent analgesic properties to BMSCs. Thus, intrathecal injection of miR-9-5p-modified mouse BMSCs modulates MOR expression by targeting REST, thereby suppressing inflammatory responses and alleviating BCP [221]. Additionally, intrathecal injection of miR-199a-3p agomir directly targets DNMT3A to influence Nrf2 expression, thereby exerting therapeutic effects against BCP [222].
5.2.5. Targeted Natural Small Molecules
Liquiritin, derived from the TCM licorice, exhibits broad-spectrum effects unlike synthetic drugs with single targets. It exerts anti-inflammatory and antioxidant actions through multiple pathways, reflecting the multi-target synergistic characteristics of natural products. Intrathecal injection of different doses of glycyrrhizin effectively suppressed activation of the CXCL1/CXCR2 signaling pathway and production of IL-1β and IL-17 in BCP rats. It also inhibited activation of CXCL1 in spinal astrocytes and CXCR2p in neurons, alleviating BCP in rats [223].
5.3. Nanodrug Delivery Systems
NDDS utilizes nanomaterials to encapsulate drugs and deliver them to target sites, enabling precise targeting and controlled release. This approach enhances local drug concentration, reduces systemic side effects, prolongs sustained drug release [224], and mitigates adverse reactions caused by analgesics [225]. Compared to existing clinical pain medications, it achieves more sensitive and targeted treatment with fewer side effects [226]. Although no related drugs have been marketed, nanomedicine delivery systems such as liposomal NPs, polymeric NPs, magnetic NPs, co-delivery NPs, and carrier-free self-assembled NPs offer novel management approaches for cancer pain treatment. Specific details are provided in Table 5.
5.3.1. Liposome Nanoparticles
Local anesthetics are widely used in the treatment of acute and chronic pain. However, their analgesic effects last only a few hours due to their short half-life, limiting their application in cancer pain management [236]. Nevertheless, encapsulating local anesthetics in lipid-based nanocarriers offers advantages such as slow release, prolonged duration of action, and low toxicity to the central nervous and cardiovascular systems [237]. Jiqian Zhang [227] prepared ropivacaine-loaded liposomes (Rop-DPRL) via the thin-film hydration method, achieving a cumulative release rate of 71.4% over 24 h. When administered via intraperitoneal injection concurrently with caloric restriction (CR), this formulation exhibited dual inhibition of STAT3 phosphorylation and reduced vascular endothelial growth factor A (VEGF-A) levels. Repeated administration of Rop-DPRL combined with CR effectively suppressed tumor-induced cancer pain in a mouse model with tumors implanted near the sciatic nerve, achieving rapid analgesia. Additionally, Bahrami MA [228] encapsulated citrate fentanyl within nanostructured lipid carriers and synthesized NPs via thermal homogenization, achieving an 82% encapsulation rate and enabling 72-h sustained release. Under identical conditions, the lipid nanocarriers reduced the required drug dose by 50% while providing analgesic effects, potentially lowering the risk of citrate fentanyl overdose. However, further work is needed to define the therapeutic margin of this drug.
5.3.2. Polymeric Nanoparticles
Nano-controlled release microspheres represent a specific structural and functional type within polymeric NPs. They enable precise regulation of drug release, enhance drug targeting, improve the permeability of hydrophobic drug molecules across cell membranes, enhance drug stability, and modify delivery routes [238]. Encapsulating drugs within microspheres prolongs therapeutic effects. By modulating analgesic release rates, therapeutic blood concentrations can be maintained within therapeutic ranges while reducing fluctuations. Yan Zhou [229] prepared morphine sulfate nano-controlled release microspheres via an emulsification-crosslinking method. At a crosslinker ratio of 8:1, the highest drug loading capacity and encapsulation efficiency were achieved, reaching 15.1% and 54.0%, respectively. with drug release rates of 74.6% and 99.8% at 4 h and 72 h, respectively. These microspheres demonstrated excellent in vitro drug release characteristics, reduced NE levels in the hypothalamus of viscerally painful mice, promoted 5-HT synthesis and secretion, effectively decreased CNS pain sensitivity, alleviated tumor-induced visceral pain, elevated pain thresholds, prolonged pain relief duration, and exhibited favorable safety profiles. Additionally, protease-activated receptor 2 (PAR2) is a G protein-coupled receptor (GPCR) mediating oral cancer pain. Divya Bhansali [230] developed a polymeric nanoparticle encapsulating the PAR2 inhibitor AZ3451, with encapsulation rates ranging from 95.8% to 99.6%, enabling sustained release over 24 h. These NPs simultaneously target endosomal signaling in the TME and neurons. These findings indicate that PAR2 on oral cancer cells and neurons participates in oral cancer pain. Compared to free drugs, NPs loaded with PAR2 antagonists provide higher analgesic effects and improved oral function.
5.3.3. Magnetic Nanoparticles
In recent years, magnetic NPs (MNPs) have emerged as a research hotspot in targeted pain relief due to their controllable magnetic responsiveness, high drug loading capacity, and biocompatibility [239]. However, most MNPs studies still rely on non-green synthesis processes, such as chemical reduction methods, which may pose biosafety risks [240]. Xiaoli Lv [231] pioneered the integration of green synthesis strategies with transdermal delivery systems for magnetic NPs (MNPs-TDDS), developing folic acid-targeted magnetic nanocomposites (catHEC·FA@SPIO) using aqueous coprecipitation and a biocompatible polymer coating (hydroxyethyl cellulose), demonstrating its significant advantages in nasopharyngeal cancer pain management through multidimensional clinical metrics. The study showed a cumulative release rate of 82.4 ± 3.1% at pH 5.5 over 72 h, exceeding traditional liposomes by 60%. At a magnetic field strength of 0.5 Tesla (T), the drug penetration depth in tumors was only 0.006 cm; however, at magnetic field strengths of 1.5 T and 2.5 T, the penetration depth increased to 0.071 cm and 0.192 cm, representing 11.8-fold and 32-fold enhancements, respectively. Furthermore, the average drug concentration within tumors significantly increased with magnetic field strength, indicating that high-intensity magnetic fields enhance drug accumulation and efficacy in deep-seated tumors. This not only offers a novel strategy for cancer pain management but also lays the foundation for the application of MNPs in chronic diseases.
5.3.4. Size-Tunable Nanoparticles
The absolute quantity and size of NPs significantly influence drug diffusion and retention properties within tumor tissues. These factors not only regulate drug distribution within tumors but are also directly correlated with local tumor ablation efficacy. Yu Tan [232] synthesized size-controlled HA-As_2_S_3_ NPs using sodium hyaluronate (HA) of varying molecular weights as a supramolecular scaffold. HA first coordinates with arsenic ions (As^3+^) to form HA-As^3+^ framework intermediates of varying sizes. These HA-As^3+^ intermediates subsequently reacted with sulfide ions to form size-controlled HA-As_2_S_3_ particles (HA-As_2_S_3_ NPs). This approach enables precise control over As_2_S_3_ particle size and provides a simple, environmentally friendly method for synthesizing size-controlled metal sulfide NPs. The synthesized HA-As_2_S_3_ NPs exhibited excellent stability. The combination of hydrogen sulfide (H_2_S) gas therapy and locally targeted interventional ablation may represent a promising approach for eradicating localized cancer pain. This study employed ultrasound-guided interventional therapy to directly inject HA-As_2_S_3_ NPs in situ into mouse tumors, ensuring precise nanoparticle delivery. This achieved safe tumor ablation and effective cancer pain relief. The released H_2_S gas and As^3+^ achieve targeted tumor cell treatment within the acidic TME, significantly enhancing mitochondrial damage and ROS accumulation. This effectively induces tumor cell apoptosis while markedly alleviating cancer pain, demonstrating favorable biosafety.
5.3.5. Co-Delivery Nanoparticles
The treatment of cancer pain requires multi-targeted interventions. Co-delivery NPs serve as nanoscale carriers capable of simultaneously loading and delivering two or more distinct therapeutic or diagnostic agents, achieving synergistic effects. Xu Chu [233] loaded the antagonist AZ-23 and the external modulator alendronate sodium (ALD) within a layered double hydroxide (LDH/AZ-ALD, abbreviated as LAD) nanoscale carrier. This Mg/Al layered double hydroxide nanoscale shell (Mg/Al-LDH) achieved neuro-antagonistic effects by simultaneously inhibiting the N-acetylaspartate (NAA) transporter and modulating the activity of the N-acetylaspartate receptor. AZ-23 and externally modifying Mg/Al layered double hydroxide nanocapsules (Mg/Al-LDH) with ALD achieved a neuro-cancer crosstalk blockade strategy for metastatic BCP. As anticipated, LAD precisely targeted bone cancer sites under ALD guidance. H^+^, the primary pain-inducing factor in BCP (pH ≈ 4.5). Concurrently, Mg^2+^’s role in promoting osteoblastic differentiation protects bone from further damage. Furthermore, AZ-23 released upon LDH degradation fundamentally inhibits cancer-induced neurogenesis by blocking the NGF/TrkA pathway, thereby preventing the development of hyperalgesia and allodynia. All these actions collectively reduce neuronal excitability and alleviate pain. As a positive feedback loop, decreased neuronal excitability directly diminishes neural influence on cancer progression. It significantly inhibits tumor growth through Ca^2+^-dependent cell cycle events, suppresses activation of TRPV1/ASIC channels in pain-sensing neurons, releases NGF/TrkA pathway antagonists, and blocks nerve hyperplasia and tumor proliferation, thereby treating bone metastatic cancer pain (Figure 9).
The development of co-delivery bionic nanotechnology provides insights and momentum for the modernization of TCM, offering new opportunities for cancer pain management [241]. Dian-Chao Cao [234] developed an oxygen-producing bionic nano-herbal delivery system named (Q+M/MnOx)@Clip. This system fuses membranes from TNBC 4T1 cells targeted for tumor delivery with liposome membranes, synthesizing natural melanin—which induces immunogenic cell death (ICD)—via one-step biomineralization with potassium permanganate to produce melanin/MnOx (M/MnOx) hybrids. Quercetin (Q), used for tumor suppression and pain relief, is encapsulated within the lipid bilayer of the nano-herbal delivery system, with M/MnOx integrated into its hydrophilic core. Following cancer cell recognition and internalization, the nanodelivery system interacts with endogenous H_2_O_2_/H^+^ to generate O_2_. This oxygen production induces internal pressure and oxidative stress, leading to disruption of the (Q+M/MnOx)@Clip nanocarrier’s biomimetic cancer cell membrane coating. This disruption facilitates subsequent release of MnOx and other therapeutic agents from the system. This process alleviates hypoxic and acidic conditions within the immunosuppressive TME and rapidly triggers the rupture of the nanosystem within cancer cells, ensuring efficient release of the loaded drugs (Figure 10). This innovative system adeptly performs CDT and triggers DC activation while enhancing the body’s immune system, ultimately leading to cancer cell death. Furthermore, the T1-weighted imaging capability of (Q+M/MnOx)@Clip facilitates innovative imaging-guided precision cancer therapy. The system also significantly reduces VEGF-A levels, paving the way for alleviating cancer-related pain.
5.3.6. Carrier-Free Self-Assembled Nanoparticles
The self-assembly of molecular components is emerging as a common strategy for designing and synthesizing nanomaterials in biomedical applications. Molecular synergy is becoming a key indicator in both natural and synthetic self-assembled nanostructures [242]. Pengfei Zhang [235] developed a nanomaterial-mediated microknife (NP-MK) ablation for interventional ablation therapy (IAT), aimed at locally eliminating cancer pain and tumors. The IAT system employs nanoprecipitation to self-assemble Paclitaxel (PTX) and Hematoporphyrin (HP) at a 4:1 mass ratio into a carrier-free nanomedicine (PTX-HP nanomedicine) with 63% drug loading. Combining PTX and HP via self-assembly addresses their poor water solubility and generates potent synergistic anticancer and analgesic effects. Combining infusion catheters, puncture needles, syringe pumps, and empirical tumor ablation formulations, the PTX-HP nanodrug is directly infused into tumors under imaging guidance via puncture needles and syringe pumps. Assisted by the targeting ligand HP, the NP-MK system eliminates localized cancer pain. Following IAT treatment, pain-related symptoms in mice completely resolved. Thus, NP-MK technology offers an alternative pathway for expanding the application scope of nanomedicines. By adopting approaches similar to the NP-MK system, various nanocarriers will flourish in the field of precise intra-tumoral therapy.
6. Discussion
Cancer pain is one of the most common and dreaded symptoms experienced by patients with malignant tumors, severely impacting their quality of life and adherence to anticancer treatments. Since the WHO introduced the “Three-Step Pain Management Guidelines for Cancer” in 1986, this protocol has become the cornerstone of global cancer pain management. However, its limitations have become apparent during long-term use, particularly the tolerance and addiction associated with opioid medications, along with a range of adverse effects such as constipation, nausea and vomiting, and respiratory depression, which limit its clinical utility [243].
Against this backdrop, the integrated Chinese and Western medicine approach to cancer pain management demonstrates immense potential and unique advantages. The combination of multiple Chinese herbal formulas and proprietary Chinese medicines with standard opioid medications can maintain or even enhance overall analgesic efficacy while significantly reducing the average daily opioid dosage, decreasing the frequency of breakthrough pain episodes, and alleviating adverse drug reactions such as dizziness, constipation, nausea, and vomiting. Furthermore, the integrated strategy—combining Western medicine’s blockade of core pain pathways with Chinese medicine’s regulation of the TME, suppression of neuroimmune inflammation, and restoration of bone homeostasis—provides the pharmacological basis for achieving “enhanced efficacy with reduced toxicity” in combined TCM-Western medicine treatment. However, many current clinical studies suffer from small sample sizes, inadequate research design rigor, and short follow-up periods, resulting in low-grade evidence that struggles to gain widespread adoption in international guidelines. Additionally, the “multi-component, multi-target” nature of TCM, while an advantage, also poses significant research challenges. Most current studies on the mechanisms of action of compound formulas remain confined to whole-animal experiments and limited pathway validation. Systematic and in-depth elucidation of how these formulas precisely regulate the neuro-immune-TME network, and which specific active components play key roles, remains lacking. Furthermore, standardized guidelines for clinical application are absent. Therefore, it is crucial to design and conduct large-scale, multicenter, randomized, double-blind, placebo-controlled clinical trials. By integrating cutting-edge technologies such as systems pharmacology, network pharmacology, and metabolomics, we must deeply analyze the effective component groups, target networks, and synergistic mechanisms of TCM formulas. This will enable us to explain their “synergistic efficacy and reduced toxicity” principles using modern scientific language. Establishing standardized clinical pathways and expert consensus/guidelines is particularly important [244].
The pathogenesis of cancer pain involves complex regulation between the peripheral and CNS. Modern research reveals that its mechanisms primarily include tumor cells and infiltrating immune cells releasing large amounts of inflammatory mediators and nociceptive substances such as IL-1β, IL-6, TNF-α, PGE2, NGF, and ATP, which continuously stimulate and sensitize peripheral nociceptors, leading to peripheral sensitization; Upregulation or abnormal activation of TRPV1, VGSCs, and calcium channels significantly lowers neuronal excitation thresholds, resulting in spontaneous pain and hyperalgesia; Persistent nociceptive signals transmitted to the CNS cause excessive activation of the glutamate-NMDA receptor system, while concurrent relative insufficiency in descending inhibitory systems collectively exacerbates pain perception and maintenance; Activated microglia and astrocytes in the spinal cord release large amounts of proinflammatory cytokines, forming positive feedback loops with neurons to drive and sustain chronic pain states; Tumors disrupt the bone microenvironment by overactivating osteoclasts through the OPG/RANKL/RANK pathway, causing bone destruction and local microenvironment acidification that directly stimulates nerve endings. These parallel and interacting networks of mechanisms determine the limitations of single-target drugs and underscore the necessity of developing multi-mechanism synergistic intervention strategies. However, cancer pain represents a dynamically evolving process. Existing research predominantly focuses on identifying the role of specific molecules or cells in cancer pain, lacking a framework capable of dynamically guiding multimodal treatment combinations tailored to different stages and subtypes of cancer pain. Consequently, the future of cancer pain management will inevitably rely on integrated strategies that synergistically target multiple pathways and maximize therapeutic windows [245]. Subsequent research must follow a timeline to reveal how the dominant mechanism of pain transitions from primarily “peripheral sensitization” in early-stage tumors to “central sensitization” and “neuroimmune dysregulation” in advanced stages. Only through a profound understanding of these mechanisms can next-generation therapies be developed to directly interrupt the vicious cycle of cancer pain. This will also provide clearer modern scientific evidence and more precise combined treatment targets for integrated Chinese and Western medicine therapies.
Although integrated Chinese and Western medicine therapies demonstrate significant potential in synergistic mechanisms and clinical efficacy enhancement with reduced toxicity, the ultimate realization of therapeutic effects—whether from Western or traditional Chinese medicines—remains highly dependent on the efficiency of drug delivery within the body. Traditional administration methods (such as oral tablets or injections) often encounter issues like significant pharmacokinetic variability, high systemic exposure, and poor targeting. This leads to inconsistent analgesic effects, increased adverse reactions, and reduced patient compliance. To overcome these bottlenecks, advanced DDS have emerged, propelling cancer pain management from the traditional “drug selection” model toward a modern paradigm of “precision delivery.”
Oral controlled-release and sustained-release systems achieve steady, sustained drug release within the gastrointestinal tract through technological optimization, effectively avoiding the “peak-trough” phenomenon in blood drug concentrations. This not only reduces dosing frequency and improves patient compliance but, more crucially, provides stable background analgesia, laying the foundation for managing chronic cancer pain. However, such systems are unsuitable for advanced cancer pain patients with dysphagia. They require time to reach steady-state concentrations in the body. Crushing, chewing, or co-administration with alcohol poses risks of dose bursts, increasing adverse reaction rates. Individual variations in gastrointestinal function and pathological states may also affect drug absorption, leading to inconsistent efficacy or adverse reactions. To overcome these limitations, the development of “rapid-release + sustained-release” combination formulations offers the dual advantages of rapid onset and prolonged analgesia. For patients with swallowing difficulties, the microencapsulation system allows capsules to be opened, enabling patients to swallow intact sustained-release microparticles with soft food. Orally disintegrating tablets provide a convenient alternative that requires no water. Both approaches offer new perspectives for cancer pain management. In the realm of safety, integrating abuse-deterrent technologies is a key direction. The use of physical barriers, added antagonists, or aversive agents can effectively curb the risks of drug abuse and misuse.
Mucosal delivery systems and transdermal delivery systems represent significant advances in non-invasive, rapid-acting, or sustained-release drug administration. Mucosal delivery utilizes the rich vascular and lymphatic networks of oral and nasal mucosa to bypass hepatic first-pass metabolism, enabling rapid drug absorption. This provides breakthrough solutions for cancer pain with onset times measured in minutes. However, current research on the mechanisms of mucosal drug delivery remains insufficient, and numerous technical challenges persist. These include the mucus layer on mucosal surfaces potentially hindering drug penetration, proteases or cytochromes present in mucosa potentially degrading drugs, drugs being readily cleared, certain mucosal sites being prone to triggering immune responses, and mucosal delivery potentially being limited by local irritation or tolerance issues affecting long-term use [246]. Future applications could integrate functional nanocarriers from MDDS into existing formulations [247], leveraging their advantages in targeted positioning and prolonged drug release. Another approach involves loading phospholipid surfactants and octadecylamine into solid lipid NPs, enabling targeted drug delivery to tissues expressing phosphatase. This facilitates penetration through the mucus layer while maintaining close proximity to the absorption membrane, thereby achieving targeted, site-specific mucosal drug delivery [248]. With advances in modern pharmaceutical technology and the ongoing refinement of mucosal delivery theory, more rational and effective mucosal delivery systems are expected to achieve clinical translation, offering additional treatment options for cancer pain patients.
Transdermal patches deliver sustained and stable drug penetration through the skin’s stratum corneum, providing continuous analgesia for up to several days. They are particularly suitable for patients with swallowing difficulties or gastrointestinal dysfunction. While this system significantly expands clinical administration pathways to meet diverse therapeutic needs, transdermal drug absorption is susceptible to skin barrier integrity and environmental factors [249]. Additionally, skin irritation or allergic reactions may occur at the application site. From a safety perspective, localized skin reactions remain a significant factor limiting long-term use. Regarding scalability, challenges persist in the mass production and quality control of patches, while variations in skin permeability among individuals further restrict their standardized application. Advancements in skin permeation strategies now enable transdermal delivery of diverse anticancer therapies—from lipophilic small molecules to hydrophilic biomolecules—promising to overcome limitations of existing transdermal technologies and enhance cancer pain relief efficacy [250]. Beyond this, the advent of MN technology offers an innovative solution for cancer pain management. MN arrays, composed of hundreds of micrometer-scale MNs, physically penetrate the skin’s outermost stratum corneum layer in an instant while stopping just above the dermis, avoiding contact with nerve endings. This enables painless, bloodless, and minimally invasive drug delivery. This characteristic offers significant clinical advantages for cancer pain patients requiring long-term, frequent dosing who may be debilitated or cachectic. It not only enhances transdermal absorption rates and reduces pain perception but also enables convenient self-administration, providing an ideal platform for precise analgesia with high local concentrations and low systemic exposure. Despite its promising prospects, translating MN technology from the laboratory to large-scale clinical application in cancer pain management faces several challenges. For instance, the drug loading capacity per MN is extremely low. For potent opioids with high daily requirements, this may necessitate an exceptionally large patch area. Additionally, manufacturing processes demand high precision and stability to ensure the mechanical strength of needle tips for successful skin penetration while preserving drug bioactivity during production and storage. Finally, long-term safety requires thorough evaluation, including potential risks of skin irritation and possible local immune responses. To address these issues, research should develop novel materials and structures with high drug-loading capacity or construct “NP@MN” composite delivery systems to overcome loading limitations. Production processes must be optimized to ensure mechanical strength and drug stability, while prioritizing materials with excellent biocompatibility and degradability to enhance long-term safety.
For refractory cancer pain unresponsive to conventional treatments, intrathecal targeted drug delivery represents a significant breakthrough. By delivering microdoses of opioids directly into the subarachnoid space via an implantable pump, the medication acts directly on opioid receptors in the dorsal horn of the spinal cord. The required dosage is only one-three-hundredth of an oral dose. This “central-targeted” administration achieves potent analgesia while minimizing systemic side effects, representing one of the highest levels of intervention in cancer pain management. Currently, this technology is primarily applied to patients with moderate-to-severe refractory cancer pain [251]. Although more effective than standard care, its higher cost [252] limits its adoption in primary healthcare settings. Additionally, intrathecal administration is an invasive procedure that may increase infection risk, requires strict technical conditions, and has associated adverse reaction reports [253]. Therefore, clinicians require enhanced training to reduce surgical infection risks and should promptly update infusion techniques to optimize efficacy and lower adverse event rates. Concurrently, increased public funding is urgently needed to expand its application in clinical treatment, thereby benefiting more patients. Beyond this, the application of single-use intrathecal targeted drugs has progressively expanded, now covering diverse targets from cell membranes to nuclei and from neurons to immune glial cells. The intrathecal administration of naturally occurring small molecules offers novel delivery approaches for integrated Chinese and Western medicine pain management. However, translating these cutting-edge targets from basic research into routine clinical practice remains challenging. Long-term drug safety, optimal dosage and administration cycles, and potential off-target effects require systematic evaluation in larger animal models and future human trials. Furthermore, developing agonists/antagonists capable of crossing the blood–brain barrier with higher receptor selectivity is crucial for enhancing the efficacy and safety of such therapies.
Cutting-edge nanotechnology is also paving new paths for next-generation cancer pain treatment. Nanocarrier systems achieve precise drug targeting and controlled release by encapsulating analgesics, enabling extended circulation times and passive or active targeting to sites of inflammation or neuropathy, thereby enhancing efficacy while reducing toxicity [254]. The advancement of bionic nanotechnology also provides insights and momentum for the modernization of TCM, offering new opportunities for cancer pain management [241]. However, nanocarriers themselves may raise new safety concerns, such as immunogenicity, organ accumulation toxicity, and unpredictable biodegradability. Their complex manufacturing processes and inconsistent quality control standards also hinder large-scale clinical application. Furthermore, frequent injection administration may reduce patient compliance, necessitating the development of more convenient dosage forms. For instance, designing nanocarriers that specifically respond to TME characteristics to achieve controlled drug release could enhance efficacy while further reducing off-target effects. Second, deepening the integration of TCM and modern medicine at the nanoscale is crucial. Successful examples of co-delivery bionic nanosystems (Q+M/MnOx)@Clip) demonstrate that combining natural TCM active ingredients like quercetin with modern nanotechnology can synergistically regulate multiple targets in the TME and pain signaling pathways. This offers a highly promising pathway for the modernization and internationalization of TCM. Finally, advancing interdisciplinary collaboration to optimize delivery strategies is paramount. This entails exploring non-invasive delivery methods to partially replace injection routes, integrating NDDS with interventional therapies for “targeted clearance,” and conducting large-scale animal studies alongside rigorous clinical translation research. Ultimately, these promising laboratory findings must be transformed into clinical solutions that genuinely benefit cancer pain patients.
7. Summary and Outlook
This paper systematically expounds the synergistic and attenuated advantages of the combination of traditional Chinese and Western medicine in the treatment of cancer pain for the first time. By combining TCM compound preparations with the effects of tonifying kidney and filling marrow, promoting blood circulation and removing blood stasis, clearing heat and detoxifying or warming yang and dredging stagnation with opioids, it can achieve multi-mechanism synergistic analgesic effect, reduce the dosage of opioids and the incidence of adverse reactions, and achieve better efficacy than western medicine alone in pain management. Through the summary of the therapeutic mechanism of analgesic drugs, it is found that the analgesic system can play a therapeutic role by intervening from peripheral sensitization, neuronal excitability changes, central sensitization to bone destruction. In addition, this paper summarizes the application of DDS in the treatment of cancer pain for the first time. The steady-state control of back pain can be achieved by oral sustained and controlled release. Mucosal administration can provide rapid rescue for breakthrough pain. Transdermal administration provides patients with non-invasive and long-term drug delivery options. The ultimate minimally invasive intervention for refractory pain can be achieved by intrathecal targeted delivery technology. The emergence of DDS shows the precision and individualization of analgesic therapy. The cutting-edge research of new DDS in cancer pain management such as MNs, one-time intrathecal injection and NDDS is committed to achieving targeted delivery, intelligent release and long-term sustained release, or will break through the limitations of existing therapies.
Based on the above findings, the evolution of cancer pain management reveals the limitations of single therapy and highlights the inevitable trend of integrating multi-mode strategies. The traditional WHO three-step principle and opioid-led model still have bottlenecks in dealing with complex neuropathic pain and long-term drug side effects. Although the combination of traditional Chinese and Western medicine has shown the potential of “increasing efficiency and reducing toxicity”, its application is mostly based on experience, lacking collaborative theoretical guidance and standardized programs based on precise mechanisms. Advanced DDS provide tools for achieving precise treatment, but their design is often insufficiently combined with the deep pathological mechanism of pain and the needs of specific drug combinations. The multi-mechanism approach of the dynamic evolution of cancer pain determines that the future cancer pain management is not only a simple superposition of drugs or technologies, but also a fine assessment of the type of pain in patients, and a clear understanding of its dominant pain mechanism. Based on this mechanism, a synergistic combination of Chinese and Western medications should be selected, paired with the most suitable delivery system capable of precisely and controllably delivering this combination to the target site. Looking ahead, achieving this transformation requires research to focus on key directions: Utilizing multi-omics technologies and artificial intelligence to establish mapping between different clinical stages of cancer pain and their molecular/cellular characteristics, providing objective, quantifiable standards for mechanism-based classification; Employing systems pharmacology and cutting-edge experimental models to elucidate synergistic networks of Chinese and Western medicines within key signaling pathways, thereby providing theoretical foundations for drug combinations; Advancing delivery systems toward intelligent upgrades enabling responsiveness to specific pain microenvironments, achieving on-demand drug release, and integrating with interventional therapies for precision treatment; Conducting prospective integrated clinical studies to validate the superiority of specific drug combinations paired with tailored delivery methods, gradually establishing clinical guidelines.
In summary, deepening our understanding of cancer pain mechanisms is the cornerstone for advancing treatment. The integration of Chinese and Western medicine with advanced drug delivery technologies will propel cancer pain management toward a new era of enhanced efficacy and safety. Through multidisciplinary collaboration and innovative integration, we can progress beyond current symptom control to achieve disease treatment based on pathological mechanisms, ultimately leading to a fundamental improvement in patients’ quality of life.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu D. Weng J.-S. Ke X. Wu X.-Y. Huang S.-T. The Relationship between Cancer-Related Fatigue, Quality of Life and Pain among Cancer Patients Int. J. Nurs. Sci.20231011111610.1016/j.ijnss.2022.12.00636860712 PMC 9969059 · doi ↗ · pubmed ↗
- 2van den Beuken-van Everdingen M.H.J. de Rijke J.M. Kessels A.G. Schouten H.C. van Kleef M. Patijn J. Prevalence of Pain in Patients with Cancer: A Systematic Review of the Past 40 Years Ann. Oncol.2007181437144910.1093/annonc/mdm 05617355955 · doi ↗ · pubmed ↗
- 3Gebhart G.F. Bielefeldt K. Physiology of Visceral Pain Compr. Physiol.201661609163310.1002/j.2040-4603.2016.tb 00725.x 27783853 · doi ↗ · pubmed ↗
- 4Wang G. Mechanisms of cancer pain Chin. J. Cancer Prev. Control.2017914
- 5Joshy G. Khalatbari-Soltani S. Soga K. Butow P. Laidsaar-Powell R. Koczwara B. Rankin N.M. Brown S. Weber M. Mazariego C. Pain and Its Interference with Daily Living in Relation to Cancer: A Comparative Population-Based Study of 16,053 Cancer Survivors and 106,345 People without Cancer BMC Cancer 20232377410.1186/s 12885-023-11214-537700229 PMC 10498633 · doi ↗ · pubmed ↗
- 6World Health Organization WHO Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents; WHO Guidelines Approved by the Guidelines Review Committee World Health Organization Geneva, Switzerland 2018978-92-4-155039-030776210 · pubmed ↗
- 7Shkodra M. Caraceni A. Treatment of Neuropathic Pain Directly Due to Cancer: An Update Cancers 202214199210.3390/cancers 1408199235454894 PMC 9031615 · doi ↗ · pubmed ↗
- 8Fallon M. Giusti R. Aielli F. Hoskin P. Rolke R. Sharma M. Ripamonti C.I. ESMO Guidelines Committee Management of Cancer Pain in Adult Patients: ESMO Clinical Practice Guidelines Ann. Oncol.201829 iv 166iv 19110.1093/annonc/mdy 15230052758 · doi ↗ · pubmed ↗