Heart Failure Outcomes with SGLT2 Inhibitors in Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis
Raghad Rasheed Alrasheed, Amenah Fayez Altaf, Abdullah Hameed Althurwi, Shahad Fahad Alrodan, Manal Hussain Asiri, Bushra Abdulrahman Alsaluli, Muath Awadh Alsurur, Khalid Ali Alghamdi, Ahmed Anwer Alrowaithi, Nariman Safar Almalki

TL;DR
This study finds that SGLT2 inhibitors reduce heart failure events and improve kidney outcomes in adults with type 2 diabetes and heart failure.
Contribution
The study consolidates and updates evidence from RCTs focusing on patients with both T2DM and established HF.
Findings
SGLT2i reduced worsening heart failure or cardiovascular death by 21%.
Heart failure hospitalizations were consistently reduced across trials.
SGLT2i showed renoprotective effects and a favorable safety profile.
Abstract
Background and Objectives: Type 2 diabetes mellitus (T2DM) substantially increases the risk of heart failure (HF) and worsens its prognosis. Sodium-glucose cotransporter-2 inhibitors (SGLT2i), initially developed for glycemic control, have shown important cardiovascular benefits. This systematic review and meta-analysis evaluated the effects of SGLT2i on HF hospitalizations, cardiovascular (CV) death, and renal outcomes, as well as their safety profile, in patients with T2DM and established HF. Materials and Methods: Following PRISMA 2020 guidelines, we systematically searched PubMed, the Cochrane Library, and Web of Science for randomized controlled trials (RCTs) comparing SGLT2i with placebo in adults with T2DM and HF. Data on HF hospitalizations, CV death, other clinical outcomes, and adverse events were extracted. Risk of bias was assessed using the Cochrane RoB2 tool, and pooled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
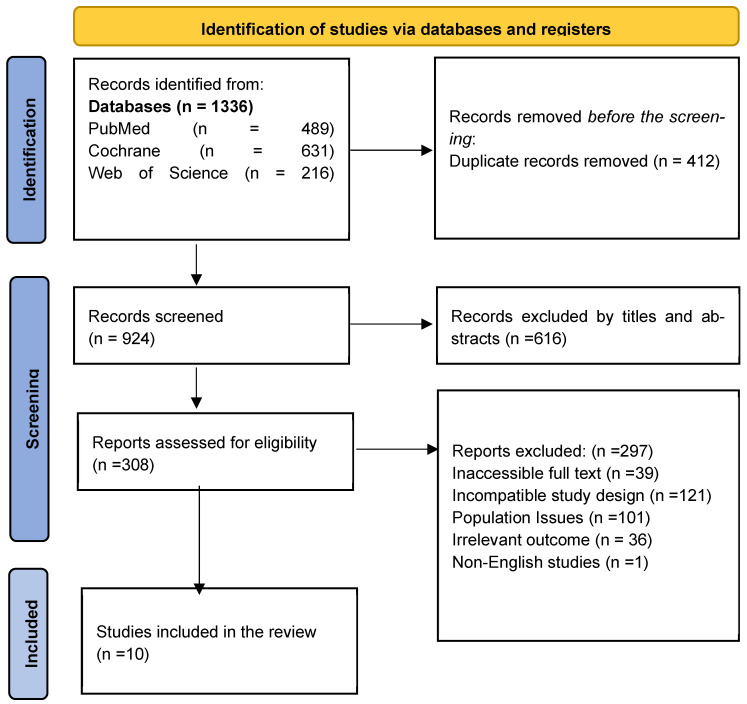 Figure 1
Figure 1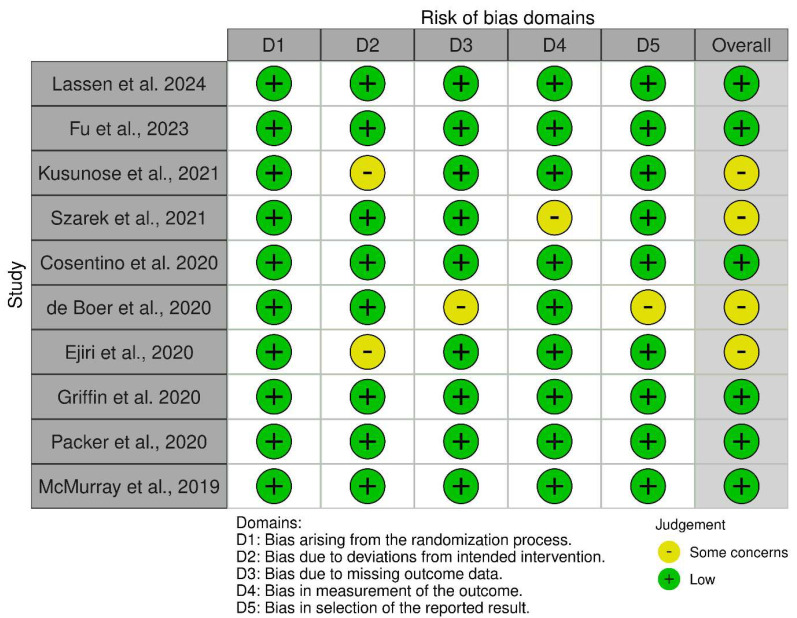 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Hyperglycemia and glycemic control in critically ill and hospitalized patients · Heart Failure Treatment and Management
1. Introduction
Type 2 diabetes mellitus (T2DM) represents a major health concern worldwide, and its prevalence is rising in both wealthy and developing countries. Recent estimates suggest that more than 500 million individuals around the globe are impacted, with T2DM representing the largest portion of these cases [1]. Among T2DM patients, cardiovascular issues are the primary contributors to illness and death. Notably, heart failure (HF) stands out as one of the most prevalent and significant consequences [2,3]. Individuals with diabetes face a significantly higher risk of experiencing HF, with their likelihood being two to five times greater compared to those without the condition [4,5]. The coexistence of T2DM and HF leads to notably adverse outcomes, such as elevated hospitalization rates, greater mortality, and rising healthcare expenses [6,7]. The primary aim of managing HF is to suppress neurohormonal pathways with medications such as angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), beta-blockers, and mineralocorticoid receptor antagonists (MRAs), particularly in patients with a reduced ejection fraction. However, prior to the arrival of SGLT2 inhibitors, there were few alternatives for managing patients with preserved ejection fraction [8].
Sodium-glucose cotransporter 2 inhibitors (SGLT2i) were primarily formed to reduce blood glucose levels. However, their therapeutic uses have evolved significantly, as they now also provide notable cardiovascular and renal advantages that go beyond just managing blood sugar [9,10]. These drugs function by encouraging the elimination of sodium through urine, enhancing circulation, decreasing the heart’s preload and afterload, lowering blood pressure, supporting moderate weight loss, improving heart muscle metabolism, and possibly mitigating oxidative stress and inflammation [11,12]. The different mechanisms suggest that SGLT2i may be crucial for preventing and treating heart failure across diverse patient groups, regardless of diabetes status.
Several RCTs have demonstrated cardiovascular benefits of SGLT2i in both diabetic and non-diabetic populations. Studies such as EMPA-REG OUTCOME (empagliflozin) [13], CANVAS (canagliflozin) [14], DECLARE-TIMI 58 (dapagliflozin) [15], DAPA-HF [8], EMPEROR-Reduced [16], EMPEROR-Preserved [17], DELIVER [18], and SOLOIST-WHF [19] have consistently shown reductions in hospitalizations for HF and CV death. As a result, recent European Society of Cardiology (ESC) heart failure guidelines now recommend SGLT2 inhibitors as a Class I, Level A therapy for patients with heart failure with reduced ejection fraction, irrespective of diabetes status [20]. Similarly, the 2023 ADA Standards of Care highlight the expanded role of SGLT2 inhibitors in patients with type 2 diabetes and heart failure [21].
Recent trial data provide robust evidence for SGLT2 inhibitors (SGLT2i); however, previous systematic reviews were largely restricted to specific outcomes or type 2 diabetes populations. Against this background, the present systematic review and meta-analysis aimed to synthesize and update evidence from randomized controlled trials on the effects of SGLT2i in patients with both T2DM and established HF, with a focus on HF hospitalizations, CV death, overall cardiovascular outcomes, and renal endpoints.
2. Methodology
This systematic review and meta-analysis were conducted and reported in accordance with the PRISMA 2020 statement [22]. The review protocol was not prospectively registered in a public database.
2.1. Literature Search Strategy
PubMed, Web of Science, and the Cochrane Library were used for the search of the existing literature. The following combination of keywords: (“Type 2 Diabetes Mellitus” OR “Type II Diabetes Mellitus” OR “Type 2 Diabetes” OR “NIDDM” OR “Maturity Onset Diabetes Mellitus” OR “MODY”) AND (“Heart Failure” OR “HF” OR “Congestive Heart Failure” OR “Cardiac Failure” OR “Heart Failure With Reduced Ejection Fraction” OR “Heart Failure With Preserved Ejection Fraction” OR “HFrEF” OR “HFpEF”) AND (“SGLT-2 Inhibitor” OR “SGLT 2 Inhibitor” OR “SGLT2 Inhibitor” OR “Sodium-Glucose Transporter 2 Inhibitor” OR “Gliflozin” OR “SGLT2i” OR “Canagliflozin” OR “Dapagliflozin” OR “Empagliflozin” OR “Ertugliflozin” OR “Sotagliflozin” OR “Ipragliflozin” OR “Luseogliflozin” OR “Tofogliflozin” OR “Invokana” OR “Farxiga” OR “Jardiance”) AND (“Placebo” OR “Standard care” OR “Standard therapy” OR “Usual care” OR “Control group” OR “Comparator”) AND (“Heart failure hospitalization” OR “Cardiovascular death” OR “CV death” OR “All-cause mortality” OR “MACE” OR “Hospitalization for heart failure” OR “Cardiovascular morbidity” OR “LVEF” OR “Cardiac remodeling” OR “functional status” OR “Quality of life” OR “Biomarkers” OR “Adverse events”).
2.2. Selection of Articles
Following an initial search of the database, two separate reviewers assessed the titles and abstracts to investigate studies that aligned with the established inclusion criteria. The chosen articles were then subjected to a thorough review of their full text for eligibility by the same reviewers. Any discrepancies in their assessments were addressed through discussion or by consulting a third reviewer. Studies were included in the analysis if they examined the safety or efficacy of SGLT2i, used alone or in conjunction with other therapies, and consisted of RCTs, cohort studies, or case-control studies reporting at least one pertinent clinical outcome, including hospitalization due to HF, CV-related deaths, overall mortality, or quality of life, with publications available in English. On the other hand, studies were excluded from consideration if they pertained to type 1 diabetes mellitus, gestational diabetes, or pediatric groups, or if they were animal studies, in vitro experiments, mechanistic studies, reviews, editorials, letters to the editor, case reports, or conference abstracts lacking full text. Additionally, studies with insufficient data or unclear methodology, as well as duplicate publications, were excluded, with only the most comprehensive or recent version being considered. The data extraction process was carried out using a uniform, pre-tested methodology.
2.3. Data Extraction
Two reviewers collected data utilizing a pre-structured Excel spreadsheet alongside a standard data extraction form that was tested beforehand. The relevant studies were first identified and organized through EndNote reference management software. For every study that satisfied the inclusion criteria, details were gathered regarding study characteristics (including the first author’s name, publication year, country, and type of study), as well as participant information (total sample size, mean or median age, gender distribution, and diagnostic criteria for T2DM and HF), intervention details (type and name of SGLT2 inhibitor used, dosage, and duration of follow-up), the comparison group (type of comparator used, such as placebo, standard care, or other antidiabetic agents), outcomes of interest (including reduction in heart failure hospitalizations, cardiovascular death, and improvement in overall clinical outcomes), and key findings (reported effect estimates, confidence intervals, and statistical significance). Data were independently extracted by the primary reviewer. When information was missing or unclear, the study authors were contacted for clarification, when possible. All extracted data were organized and reviewed for accuracy and completeness before synthesis.
2.4. Quality Assessment
The Cochrane risk-of-bias tool for randomized trials (RoB2) [23] was used for assessing risk of bias. This framework assesses the likelihood of bias in randomized controlled trials (RCTs) by examining five key components: the implementation of randomization, variations from intended interventions, management of missing data, methods for evaluating outcomes, and the criteria for selecting reported outcomes. Every element is evaluated and assigned a bias risk level of low, moderate, or high, and the overall bias risk for each study is established based on these evaluations.
2.5. Statistical Analysis
We used RevMan 5.4.1 [24]. The findings were presented as hazard ratios accompanied by 95% confidence intervals (CIs), utilizing a random-effects model. To assess the degree of statistical heterogeneity among the studies, the I-squared (I^2^) and chi-squared (Chi^2^) statistics were employed.
3. Results
An extensive search yielded 1336 research articles across three databases: PubMed, Web of Science, and Cochrane. Of these, 412 were removed due to duplication, and 616 were eliminated after reviewing their titles and abstracts. Following a thorough full-text assessment, an additional 297 articles were excluded. Only ten studies met the inclusion criteria for the systematic review, as shown in the PRISMA 2020 flow diagram (Figure 1).
Our analysis comprised RCTs conducted primarily on an international scale, involving more than 21,000 participants. These investigations focused on the impact of various SGLT2 inhibitors, including Dapagliflozin, Sotagliflozin, Canagliflozin, Ertugliflozin, Licogliflozin, Empagliflozin, and Luseogliflozin, in individuals with both chronic HF and T2DM. The trials thoroughly explored the heart failure spectrum, enrolling patients with both reduced ejection fraction (HFrEF, LVEF ≤ 40%) and preserved ejection fraction (HFpEF, LVEF > 40%). These classifications were based on standardized criteria, including NYHA functional class and elevated levels of natriuretic peptides (BNP/NT-proBNP). The interventions were consistently administered as add-on therapies to standard care, using doses equivalent to those prescribed for glycemic control. They were tested against a placebo in double-blind designs to minimize performance bias. The follow-up durations ranged from 12 weeks to 4 years, and these trials aimed to assess both physiological and major adverse clinical endpoints. This design allowed for a comprehensive evaluation of the effects of the SGLT2 inhibitor class across a broad and clinically relevant patient population. The characteristics of the included randomized controlled trials are summarized in Table 1.
Our study highlights that SGLT2 inhibitors offer significant benefits for patients with HF and T2DM, regardless of their ejection fraction levels. They are particularly effective in reducing heart failure hospitalizations (HHF), with hazard ratios (HRs) ranging from 0.61 to 0.75 across major trials such as DAPA-HF, EMPEROR-Reduced, and VERTIS-CV. These benefits result from evidence that the heart can improve its function, along with increased urine output and reduced blood volume, without causing any negative hormonal changes. While the impact on CV death varied among trials, the overall decrease in the combined result of hospitalization for heart failure (HHF) or CV death remained consistent. Importantly, patients experience increased days alive and improved health status. The safety profile is favorable; there is no heightened risk of severe negative side effects, low blood sugar events, or kidney problems; rather, there is a beneficial impact on kidney health. The most common side effect is a mild increase in genital infections. In conclusion, SGLT2 inhibitors are foundational in heart failure management for type 2 diabetes, offering significant reductions in heart failure events and renal protection with a strong risk-benefit profile, as shown in Table 2.
Most of the studies assessed were considered to have a minimal overall risk of bias, indicating their strong methodological standards. While most studies demonstrated low risk across all specific domains, particularly in the randomization process, several concerns were raised, primarily regarding discrepancies from the planned interventions and how the outcomes were measured. Therefore, the body of evidence is robust, but the findings should be interpreted with slight limitations (Figure 2).
The data presented in Figure 3 indicate that SGLT2 inhibitors lower the likelihood of worsening heart failure or cardiovascular death by 21% when compared to the control group (HR = 0.79; 95% CI: 0.69 to 0.89). This result is statistically significant (p = 0.0001) with low heterogeneity.
4. Discussion
This review highlights that SGLT2 inhibitors provide clinically meaningful benefits for individuals with T2DM and HF. Our meta-analysis indicates that SGLT2i reduce the composite risk of worsening HF or CV death by 21%. The most pronounced effect was a reduction in HHF, while CV mortality effects varied across trials but were generally favorable. SGLT2i were associated with improvements in patient-reported health status and renal outcomes. Overall, they were well tolerated, with a modest increase in genital infections. Our findings support and expand upon previous systematic reviews. A large meta-analysis by McGuire et al. (2021) [33] concluded that SGLT2i reduces HHF and the composite of HHF/CV death in patients with T2DM, with broadly consistent effects across key subgroups. More recently, Chen et al. (2023) [34] conducted a network meta-analysis comparing individual SGLT2 inhibitors, confirming that the cardiovascular benefits are broadly similar across different agents, with dapagliflozin and empagliflozin demonstrating the strongest evidence.
Additionally, a review by Gao et al. (2024) [35] focused on functional abilities and quality of life, showing that SGLT2 inhibitors lead to higher KCCQ scores and improved exercise capacity in HF patients. Lastly, a comprehensive meta-analysis published in 2024 [36] reinforced that SGLT2i improve cardiovascular and kidney outcomes in patients with diabetes.
Emerging evidence also suggests that SGLT2 inhibitors may have potentially beneficial effects on arrhythmic outcomes. A recent literature review on oral glucose-lowering agents and life-threatening arrhythmias in patients with T2DM reported heterogeneous effects across drug classes but did not identify an increased risk of serious arrhythmias with SGLT2i. In some of the included studies, SGLT2i were associated with a lower prevalence of atrial fibrillation and sudden cardiac arrest, whereas the impact on ventricular arrhythmias remained less certain [37]. Although these data are indirect and based on nonrandomized evidence, they support the hypothesis that SGLT2i may confer additional protection against malignant arrhythmic events beyond the reduction in HF hospitalizations observed in our meta-analysis.
Heart failure hospitalizations were notably reduced in several key trials investigating the effects of SGLT2i. In the DAPA-HF trial conducted by McMurray et al. (2019) [8], dapagliflozin demonstrated a substantial 30% reduction in the risk of HHF compared to a placebo. Similarly, the EMPEROR-Reduced trial by Packer et al. (2020) [16] reported a 25% reduction with empagliflozin. VERTIS-CV, conducted by Cosentino et al. (2020) [29], also reported a significant decrease in heart failure hospitalizations with ertugliflozin, although the magnitude of this effect was less pronounced. Importantly, in patients who had preserved ejection fraction, both (Anker et al., 2021) [17] and DELIVER (Lassen et al., 2024) [25] confirmed that SGLT2 inhibitors may contribute to a decrease in hospitalizations due to HF, even in this historically treatment-resistant group. In contrast, smaller studies like those by Ejiri et al. (2020) [31] with luseogliflozin and Kusunose et al. (2021) [27] with canagliflozin reported no statistically significant reductions in HHF, likely due to limited sample sizes and shorter follow-up durations.
The effect of SGLT2i on CV mortality presented more variability. DAPA-HF [8] reported a significant reduction in CV death, while EMPEROR-Reduced [16] and VERTIS-CV [29] did not show significant effects. The SOLOIST-WHF trial (Szarek et al., 2021) [28] indicated that sotagliflozin reduced total CV events, even though the decrease in cardiovascular-related deaths did not achieve statistical significance. The meta-analysis revealed a positive trend across trials, suggesting that while the benefits regarding mortality may differ across trials, the overall effect of the class on the combined outcome of HHF and cardiovascular death remains stable.
Regarding all-cause mortality, few trials were adequately powered to detect differences. DAPA-HF [8] noted a modest reduction in all-cause mortality, while EMPEROR-Reduced [16] and VERTIS-CV [29] did not show significant results. Mechanistic studies, such as those conducted by Fu et al. (2023) [26] and Griffin et al. (2020) [32], were not explicitly designed to assess mortality. However, they provided supportive evidence of improved cardiac function and hemodynamics, which may confer long-term survival benefits.
Mechanistic and imaging-focused studies offered valuable insights into how SGLT2i exert their beneficial effects. According to Fu et al. (2023) [26], there were notable enhancements in left ventricular ejection fraction, showing a 5.5% rise in comparison to a 2.5% increase observed with the placebo. Additionally, there was a decrease in left ventricular volumes, suggesting reverse remodeling. Griffin et al. (2020) [32] reported that empagliflozin enhanced diuretic efficiency and improved renal hemodynamics, reinforcing its role in volume management. Kusunose et al. (2021) [27] found that canagliflozin reduced NT-proBNP levels in patients with impaired diastolic function, suggesting benefits for HFpEF physiology. Beyond these clinical and imaging findings, experimental and translational work suggests that SGLT2 inhibition exerts pleiotropic cardio-renal effects, including hemodynamic unloading through osmotic diuresis and natriuresis, improvement in myocardial energetics partly via activation of AMP-activated protein kinase (AMPK), attenuation of inflammation and oxidative stress, and modulation of ion homeostasis through inhibition of the cardiac Na^+^/H^+^ exchanger (NHE1). In line with these mechanisms, a recent meta-analysis of adjudicated randomized trials reported that empagliflozin and dapagliflozin reduced the risk of sudden cardiac death by about 18% (odds ratio ≈ 0.82), thereby extending the spectrum of cardiovascular protection conferred by SGLT2i beyond their impact on HF outcomes [38]. Collectively, these findings lend mechanistic plausibility to the reductions in clinical events observed in larger outcome trials. Renal protection emerged as a consistent secondary benefit across major trials. Both DAPA-HF [8] and EMPEROR-Reduced [16] reported that the SGLT2 inhibitor groups demonstrated a slower decrease in estimated glomerular filtration rate (eGFR) and experienced a reduced number of renal composite events. This protective effect on the kidneys was observed regardless of initial diabetes status, underscoring the dual benefits for both the heart and kidneys associated with this class of medication.
Patient-reported outcomes also showed improvements. In the EMPEROR-Reduced and DELIVER trials, empagliflozin and dapagliflozin significantly improved KCCQ scores, indicating reduced symptom burden and improved quality of life. These findings align with Gao et al. (2024) [35], which confirmed that SGLT2i improve functional capacity and health status in HF patients. Finally, the safety profile of SGLT2i across all studies indicated that they were well-tolerated. The most frequently reported adverse event was a modest increase in genital infections, which were generally mild and manageable. Importantly, there was no excess risk of hypoglycemia, diabetic ketoacidosis, or renal dysfunction. This favorable safety profile was consistent across both large outcome trials and smaller mechanistic studies, underscoring the clinical applicability of SGLT2i in a broad range of patient populations.
Overall, CV mortality effects varied across trials, but SGLT2i consistently reduced HHF, improved patient-reported outcomes, and protected renal function. Combined with a favorable safety profile, these features position them alongside established therapies such as ACE inhibitors, beta-blockers, and mineralocorticoid receptor antagonists. Future studies should prioritize examining long-term effects, direct comparisons with other innovative treatments like angiotensin receptor-neprilysin inhibitors and GLP-1 receptor agonists, as well as assessing real-world efficacy in populations that are often overlooked.
Our work adds several elements to the existing literature. First, we focused specifically on randomized controlled trials that enrolled patients with both T2DM and established HF, rather than broader cardiovascular or diabetes populations, allowing a more precise estimate of treatment effects in this particularly vulnerable group. Second, we integrated data across the full spectrum of ejection fraction and on contemporary background HF therapy, which reflects current clinical practice. Third, in addition to the composite of HF hospitalization and CV death, we summarized evidence on cardiac remodeling, patient-reported health status, and renal outcomes, thereby providing a comprehensive view of the multidimensional benefits of SGLT2i in T2DM-HF.
5. Limitations
This review acknowledges limitations arising from clinical and methodological diversity across included trials, including variations in follow-up and standard care. First, although screening was performed independently by two reviewers, we did not calculate an inter-rater reliability coefficient (e.g., Cohen’s κ). Second, given the limited number of included trials, we did not formally assess publication bias (funnel plot/Egger’s test) or perform sensitivity analyses or fail-safe N calculations. Third, because only aggregate data were available and reporting of NYHA class, diabetes duration, and baseline HbA1c was inconsistent, we could not explore heterogeneity using meta-regression. While the overall quality was high, residual bias cannot be excluded, and the analysis was constrained to study-level data, limiting subgroup explorations. Future studies should emphasize the long-term effects, their impact in under-represented HF and diabetes subgroups, and comparative analyses with other cardioprotective therapies.
6. Conclusions
This review demonstrates that SGLT2i therapy provides significant cardiovascular and renal benefits for patients with T2DM and HF. SGLT2 inhibitors reduce HF hospitalizations and improve key HF outcomes, with a consistent trend toward lower mortality and a favorable safety profile. In line with contemporary heart failure guidelines, SGLT2i (such as dapagliflozin and empagliflozin) should be considered a foundational treatment option for patients with T2DM and HF, and early initiation in appropriate candidates is encouraged.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Diabetes Federation IDF Diabetes Atlas 10th ed.International Diabetes Federation Brussels, Belgium 2021
- 2Mac Donald M.R. Petrie M.C. Varyani F. Ostergren J. Michelson E.L. Young J.B. Solomon S.D. Granger C.B. Swedberg K. Yusuf S. Impact of diabetes on outcomes in patients with heart failure according to left ventricular systolic function Eur. Heart J.2008291377138510.1093/eurheartj/ehn 15318413309 · doi ↗ · pubmed ↗
- 3Shah A.D. Langenberg C. Rapsomaniki E. Denaxas S. Pujades-Rodriguez M. Gale C.P. Deanfield J. Smeeth L. Timmis A. Hemingway H. Type 2 diabetes and incidence of cardiovascular diseases: A cohort study in 1.9 million people Lancet Diabetes Endocrinol.2015310511310.1016/S 2213-8587(14)70219-025466521 PMC 4303913 · doi ↗ · pubmed ↗
- 4Kannel W.B. Mc Gee D.L. Diabetes and cardiovascular disease: The Framingham Study JAMA 19792412035203810.1001/jama.1979.03290450033020430798 · doi ↗ · pubmed ↗
- 5Cavender M.A. Steg P.G. Smith S.C.Jr. Eagle K. Ohman E.M. Goto S. Kuder J. Im K. Wilson P.W.F. Bhatt D.L. Impact of diabetes mellitus on hospitalization for heart failure, cardiovascular events, and death: Outcomes at 4 years from the REACH Registry Circulation 201513292393110.1161/CIRCULATIONAHA.114.01479626152709 · doi ↗ · pubmed ↗
- 6Nichols G.A. Hillier T.A. Erbey J.R. Brown J.B. Congestive heart failure in type 2 diabetes: Prevalence, incidence 3, and risk factors Diabetes Care 2001241614161910.2337/diacare.24.9.161411522708 · doi ↗ · pubmed ↗
- 7Mc Hugh K. De Vore A.D. Wu J. Matsouaka R.A. Fonarow G.C. Heidenreich P.A. Yancy C.W. Green J.B. Altman N. Hernandez A.F. Heart failure with preserved ejection fraction and diabetes: JACC State-of-the-Art Review J. Am. Coll. Cardiol.20197360261110.1016/j.jacc.2018.11.03330732715 · doi ↗ · pubmed ↗
- 8Mc Murray J.J.V. Solomon S.D. Inzucchi S.E. Køber L. Kosiborod M.N. Martinez F.A. Ponikowski P. Sabatine M.S. Anand I.S. Bělohlávek J. Dapagliflozin in patients with heart failure and reduced ejection fraction N. Engl. J. Med.20193811995200810.1056/NEJ Moa 191130331535829 · doi ↗ · pubmed ↗