Genomic Profiling of Laryngeal Squamous Cell Carcinoma Reveals Novel Biomarkers for Precision Medicine
Beau Hsia, Gabriel A. Bitar, Nathan S. Tran, Katelin Keenehan, Pedro S. Bonilla, Saif Alshaka, Eli Oved, Peter T. Silberstein, Abubakar Tauseef, Vijay A. Patel, Aliasgher Khaku

TL;DR
This study identifies key genetic mutations in laryngeal cancer, revealing potential biomarkers for personalized treatment strategies.
Contribution
The study discovers gender-specific and metastasis-linked mutations in laryngeal cancer, offering new targets for precision therapy.
Findings
TP53 mutations are most common in laryngeal squamous cell carcinoma.
ATP8B1 and SAMD9L mutations are associated with metastatic disease.
Gender-specific mutations like CDK8 in females and ATP8B1 in males suggest personalized treatment opportunities.
Abstract
Objective(s): To characterize the somatic mutational landscape of laryngeal squamous cell carcinoma (LSCC) using AACR Project GENIE data to identify potential biomarkers for tumor progression and guide precision therapy. Methods: Clinical and genomic data from 135 LSCC samples (primary and metastatic) were analyzed from the AACR Project GENIE database. Mutations were compared by tumor site and gender using chi-squared and Mann–Whitney U tests; co-occurrence and mutual-exclusivity analyses were performed. Results: TP53 mutations were most common (89.6%), followed by KMT2D (27.4%), FAT1 (20.7%), and NOTCH1 (20.7%). CDK8 mutations were enriched in females (p = 0.011) and ATP8B1 in males (p = 0.013). DMD mutations characterized primary tumors (p = 0.049), whereas ATP8B1 and SAMD9L were linked to metastases (p < 0.001). The cohort was 85.9% male and 71.5% White; 59.2% of samples were primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
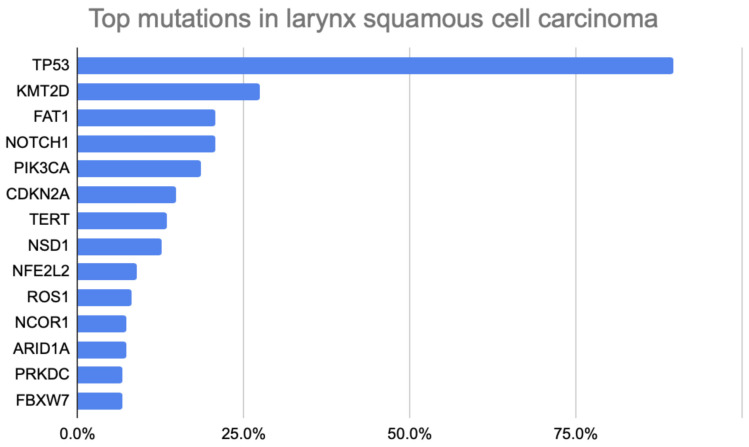 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Esophageal Cancer Research and Treatment · Cancer Genomics and Diagnostics
1. Introduction
Larynx squamous cell carcinoma (LSCC) is a malignant epithelial tumor arising from the squamous cells lining the larynx, particularly affecting structures such as the glottis, supraglottis, and subglottis [1]. The United States alone was responsible for 12,650 new cases and 3880 deaths in 2024 [2]. This cancer exhibited notable disparities by race and sex, with men having a higher incidence than women (10,030 cases versus 2620) [2]. LSCC encompasses the majority of laryngeal cancers with the largest number of cases originating from the glottic region, followed by the supraglottic area [3]. Clinically, LSCC typically presents with progressive symptoms such as persistent hoarseness, dysphagia, throat pain, or respiratory obstruction, depending on the tumor’s location and size [4]. In contemporary oncology, the integration of Next-Generation Sequencing (NGS) and mutation diagnostics has become pivotal, transitioning treatment paradigms from histology-based to molecularly-driven precision medicine.
Several risk factors have been closely linked to LSCC, including prolonged tobacco use, excessive alcohol consumption, gastro-esophageal reflux, occupational exposures, as well as infection with high-risk human papillomavirus (HPV) strains, particularly HPV-16 and HPV-18 [5,6]. The etiological role of HPV in LSCC remains debated; while occasional coinfection has been reported, its contribution is likely limited compared to oropharyngeal SCC. Recently, there has been growing attention to how socioeconomic factors, including ethnicity, gender, age, type of insurance coverage, and geographic location, influence treatment outcomes and survival rates [7,8,9].
Approximately 90% of malignant neoplasms of the larynx are squamous cell carcinomas and can be graded as well, moderately, or poorly differentiated. Symptoms, treatment, and prognosis of LSCC vary depending on the subsite of onset. LSCC presents challenges due to its proximity to critical structures involved in breathing, speech and swallowing [6]. Supraglottic and subglottic cell carcinoma typically have worse outcomes compared to glottic SCC [10,11,12].
Treatment recommendations vary by tumor site and stage as well as patient factors. Early-stage LSCC (stages I and II) is typically treated with radiotherapy or endoscopic laser surgery in malignant neoplasms of the supraglottic and glottic larynx, which offer high rates of local control while preserving laryngeal function [13]. In contrast, advanced-stage LSCC (stages III and IV) frequently necessitates a multimodal approach, which involves total laryngectomy, chemotherapy, and radiotherapy [14,15,16]. While these aggressive treatments improve survival rates, they profoundly impact quality of life, often resulting in the loss of natural voice and changes to the airway [17]. Advanced laryngeal cancers have shifted from surgery as the gold standard treatment to primarily chemoradiotherapy, driven by clinical trials showing high rates of larynx preservation. However, concerns have arisen about reduced survival rates, and surgical salvage through total laryngectomy remains a viable option for post-radiotherapy recurrences confined to the larynx [18].
Despite advances in management, survival for advanced LSCC remains suboptimal, underscoring the need for improved molecular understanding. Prior studies such as TCGS have identified recurrent mutations in TP53, NOTCH1, FAT1, and KMT2D, but sex-specific and metastasis-specific landscapes remain poorly defined. This study aims to analyze the somatic mutational landscape of LSCC using AACR Project GENIE, focusing on distinctions between primary vs. metastatic tumors and male vs. female patients.
2. Materials and Methods
This study was exempt from the Creighton University institutional review board approval as the database is deidentified and publicly available. The American Association for Cancer Research (AACR) Project Genomics Evidence Neoplasia Information Exchange (GENIE)^®^ database was accessed using the cBioPortal (v16.1-public) online software [19] on 22 July 2024, with clinical data dating back to 2017. Genomic sequencing information from 19 international cancer centers is compiled in the AACR GENIE^®^ database. Only a select number of cancer types include therapeutic response along with clinical outcomes data, but treatment regimens were not recorded for LSCC. Additionally, each participating institution may use different pipelines from each other (and within the same institution). Participating institutions use either unbiased whole genomic/exome sequencing or targeted panels of up to 555 genes.
We queried all patients with head and neck tumors and a pathologic diagnosis of larynx squamous cell carcinoma. The dataset included genomic data (e.g., somatic mutations), histological subtype, as well as clinical characteristics (e.g., race and age). Specific copy number alterations and structural variants were excluded from this analysis. Tumor mutational burden was calculated based on the number of detected somatic mutations. Survival data was not available. Samples with missing data were excluded from the analysis to ensure the integrity of the results. Discrepancies in total numbers across different demographic categories (e.g., ethnicity versus sex) arise because not all participating institutions reported every data field for every patient; samples with missing specific data points were excluded from those specific sub-group analyses. Statistical analyses were conducted using R/R Studio (Version 4.5.2, R Foundation for Statistical Computing, Boston, MA, USA), with significance set at p < 0.05. Continuous variables were reported as means ± standard deviations (SD), and categorical variables were presented as frequencies and percentages. Differences between categorical variables were assessed using the chi-squared test. For comparisons of means between two groups, a two-sided T-test and nonparametric tests, such as the Mann–Whitney U test for non-normally distributed data, were applied. The Benjamini–Hochberg False Discovery Rate (FDR) correction was used to adjust for multiple comparisons.
3. Results
3.1. Larynx Squamous Cell Carcinoma Patients’ Demographics
The larynx squamous cell carcinoma patient demographics are described in detail in Table 1. 135 samples were taken from 130 adult patients. 116 (89.2%) were from males and 19 (14.6%) were from females. 93 (71.5%) patients were White, 11 (8.5%) were Asian, and 4 (3.1%) were Black. 77 (59.2%) samples were of the primary tumor and 51 (39.2%) were from metastasized tumors. Primary tumors had a mutation count ≤3 in 30 (62.5%) samples compared to 18 (37.5%) of metastasized samples. These results are outlined in Table 1.
3.2. Larynx Squamous Cell Carcinoma Top Somatic Mutations
The top mutations detected in this larynx squamous cell carcinoma patient cohort are shown in Figure 1. Briefly, the most common mutations observed were in TP53 (n = 121; 89.6%), KMT2D (n = 37; 27.4%), FAT1 (n = 28; 20.7%), NOTCH1 (n = 28; 20.7%), PIK3CA (n = 25; 18.5%), CDKN2A (n = 20; 14.8%), TERT (n = 18; 13.3%), NSD1 (n = 17; 12.6%), NFE2L2 (n = 12; 8.9%), ROS1 (n = 11; 8.1%), NCOR1 (n = 10; 7.4%), ARID1A (n = 10; 7.4%), PRKDC (n = 9; 6.7%), and FBXW7 (n = 9; 6.7%). Specifically, co-occurrence was observed throughout mutated genes. Of the 25 patients with PIK3CA mutations, 11 (44.0%) had the CDKN2A mutation (p = 0.063).
3.3. Mutation Landscape in Key Genes
TP53 mutations were diverse, with alterations such as Y220C and R273H identified. The allele frequency (AF), representing the proportion of a specific gene variant within a population, demonstrated significant variability among TP53 mutations. Mutations such as R248L (AF = 0.69) and G224C (AF = 0.77) exhibited higher prevalence, indicating their occurrence in a larger proportion of the analyzed samples. Conversely, mutations such as G226R (AF = 0.04) were observed less frequently. Splice site mutations such as X125_splice (AF = 0.92) and nonsense mutations such as E204* (AF = 0.36) were also observed, emphasizing the range of TP53 alterations in larynx squamous cell carcinoma.
3.4. Co-Occurrence and Mutual Exclusivity of Mutations
Of the 34 samples with either KMT2D or PIK3CA mutations, 9 (26.4%) had both mutations, although this did not represent statistically significant co-occurrence. Of the 17 samples that had the NSD1 mutation, 4 (23.5%) had the ROS1 mutation (p = 0.049). Co-KMT2D and TP53 mutations were relatively mutually exclusive (p = 0.018) in larynx squamous cell carcinoma patients.
3.5. Gender Genetic Differences
When stratified by sex, female and male patients demonstrated significant enrichment of specific mutations. Mutations in CDK8 (22.22% vs. 0%; p = 0.011) were exclusively seen in females. Conversely, mutations in ATP8B1 (0% vs. 66.67%; p = 0.013) and EPHB2 (0% vs. 50%; p = 0.024) were exclusively seen in males. Additional mutations such as JAK3 (15.79% vs. 1.72%; p = 0.02), MED12 (27.27% vs. 3.85%; p = 0.02), KMT2B (50% vs. 4.88%; p = 0.034), GLI1 (18.18% vs. 1.30%; p = 0.04), and FGF19 (44.44% vs. 13.85%; p = 0.045) occurred at higher frequencies in female patients when compared to male patients. These results are outlined in Table 2.
3.6. Primary vs. Metastatic Tumors
In this cohort, distinct mutational patterns were observed between primary and metastatic tumors. Among the 77 primary tumor samples, DMD (13.33%; p = 0.049) was identified exclusively in primary samples and absent in all metastatic samples. Additionally, mutations in KMT2D were also observed more frequently in primary samples when compared to metastatic samples (35.29% vs. 13.51%; p = 0.027). Within the 51 metastatic samples, mutations in ATP8B1 (66.67%; p < 0.001), FRK (33.33%; p = 0.038), NRIP1 (33.33%; p = 0.038), and SAMD9L (33.33%; p = 0.038) were identified exclusively in metastatic samples and absent in all primary samples.
In this cohort, among the 77 primary tumor samples, mutations were observed in TP53 (n = 61; 79.2%), KMT2D (n = 18; 23.4%), NOTCH1 (n = 14; 18.2%), PIK3CA (n = 15; 19.5%), FAT1 (n = 7; 9.10%), NSD1 (n = 6; 7.79%), CDKN2A (n = 9; 11.7%), BRCA1 (n = 7; 9.10%), ATM (n = 7; 9.10%), ROS1 (n = 6; 7.79%), and ARID1A (n = 7; 9.10%). In contrast, among the 51 metastatic tumor samples, mutations were observed in TP53 (n = 38; 74.5%), FAT1 (n = 12; 23.5%), TERT (n = 10; 19.6%), PIK3CA (n = 9; 17.6%), NSD1 (n = 7; 13.7%), CDKN2A (n = 8; 15.7%), NOTCH1 (n = 8; 15.7%), HGF (n = 5; 9.80%), KMT2D (n = 5; 9.80%), PRKDC (n = 4; 7.84%), and NCOR1 (n = 2; 3.92%). These results are outlined in Table 3.
4. Discussion
In this study, we aimed to profile the somatic mutational landscape of laryngeal squamous cell carcinoma (LSCC) using the AACR GENIE database, with a particular focus on identifying actionable alterations that can inform personalized medicine strategies. LSCC is characterized by a high prevalence of TP53 mutations (89.6%), followed by KMT2D (27.4%), FAT1 (20.7%), and NOTCH1 (20.7%). These findings reaffirm prior work, including The Cancer Genome Atlas Program (TCGA) analyses, but extend them by examining metastatic samples and sex-based differences that have not been well-characterized in LSCC. Our analysis moves beyond cataloging mutations to interpreting their potential for guiding patient-specific therapies, a cornerstone of personalized medicine that seeks to tailor treatment to the individual molecular characteristics of a tumor.
4.1. Therapeutic Implications of Key Mutations and Pathways
The genomic alterations identified in this cohort underscore the potential for targeted therapeutic interventions in LSCC. Gender-specific variations were also noted, as CDK8 mutations were exclusively present in females, whereas ATP8B1 and EPHB2 were exclusively seen in males. These results are intriguing but must be interpreted cautiously, given the small number of female patients. However, they open an important avenue for personalized medicine, suggesting that optimal treatment strategies may ultimately need to be stratified by sex. Validation in larger and more balanced cohorts will be essential to confirm these potential sex-linked genomic differences. Similarly, distinct mutational patterns emerged between primary and metastatic tumors, with DMD and KMT2D more prevalent in primary tumors, while SAMD9L and ATP8B1 were found in metastases. Because samples were not paired, these differences should be viewed as hypothesis-generating rather than definitive evidence of metastatic drivers. Nevertheless, these findings highlight the critical need for genomic profiling of metastatic sites to guide personalized therapy in advanced disease, as the mutational landscape may evolve from the primary tumor.
Our findings align with previous research identifying TP53 as the most frequently mutated gene in LSCC and a key driver of the poor prognosis and progression of tumors [20]. Disruptions in the gene impair DNA repair, apoptosis, and cell cycle regulation, contributing to aggressive tumor behavior and resistance to conventional therapies. While TP53 mutations have historically been challenging to target directly, they remain a critical biomarker for risk stratification. Developing strategies to counteract the effects of TP53 loss is a major goal of personalized oncology. Compared to TCGA, which primarily included primary tumors, GENIE’s inclusion of recurrent/metastatic samples provides additional insight into disease progression. The Hedberg et al. study described mutational features of metastatic and recurrent HNSCC broadly [21]; however, our work isolates LSCC specifically, identifying SAMD9L and ATP8B1 as candidate metastasis-associated mutations not previously reported in this tumor type. This distinction is vital for developing personalized approaches for patients with metastatic LSCC.
The gender differences observed in CDK8, ATP8B1, and EPHB2 mutations are not well-established in the LSCC literature. Their identification here may suggest unexplored biological pathways influenced by sex, which is a growing area of interest in personalized medicine. Acknowledging these differences could lead to more effective, gender-specific treatment protocols. However, these findings also raise the possibility of false discovery given the limited sample size. Further validation in other datasets will be required to confirm these observations and explore their therapeutic relevance.
In a comprehensive review of parallel sequencing of head and neck squamous cell carcinomas, Nadal et al. confirm the role of TP53 as the pivotal mutation in the profile of conventional head and neck squamous cell carcinomas. Additionally, they also found TP53, FAT1, NOTCH1, KMT2C, and CDKN2A to be the most frequently mutated genes in LSCC [22]. KMT2D mutations highlight the role of chromatin remodeling in LSCC. Prior research identifies KMT2D as a tumor suppressor, where loss-of-function mutations impair transcriptional regulation and promote oncogenesis. This finding aligns with studies demonstrating KMT2D’s role in early tumor development. In a systematic review of KMT2D involvement in the pathogenesis of head and neck cancer, Santos et al. found the gene’s involvement in cell cycle inhibitors leads to the accumulation of DNA damage and the tumor’s aggressive advancement [23]. Due to the high mutational frequency of the KMT2D gene in their review, they assert the strong association of the gene with tumor progression and its potential to serve as a biomarker for predicting immunotherapy response. Our findings of the mutual exclusivity of KMT2D and TP53 mutations can be described in a study by Lee et al. in which they conclude that KMT2D can act as a coactivator of TP53 as part of the ASCOM complex [24]. Loss of KMT2D has been shown to impair TP53 target gene activation, mimicking the effects of TP53 inactivation. Consequently, tumors with KMT2D mutations may not require TP53 mutations to bypass tumor suppressor pathways. Therefore, a plausible explanation of the observed mutual exclusivity could be due to KMT2D tumors inactivating TP53 function indirectly by disrupting chromatin remodeling and reducing accessibility to TP53 target gene promoters. Conversely, TP53 tumors could directly override TP53 transcriptional activity, bypassing the need for functional KMT2D. These findings suggest that LSCC represents distinct molecular subtypes with unique vulnerabilities that should be explored further for targeted therapies. This molecular distinction is fundamental to personalized medicine, suggesting that patients with KMT2D mutations may respond to epigenetic therapies, while those with TP53 mutations might require different strategies.
While most of our results align with existing studies, the unique identification of mutations such as SAMD9L and ATP8B1 in metastatic tumors and gender-specific enrichment of CDK8 and EPHB2 are less commonly reported and may represent new areas for investigation in personalized therapeutics. SAMD9L mutations have been implicated in other cancers as contributors to tumor survival under stress, such as in gastric cancer and myelodysplastic syndrome; however, their role in LSCC metastasis is largely unexplored [25,26]. Similarly, ATP8B1 mutations, associated with lipid metabolism, are rarely discussed in LSCC literature but have been proposed as a novel predictive biomarker in lung squamous cell carcinoma [27]. Although gender differences in cancer genetics are recognized in other malignancies, LSCC-specific studies have not reported these genetic patterns such as the mutations of CDK8 in females and ATP8B1 in males, warranting further investigation to determine if these could serve as sex-specific therapeutic targets or biomarkers.
Some studies report lower TP53 mutation frequency in HPV-positive LSCC [22,28], as the E6 protein from the virus inactivates TP53 functions directly, obviating the need for genetic mutations. On the other hand, HPV-negative tumors are dominated by alterations in tumor suppressor genes like TP53 and CDKN2A as well as oncogenes CCND1 and MYC [29]. This well-established dichotomy is a prime example of personalized medicine, where HPV status is already used to guide treatment and predict prognosis in head and neck cancers.
Our findings comparing primary and metastatic tumors add to the understanding of tumor progression from a personalized medicine perspective. In primary tumors, mutations in the DMD gene contribute significantly to tumor progression due to the loss of dystrophin expression. While altered dystrophin expression leads to the developmental onset of Duchenne muscular dystrophy, it also has been associated with downregulation across various malignancies and enrichment across multiple pathways within transcriptomes of primary tumors [30]. In a study by Jones et al., they describe the pathogenesis of DMD in several primary tumors including sarcomas, leukemias, lymphomas, and melanomas [31]. Similarly in mutations of the KMT2D gene, mutations drive the progression of tumor formation through distinct epigenetic mechanisms. By disrupting its role in chromatin remodeling and gene regulation, these mutations promote genetic instability, increasing susceptibility to further oncogenic changes and altering the tumor microenvironment by fostering immune evasion. Higher frequencies in primary mutations of the KMT2D gene have been highlighted in the literature including studies related to the mutational landscape of primary nasopharyngeal carcinomas and oropharyngeal cancers [32,33]. In metastatic tumors, the exclusive presence of mutations in ATP8B1 and FRK in metastatic samples mirrors recent research on colorectal and breast cancers indicating that these genes play a role in tumor dissemination and metastatic colonization [34,35]. The potential of these mutations to serve as biomarkers for metastatic disease or as therapeutic targets aligns with ongoing research focused on identifying novel molecular markers for the early detection and management of metastasis [36,37,38]. This genomic divergence underscores the importance of serial biopsies and genomic monitoring in patients with advanced disease to tailor therapies to the evolving tumor landscape. However, it is important to note that these findings are exploratory given the lack of paired primary-metastatic samples in the database.
4.2. Current Experimental Therapies and Future Personalized Directions
Several emerging therapies align with the pathways indicated in this study, paving the way for a more personalized approach to LSCC treatment. For TP53 mutations, intramural injections of p-53 and the use of cisplatin in radiation therapy are being explored in clinical trials for LSCC [39,40]. Cisplatin was also being explored in combination with cetuximab, docetaxel, and atezolizumab for targeting mutations in PIK3CA and high-risk HPV-negative cases [41]. The high frequency of mutations in chromatin-modifying genes like KMT2D suggests a potential vulnerability to epigenetic drugs, such as histone deacetylase (HDAC) inhibitors or EZH2 inhibitors, which could be a promising personalized strategy for this patient subset. Some alternate pathways on therapeutics for LSCC include the use of nivolumab, carboplatin, and paclitaxel in the exploration of PDL1 expression, soy isoflavones in the expression of p16, COX-2, VEGF, IL6, p53, and Bcl-xL, and saracatinib on c-Src and downstream signaling molecules STAT3 and STAT5 [42,43,44,45,46,47,48]. Identifying which patients are most likely to benefit from these targeted agents based on their specific mutational profile is a key goal of personalized medicine.
Several limitations must be acknowledged. Participating GENIE institutions used heterogeneous sequencing platforms, ranging from targeted panels to whole-exome sequencing, introducing variability in mutation detection. Additionally, survival and treatment data were not available, limiting our ability to directly correlate genomic findings with clinical outcomes, a crucial step for translating this research into personalized clinical practice. Missing demographic and sample site data (e.g., race available for 108 of 130 patients) further complicates interpretation and explains why denominators vary across analyses. Lastly, the demographic skew towards males and white patients reduces the generalizability of findings across diverse populations.
Despite these limitations, this study provides significant insights into LSCC’s genetic landscape that are highly relevant to the field of personalized medicine. The prevalence of TP53 and other mutations such as KMT2D and NOTCH1 provides valuable insights into tumorigenesis, while distinctions between primary and metastatic tumors reveal potential markers for metastasis that could be used to guide treatment decisions. Furthermore, the mutational differences between genders offer new avenues for developing tailored therapeutic strategies. The study contributes to the growing body of evidence that genomic and epigenetic alterations in LSCC can inform targeted therapy development, moving beyond a one-size-fits-all approach. Future studies should integrate more diverse datasets, including transcriptomic and clinical outcomes, to substantiate these findings and maximize their translational impact.
In summary, this study contributes to the growing body of LSCC genomic research by highlighting both established drivers (TP53, KMT2D) and less characterized findings (ATP8B1, SAMD9L, CDK8). By framing these findings within the context of patient stratification and targeted therapy, this work underscores the immense potential of genomic profiling to usher in a new era of personalized medicine for patients with laryngeal cancer. These results should be interpreted as hypothesis-generating and provide a strong rationale for further studies integrating genomic, transcriptomic, and clinical outcome data to build a comprehensive molecular framework for individualized patient care.
5. Conclusions
This study provides a detailed characterization of the mutational landscape of laryngeal squamous cell carcinoma (LSCC), highlighting critical genetic alterations, particularly in TP53, KMT2D, FAT1, and NOTCH1. Notably, significant genetic heterogeneity exists between primary and metastatic tumors, with mutations in ATP8B1 and SAMD9L prominently associated with metastasis. Additionally, gender-specific genetic variations, including CDK8 mutations in females and ATP8B1 mutations in males, suggest potential avenues for tailored therapeutic strategies. The identification of these molecular signatures contributes substantially to our understanding of LSCC tumorigenesis and progression, supporting the advancement of precision medicine approaches. Future research should integrate comprehensive genomic, transcriptomic, and clinical outcome data to further validate these findings and enhance therapeutic targeting in LSCC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coskun H. Mendenhall W.M. Rinaldo A. Rodrigo J.P. Suárez C. Strojan P. López F. Mondin V. Saba N.F. Shaha A.R. Prognosis of subglottic carcinoma: Is it really worse?Head Neck 20194151152110.1002/hed.2517229947111 · doi ↗ · pubmed ↗
- 2Dizon D.S. Kamal A.H. Cancer statistics 2024: All hands on deck CA Cancer J. Clin.2024748910.3322/caac.2182438230825 · doi ↗ · pubmed ↗
- 3Hoffman H.T. Porter K. Karnell L.H. Cooper J.S. Weber R.S. Langer C.J. Ang K. Gay G. Stewart A. Robinson R.A. Laryngeal cancer in the United States: Changes in demographics, patterns of care, and survival Laryngoscope 200611611310.1097/01.mlg.0000236095.97947.2616946667 · doi ↗ · pubmed ↗
- 4Shephard E.A. Parkinson M.A. Hamilton W.T. Recognising laryngeal cancer in primary care: A large case-control study using electronic records Br. J. Gen. Pract.201969 e 127e 13310.3399/bjgp 19X 70099730692092 PMC 6355262 · doi ↗ · pubmed ↗
- 5Liberale C. Soloperto D. Marchioni A. Monzani D. Sacchetto L. Updates on Larynx Cancer: Risk Factors and Oncogenesis Int. J. Mol. Sci.2023241291310.3390/ijms 24161291337629093 PMC 10454133 · doi ↗ · pubmed ↗
- 6Steuer C.E. El-Deiry M. Parks J.R. Higgins K.A. Saba N.F. An update on larynx cancer CA Cancer J. Clin.201767315010.3322/caac.2138627898173 · doi ↗ · pubmed ↗
- 7Sharma S. Bekelman J. Lin A. Lukens J.N. Roman B.R. Mitra N. Swisher-Mc Clure S. Clinical impact of prolonged diagnosis to treatment interval (DTI) among patients with oropharyngeal squamous cell carcinoma Oral Oncol.201656172410.1016/j.oraloncology.2016.02.01027086482 PMC 4968047 · doi ↗ · pubmed ↗
- 8Morse E. Fujiwara R.J.T. Judson B. Mehra S. Treatment delays in laryngeal squamous cell carcinoma: A national cancer database analysis Laryngoscope 20181282751275810.1002/lary.2724729756382 · doi ↗ · pubmed ↗