Clinical and Prognostic Relevance of BRIP1 Expression in Colorectal Cancer: Evidence from TCGA and Korean Cohorts
Dongbin Park, Yu-Ran Heo, Jae-Ho Lee

TL;DR
This study explores how BRIP1 gene expression relates to colorectal cancer outcomes, suggesting it could be a useful biomarker for predicting patient survival and disease progression.
Contribution
The study provides new evidence linking BRIP1 expression levels to clinicopathological features and survival outcomes in colorectal cancer patients.
Findings
Low BRIP1 expression is significantly associated with poor overall survival in both rectal and colon cancers.
BRIP1 expression correlates with clinicopathological features like gender, lymphatic invasion, and tumor stage in colon cancer.
Lower BRIP1 expression is linked to elevated CEA levels and unfavorable clinical outcomes in CRC patients.
Abstract
Background and Objectives: BRCA1-interacting protein C-terminal helicase 1 (BRIP1) encodes a member of the RecQ DEAH helicase family and interacts with the BRCT repeats of breast cancer type 1 (BRCA1). It also participates in DNA damage repair and tumor suppression; thus, its mutations may be associated with an increased risk of several cancers, including fallopian tube and ovarian cancer. Recent research has explored whether BRIP1 dysregulation also contributes to the development and progression of other malignancies. This study investigated the clinical and prognostic value of BRIP1 in colorectal cancer (CRC). Materials and Methods: We first analyzed The Cancer Genome Atlas (TCGA) dataset to evaluate the prognostic significance of BRIP1 mRNA expression in CRC. BRIP1 expression was subsequently examined in tumor tissues from 60 CRC patients, and its associations with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
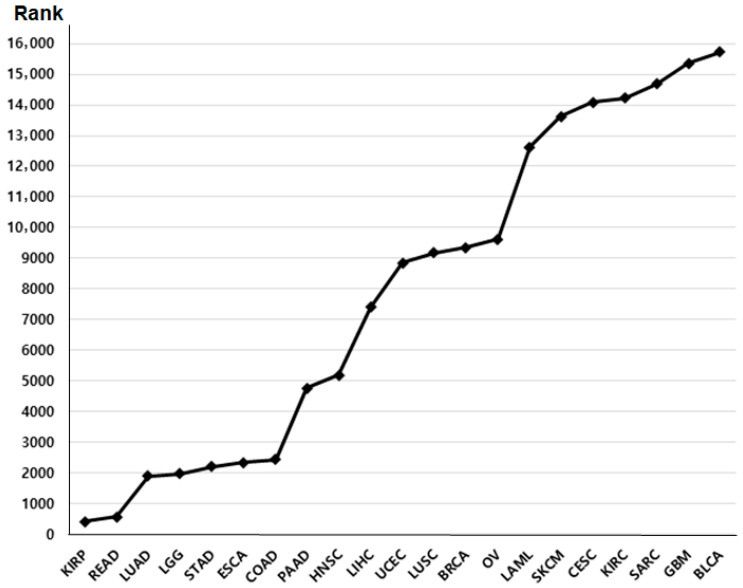 Figure 1
Figure 1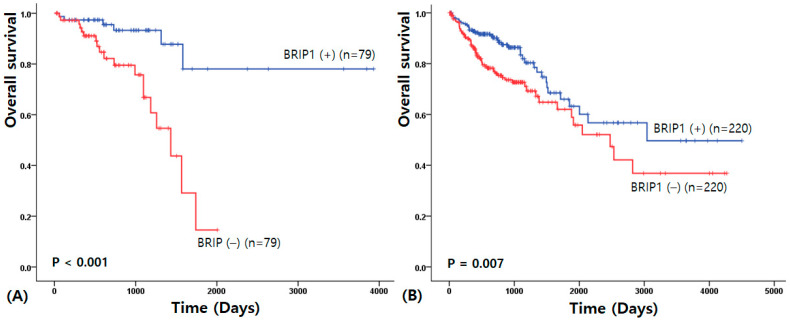 Figure 2
Figure 2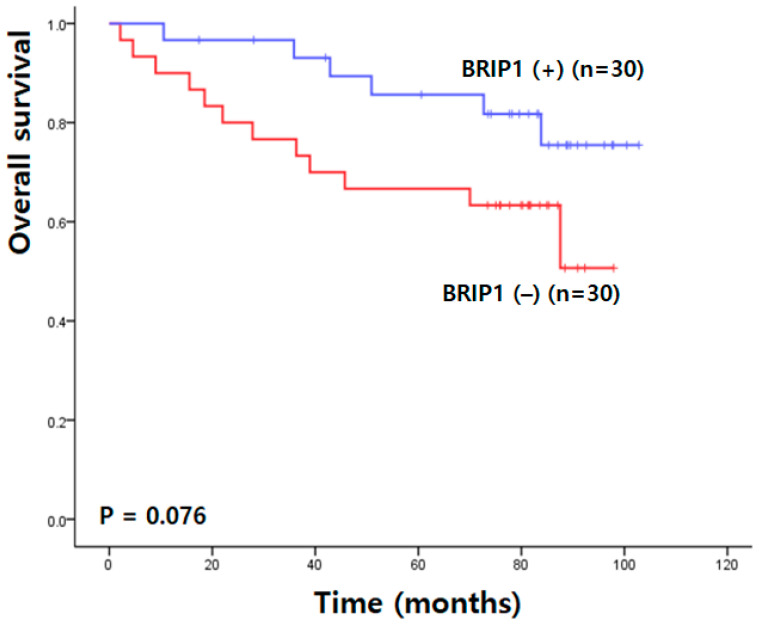 Figure 3
Figure 3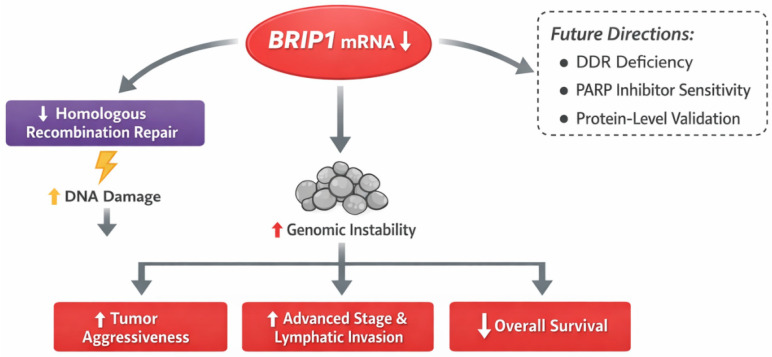 Figure 4
Figure 4- —National Research Foundation of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBRCA gene mutations in cancer · Genetic factors in colorectal cancer · PARP inhibition in cancer therapy
1. Introduction
Colorectal cancer (CRC) ranked as the third most frequently diagnosed cancer globally in 2022, accounting for 9.6% of newly diagnosed malignancies. It was also the second leading cause of cancer-related death, responsible for 9.3% of global cancer deaths [1]. Both genetic predispositions and lifestyle-related factors—such as consumption of processed foods and high-sugar beverages and obesity—substantially contribute to CRC development [1]. While the majority of CRC cases arise sporadically, 20–30% demonstrate hereditary components, most linked to high-penetrance genetic syndromes, such as Lynch syndrome (3–4%) and familial adenomatous polyposis (around 1%) [2].
The adenoma–carcinoma sequence represents the most widely recognized pathway in CRC tumorigenesis and involves the sequential accumulation of mutations in key regulatory genes such as APC, K-ras, and p53 [3]. Despite extensive research, colorectal tumorigenesis remains incompletely understood, as it results from complex interactions among numerous genes and signaling pathways [4,5]. In particular, dysregulation of DNA damage response (DDR) pathways and genomic instability have been increasingly recognized as important contributors to CRC progression and clinical heterogeneity. Consequently, identifying DDR-related biomarkers that can refine prognostic prediction and potentially guide therapeutic strategies has become an important priority in CRC research.
BRCA1-interacting protein C-terminal helicase 1 (BRIP1), also referred to as FANCJ or BACH1, is encoded by gene located on chromosome 17q22 and belongs to the RecQ DEAH helicase family [6,7]. It interacts directly with BRCA1 and is essential for DNA damage repair and tumor suppression [8]. Alterations in BRIP1 that impair its helicase function have been identified in patients with early-stage breast cancer, and several of these missense variants are considered to confer increased susceptibility to breast cancer [9]. Accordingly, BRIP1 is classified as a moderate-penetrance breast cancer susceptibility gene [10]. Beyond breast cancer, BRIP1 mutations have been implicated in multiple other malignancies, including cervical, ovarian, and prostate cancers [7,9,10,11,12,13,14]. Although BRIP1 has been primarily investigated in the context of germline susceptibility, emerging studies indicate that altered expression of DDR-related genes at the tumor level may influence cancer aggressiveness and patient outcomes, even in sporadic cancers. However, the biological and clinical significance of BRIP1 expression in colorectal cancer remains poorly characterized, and data regarding its prognostic relevance are limited. To address this critical knowledge gap, the present study aimed to systematically evaluate the clinical relevance and prognostic significance of BRIP1 mRNA expression in CRC by integrating transcriptomic data from The Cancer Genome Atlas (TCGA) with analyses of tumor tissues obtained from an independent cohort of 60 CRC patients [15,16]. We hypothesized that reduced BRIP1 expression reflects impaired DDR function in colorectal tumors and is associated with more aggressive clinicopathological features and unfavorable clinical outcomes.
2. Materials and Methods
2.1. TCGA Data Analysis
We retrieved primary datasets from The Cancer Genome Atlas (TCGA) portal “http://cancergenome.nih.gov/, accessed on 10 June 2025”. Normalized RNA sequencing (RNA-seq) expression data (TPM values) and corresponding clinical information were obtained from the TCGA-COAD and TCGA-READ cohorts. This database provides p-value rankings indicating the prognostic significance of BRIP1 expression across multiple cancer types (Figure 1). Among these cancers, colon and rectal cancers exhibited the most significant associations; therefore, these two cancer types were selected for further in-depth analysis. A total of 440 patients with colon cancer (TCGA-COAD) and 158 patients with rectal cancer (TCGA-READ) were included in the clinical correlation and survival analyses. BRIP1 expression values were log2-transformed for analysis, and patients were stratified into high- and low-expression groups based on the median BRIP1 expression level. Overall survival was defined as the time interval between the date of surgery and the date of death.
2.2. CRC Patient Analysis
A total of 60 patients (mean age, 63.6 ± 10.5 years; range, 34–83 years) who underwent colorectal cancer (CRC) surgery at Dongsan Medical Center (Daegu, Republic of Korea) between April 2008 and January 2010 were included in this study. Tumor tissues and paired adjacent non-cancerous tissues were obtained from the Keimyung Human Bioresource Bank. All patients were fully informed of the study purpose, and written informed consent was obtained from each participant. The study protocol was approved by the Institutional Review Board of Keimyung University Dongsan Medical Center (No. 2020-07-027).
Clinicopathological information for all patients was reviewed. Individuals with a history of other malignancies or those who had received preoperative treatments—including chemotherapy, radiofrequency ablation, or transarterial chemoembolization—were excluded. Tumor staging was determined according to the 7th edition of the American Joint Committee on Cancer (AJCC) staging system, based on the characteristics of the primary tumor (T), regional lymph node involvement (N), and distant metastasis (M).
Total RNA was extracted from the tumor and paired non-malignant samples using TRIzol reagent (Molecular Research Center Inc., Cincinnati, OH, USA) [17], and RNA quantity and purity were assessed by measuring absorbance at 260 and 280 nm using a NanoDrop 1000 spectrophotometer (Thermo Scientific, Wilmington, DE, USA). Complementary DNA (cDNA) was synthesized from 2 μg of total RNA using M-MLV reverse transcriptase (Promega, Madison, WI, USA). Quantitative PCR (qPCR) was performed using SYBR Green-based detection with specific primers for BRIP1 as follows: forward 5′-CTTACCCGTCACAGCTTGCTA-3′ and reverse 5′-CACTAAGAGATTGTTGCCATGCT-3′. GAPDH was used as an internal control. RT-qPCR was then carried out on the CFX Connect™ Real-Time PCR Detection System (Bio-Rad, Hercules, CA, USA) using the following program: UNG incubation at 50 °C for 2 min, polymerase activation at 95 °C for 20 s, followed by 40 cycles of denaturation at 95 °C for 30 s and annealing/extension at 60 °C for 30 s. The relative expression level of BRIP1 mRNA was calculated using the 2^−ΔCt^ method, where ∆Ct is the difference between the threshold cycles (Ct) values of the GAPDH and BRIP1 genes. All reactions were performed in triplicate, and five serially diluted control samples were included in each experiment to ensure assay reliability
2.3. Statistical Analysis
Statistical analyses were performed using SPSS software (version 25.0; IBM SPSS, Armonk, NY, USA). Patients were stratified into high- and low-expression groups based on the median BRIP1 expression level. Tumor staging was classified according to the 7th edition of the AJCC staging system. Clinicopathological characteristics—including age, sex, carcinoembryonic antigen (CEA) level, and pathological TNM stage—were compared using the chi-square test. Spearman’s correlation analysis was used to evaluate the association between BRIP1 expression and clinical variables in rectal cancer. Univariate survival analysis was conducted using Kaplan–Meier survival curves and the log-rank test. Overall survival was defined as the interval from diagnosis to death. A p-value of <0.05 was considered statistically significant.
3. Results
3.1. BRIP1 Expression in the Cancer Genome Atlas (TCGA) Data
To evaluate the clinical significance of BRIP1 expression, patients with rectal and colon cancer were stratified into high- and low-expression subgroups based on the median BRIP1 expression level (Table 1 and Table 2). In rectal cancer, a higher BRIP1 expression was significantly associated with younger age (59.5% vs. 41.0%, p = 0.021). Male sex (55.2% vs. 42.9%), absence of lymphatic invasion (53.7% vs. 40.4%) and absence of venous invasion (52.0% vs. 37.1%), were more frequently observed in the high BRIP1 expression group; however, these associations did not reach statistical significance. No significant correlations were observed between BRIP1 expression and other clinicopathological variables.
In colon cancer, BRIP1 expression demonstrated significant associations with female (55.6% vs. 45.3%, p = 0.031), absence of lymphatic invasion (56.0% vs. 40.8%, p = 0.003), low CEA level (57.1% vs. 42.2%, p = 0.020), lower pathological stage (p = 0.022), no M stage (50.8% vs. 36.1%, p = 0.035), lower N stage (p = 0.002), microsatellite instability (MSI) status (p < 0.001), and anatomic tumor location (p = 0.030).
Overall survival analysis indicated that BRIP1 expression had significant prognostic value in both rectal and colon cancer. In rectal cancer, patients with high BRIP1 expression exhibited markedly longer overall survival compared with those with low expression (3324.42 ± 269.84 vs. 1305.64 ± 98.40 days; χ^2^ = 13.94; p < 0.001) (Figure 2A). Similarly, in colon cancer, high BRIP1 expression was associated with improved survival outcomes (2975.55 ± 222.49 vs. 2421.43 ± 206.15 days; χ^2^ = 7.304; p = 0.007) (Figure 2B).
3.2. BRIP1 Expression in CRC Patients
BRIP1 expression was analyzed in 60 CRC tissues, and its expression level was not significantly different between tumor and paired adjacent non-tumorous tissues (p = 0.57). When normalized as the tumor-to-non-tumor expression ratio, the mean BRIP1 expression level was 2.71 ± 1.62.
To identify the clinicopathological significance of BRIP1, patients were stratified into high- and low-expression groups based on the median BRIP1 expression value. The clinicopathological characteristics associated with BRIP1 mRNA expression in CRC patient tissues are summarized in Table 3. Higher BRIP1 expression was significantly associated with lower carcinoembryonic antigen (CEA) levels (57.1% vs. 42.2%, p = 0.028), whereas no other clinicopathological variables showed statistically significant associations.
Kaplan–Meier survival analysis demonstrated that patients with higher BRIP1 expression tended to have improved overall survival compared with those with lower expression; however, this difference did not reach statistical significance (90.80 ± 4.65 vs. 70.40 ± 6.58 months; χ^2^ = 3.14; p = 0.076) (Figure 3).
4. Discussion
In this study, we evaluated the clinical relevance and potential prognostic association of BRIP1 expression in colorectal cancer using TCGA datasets and an independent cohort of 60 CRC patients. The primary objective of this study was to investigate the clinical significance of BRIP1 at the mRNA expression level by directly comparing large-scale transcriptomic data with real-world patient samples. To our knowledge, this is the first study to comprehensively examine BRIP1 expression in both rectal and colon cancers and to integrate RNA expression profiling from patient tissues.
As revealed through TCGA data, a higher BRIP1 expression was significantly associated with younger age in rectal cancer. In colon cancer, BRIP1 expression showed significant associations with several clinicopathological parameters, including gender, lymphatic invasion, CEA levels, pathological stage, M stage, N stage, MSI status, and anatomic tumor location. Kaplan–Meier survival analyses demonstrated that lower BRIP1 expression was associated with poorer overall survival in both colon and rectal cancers, supporting a prognostic association. Importantly, these findings suggest a correlational rather than a strictly independent prognostic role, indicating that BRIP1 expression may reflect underlying tumor biology rather than act as a standalone prognostic determinant. In our CRC patient cohort, BRIP1 mRNA levels were significantly associated with the serum CEA level, although other clinicopathological variables did not exhibit statistically significant relationships. Although higher BRIP1 expression tended to be associated with improved overall survival, this trend did not reach statistical significance—likely due to the small sample size. Nonetheless, the directionality of survival trends was consistent with TCGA findings, supporting the hypothesis that reduced BRIP1 expression may be associated with more aggressive tumor behavior. Taken together, these findings suggest that transcript-level alterations of BRIP1 alone may capture clinically meaningful prognostic information in colorectal cancer.
From a biological perspective, BRIP1 has emerged as a key component of the DNA damage response (DDR) machinery, functioning as a helicase that cooperates with BRCA1 in homologous recombination-mediated DNA repair. Dysregulation of BRIP1 can lead to genomic instability, a hallmark of colorectal cancer progression [18]. Recent genomic and transcriptomic studies have reported BRIP1 mutations or reduced expression in subsets of sporadic CRC, particularly those exhibiting defective homologous recombination or chromosomal instability signatures [19]. These observations support the concept that BRIP1 may influence colorectal tumor biology not only through genetic alterations, but also through transcriptional dysregulation detectable at the mRNA level. Collectively, these findings position BRIP1 mRNA expression as a biologically relevant and clinically informative molecular feature, while also providing a rationale for future integrative multi-omics investigations.
This study has several limitations. First, the analyzed TCGA cohort was relatively small compared to other cancer datasets, underscoring the need for larger, multi-institutional studies with multivariate analyses. Second, although this study intentionally focused on mRNA expression to ensure consistency and comparability across large datasets and patient cohorts, transcriptomic data may not fully reflect BRIP1 protein abundance or functional activity due to post-transcriptional or post-translational regulation. Future validation at the protein level, using immunohistochemistry, Western blotting, or proteomic approaches, will therefore be essential. Third, while our findings suggest a prognostic association, functional studies are required to elucidate the mechanistic role of BRIP1 in colorectal cancer progression. Such studies should include in vitro and in vivo models involving BRIP1 knockdown or overexpression, DNA repair capacity assays, and pathway-based analyses.
Finally, future investigations integrating genomic alterations, MSI status, proteomic profiles, and therapeutic response data may clarify whether BRIP1 serves as a surrogate marker of DDR deficiency and a potential predictor of response to DNA damage-targeted therapies, such as PARP inhibitors (Figure 4). Such integrative approaches may ultimately establish BRIP1 as a clinically actionable biomarker in colorectal cancer.
5. Conclusions
This study demonstrated that BRIP1 expression is significantly associated with key clinicopathological features and overall survival in colorectal cancer based on TCGA analyses. These findings were further supported by the BRIP1 expression patterns observed in patient tumor tissues. Collectively, our results suggest that BRIP1 expression may have potential prognostic relevance in colorectal cancer; however, these findings should be interpreted as exploratory. Additional studies integrating larger clinical cohorts, comprehensive protein-level validation, and mechanistic experiments are required to elucidate the biological roles of BRIP1 and to determine its applicability in clinical decision-making and therapeutic development.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Whiffin N. Hosking F.J. Farrington S.M. Palles C. Dobbins S.E. Zgaga L. Lloyd A. Kinnersley B. Gorman M. Tenesa A. Identification of susceptibility loci for colorectal cancer in a genome-wide meta-analysis Hum. Mol. Genet.2014234729473710.1093/hmg/ddu 17724737748 PMC 4133584 · doi ↗ · pubmed ↗
- 3Conlin A. Smith G. Carey F.A. Wolf C.R. Steele R.J. The prognostic significance of K-ras, p 53, and APC mutations in colorectal carcinoma Gut 2005541283128610.1136/gut.2005.06651415843421 PMC 1774675 · doi ↗ · pubmed ↗
- 4Wang Q.Q. Zhou Y.C. Zhou Ge Y.J. Qin G. Yin T.F. Zhao D.Y. Tan C. Yao S.K. Comprehensive proteomic signature and identification of CDKN 2A as a promising prognostic biomarker and therapeutic target of colorectal cancer World J. Clin. Cases 2022107686769710.12998/wjcc.v 10.i 22.768636158487 PMC 9372836 · doi ↗ · pubmed ↗
- 5Sameer A.S. Colorectal cancer: Molecular mutations and polymorphisms Front. Oncol.2013311410.3389/fonc.2013.0011423717813 PMC 3651991 · doi ↗ · pubmed ↗
- 6Cantor S.B. Guillemette S. Hereditary breast cancer and the BRCA 1-associated FANCJ/BACH 1/BRIP 1Future Oncol.2011725326110.2217/fon.10.19121345144 PMC 3109611 · doi ↗ · pubmed ↗
- 7Song H. Ramus S.J. Kjaer S.K. Hogdall E. Dicioccio R.A. Whittemore A.S. Mc Guire V. Hogdall C. Jacobs I.J. Easton D.F. Tagging single nucleotide polymorphisms in the BRIP 1 gene and susceptibility to breast and ovarian cancer P Lo S ONE 20072 e 26810.1371/journal.pone.000026817342202 PMC 1800910 · doi ↗ · pubmed ↗
- 8Ouhtit A. Gupta I. Shaikh Z. BRIP 1, a potential candidate gene in development of non-BRCA 1/2 breast cancer Front. Biosci.2016828929810.2741/e 76726709662 · doi ↗ · pubmed ↗