Growth Differentiation Factor 15 as a Link Between Obesity, Subclinical Atherosclerosis, and Heart Failure: A Systematic Review
Raluca-Elena Alexa, Alexandr Ceasovschih, Bianca Codrina Morărașu, Andreea Asaftei, Mihai Constantin, Alexandra-Diana Diaconu, Anastasia Balta, Raluca Ecaterina Haliga, Victorița Șorodoc, Laurențiu Șorodoc

TL;DR
This review explores how GDF-15, a cytokine, connects obesity, heart failure, and atherosclerosis through shared metabolic and inflammatory pathways.
Contribution
The paper synthesizes evidence suggesting GDF-15 as an integrative biomarker for cardiometabolic risk.
Findings
GDF-15 levels are associated with increased atherosclerotic burden in multiple populations.
GDF-15 reflects overlapping pathways of inflammation, oxidative stress, and metabolic dysregulation.
Current evidence supports GDF-15's potential as a prognostic biomarker for cardiovascular risk.
Abstract
Background and Objectives: Obesity, heart failure (HF), and atherosclerosis have common pathways, including chronic inflammation, immune cells activation, and metabolic disturbances. These pathways often coexist and overlap, increasing cardiometabolic risk. Growth differentiation factor 15 (GDF-15) is an emerging cytokine linked to inflammation, oxidative stress, and metabolic dysregulation, which are common pathways between heart failure, obesity and atherosclerosis. Beyond its established prognostic value in cardiovascular diseases (CVD) and HF, recent evidence suggests that GDF-15 may also reflect subclinical atherosclerosis, potentially improving early risk stratification in obese and HF populations. The aim of this review is to synthesize current evidence on the association between GDF-15 and markers of subclinical atherosclerosis, and to evaluate whether GDF-15 may serve as an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
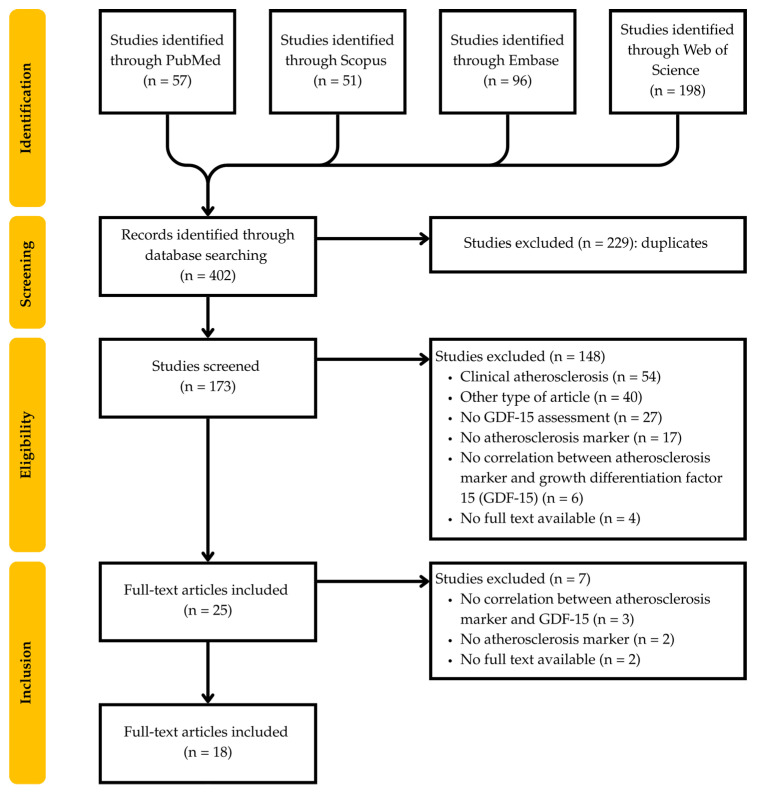 Figure 1
Figure 1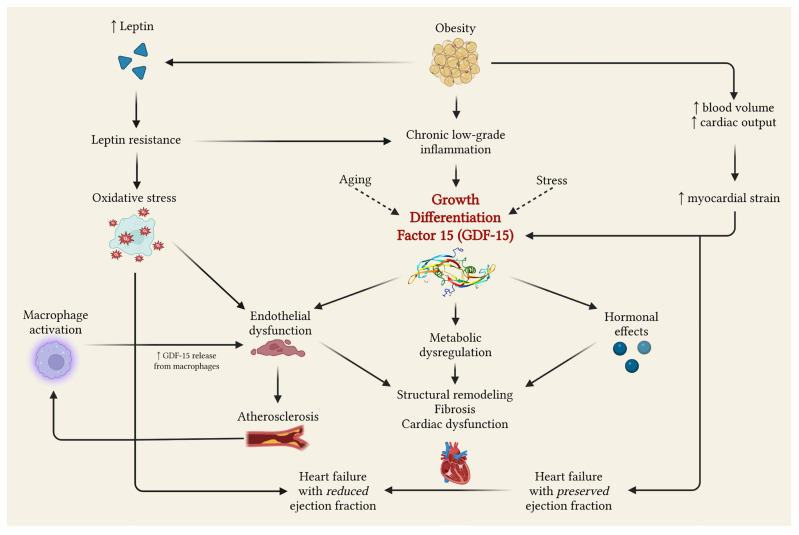 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGDF15 and Related Biomarkers · IL-33, ST2, and ILC Pathways · Kruppel-like factors research
1. Introduction
Obesity, subclinical atherosclerosis, and heart failure (HF) share common pathways influenced by chronic inflammation, oxidative stress, endothelial dysfunction, and metabolic disturbances. Increased adiposity promotes insulin resistance, activates immune and inflammatory mediators, and induces atherogenic dyslipidemia, ultimately contributing to metabolic syndrome and end-organ dysfunction [1,2,3].
Worldwide, cardiovascular diseases (CVD) remain the leading cause of mortality and morbidity, with obesity rising dramatically among individuals in their third to fifth decade of life. This trend contributes to the increasing burden of cardiometabolic disorders and supports the need for early prevention and the identification of subclinical disease states [4,5].
In recent years, GDF-15 has emerged as a promising biomarker, as it is involved in many of the pathological mechanisms underlying obesity, HF, and atherosclerosis [6,7]. GDF-15 is a stress-responsive cytokine, triggered by inflammation, mitochondrial dysfunction, hypoxia, insulin resistance, and endothelial injury [8,9]. Moreover, elevated GDF-15 levels have a strong prognostic value for cardiometabolic disorders and all causes mortality, in addition to traditional biomarkers [8,10,11,12].
Although several studies have explored the relationship between GDF-15 and obesity, atherosclerosis, or heart failure, no study has simultaneously assessed all three conditions together. This is a knowledge gap, as these disorders frequently coexist and share common pathways.
The aim of this review is to synthesize recent evidence on the relationship between GDF-15 and different subclinical atherosclerosis markers, and to evaluate whether GDF-15 may represent an integrative biomarker reflecting shared pathways between atherosclerosis, obesity, and heart failure.
2. Methods
We conducted a systematic review of the literature regarding the association between GDF-15 and subclinical atherosclerosis. We registered the review protocol in PROSPERO under the registration number CRD420251267457, and developed our study strategy based on the Population, Intervention, Comparison, Outcome, and Study design strategy, using the PRISMA statement for systematic reviews [13].
2.1. Research Question and Search Strategy
We conducted systematic literature research in PubMed, Scopus, Embase, and Web of Science, from database inception to 30 November 2025. Search strategies included MeSH and Emtree controlled vocabulary terms, free text terms, such as “growth differentiation factor-15”, ankle-brachial index, intima media thickness, coronary artery calcium score, and subclinical atherosclerosis. We used search syntax such as (“GDF-15” OR “growth differentiation factor-15”) AND (“ankle brachial index” OR “ ABI”), (“GDF-15” OR “growth differentiation factor-15”) AND (“coronary artery calcium score” OR “CACS”), (“GDF-15” OR “growth differentiation factor-15”) AND (“intima-media thickness” OR “ IMT”), (“GDF-15” OR “growth differentiation factor-15”) AND (“subclinical atherosclerosis”, and obtained 57 articles from PubMed, 51 articles from Scopus, 96 articles from Embase, and 198 articles from Web of Science.
2.2. Inclusion Criteria
The inclusion criteria were original full-text articles published until 30 of November 2025, conducted on human populations, including randomized controlled trials, clinical trials, and cross-sectional, observational, and cohort studies that studied the association between GDF-15 serum levels and subclinical atherosclerosis.
2.3. Exclusion Criteria
The exclusion criteria included case report articles, reviews, systematic reviews, meta-analyses, letters to the editors, articles published in languages other than English, or articles from pre-clinical studies. We also excluded studies conducted in patients younger than 18 years old.
2.4. Study Selection
Studies that met eligibility criteria (1) included human participants; (2) evaluated the correlation between GDF-15 serum levels and subclinical atherosclerosis marker; (3) provided statistical results such as p-values. Studies were excluded if they (1) were other types of articles (such as reviews, meta-analyses, abstracts, posters, etc.); (2) provided insufficient data; (3) did not correlate GDF-15 with a subclinical atherosclerosis marker; (4) included patients with clinical atherosclerosis; (5) did not assess GDF-15 serum levels.
The study selection process is detailed in Figure 1. From 402 studies initially identified, 229 were duplicates, and 155 were excluded based on exclusion criteria. We identified 18 eligible studies, including 14 cross-sectional studies, 3 cohort studies, and 1 case–control study, covering metabolic disorders, chronic inflammatory diseases, HIV cohorts, elderly or general population, and other disorders such as chronic kidney disease or beta-thalassemia.
2.5. Data Extraction
Two independent researchers screened the articles to identify correlations between at least one subclinical atherosclerosis marker and GDF-15 serum levels, and, additionally, for correlations between GDF-15 and body mass index, obesity, metabolic profile, heart failure, and cardiovascular risk. Other relevant information regarding the association between obesity, heart failure, and subclinical atherosclerosis was noted. This process was standardized by including information about the study design, study population, aim, inclusion and exclusion criteria, and outcomes. If any disagreements occurred, they were settled by a third reviewer.
2.6. Risk of Bias Assessment
Risk of bias was assessed using the Joanna Briggs Institute (JBI) appraisal tool [14], namely the JBI Checklist for analytical cross-sectional studies, JBI Checklist for case–control studies, and JBI Checklist for cohort studies. All the items were judged as Yes/No/Unclear/Not applicable, according to the instructions. The purpose of this assessment was to evaluate the methodological quality, the validity of biomarker and imaging measurements, identification and control of confounding, and statistical adequacy.
Table 1, Table 2 and Table 3 summarize the risk of bias assessment for included studies. Most of the studies clearly defined the eligibility criteria, described the study population, used validated methods for GDF-15 serum levels measurements, and standardized protocols for subclinical atherosclerosis assessment. Regarding possible bias, some studies had partial or no adjustment for confounders, leading to some uncertainty. Furthermore, no major concerns were identified regarding exposure or outcome, meaning that the principal source of bias relates to residual confounding rather than measurement error.
2.7. Strategy of Data Synthesis
After the selection process, 18 studies were included in this systematic review. A narrative synthesis of the findings was performed, focusing on the association between GDF-15 serum levels and subclinical atherosclerosis in human population.
Table 4 summarizes the correlation between GDF-15, subclinical atherosclerosis, and, where available, correlations between GDF-15 and heart failure or cardiovascular risk, metabolic profile (obesity or lipid profile), and other findings relevant to our aim.
To our knowledge, no study has directly evaluated the association between GDF-15 and subclinical atherosclerosis in patients with obesity and heart failure. Therefore, the results regarding this population are indirect and derive from studies in which GDF-15 also correlates with body mass index or heart failure. These findings may support the hypothesis of a potential role of GDF-15 involvement in subclinical atherosclerosis in patients with obesity and heart failure. However, this extrapolation should be interpreted with caution due to the lack of dedicated studies.
3. Results
Table 4 summarizes the clinical studies regarding GDF-15 association with subclinical atherosclerosis in patients with metabolic inflammatory, infectious, and renal disorders, along with elderly and general population. The subclinical atherosclerosis markers were ankle-brachial index, coronary artery calcium score, carotid intima-media thickness, and atherosclerotic plaque measurement.
3.1. Results from Studies
3.1.1. Metabolic Disorders
Across metabolic conditions, GDF-15 was associated with multiple markers of subclinical atherosclerosis, such as ABI, CIMT, or FIMT. Typically, these populations exhibit visceral adiposity which induces insulin resistance and chronic low-grade inflammation, these mechanisms triggering GDF-15 expression. Moreover, the relationship between GDF-15 and different metabolic parameters such as HOMA-IR or steatosis score, connects GDF-15 to metabolic disturbances beyond adiposity [17,20]. Since within these cohorts, GDF-15 appears to capture metabolic and vascular stress, it could be a promising biomarker for early vascular disease diagnosis in patients with risk for cardiometabolic complications.
3.1.2. Chronic Inflammatory Diseases
In inflammatory diseases, the main cause of atherosclerotic disease is endothelial dysfunction, which is the result of different mechanisms. In patients with chronic obstructive pulmonary diseases, elevated GDF-15 levels may be explained by intrathoracic mechanics and hypoxia [24]. In contrast, chronic inflammation primarily triggers for GDF-15 expression in psoriasis [21], and immunosuppression contributes in rheumatoid arthritis [26], leading to endothelial dysfunction and pro-atherogenic processes. Furthermore, in antiphospholipid syndrome, the main mechanism is represented by impaired nitric oxide release, which eventually leads to endothelial dysfunction [27]. Overall, GDF-15 reflects vascular injury induced through different pathways.
3.1.3. Human Immunodeficiency Virus (HIV) Cohorts
In patients with HIV, the studied cohorts were heterogenous. In younger patients, with low cardiovascular risk, GDF-15 was not associated with atherosclerosis [15,33], whereas in older, metabolically compromised, where GDF-15 was associated with plaque volume [25]. The differences between groups could be explained by age, antiretroviral therapy duration, metabolic health, and systemic inflammation, which are more frequent in older patients and modulate the GDF-15-atherosclerosis association in HIV populations. Thus, GDF-15 appears useful primarily in high-risk HIV patients.
3.1.4. General Population
In the general population and elderly patients, GDF-15 was frequently associated with atherosclerotic plaque [16,18,19,23] and a coronary artery calcium score [22,30]. Moreover, genetic variants were associated with atherosclerotic plaque and risk of T2DM [19], and age was correlated with N-terminal pro-B-type natriuretic peptide [16,23,30]. These results suggest that mitochondrial dysfunction, oxidative stress, and systemic inflammation induced by aging are responsible for GDF-15 increased levels, being a good predictor for mortality and atherosclerotic events in the elderly.
3.1.5. Other Diseases
In patients with chronic kidney disease (CKD), chronic inflammation status and uremic toxicity lead to vascular injury, being associated with CIMT. Furthermore, GDF-15 reflects a combination between metabolic, vascular, and uremic stress, being correlated with cardiovascular risk [31].
In patients with beta-thalassemia, the association between CIMT and GDF-15 levels was significant. Although pathogenic mechanisms differ from typical cardiometabolic disease, oxidative stress leads to endothelial dysfunction and vascular inflammation, stimulating GDF-15 expression.
3.2. Effect Direction and Magnitude
In most of the studies, the association between GDF-15 and markers of subclinical atherosclerosis was positive, and directly correlated with atherosclerotic burden [16,17,18,19,20,21,22,23,24,25,26,27,30,31,32]. This pattern was observed in patients with metabolic disorders, chronic inflammatory diseases, the general population, elderly individuals, and patients with chronic kidney disease, supporting the relationship between systemic inflammation and endothelial dysfunction. In contrast, in patients with HIV and younger individuals, the association was weak or absent, indicating the fact that the effect depends on the underlying condition. In studies where adjustment for confounders was possible, the positive association was mostly preserved, but decreased, further suggesting that confounders contribute to, but do not explain, the results.
3.3. Heterogeneity
The correlation between GDF-15 concentrations and markers of subclinical atherosclerosis showed a significant variability among different cohorts. The association was strongest in elderly patients, in those with chronic inflammatory disorders, and those with chronic kidney disease, where GDF-15 correlated with CIMT, atherosclerotic plaque, or coronary calcification. For these situations, the association remained statistically significant after adjustment for traditional risk factors, indicating the cumulative influence of inflammation, oxidative stress, and metabolic disturbances [18,19,22,23,24,25,27,30,32].
In metabolic disorders, GDF-15’s association with subclinical atherosclerosis was present, but inconsistent, since this association tended to be stronger in patients with advanced metabolic disturbances, and weaker in younger patients or those with better metabolic control [17,20,34].
In contrast, in HIV cohorts, which were generally younger patients with lower cardiovascular risk, the association was weaker [25] or absent [15,33]. After adjustment for confounders, the previously positive association was attenuated or lost, suggesting that in lower-risk settings, GDF-15 may reflect background systemic stress rather than atherosclerotic process directly.
Taken together, these findings support the idea that the association between GDF-15 and subclinical atherosclerosis is context-dependent, being most evident in situations involving inflammation, metabolic imbalance, vascular aging, or impaired renal function, all of these being risk factors for atherosclerosis.
Interpretation of statistical analysis must consider methodological heterogeneity. First, GDF-15 was measured using ELISA in most studies, but also other types of immunoassay platforms [15,16,18,21,22,27] or PCR [19]. Second, the results were reported different units, and data were analyzed using absolute value, log-transformed scales, or tertiles. Third, the atherosclerosis assessment varied, and the imaging protocols were different. All these factors limit direct comparability of effect data, despite consistent directional trends.
3.4. Evidence Gaps
Despite GDF-15 relevance in cardiometabolic disorders, several gaps still remain regarding its implication in the triad of obesity–heart failure–subclinical atherosclerosis. First, no study simultaneously evaluated its implication in the triad mentioned above, which is the main interest for this review. Therefore, the results are indirect and derived from different and heterogeneous populations, and the conclusions are not easy to generalize.
Second, the majority of studies are cross-sectional, which limit causality. Moreover, the incremental predictive value of GDF-15 beyond established cardiovascular risk factors has been evaluated in only few cohorts, and the results are not conclusive.
Third, the heterogeneity of studies, reflected in differences in vascular imaging protocols, statistical analysis, or endpoints, makes it more difficult to compare study results, and contribute to discordant findings. Confounders such as age, renal impairment, chronic inflammation, metabolic dysfunction, and cardiovascular risk remain key determinants in GDF-15’s involvement in both cardio–reno–metabolic disorders and atherosclerosis.
Finally, few studies differentiated between heart failure phenotypes when evaluating GDF-15’s involvement, particularly in patients with obesity, where it may have greater diagnostic and prognostic significance.
Overall, there is a need for dedicated studies, with standardized protocols for vascular assessment, clear endpoints, and statistical analysis to clarify whether GDF-15 represents a marker of systemic stress or an integrative biomarker, with independent clinical utility in cardiometabolic disorders.
4. Discussion
4.1. GDF-15 Physiopathological Implications
GDF-15 is a member of the transforming growth factor-β (TGF-β) superfamily and is involved in several biological processes, including oxidative stress response, weight management, inflammation, and cancer progression [7,35]. Circulating levels of GDF-15 increase with age, suggesting its role as a systemic biomarker of age-related diseases, including cardiometabolic conditions [8,10,36,37] (Figure 2).
4.1.1. Tissue Expression and Stress Responsiveness
GDF-15 is expressed in various tissues, including the heart, lung, colon, liver, kidney, vascular smooth muscle cells, and endothelial cells. Under stress condition, its expression increases, highlighting its role as a stress-response cytokine and its utility as a diagnostic, prognostic, and potentially therapeutic biomarker [8,38,39].
4.1.2. Molecular Regulation
At the molecular level, GDF-15 transcription is regulated through pathways, such as p53, EGR-1, strongly linking it to cellular damage, senescence, and immunomodulation [11,36].
Serum levels are typically low in young and healthy individuals, but they rise progressively with age, modulating the subclinical development of cardiometabolic disorders. Moreover, GDF-15 exerts autocrine, endocrine, and paracrine effects depending on the tissue involved and the stage of disease [10,36,37].
4.1.3. GFRAL-RET Axis and Metabolic Effects
According to the studies, GDF-15’s effect is mediated through a complex formed by the glial cell-derived neurotrophic factor family receptor alpha-like (GFRAL) and a tyrosine kinase receptor (RET), located in area postrema and nucleus tractus solitarius. Through this pathway, GDF-15 exerts an anorexigenic effect, reducing appetite and food intake, which confers a central role in influencing body weight and energy expenditure [40,41]. Murine studies have demonstrated that GFRAL-RET agonism improves metabolic parameters, while its antagonism leads to weight gain and metabolic dysfunctions [8,42].
4.2. Diagnostic and Prognostic Role of GDF-15
Although elevated GDF-15 levels are not specific to a single condition, the molecule is considered a valuable biomarker of global disease burden and systemic stress rather than a disease-specific indicator [8,10]. Its strongest evidence base lies in CVD, where increased levels are found in hypertension, atherosclerosis, heart failure, especially with preserved ejection fraction, and peripheral artery disease. In these conditions, GDF-15 serves as a prognostic biomarker, and is independently associated with cardiovascular events and mortality beyond traditional risk markers [9,36,43,44]. However, its diagnostic value is limited due to confounders, such as age, renal impairment [30,31], metabolic disturbances, and inflammation [21,27], which decrease its specificity for individual conditions.
Because its expression is stress-related and amplified by inflammation, elevated levels are also encountered in patients with obesity, insulin resistance, type 2 diabetes mellitus (T2DM), or steatotic liver disease [9,34,36]. Moreover, GDF-15 levels rise with aging, and are strongly correlated with frailty and physical function decline in older adults [11,37,45]. Accordingly, recent research describes GDF-15 as a molecule situated at the crossroads of inflammation, metabolism, and aging. Its utility in risk stratification and phenotyping is particularly enhanced when integrated into multimarker strategies along with biomarkers such as NT-proBNP or hs-CRP, improving patient classification, and therefore supporting its prognostic value rather than diagnostic. [8,10,11,12,30],
4.3. Possible Mechanisms Between Atherosclerosis, Heart Failure and Obesity
Obesity induces chronic low-grade inflammation, which increases the secretion of proinflammatory cytokines such as tumor necrosis factor α (TNF-α), and chemokines, such as GDF-15. These molecules induce endothelial dysfunction and insulin resistance, perpetuating the inflammatory state and driving immunological dysfunction through activation of immune system cells [2,46,47,48].
Hemodynamically, obesity increases blood volume and cardiac output, contributing to left ventricular hypertrophy and diastolic dysfunction, features of HF with preserved ejection fraction (HFpEF). I would like to rephrase it: Furthermore, obesity leads to structural heart changes and HF with reduced ejection fraction (HFrEF) by activating neurohormonal pathways, especially through leptin [46,49]. Paradoxically, in spite of the elevated leptin levels in obese patients, leptin resistance further contributes to molecular mechanisms in oxidative stress, endothelial dysfunction, and chronic inflammation. All these promote and sustain the atherosclerotic process [50,51].
In atherosclerosis, macrophage activation facilitates the uptake of oxidized low-density lipoprotein and secretion of GDF-15, contributing to the atherosclerotic plaque formation and to the local inflammation [8,46,52]. As a consequence, GDF-15 is released from macrophages within atherosclerotic plaques and correlates with vascular inflammation, promoting plaque progression and stenosis [1,48]. Despite inconsistencies in published findings, most studies suggest an association between elevated GDF-15 and subclinical or progressive atherosclerosis, as well as with cardiovascular outcomes [8].
Chronic HF represents the final common pathway of hemodynamic overload, metabolic disturbances, and inflammation, often originating from obesity and atherosclerosis. All these modifications promote structural remodeling, fibrosis, and progressive cardiac dysfunction [53,54]. According to contemporary studies, GDF-15 is a strong predictor of HF severity and mortality, reflecting hypoxia, oxidative stress, systemic inflammation, and mechanical strain [1,18]. Beyond its prognostic role, GDF-15 exerts immunomodulatory effects and may attenuate the maladaptive hypertrophy response [16,18].
In summary, GDF-15 integrates the major sources of cardiometabolic stress. It highlights metabolic and inflammatory response associated with obesity [2,46], vascular inflammation of atherosclerotic plaques [1,3], and mechanical, oxidative, and hypoxic stress driven to chronic HF progression [18,53]. Thus, GDF-15 can be considered a biomarker capable of quantifying the interaction between obesity, atherosclerosis, and HF.
4.4. GDF-15 as Pathophysiological Mediator vs. Risk Biomarker
Since there are several mechanisms that could link obesity, heart failure, and atherosclerosis through GDF-15, an important question remains: should GDF-15 be interpreted as a risk biomarker or an active mediator in this triad?
All the mechanisms explained before position GDF-15 as a molecule capable of influencing vascular remodeling, plaque development, and myocardial structure and function. However, clinical evidence supports GDF-15 more strongly as a risk marker than a mediator. In most studies included in this review, the association between GDF-15 and subclinical atherosclerosis decreases after adjustment for confounders. Moreover, it is difficult to establish whether GDF-15 elevation precedes vascular dysfunction or represents a primary driver leading to it.
To move from association to causality, evidence of temporality, dose–response relationships, consistency across populations and methods, and ideally genetic phenotyping is required, since modulation of GDF-15 signaling could be influenced by the genetic profile.
Based on the current data available, GDF-15 appears to more likely be an integrative stress biomarker, capturing the influence of inflammation, metabolic dysregulation, endothelial dysfunction, and renal dysfunction. Whether it can act as a mediation in the triad of obesity–heart failure–atherosclerosis remains an open question that requires further studies.
4.5. Confounders
All results about the relationship between GDF-15 and subclinical atherosclerosis should be interpreted taking into account several important confounders. As we mentioned before, these include age, renal impairment, endothelial dysfunction, inflammation, and cumulative comorbidity burden. Table 5 summarizes the main confounders and the statistical results after adjustment (Table 5).
Age is one of the strongest determinants of GDF-15 serum levels, and correlates with endothelial dysfunction, and chronic comorbidities commonly associated with aging. Reduced renal function also increases GDF-15 serum concentration, particularly in patients with chronic kidney disease. In this population, uremia, inflammation, and malnutrition may explain the association between atherosclerosis and increased levels of GDF-15 [31].
Metabolic status plays an important role. Obesity, insulin resistance, diabetes, and fatty liver disease are positively associated with GDF-15 serum levels, reflecting metabolic and vascular stress, and endothelial dysfunction [18,19,21,24]. Additionally, frailty and chronic systemic disease also increase GDF-15 concentrations, independently of other confounders. Finally, in patients with HIV, antiretroviral treatment, along with anti-inflammatory agents or cardiometabolic medications, such as SGLT2 inhibitors, influence GDF-15 expression, but the results are inconsistent across studies [15,25,33].
After adjustment for confounders, the strength of the association between GDF-15 and atherosclerosis diminishes, and in some cases the statistical significance is lost [21,25,27]. Consistent, comprehensive confounder adjustment is mandatory in future studies, to ensure more accurate results and clinical interpretation.
4.6. Clinical Implications
Current evidence suggests that GDF-15 may serve as a global risk stratification and prognosis marker rather than a specific diagnostic marker. Elevated GDF-15 levels correlate with cardiometabolic risk, inflammation, and endothelial dysfunction and are linked to vascular disease. However, the inconsistent results limit at this moment its use in clinical practice, even after adjusting for confounders. GDF-15 is likely more effective when used alongside other biomarkers rather than alone. Moreover, the lack of longitudinal studies hinders the assessment of GDF-15’s diagnostic role for specific disorders. Further studies should focus on its role in specific populations, and assess its role in predicting the risk and treatment strategy.
4.7. Limitations
Across all included studies, the most common limitations were the predominance of cross-sectional designs, the use of small or highly specific samples, insufficient adjustment for confounders, and incomplete cardiovascular or metabolic evaluation, all of which may interfere with the results (Table 6). Several studies relied on self-reported medical histories, introducing measurement bias. Additionally, variation in imaging techniques contributes to heterogeneity, while differences in body composition across populations limited generalizability.
The heterogeneity across studies results from the differences in population characteristics, age, cardiovascular risk, and comorbidity burden. Methodological heterogeneity arose from differences in study design, imaging protocols applied to evaluate subclinical atherosclerosis, and statistical adjustment for confounders, especially renal function, systemic inflammation, malignancy, and metabolic factors.
In chronic inflammatory diseases, disease activity itself may influence circulating GDF-15, limiting the capacity to estimate the exact contribution of inflammation to GDF-15-atherosclerosis relationship.
In HIV cohorts, key variables such as viremia, antiretroviral therapy, and metabolic syndrome status were inconsistently reported. Many participants were relatively young and without CVD, reducing the probability of detecting GDF-15-atherosclerosis association.
Studies in beta-thalassemia and CKD on hemodialysis included small, highly specific samples, reducing external validity. In CKD, malnutrition status may elevate GDF-15, complicating interpretation.
In general population cohorts, most sources of bias included limited age ranges and voluntary enrollment, reducing sample representativeness. Missing information regarding BMI and HF association with GDF-15 limited the adjustment for confounders.
Taken together, these limitations restrict the capacity to determine causality and prevent a complete assessment of the role of GDF-15 across the triad of obesity, subclinical atherosclerosis, and HF.
4.8. Future Perspectives
To our knowledge, there is no study in the literature that has assessed GDF-15 involvement in subclinical atherosclerosis among patients with obesity and heart failure. Future research should aim to clarify whether GDF-15 serves as a biomarker that quantifies cardiometabolic stress across obesity and HF, and whether it can enhance early detection of subclinical atherosclerosis. Furthermore, investigations should integrate standardized vascular imaging, clinical evaluation of symptoms and comprehensive metabolic, inflammatory, and cardiac phenotyping.
The relationship between GDF-15 and HF, especially HFpEF in the context of obesity, requires focused investigation, as metabolic inflammation and myocardial strain may independently influence GDF-15 expression. In addition, molecular studies should examine how GDF-15 links mitochondrial dysfunction, endothelial damage, and neurohormonal activation. Given the increasing significance of the GFRAL-RET pathway, interventional studies targeting this axis may elucidate whether modulation of GDF-15 signaling provides therapeutic benefits or enhances diagnostic precision.
The development of multimarker panels including GDF-15, along with natriuretic peptides and inflammatory or metabolic biomarkers, may improve early detection of high-risk phenotypes. Also, more diverse and representative populations covering multiple races, age groups, and cardiometabolic phenotypes, are essential for improving external validity and understanding population-specific patterns.
5. Conclusions
Obesity, heart failure, and subclinical atherosclerosis are linked through pathogenic pathways primarily driven by inflammation, oxidative stress, endothelial damage, and metabolic disturbances. GDF-15 integrates signals from all these pathways, indicating its potential role in cardiometabolic disorder assessment. Clinical evidence establishes a correlation between GDF-15 and subclinical atherosclerosis in specific clinical context; however, no research links GDF-15 to HF, obesity and subclinical atherosclerosis.
Despite the heterogeneity and limitations of research due to the studies’ designs, cohorts, and inadequate cardiometabolic evaluation, the overall findings endorse GDF-15 as a possible biomarker for global cardiometabolic stress. Its capacity to detect metabolic, vascular, and cardiac anomalies indicates a possible use in detecting patients at elevated risk for concurrent obesity-related CVD.
Additional prospective studies are required to validate the clinical use of GDF-15 in quantifying the relationship between obesity, heart failure, and subclinical atherosclerosis, as well as to assess its significance in individualized risk estimation and disease prevention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Asrih M. Wei S. Nguyen T.T. Yi H. Ryu D. Gariani K. Overview of Growth Differentiation Factor 15 in Metabolic Syndrome J. Cell. Mol. Med.2023271157116710.1111/jcmm.1772536992609 PMC 10148061 · doi ↗ · pubmed ↗
- 2Manta E. Iliakis P. Fragoulis C. Leontsinis I. Stamoulopoulos I. Chrysohoou C. Tsioufis K. Tracking Pathways Linking Obesity with Heart Failure Nutrients 202517125010.3390/nu 1707125040219007 PMC 11990613 · doi ↗ · pubmed ↗
- 3Dronkers J. Van Veldhuisen D.J. Van Der Meer P. Meems L.M.G. Heart Failure and Obesity J. Am. Coll. Cardiol.2024841666167710.1016/j.jacc.2024.07.01639415402 · doi ↗ · pubmed ↗
- 4Koskinas K.C. Van Craenenbroeck E.M. Antoniades C. Blüher M. Gorter T.M. Hanssen H. Marx N. Mc Donagh T.A. Mingrone G. Rosengren A. Obesity and Cardiovascular Disease: An ESC Clinical Consensus Statement Eur. Heart J.2024454063409810.1093/eurheartj/ehae 50839210706 · doi ↗ · pubmed ↗
- 5Ng M. Fleming T. Robinson M. Thomson B. Graetz N. Margono C. Mullany E.C. Biryukov S. Abbafati C. Abera S.F. Global, Regional, and National Prevalence of Overweight and Obesity in Children and Adults during 1980–2013: A Systematic Analysis for the Global Burden of Disease Study 2013 Lancet 201438476678110.1016/S 0140-6736(14)60460-824880830 PMC 4624264 · doi ↗ · pubmed ↗
- 6Vila G. Riedl M. Anderwald C. Resl M. Handisurya A. Clodi M. Prager G. Ludvik B. Krebs M. Luger A. The Relationship between Insulin Resistance and the Cardiovascular Biomarker Growth Differentiation Factor-15 in Obese Patients Clin. Chem.20115730931610.1373/clinchem.2010.15372621164037 · doi ↗ · pubmed ↗
- 7Desmedt S. Desmedt V. De Vos L. Delanghe J.R. Speeckaert R. Speeckaert M.M. Growth Differentiation Factor 15: A Novel Biomarker with High Clinical Potential Crit. Rev. Clin. Lab. Sci.20195633335010.1080/10408363.2019.161503431076013 · doi ↗ · pubmed ↗
- 8Tian T. Liu M. Little P.J. Strijdom H. Weng J. Xu S. Emerging Roles of GDF 15 in Metabolic and Cardiovascular Diseases Research 20258083210.34133/research.083240837873 PMC 12361751 · doi ↗ · pubmed ↗