Efficacy of Specific Probiotic Strains in Subtypes of Irritable Bowel Syndrome: Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abdulrahman Saud Almalki, Norah Yhya Jaafari, Norah Ghalib Aldossari, Anwar Ayed Alharbi, Abdulrahman Abdullah Alrdeeni, Alanoud Abdullah Alshareef, Abdulrahman Abed Al-subhi, Ammar Faisal Alsubhi, Muath Salem Alsubhi, Abdullah Almaqhawi

TL;DR
This study finds that specific probiotic strains can effectively reduce symptoms of irritable bowel syndrome, improving quality of life without significant side effects.
Contribution
This paper provides a meta-analysis showing the efficacy and safety of probiotics across different subtypes of IBS.
Findings
Probiotics significantly reduced intestinal discomfort and IBS severity scores.
Probiotics showed a clinically significant improvement compared to placebo.
Probiotics were well tolerated with no increase in adverse events.
Abstract
Background and Objectives: The purpose of this systematic review and meta-analysis is to assess the patient’s quality of life, as well as the safety and effectiveness of different probiotic strains in treating IBS symptoms such as IBS-C, IBS-D, IBS-M, and IBS-U. Additionally, we contrast the side effects of probiotics that are single-strain and multi-strain. Materials and Methods: PRISMA criteria were followed in the conduct and reporting of this study. The protocol for this review (CRD420251120965) was entered into PROSPERO. RCTs comparing probiotic usage to placebo or usual therapy in adult IBS patients were found using four online databases: PubMed, Google Scholar, Ovid Medline, and the Cochrane Library. Review Manager was used for data synthesis and statistical analysis. Results: After screening 660 records, 16 randomized, double-blind, placebo-controlled trials with 2823 IBS…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
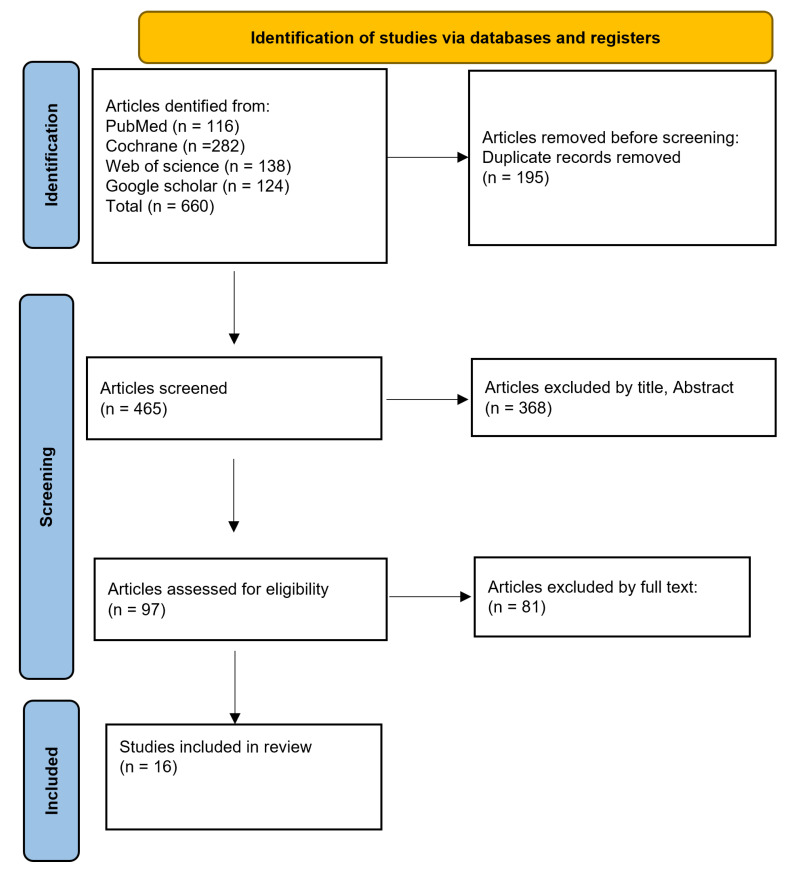 Figure 1
Figure 1 Figure 2
Figure 2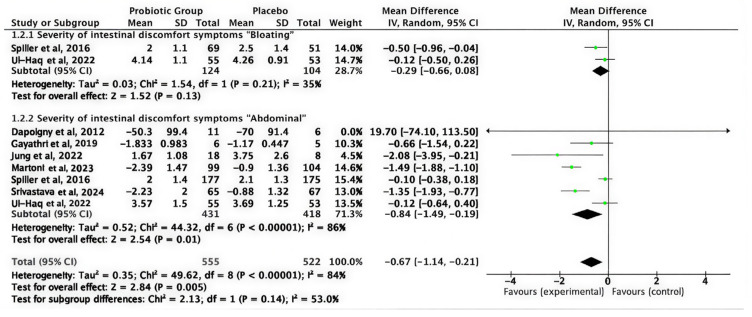 Figure 3
Figure 3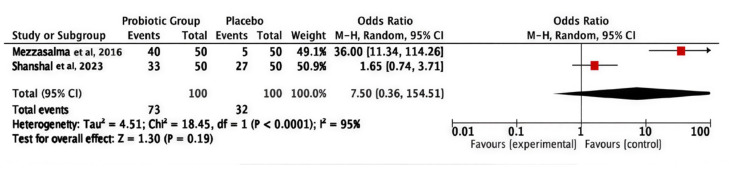 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7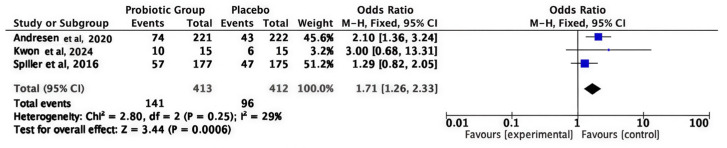 Figure 8
Figure 8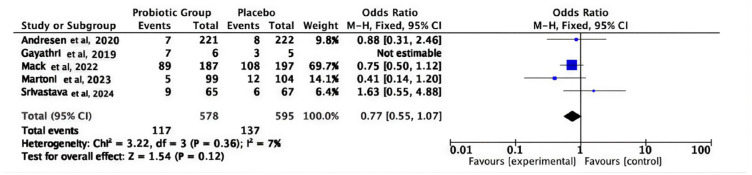 Figure 9
Figure 9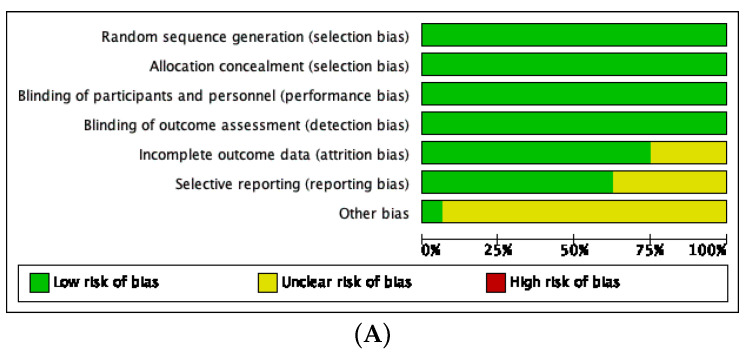 Figure 10
Figure 10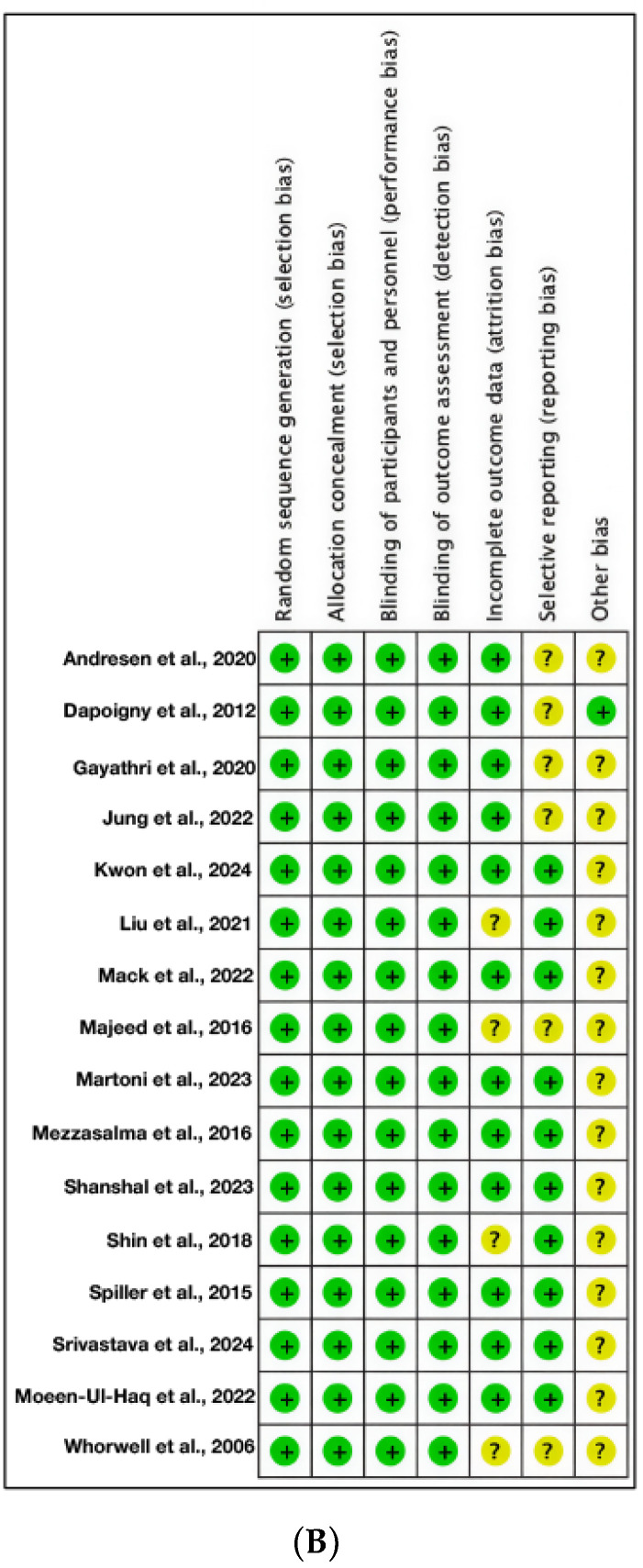 Figure 11
Figure 11- —King Faisal University in Saudi Arabia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal motility and disorders · Probiotics and Fermented Foods · Gut microbiota and health
1. Introduction
Irritable bowel syndrome (IBS) is a widely prevalent, chronic functional gastrointestinal disorder characterized by abdominal discomfort, including bloating, alterations in bowel habits, and recurrent abdominal pain [1]. This syndrome significantly affects patients’ health-related quality of life and imposes a substantial burden on healthcare systems worldwide [2]. Despite its high prevalence, the multifactorial etiology of IBS encompassing abnormalities in gastrointestinal motility, visceral hypersensitivity, alterations in gut microbiota, psychological comorbidities such as anxiety and depression, genetic predisposition, and sex-specific factors remains incompletely understood [3,4]. Central to the pathophysiology of IBS is a dysregulation of the gut–brain axis, which explains the frequent association of IBS with mood disorders and emphasizes the need for comprehensive, multidisciplinary management approaches [5].
Globally, the prevalence of IBS varies depending on the diagnostic criteria and population demographics. Some meta-analytical studies have indicated an overall prevalence of approximately 14.1%, with a female predominance (odds ratio 1.49) and psychological factors like stress playing significant contributory roles [6,7]. Regionally, prevalence estimates may differ, with rates reported as high as 20.7% in Saudi Arabia [8]. Diagnosis is primarily clinical, based on symptom criteria established by the Rome IV consensus, with IBS subtyped into four subgroups: constipation-predominant (IBS-C), diarrhea-predominant (IBS-D), mixed (IBS-M), and finally unclassified (IBS-U), which informs personalized management strategies [9,10].
Current treatment modalities, including dietary modification, pharmacotherapy, and behavioral interventions, are limited by suboptimal efficacy, variable patient response, and the risk of adverse effects [11,12]. Typically, dietary changes require careful supervision to prevent nutritional imbalances, as well as pharmacological agents that target isolated symptoms rather than addressing the overall manifestations of IBS [12]. All of these limitations necessitate exploration into alternative therapeutic modalities.
Probiotics, defined as live microorganisms which, when administered in adequate amounts, confer health benefits to the host, have gained interest as potential modulators of the gut microbiota aiming to restore microbial homeostasis, enhance mucosal barrier function, reduce inflammation, and modulate the gut–brain axis [13,14]. Specific probiotic strains, including Bifidobacterium bifidum, Lactobacillus plantarum, Lactobacillus rhamnosus GG, and Bifidobacterium longum, as well as multi-strain formulations, have demonstrated therapeutic potential, particularly in patients with moderate-to-severe IBS [14,15,16].
However, the wide heterogeneity in clinical trial designs, probiotic strains, dosages, administration durations, and outcome measures complicates the interpretation of efficacy [17,18,19,20,21,22,23]. Most importantly, the existing systematic reviews and meta-analyses often do not stratify effects according to IBS subtypes, and limited long-term safety data constrain the development of evidence-based guidelines [24,25]. This highlights a critical research gap concerning the identification of strain-, dose-, and subtype-specific probiotic efficacy and safety profiles.
Moreover, this systematic review and meta-analysis aim to rigorously evaluate the efficacy and safety of specific probiotic strains in managing distinct IBS subtypes, including IBS-C, IBS-D, IBS-M, and IBS-U, to establish evidence-based recommendations for personalized probiotic therapy. In line with this aim, the objectives of the review are to assess the effect of defined probiotic strains on global IBS symptom severity, including abdominal pain, bloating, and stool irregularities; evaluate the impact of probiotic interventions on IBS-related quality of life metrics; compare the therapeutic efficacy of single-strain versus multi-strain probiotic formulations; determine the influence of probiotic dosage and duration of treatment on clinical outcomes; synthesize safety data, including adverse events and treatment discontinuation rates associated with probiotic use in IBS patients; and explore subtype-specific responses to probiotics to identify optimal strain–subtype matching.
2. Materials and Methods
2.1. Registration and Protocol
This study was conducted and reported according to the Preferred Reporting Items (PRISMA) guidelines for systematic review and meta-analyses (Supplementary Materials Table S1) [26]. This review had been registered as a protocol on PROSPERO (CRD420251120965), which outlines our objective, methodology, and approach for our criteria [27]. Ethical approval and patient consent were not required as all the analyses were performed using previously published studies.
2.2. Search Strategy and Information Source
A literature review was conducted using four electronic databases as stated in our protocol: PubMed, Google Scholar, Web of Science, and Cochrane Library, with no restrictions applied to the publication date. The search strategy was constructed using the following key components: (“irritable bowel syndrome” OR “IBS” OR “spastic colon” OR “irritable colon” OR “functional bowel disorder”) AND (“probiotics” OR “probiotic therapy” OR “Lactobacillus acidophilus” OR “Lactobacillus rhamnosus” OR “Lactobacillus casei” OR “Lactobacillus plantarum” OR “Lactobacillus reuteri” OR “Lactobacillus salivarius” OR “Bifidobacterium infantis” OR “Bifidobacterium longum” OR “Bifidobacterium breve” OR “Bifidobacterium bifidum” OR “Bifidobacterium lactis” OR “Saccharomyces boulardii” OR “Streptococcus thermophilus” OR “Enterococcus faecium” OR “Bacillus coagulans” OR “Escherichia coli Nissle”) AND (“efficacy” OR “effectiveness” OR “outcomes”) AND (“randomized controlled trial” OR “RCT”). Furthermore, we extended our search by reviewing previously published systematic reviews and examining their reference lists to identify any RCTs that may have been missed during the initial literature search. We conducted the literature search and independently screened the retrieved articles for eligibility.
2.3. Eligibility Criteria
The studies included in our review met the following criteria for transparency and consistency with our protocols: they were randomized controlled trials (RCTs), controlled clinical trials, cohort studies (prospective or retrospective), or case-control studies. Participants were adults (≥16 years) diagnosed with IBS based on Rome II, III, or IV criteria. Each intervention involved clearly defined probiotic strains, used either as single-strain or multi-strain formulations, with a comparator group receiving placebo, standard care, or another specific probiotic formulation. Studies reporting clinical outcomes related to IBS symptoms, with a minimum duration of 4 weeks for probiotic intervention, were included, provided there was full-text availability in English. Studies were excluded if they were non-randomized, involved participants under 16 years of age, used undefined probiotic formulations, lacked a comparator group, had insufficient data, or were animal or in vitro studies, as were non-English publications.
2.4. Study Selection Process
The initial database search yielded 660 results. Following the title and abstract screening process, 195 duplicate entries were removed from the remaining 465 articles, resulting in 97 articles for further evaluation. The full-text review phase led to the selection of 97 eligible studies, which met the established inclusion criteria for data extraction and analysis. From these, 16 randomized controlled trials (RCTs) were selected for data extraction as they met the predefined criteria for inclusion.
2.5. Data Extraction and Outcome Measures
Two reviewers independently extracted data using a standardized form. The extracted data encompassed study characteristics (e.g., lead author, publication year, country, and study design), participant demographics, diagnostic criteria (Rome II, III or IV), probiotic treatment details (including strain, dosage, formulation, and duration), comparison groups, and documented IBS symptom outcomes. To ensure consistency in outcome measurement, only studies that assessed symptom severity using the IBS-Severity Scoring System (IBS-SSS) were pooled using the mean difference (MD). Studies employing different symptom scales were not combined with IBS-SSS outcomes. Any discrepancies between reviewers were resolved through mutual agreement.
2.6. Risk of Bias Assessment
Study quality was assessed using the Cochrane Risk of Bias (ROB 1) tool in RevMan 5.4, covering seven domains: random sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and other bias. Each domain was rated as having low, unclear, or high risk [28].
2.7. Statistical Analysis and Data Synthesis
Data synthesis and statistical analyses were performed using Review Manager (RevMan, Version 5.4; The Cochrane Collaboration, Oxford, UK) [29]. For continuous outcomes, pooled mean differences (MDs) and corresponding 95% confidence intervals (CIs) were calculated. MD was used only when all included studies within an outcome employed the same measurement scale (e.g., IBS-SSS). If future analyses require pooling studies using different scales, standardized mean difference (SMD) would be applied. For dichotomous outcomes, pooled odds ratios (ORs) with 95% CIs were estimated. A random-effects model (DerSimonian–Laird method) was applied when heterogeneity was substantial, while a fixed-effect model (Mantel–Haenszel method) was used for homogeneous data. Statistical heterogeneity among studies was assessed using the I^2^ statistic, with thresholds of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. A p-value < 0.10 for the Chi-squared test indicated significant heterogeneity.
3. Results
3.1. Literature Search
A total of 660 records were initially retrieved. After removing 195 duplicates, title and abstract screening excluded an additional 368 records. This process left 97 articles for full-text evaluation. Upon thorough assessment, 16 studies met all inclusion criteria and were incorporated into the final review (Figure 1).
3.2. Baseline Characteristics of Included Patients and Summary
Sixteen randomized, double-blind, placebo-controlled clinical trials were performed, encompassing 2823 patients diagnosed with irritable bowel syndrome (IBS). The study was conducted in Korea, Italy, India, Germany, and South Korea, mostly involving individuals aged 16 to 70 years. The IBS subtypes varied between trials, with most focusing on constipation-predominant (IBS-C) or diarrhea-predominant (IBS-D) forms, categorized according to Rome II, III or IV criteria. The number of male participants varied from 8 to 119 whilst female participants ranged from 18 to 317. All interventions involved the administration of oral probiotics, predominantly in capsule form, employing either single-strain or multi-strain formulations at daily dosages ranging from 5 × 10^9^ to 1 × 10^10^ CFU, administered once daily for a period of 4 to 8 weeks. The baseline demographic and clinical characteristics were comparable between the treatment and control groups across the studies, as illustrated in Table 1.
Based on our included randomized controlled trials, various probiotic strains exhibited notable effectiveness in mitigating symptoms of IBS, with differing impacts among IBS subtypes. Lacticaseibacillus rhamnosus IDCC 3201 and several multispecies formulations (e.g., L. acidophilus, L. reuteri, L. plantarum, L. rhamnosus, B. lactis) markedly alleviated IBS-C symptoms, especially abdominal bloating, pain, and bowel habit satisfaction, while improving the quality of life and modulating gut microbiota composition. In cases of IBS-D, various strains of Lactiplantibacillus plantarum (APsulloc 331261 GTB1, Jeju, Republic of Korea, CCFM8610 Jiangnan University Culture Collection Center (CCFM), Wuxi, China) and Lactobacillus gasseri BNR17 consistently alleviated symptom severity—particularly abdominal pain, distension, and diarrhea—while enhancing stool consistency, perceived stress, and quality of life, alongside beneficial alterations in microbiota and metabolic profiles. Bifidobacterium-based therapies (e.g., B. longum CECT 7347, B. infantis 35624, heat-inactivated B. bifidum MIMBb75) exhibited extensive symptom alleviation across IBS subtypes, enhancing abdominal pain, bloating, stool consistency, and anxiety, while being well tolerated. Saccharomyces cerevisiae CNCM I-3856 enhanced stomach discomfort and stool consistency across all subtypes, but one experiment indicated benefits mostly in IBS-C. In contrast, L. plantarum 299v, LCR35, and bacterial lysates produced variable or subtype-restricted advantages, as shown in Table 2.
3.3. Safety and Efficacy Outcomes
3.3.1. IBS-Severity Scoring System (IBS-SSS)
Pooled analysis of three studies showed that probiotics significantly decreased the IBS-SSS compared with placebo (MD: −93.92; 95% CI (−133.11 to −54.73); p < 0.00001), indicating a significant improvement in overall symptom severity. Pooled studies under the random effect model were heterogeneous (I^2^ = 71%), suggesting variation among probiotic strains or IBS subtypes. These results support a robust overall therapeutic effect of probiotics in alleviating IBS symptom burden, as shown in Figure 2.
3.3.2. Intestinal Discomfort Symptoms
A pooled analysis of nine studies evaluating distinct intestinal discomfort symptoms indicated that probiotics significantly alleviated overall intestinal discomfort compared to placebo (MD = −0.67; 95% CI (−1.14 to −0.21); p = 0.005). The pooled studies under the random effects model were heterogeneous (I^2^ = 84%). Subgroup analysis indicated a reduction in abdominal pain severity (MD = −0.84; 95% CI −1.49 to −0.19; p = 0.01; I^2^ = 86%), emphasizing that the greatest significant improvement was noted in pain-related symptoms, as shown in Figure 3.
All affected children in both groups. This difference was statistically significant (χ^2^ = 7.179, p = 0.008). The likelihood of enduring postoperative mild hearing loss was around 16 times greater in the mucoid group than in the serous group (adjusted OR = 15.97, 95% CI not displayed), indicating that mucoid effusions correlate with inferior auditory recovery post surgery.
3.3.3. Frequency of Bowel Movement (Defecation Frequency)
The pooled odds ratio was 7.50 (95% CI 0.36–154.51; p = 0.19), indicating a non-statistically significant difference between the two compared groups. Pooled studies under the random effect model were heterogeneous (I^2^ = 95%, p < 0.0001), predominantly influenced by Mezzasalma et al. (2016), which indicated a substantially greater effect (OR = 36.00; 95% CI 11.34–114.26) in contrast to Shanshal et al. (2023) (OR = 1.65; 95% CI 0.74–3.71), as shown in Figure 4 [31,37].
3.3.4. Adequate Global Relief from IBS Symptoms
The pooled analysis revealed no significant difference between probiotics and placebo (OR = 1.34, 95% CI 0.65–2.79; p = 0.43), suggesting variability in response across strains and subtypes, as shown in Figure 5. Pooled studies under the random effect model were heterogeneous (I^2^ = 74%, p = 0.004). This inconsistency was likely influenced by the heterogeneous definitions used for “adequate global relief” across trials. Some studies assessed weekly symptom resolution whereas others used multi-week or composite criteria, leading to nonuniform thresholds for defining clinical improvement. These methodological differences may partially explain the discrepancy between this outcome and the more consistent findings presented in Figure 2 and Figure 3. Standardized definitions of global relief will be essential to improve comparability in future research.
3.3.5. Quality of Life (QoL)
Pooled analysis indicated that probiotics significantly enhanced the quality of life for individuals with IBS (MD = 24.48; 95% CI 20.4–28.5; p < 0.00001). Because higher QoL scores indicate better patient well-being, the positive mean difference reflects a greater improvement in the probiotic group. Although the forest plot visually places the diamond toward the “control” side due to scale orientation, the numerical results consistently favor probiotics. Pooled studies under the fixed effect model were homogeneous (I^2^ = 0%, p = 0.7), as shown in Figure 6.
3.3.6. Stool Type Classification (Bristol Stool Scale)
A pooled analysis of three studies indicated that probiotics enhanced stool consistency relative to placebo (OR = 24.11; 95% CI 4.39–132.3; p = 0.0002). Pooled studies under the random effect model were heterogeneous (I^2^ = 79%), attributed to variations in probiotic formulations and IBS subtypes, as illustrated in Figure 7.
3.3.7. FDA-Defined Global Improvement (Responder Analysis)
The pooled analysis of three studies showed a clinically meaningful improvement in overall IBS symptoms consistent with FDA responder definitions and the superiority of probiotics over placebo (OR = 1.71; 95% CI 1.26–2.33; p = 0.0006). Pooled studies under the fixed effect model were homogeneous (I^2^ = 29%), as shown in Figure 8.
3.3.8. Adverse Events
The pooled analysis revealed that the incidence of adverse events was comparable between the two groups (OR = 0.77; 95% CI 0.55–1.07; p = 0.12); the pooled studies under the fixed effect model demonstrated homogeneity (I^2^ = 7%), suggesting that probiotics were predominantly well tolerated without an elevated risk of adverse effects, as shown in Figure 9.
3.4. Risk of Bias Assessment
The risk-of-bias evaluation revealed that most studies demonstrated a low risk of bias across all domains, particularly in randomization, allocation concealment, and blinding. A few studies showed an unclear risk, mainly due to incomplete outcome data, selective reporting, or other potential biases, while no high-risk assessments were identified, as illustrated in Figure 10A,B.
4. Discussion
This systematic review with meta-analysis combines results from 16 well-conducted randomized controlled trials (RCTs) including 2823 patients with irritable bowel syndrome (IBS). The findings provide strong evidence supporting the effectiveness of oral probiotics in achieving IBS symptom control. The primary outcome demonstrates that probiotics are significantly more beneficial than placebo in improving overall symptoms, with a substantial reduction in IBS-Severity Scoring System (IBS-SSS) scores (mean difference = −93.92; 95% CI: −133.11 to −54.73; p < 0.00001). This improvement suggests a meaningful enhancement in patient quality of life. Consistent gains in global improvement—based on FDA-proposed responder definitions (OR = 1.71; 95% CI: 1.26–2.33; p = 0.0006)—and low heterogeneity (I^2^ = 29%) further reinforce the reliability of these results. Additionally, reductions in abdominal discomfort support potential mechanisms involving gut–brain axis modulation, visceral sensitivity, or microbiome regulation [46].
The results align with previous evidence supporting probiotic use in IBS [47]. The favorable safety profile (OR = 0.77; p = 0.12; I^2^ = 7%) suggests no increased risk of adverse events compared with placebo. However, interpreting continuous outcomes remains challenging due to high heterogeneity in IBS-SSS (I^2^ = 71%) and intestinal discomfort (I^2^ = 84%). This variability may reflect clinical diversity related to heterogeneous IBS subtypes [48] and the strain-specific nature of probiotic effects [49]. Methodological differences including variable strain combinations, dosages, and formulations also contribute to inconsistencies in reported efficacy [50].
Current clinical guidelines provide a nuanced context for interpreting these findings. The 2021 American College of Gastroenterology (ACG) Clinical Guideline for the Management of IBS suggests against the routine use of probiotics for global IBS symptoms, citing low certainty of evidence and substantial heterogeneity across trials [51]. This cautious recommendation reflects earlier inconsistencies in probiotic formulations, strain selection, and outcome reporting rather than a clear lack of therapeutic effect. Importantly, the present meta-analysis incorporates a larger and more contemporary evidence base, including higher-quality RCTs and standardized outcome measures, which may partially address the limitations highlighted in the ACG guideline. Our findings therefore contribute updated evidence that may inform future guideline revisions, particularly as probiotic research continues to evolve.
Recent evidence highlights the potential superiority of multi-strain and multispecies probiotic formulations. For example, Allegretti et al. (2025) reported significant improvements in bloating, gas, and abdominal discomfort using a 24-strain synbiotic, suggesting that broader microbial diversity may enhance clinical benefits [52]. These advanced diagnostic tools allow clinicians to characterize individual microbiome patterns before and after treatment, offering opportunities to tailor probiotic interventions. With microbiome assessment becoming increasingly integrated into clinical care, these approaches may refine future therapeutic strategies [53]. A recent meta-analysis by Yang et al. (2024), which included 72 RCTs, demonstrated modest but significant improvements in global IBS symptoms and abdominal pain with probiotic use while similarly noting considerable heterogeneity and strain-specific effects [15].
The clinical implications of this review are noteworthy. Probiotics demonstrate measurable symptom relief, good tolerability, and potential value for patients who do not respond adequately to first-line therapies. These findings support considering probiotics as a meaningful component of IBS management rather than solely an adjunctive option. At the same time, the growing evidence base for multi-strain and personalized probiotic therapy underscores the need for updated clinical frameworks that account for strain specificity, microbiome profiles, and biological mechanisms.
Future research should focus on large, well-designed RCTs evaluating specific strains in defined IBS subtypes; mechanistic studies addressing microbial changes, SCFA pathways, and mucosal barrier effects; and long-term follow-up to understand sustained benefits. Despite some limitations, including heterogeneity and incomplete reporting, this review provides robust evidence supporting probiotic use while highlighting the need for more precise and personalized therapeutic approaches.
5. Conclusions
This systematic review and meta-analysis study of 16 randomized controlled trials involving 2823 patients with irritable bowel syndrome provides robust evidence supporting the efficacy of oral probiotics for symptom management. The results demonstrated that probiotic therapy significantly reduced total symptom severity and meaningful global improvement compared with placebo, with additional benefits observed across key symptom domains (abdominal pain and diarrhea). Importantly, probiotics demonstrated a favorable safety profile, with no significant increase in adverse events relative to placebo.
Taken together, all of these findings indicate that probiotics represent a safe and effective therapeutic option for improving symptoms in overall patients who have IBS. However, given the variability in probiotic strains, dosages, and study durations, further well-designed, large-scale trials are warranted to establish optimal regimens and confirm long-term benefits.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Center for Biotechnology Information Irritable bowel syndrome Bookshelf U.S. National Library of Medicine Bethesda, MD, USA 2025 Available online: https://www.ncbi.nlm.nih.gov/books/NBK 534810/(accessed on 11 November 2025)
- 2Chen M. Ruan G. Chen L. Ying S. Li G. Xu F. Xiao Z. Tian Y. Lv L. Ping Y. Neurotransmitter and Intestinal Interactions: Focus on the Microbiota-Gut-Brain Axis in Irritable Bowel Syndrome Front. Endocrinol.20221381710010.3389/fendo.2022.81710035250873 PMC 8888441 · doi ↗ · pubmed ↗
- 3Soufan F. Ghosson A. Jaber R. Ghandour A. Uwishema O. The Gut-Brain Axis in Irritable Bowel Syndrome: Implementing the Role of Microbiota and Neuroimmune Interaction in Personalized Prevention—A Narrative Review Health Sci. Rep.20258 e 7066010.1002/hsr 2.7066040256131 PMC 12006843 · doi ↗ · pubmed ↗
- 4Xie X. He J. Xu S. Xu Z. Long Y. Duan Z. Yang J. Zhang Z. Wu J. Cai L. Psychological factors may affect the quality of life in irritable bowel syndrome patients more than the gut itself? A multicenter cross-sectional study JGH. Open 20248 e 1304510.1002/jgh 3.1304538544955 PMC 10966133 · doi ↗ · pubmed ↗
- 5Oka P. Parr H. Barberio B. Black C.J. Savarino E.V. Ford A.C. Global prevalence of irritable bowel syndrome according to Rome III or IV criteria: A systematic review and meta-analysis Lancet Gastroenterol. Hepatol.2020590891710.1016/S 2468-1253(20)30217-X 32702295 · doi ↗ · pubmed ↗
- 6Guido V. Pontet Y. López V. Olano C. Prevalence of irritable bowel syndrome and other functional gastrointestinal disorders in Uruguay Rev. Gastroenterol. Mex. (Engl. Ed.)20248925826410.1016/j.rgmxen.2023.06.00538644084 · doi ↗ · pubmed ↗
- 7Zhang T. Ma X. Tian W. Zhang J. Wei Y. Zhang B. Wang F. Tang X. Global research trends in irritable bowel syndrome: A bibliometric and visualized study Front. Med. (Lausanne)2022992206310.3389/fmed.2022.92206335833106 PMC 9271748 · doi ↗ · pubmed ↗
- 8Almasary M. Alkhalifah K.M. Alotaibi S.H. Elhefny M. Alabssi H. Alaklabi S.S. Alayed R.S. Alghamdi A.A. Albalawi A. Prevalence of Irritable Bowel Syndrome in Saudi Arabia: A Systematic Review and Meta-Analysis Cureus 202315 e 4535710.7759/cureus.4535737849586 PMC 10577611 · doi ↗ · pubmed ↗