Comparative Evidence on Negative Pressure Therapy and Hyperbaric Oxygen Therapy for Diabetic Foot Ulcers: A Systematic Review of Independent Effectiveness and Clinical Applicability
Álvaro Astasio-Picado, Jesús Jurado-Palomo, Belén Pozo-Aranda, Paula Cobos-Moreno

TL;DR
This paper compares two treatments for diabetic foot ulcers—negative pressure therapy and hyperbaric oxygen therapy—finding both effective but highlighting the need for individualized treatment choices.
Contribution
The study provides a systematic review comparing the clinical effectiveness and applicability of NPWT and HBOT for diabetic foot ulcers.
Findings
NPWT accelerates wound healing but effectiveness varies by intervention type and clinical context.
HBOT reduces major amputations and promotes angiogenesis.
Both therapies are effective but require individualized treatment decisions.
Abstract
Background and Objectives: To evaluate and synthesize evidence on the independent clinical effectiveness, safety, and applicability of Negative Pressure Wound Therapy (NPWT) and Hyperbaric Oxygen Therapy (HBOT) in diabetic foot ulcers (DFUs), and to determine whether current evidence allows for a direct comparison between both interventions: NPWT and HBOT are widely advanced therapies for DFUs. Although both show benefits, the relative superiority of one over the other remains unclear. Systematic review of the literature conducted in accordance with PRISMA guidelines. Materials and Methods: A comprehensive literature search was performed using two electronic databases. The review included randomized controlled trials, systematic reviews, meta-analyses, and non-randomized studies. Methodological quality and risk of bias were assessed using validated tools: RoB 2.0 for randomized trials,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
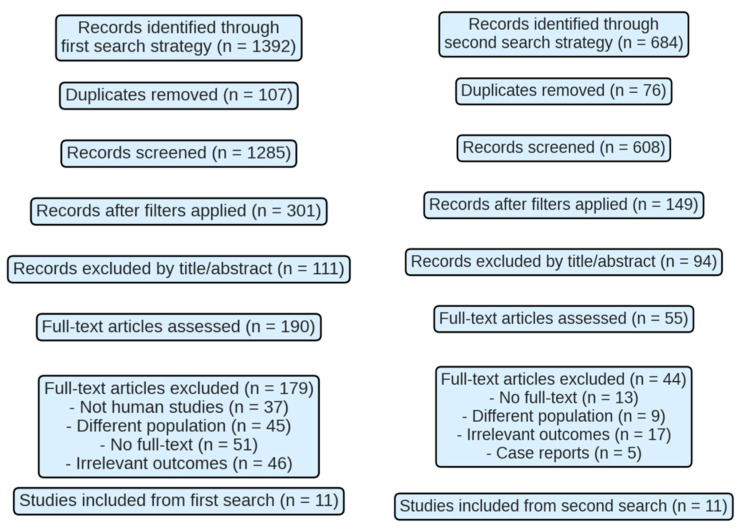 Figure 1
Figure 1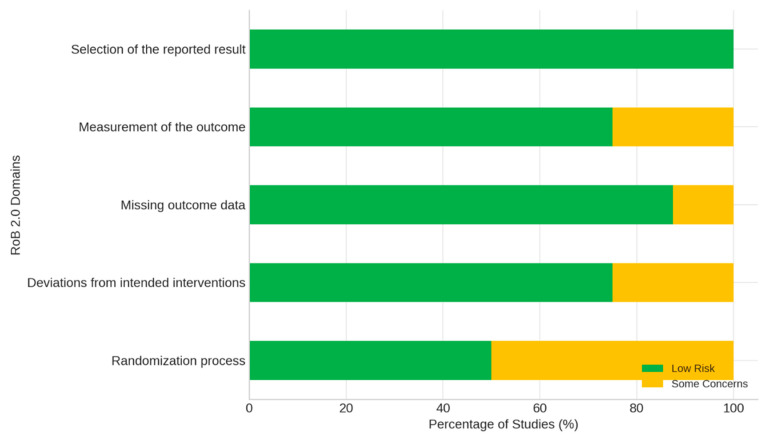 Figure 2
Figure 2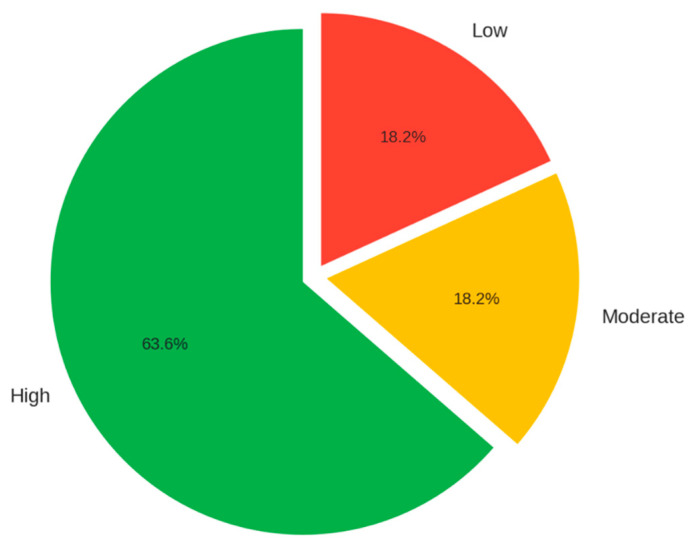 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetic Foot Ulcer Assessment and Management · Wound Healing and Treatments · Surgical site infection prevention
1. Introduction
Diabetic foot (DF) is one of the most common, debilitating, and costly complications of diabetes mellitus (DM), affecting a substantial proportion of patients and representing a major cause of morbidity, mortality, and long-term disability worldwide [1]. Diabetic foot ulcers (DFUs), in particular, constitute a major clinical challenge due to their complex pathophysiology and their high propensity to deteriorate into deep infections, osteomyelitis, or severe ischemic damage, frequently culminating in partial or major lower-limb amputation [2]. This cascade of events profoundly affects patients’ quality of life by reducing functional independence, mobility, and social participation, while simultaneously generating a disproportionate economic burden for healthcare systems and families [3].
DM is a chronic endocrine-metabolic disorder characterized by persistent hyperglycemia resulting from impaired insulin secretion, insulin action, or both [4,5,6,7]. Over recent decades, the global prevalence of DM has risen dramatically, driven by aging populations, sedentary lifestyles, increased rates of obesity, and greater exposure to energy-dense diets [8]. This escalation has been particularly pronounced in low- and middle-income countries, where rapid urbanization and limited access to preventive care have intensified the public health impact of the disease. Among its chronic complications, diabetic foot pathology (PD) stands out as one of the most severe due to its multifactorial nature and the wide spectrum of associated clinical consequences [5,6,7,8,9,10,11,12,13].
DFU development results from the convergence of three major physiopathological processes peripheral neuropathy, peripheral arterial disease, and biomechanical foot alterations. Sensory neuropathy diminishes protective sensation and prevents recognition of repetitive trauma; motor neuropathy leads to structural deformities and abnormal plantar pressures; while autonomic neuropathy reduces sweating, leading to dry, fissured skin vulnerable to injury [5,13,14,15]. In parallel, peripheral arterial disease compromises tissue oxygenation, impeding wound healing, and worsening susceptibility to infection. Once an ulcer appears, impaired immune responses, reduced leukocyte function, and persistent hyperglycemia foster bacterial colonization and chronic inflammation, generating an ideal environment for non-healing wounds.
The magnitude of the problem is alarming: according to the International Diabetes Federation, more than 4 million people develop DFUs every year [1], and up to 25% of individuals with diabetes will experience at least one ulcer during their lifetime. Recurrence is common, with nearly 40% of healed ulcers reappearing within one year and up to 65% within five years. DFUs remain the leading cause of non-traumatic lower-limb amputations globally, with amputation risk up to 20 times higher in diabetic populations. Post-amputation mortality is high, reaching 70% at five years, surpassing many cancer survival rates [14].
Beyond the individual burden, DFUs impose an immense financial challenge. Their management requires intensive healthcare resources—hospital admissions, diagnostic procedures, revascularization surgeries, prolonged antibiotic therapies, advanced wound care, and long-term rehabilitation. According to global estimates, DFU treatment consumes billions of dollars annually, and costs increase exponentially when complications or amputations occur, further underscoring the imperative for early, effective interventions.
Traditional management strategies—consisting of glycemic control, wound debridement, infection treatment, vascular evaluation, antimicrobial therapy, pressure offloading, and moisture-balanced dressings—form the cornerstone of DFU care. However, despite their importance, healing is often slow, and recurrence remains distressingly common [3]. This clinical reality has prompted the integration of advanced adjunctive therapies capable of enhancing the wound microenvironment, promoting perfusion, and accelerating tissue regeneration.
Among these innovative interventions, Hyperbaric Oxygen Therapy (HBOT) and Negative Pressure Wound Therapy (NPWT) are two of the most widely studied and increasingly utilized modalities. HBOT involves administering100% oxygen at pressures than atmospheric levels, achieving a substantial rise in dissolved oxygen within plasma. This hyperoxygenation stimulates angiogenesis, enhances fibroblast proliferation and collagen synthesis, augments leukocyte bactericidal activity, and improves the efficacy of certain antibiotics [16,17,18,19]. Clinical studies have suggested that HBOT may reduce major amputation rates and improve healing trajectories in chronic or ischemic DFUs, particularly when microcirculatory impairment plays a critical role.
NPWT, in contrast, applies controlled subatmospheric pressure to the wound through a sealed dressing connected to a vacuum pump. This mechanism removes excess exudate, decreases bacterial burden, reduces interstitial edema, increases local perfusion, and mechanically stimulates granulation tissue formation [14,20]. NPWT has shown considerable therapeutic value in complex, exudative, or deep wounds especially those unresponsive to conventional treatment modalities.
The implementation of both HBOT and NPWT requires skilled multidisciplinary collaboration. In this context, nursing professionals perform essential functions such as wound assessment, device management, patient education, adherence monitoring, identification of early complications, and integration of care strategies [2]. Their clinical role is central to therapy effectiveness and patient outcomes.
Despite the accumulated evidence supporting both interventions, notable conceptual and methodological gaps persist. Although the literature often debates which therapy may offer superior clinical outcomes in terms of efficacy, safety, and applicability, these dimensions have seldom been explored systematically or in a manner that allows direct comparison. Regarding safety, the available studies report adverse events in a heterogeneous and frequently superficial way. For HBOT, side effects such as barotrauma, middle-ear discomfort, headaches, oxygen toxicity, or transient visual changes are described inconsistently across trials [18], while NPWT-related complications including perilesional maceration, bleeding, necrosis, or localized infection—are documented in case series and observational studies but rarely assessed as primary outcomes [21,22]. This fragmented reporting prevents establishing robust and comparable risk profiles for each therapy.
Similarly, applicability has not been evaluated in depth despite being essential for real-world clinical decision-making. HBOT requires access to specialized hyperbaric chambers, trained technical personnel, and high-cost infrastructure, which limits its availability and feasibility in many health systems [16,17,18]. In contrast, NPWT depends on device accessibility, adherence to equipment protocols, and close monitoring by trained wound-care professionals to minimize complications and ensure treatment continuity, all of which directly influence its logistical and economic viability [14,20]. These contextual factors significantly affect therapeutic selection but remain underrepresented in most studies.
Furthermore, no high-quality studies directly comparing NPWT with HBOT exist. Instead, virtually all available evidence evaluates each intervention independently against standard or conventional wound care [21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42]. This evidence structure, although useful for determining individual therapeutic benefits, does not permit establishing methodologically valid conclusions regarding their relative superiority or optimal indication according to ulcer type, severity, or patient profile. Consequently, the current scientific literature provides valuable but fragmented insights that clarify the isolated effects of NPWT and HBOT but do not resolve the comparative uncertainties that persist in clinical practice.
Given these gaps, a comprehensive and systematic synthesis of the evidence is essential to guide clinical decision-making. The present systematic review aims to evaluate the independent clinical efficacy of NPWT and HBOT in the management of DFUs, with particular emphasis on their contribution to healing outcomes, complication reduction (including the prevention of amputations), and clinical applicability within multidisciplinary care frameworks.
The overarching objective of this study is to analyze and compare the available evidence on NPWT and HBOT as therapeutic strategies for DFUs, with a focus on optimizing healing outcomes and enhancing quality of life, particularly from the perspective of nursing practice, which plays a pivotal role in the management and success of advanced wound therapies.
2. Methodology
This paper constitutes a systematic review of the scientific literature aimed at evaluating the efficacy of two innovative therapies—negative pressure therapy (NPT) and hyperbaric oxygen therapy (HBOT)—in the treatment of diabetic foot ulcers (DFUs). The review was designed following a rigorous protocol and in accordance with the guidelines of the PRISMA 2020 Declaration (Supplementary Materials), ensuring a transparent, reproducible, and exhaustive process for the identification, selection, and analysis of relevant studies [43].
The protocol was previously registered in the PROSPERO international retrospective register of systematic reviews (ID: CRD420251273813).
Study eligibility criteria: Inclusion criteria were randomized clinical trials, non-randomized studies, and meta-analyses, publications in English and Spanish, studies available in full text, and research conducted in human populations. Exclusion criteria included publications prior to 2014, dissertations, case reports, literature reviews, short articles, or other documents with a low level of scientific evidence.
To guide this review, the following research question was formulated, structured according to the PICO model: ElementDescriptionP (Population)Patients with diabetes mellitus presenting with active diabetic foot ulcers.I (Intervention)NPWT or HBOT.C (Comparison)Conventional treatment. Direct comparison between NPWT and HBOT was not possible due to absence of eligible head-to-head studies.O (Outcomes)Healing rate, reduction in complications, and improvement in quality of life.
The scientific literature search was conducted in five specialized and widely recognized electronic databases in the biomedical field: PubMed, The Cochrane Library, Web of Science (WOS), SciELO, and Dialnet. These sources were selected for their multidisciplinary coverage and their usefulness in high-quality studies on therapeutic interventions.
A structured search strategy was designed using standardized descriptors in English (MeSH) and Spanish (DeCS), combined using the Boolean operators “AND” and “OR,” to optimize the retrieval of relevant studies. The main search formulas were: “(Diabetic foot ulcer) AND (Negative pressure therapy OR VAC therapy)” and “(Diabetic foot ulcer) AND (Hyperbaric oxygen therapy)”.
In addition, filters were applied to restrict the results to human studies, publications from 2014 to 2025, and languages: English and Spanish.
The selection and data collection process took place between November 2024 and March 2025, according to the previously defined inclusion and exclusion criteria. Article selection was carried out in several stages, including screening by title and abstract: elimination of irrelevant articles; full reading of potentially eligible studies; and final assessment of inclusion based on compliance with the PICO framework.
To facilitate and systematize the process, Rayyan QCRI (web version, 2023) software was used, a support tool for systematic reviews that allows for comparing decisions between reviewers and managing discrepancies.
Included studies had to evaluate the efficacy of NPT or HBOT in patients with active PD ulcers, without restriction by age, sex, or comorbidities, as long as the primary condition was the presence of diabetic ulcers. The outcomes of interest were healing rate, ulcer size reduction, healing time, adverse events or complications, and patient quality of life.
To assess the methodological quality of the included studies, different tools were used depending on the design type:
- RoB 2.0: For randomized controlled trials. It assesses the risk of bias in five critical domains and provides an overall assessment of the risk of bias per outcome (Table A1) [43].
- AMSTAR-2: For meta-analyses and systematic reviews. It analyzes 16 domains and classifies the overall confidence in the quality of the review as high, moderate, low, or critically low (Table A2) [44].
- ROBINS-I: For non-randomized studies. It assesses seven domains, including bias due to confounding, participant selection, intervention classification, and outcomes, among others. Studies are classified as low, moderate, severe, or critical risk (Table A3) [45].
Regarding the evidence synthesis, due to the heterogeneity of the selected studies in terms of design, population, type of intervention, and variables measured, a quantitative meta-analysis was not possible. Instead, a qualitative narrative synthesis was conducted, which groups and analyzes the main findings of the studies, assessing the consistency of the results and their clinical applicability.
Likewise, the GRADE (Grading of Recommendations Assessment, Development and Evaluation) system was applied to evaluate the quality of the evidence and the strength of the recommendations. GRADE classifies evidence into four levels: high, moderate, low, and very low, based on the study design, the consistency of the results, the precision of the estimates, and the risk of bias [46].
3. Results
Study selection process:
1392 records were identified in the first search strategy, of which 107 were eliminated due to duplicate results. After applying filters, 301 studies were screened, excluding 111 after reviewing the title and abstract. A total of 190 full-text articles were evaluated, of which 179 were discarded due to: lack of inclusion of human subjects (n = 37), inappropriate population (n = 45), inaccessibility of the full text (n = 51), or irrelevant results (n = 46). Eleven studies were selected (Figure 1).
The second strategy yielded 684 records, of which 76 were duplicates. After applying filters, 149 studies were screened, 94 of which were excluded. Fifty-five full texts were evaluated, with 44 excluded due to text inaccessibility (n = 13), inappropriate population (n = 9), irrelevant results (n = 17), or inadequate design (n = 5). Ultimately, 11 studies were included.
A total of 22 studies met the inclusion criteria (Table A4).
General characteristics of the included studies:
The selected studies included 9 meta-analyses, 1 systematic review, 8 randomized controlled trials (RCTs), and 4 non-randomized studies. The geographic distribution was diverse, with China (n = 6) and Spain (n = 3) being the most represented countries. The sample size ranged from 28 to 1764 participants.
Importantly, none of the included studies directly compared Negative Pressure Wound Therapy (NPWT) with Hyperbaric Oxygen Therapy (HBOT). Instead, all identified investigations evaluated each therapy independently against conventional or standard DFU management strategies. Therefore, the evidence base allows assessment of the individual effectiveness of NPWT and HBOT, but does not permit a direct comparative analysis between the two modalities.
For this reason, in the context of the present review, NPWT and HBOT are examined separately in relation to conventional treatment, rather than against each other. This distinction is essential to correctly interpret the findings and to avoid overestimating comparative conclusions that the available evidence cannot support.
Summary of results:
Meta-analyses on NPWT reported improvements in wound healing and tissue quality [23,24,25], while those focusing on HBOT showed reductions in major amputations and improvements in DFU healing in patients with peripheral arterial disease [26,27,28,29,30,31].
In RCTs, NPWT showed additional benefits when combined with antibiotic cement [33], as well as superiority over alginate dressings in terms of perfusion and grafting [34]. However, some studies found no significant differences compared to conventional treatments [35,36]. HBOT, on the other hand, was associated with a higher healing rate, fewer amputations, and improved tissue oxygenation [37,38,39,40].
Non-randomized studies supported the efficacy of NPWT in reducing lesion size and epithelialization [21,22,41], although complications such as perilesional maceration were also reported [21]. An additional study observed a 43.3% wound reduction after four weeks of low-pressure NPWT [42].
The included systematic review [32] showed benefits in transcutaneous oxygenation and ulcer area reduction with HBOT, although without a significant impact on amputation rates.
Risk of bias assessment:
RoB 2.0 was used for RCTs, AMSTAR-2 for reviews and meta-analyses, and ROBINS-I for non-randomized studies (Figure 2).
In the RCTs, 75% showed low overall risk, although concerns were noted regarding randomization (50%) and outcome measurement (25%).
In the meta-analyses and reviews, 80% showed high confidence, although 40% did not disclose funding sources and 60% did not adequately include PICO components.
The non-randomized studies showed moderate overall risk, primarily due to bias in outcome measurement.
Certainty of evidence:
According to the GRADE tool, 14 studies were classified as high quality, 4 as moderate, and 4 as low. The high-quality studies showed low risk of bias and consistent results. Methodological limitations in moderate- or low-quality studies included the presence of bias, low precision, or uncontrolled confounding, which affect confidence in their results (Figure 3).
4. Discussion
Diabetic foot ulcers (DFUs) are one of the most serious and frequent complications in people with diabetes, associated with high morbidity, prolonged hospitalization, decreased quality of life, and increased risk of lower-limb amputation. The chronicity and multifactorial origin of DFUs—often involving infection, ischemia, and neuropathy—require comprehensive and individualized treatment strategies. In recent years, advanced therapies such as Negative Pressure Wound Therapy (NPWT) and Hyperbaric Oxygen Therapy (HBOT) have gained relevance for their potential in promoting faster and more effective healing [13,14,15,16,17].
Effectiveness of Negative Pressure Wound Therapy (NPWT)
NPWT has been extensively studied and is considered one of the most effective approaches to promote healing in complex diabetic ulcers. Studies such as those by Chen L et al. [23] and Lavery LA et al. [42] demonstrated significant benefits in terms of wound area reduction, accelerated granulation tissue formation, and overall faster healing compared to conventional treatment. Similarly, Dalmedico MM et al. [24] and Wu Y et al. [34] reported higher graft survival and reduced neutrophil extracellular trap formation, respectively, when NPWT was applied in DFUs, suggesting additional biological benefits that extend beyond simple mechanical effects.
NPWT has also shown positive results from the perspective of both patients and healthcare providers. For example, Palomar Llatas F et al. [41] used the FEDPALLA and VAS scales to assess the impact of NPWT on comfort and quality of care, concluding that this therapy improved patients’ perception of treatment while optimizing clinical management.
Despite these advantages, the evidence is not universally consistent. Studies by Seidel D et al. [35], Liu Z et al. [25], and Lavery LA et al. [36] did not find statistically significant differences in healing rates when comparing NPWT to standard care, nor when comparing different NPWT modalities (e.g., high vs. low pressure), suggesting that its success may depend on other factors such as wound classification, duration of diabetes, or infection status.
The combination of NPWT with other treatment modalities appears to enhance its effectiveness. For instance, Zhong M et al. [33] observed that combining NPWT with antibiotic-loaded bone cement improved the wound bed quality by reducing inflammation (notably via IL-6 modulation) and promoting a favorable M1/M2 macrophage balance, both of which are essential for tissue regeneration.
However, complications linked to NPWT have also been reported. García Oreja S et al. [21] and Lázaro Martínez JL et al. [22] documented adverse events such as perilesional maceration, bleeding, necrosis, and localized infection. Although most patients still experienced satisfactory wound healing, these complications highlight the importance of close monitoring during therapy.
Effectiveness of Hyperbaric Oxygen Therapy (HBOT)
HBOT has also been studied as a complementary treatment for DFUs, especially in cases where chronic ischemia and tissue hypoxia hinder healing. By delivering 100% oxygen at elevated atmospheric pressures, HBOT increases tissue oxygen tension, promoting angiogenesis, fibroblast proliferation, and enhanced antimicrobial activity [32,40].
The study by Nik Hisamuddin NAR et al. [40] supports these mechanisms, showing that HBOT combined with conventional wound care (debridement, irrigation, and dressings) significantly reduced wound size and improved markers of tissue oxygenation. These findings are reinforced by systematic reviews and clinical trials conducted by Elraiyah T et al. [26], Sharma R et al. [30], Chen CY et al. [37], and Kumar A et al. [39], who observed enhanced healing rates and a notable reduction in major amputations, a key outcome in DFU treatment.
In comparative studies, HBOT also outperformed other advanced therapies. A study comparing HBOT to low-level laser therapy showed a significantly greater reduction in wound area with HBOT (89.76% vs. 89.5%), although combining both therapies did not yield additional benefits [38]. This suggests that while HBOT is effective, synergistic approaches may not always result in improved outcomes and must be evaluated on a case-by-case basis.
Nonetheless, HBOT is not without risks. Adverse events such as barotrauma, tinnitus, headaches, and episodes of hypoglycemia have been reported [27,28,29,30,31,32]. While most are mild and self-limiting, careful patient selection and monitoring are crucial, especially in those with pre-existing pulmonary, cardiovascular, or neurologic conditions.
Comparative Analysis and Clinical Considerations
Both NPWT and HBOT offer distinct advantages in the management of DFUs. NPWT is especially effective in reducing wound size, promoting granulation tissue, and decreasing local edema. It is particularly suitable for deep, exudative wounds with infection risk. On the other hand, HBOT is more appropriate for ischemic or refractory wounds where hypoxia plays a central role, and its systemic effects on oxygenation and angiogenesis may benefit tissues beyond the ulcer site.
However, both treatments also present limitations. NPWT may be less effective in ischemic wounds or in cases of poor glycemic control, and it carries a non-negligible risk of local complications [21,22]. Meanwhile, HBOT, despite its systemic benefits, involves higher costs, specialized infrastructure, and risks related to oxygen toxicity [30]. Importantly, neither therapy is a panacea and should be integrated into a multidisciplinary care plan that includes glycemic control, infection management, and pressure offloading [47,48,49].
Limitations and Future Research
The current body of evidence is limited by the heterogeneity of study designs, small sample sizes, variability in outcome measures, and short follow-up durations. In particular, differences in NPWT pressure settings and HBOT treatment protocols make comparisons difficult and hinder the generalizability of results.
Future studies should focus on:Standardizing treatment protocols for both NPWT and HBOT.Conducting large-scale randomized controlled trials with long-term follow-up.Evaluating cost-effectiveness and quality-of-life outcomes.Exploring the molecular and immunologic mechanisms behind treatment efficacy.Investigating combination therapies and personalized approaches based on wound etiology and patient profile.
5. Conclusions
Based on the available evidence, this systematic review indicates that both Negative Pressure Wound Therapy (NPWT) and Hyperbaric Oxygen Therapy (HBOT) demonstrate independent clinical benefits in the management of diabetic foot ulcers (DFUs). However, the heterogeneity of study designs, populations, and outcome measures—and the absence of direct comparative studies—prevents establishing whether one therapy is superior to the other.
NPWT shows consistent improvements in wound granulation and ulcer size reduction when compared with conventional treatment, although the magnitude of these effects varies across studies and patient characteristics. HBOT demonstrates benefits particularly in chronic or ischemic DFUs, including enhanced tissue oxygenation and a reduction in major amputations, though its use is limited by safety considerations, cost, and the need for specialized infrastructure.
Given that no included study directly compared NPWT and HBOT, this review cannot determine comparative efficacy between the two interventions. Therefore, treatment decisions should rely on the individual clinical profile of the patient, ulcer etiology, resource availability, and multidisciplinary assessment.
Nursing professionals play a crucial role in implementing both therapies, ensuring appropriate monitoring, patient education, and early detection of complications, thereby contributing to improved healing outcomes and overall quality of care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Álvarez-Seijas E. Mena-Bouza K. Faget-Cepero O. Conesa-González A.I. Domínguez-Alonso E. El pie de riesgo de acuerdo con su estratificación Rev. Cuba. Endocrinol.201526158171
- 2Del-Castillo-Tirado R.A. Fernández-López J.A. Del-Castillo-Tirado F.J. Guía de Práctica Clínica en el pie diabético Arch. Med.201410117
- 3Bandyk D.F. The diabetic foot: Pathophysiology, evaluation, and treatment Semin. Vasc. Surg.201831434810.1053/j.semvascsurg.2019.02.00130876640 · doi ↗ · pubmed ↗
- 4Rojas de P.E. Molina R. Rodríguez C. Definición, clasificación y diagnóstico de la diabetes mellitus Rev. Venez. Endocrinol. Metab.201210712
- 5American Diabetes Association Diagnosis and Classification of Diabetes Mellitus Diabetes Care 201336677410.2337/dc 13-S 06723264425 PMC 3537273 · doi ↗ · pubmed ↗
- 6World Health Organization International Diabetes Federation Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia WHO Geneva, Switzerland 20069241594934 Available online: https://www.who.int/publications/i/item/definition-and-diagnosis-of-diabetes-mellitus-and-intermediate-hyperglycaemia(accessed on 28 December 2025)
- 7Almaguer-Herrera A. Miguel-Soca P.E. SeráC.R. Mariño-Soler A.L. Oliveros-Guerra R.C. Actualización sobre diabetes mellitus Correo. Científico. Méd.201216116
- 8Magliano D.J. Boyko E.J. IDF Diabetes Atlas 10th ed.International Diabetes Federation Brussels, Belgium 2021 Available online: http://www.ncbi.nlm.nih.gov/books/NBK 581934/(accessed on 28 December 2025)