Occupational Radiation Risk Stratification and Protection in Fluoroscopy-Guided Surgeons and Interventionalists: A Multispecialty Structured Narrative Review
Nana Kwadwo Okraku-Yirenkyi, Sri Snehita Reddy Bonthu, Hanisha Bhakta, Oluwatoyin O. Duyile, Michael Bernas

TL;DR
This review examines radiation risks for surgeons using fluoroscopy and evaluates how protective gear and practices can reduce exposure and cancer risks.
Contribution
The paper provides a structured narrative review on occupational radiation exposure and protection strategies across multiple surgical specialties.
Findings
Lead aprons and thyroid collars significantly reduce radiation exposure, but eye and lower-body shielding are inconsistently used.
BEIR VII modeling suggests increased cancer risks for chronically exposed operators, though epidemiologic data is limited.
High compliance with some protective measures coexists with variability in exposure and inconsistent adherence to full shielding protocols.
Abstract
Background/Objectives: Fluoroscopy-guided procedures are widely used across surgical and interventional specialties but expose operators to ionizing radiation with associated stochastic and deterministic effects. The aim is to characterize occupational radiation exposure, evaluate the effectiveness of shielding strategies, assess long-term cancer risks, and identify compliance patterns. Methods: This structured narrative review summarizes evidence on operator dose, shielding effectiveness, compliance with protective practices, and long-term cancer risk. A search of PubMed, Scopus, Embase, and Web of Science (limited to January 2000–March 2024) identified 62 records; 27 full texts were reviewed, and 16 studies met the inclusion criteria. Results: Across studies, unshielded chest exposure averaged 0.08–0.11 mSv per procedure, and eye exposure averaged 0.04–0.05 mSv. Lead aprons reduced…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
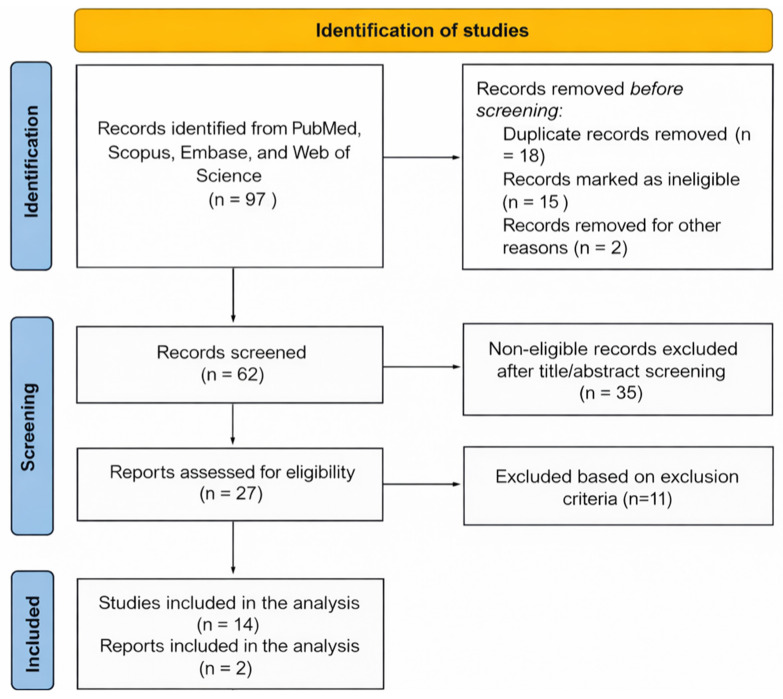 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRadiation Dose and Imaging · Digital Radiography and Breast Imaging · Radiology practices and education
1. Introduction
Fluoroscopy-guided procedures are increasingly integral to modern surgical practice, particularly in specialties such as orthopedic and trauma surgery, interventional cardiology, interventional radiology, vascular surgery, and cardiothoracic surgery. These techniques offer precision and minimally invasive approaches but also expose operators to ionizing radiation, presenting a persistent occupational hazard. A recent publication by Smith-Bindman et al. has highlighted the risk to physicians from work-related exposure to radiation in some specialties utilizing medical imaging [1].
Ionizing radiation is classified as a Group I human carcinogen by the International Agency for Research on Cancer [2]. International guidelines from organizations such as the International Commission on Radiological Protection (ICRP) recommend dose limits of 20 mSv per year with limits on equivalent dose to the lens of the eye of 20 mSv and of 500 mSv to the skin, hands and feet [3,4]. Exposure to this dose is associated with an additional lifetime risk of fatal cancer of 1 in 1000 [5]. Further guidelines emphasize ALARA (As Low As Reasonably Achievable) principles involving time, distance, and shielding to reduce exposure [3,4].
Radiation exposure can lead to stochastic effects, such as genetic aberrations and cancer that can occur randomly, and deterministic effects, such as hair loss and skin changes that occur when exposure exceeds a specified limit [6]. Beyond immediate exposure, long-term health risks, including cellular damage, cataracts, and malignancies such as skin cancer, breast cancer, thyroid cancer, and leukemia, have been documented [5,6,7]. Modeling studies, particularly those leveraging Biological Effects of Ionizing Radiation (BEIR) VII risk estimates, project elevated lifetime attributable risks (LAR)—for example, excess incidence of solid cancers and associated mortality for long-term occupational exposure [8]. Despite this, radiation safety training and systematic compliance remain inconsistent. Surveys highlight widespread gaps in education and monitoring, and adherence to protective practices such as dosimeter or shielding use, is frequently suboptimal [9,10].
Operators across specialties experience highly variable exposure patterns because procedure type, anatomic positioning, equipment configuration, and workflow differ substantially between fields such as orthopedics, interventional cardiology, and vascular surgery. These differences create distinct exposure profiles and long-term risk trajectories for different operator groups, highlighting the importance of risk stratification in evaluating occupational hazards. Understanding these specialty-specific patterns is therefore essential for ensuring that protective strategies and monitoring practices effectively address variations in operator risk. Because exposure profiles vary substantially across specialties, procedures, and operator roles, occupational radiation risk is inherently heterogeneous. Understanding and incorporating this variability aligns with personalized medicine principles by enabling risk-stratified protective strategies tailored to operator-specific exposure patterns. Primary specialties that utilize fluoroscopy include cardiology, orthopedics, gastroenterology, urology, vascular surgery, gynecology, and pain medicine. In fluoroscopy, X-rays constitute the primary form of ionizing radiation with both bremsstrahlung radiation and characteristic X-rays [11]. The energy range for X-ray photons used in fluoroscopy is typically between 40 and 125 kilovolts peak (kVp).
Within this context, we conducted a structured narrative review encompassing a range of surgical and interventional specialties that utilize fluoroscopy, aiming to characterize occupational radiation exposure, evaluate the effectiveness of shielding strategies, assess long-term cancer risks, and identify compliance patterns.
2. Materials and Methods
This structured narrative review followed guidelines from Sukhera [12] and utilized a comprehensive literature search independently conducted between March and May 2025 using PubMed, Scopus, Embase, and Web of Science. The Boolean search strategy was used to identify relevant literature. The search string used in the electronic databases was: “radiation protection” OR “lead vest” OR “lead apron” OR “thyroid shield” OR “radiation shielding” AND “occupational exposure” OR “operator dose” OR “fluoroscopy” OR “interventional procedures” OR “surgeon” OR “interventional cardiology” OR “orthopedic surgery” OR “vascular surgery” OR “interventional radiology.” This initial search strategy resulted in over 10,000 results that were a logistical challenge. Therefore, smaller, targeted Boolean variants (accomplished by reducing the number of search terms) were generated iteratively to improve search specificity. Filters were also applied to limit results to human studies, English-language publications, and peer-reviewed articles between 2000 and 2024. Inclusion and exclusion criteria (Table 1) were also utilized (see below). Additionally, reference lists of highly relevant papers were manually screened to identify supplementary eligible studies.
2.1. Article Selection
All studies identified in the search were eligible for review. The initial search yielded 62 articles after duplicate removal. Two independent authors screened titles and abstracts for relevance to occupational radiation exposure and protection strategies and retrieved 27 articles for full-text review. After applying the inclusion and exclusion criteria detailed in Table 1 at the full-text stage, 16 articles were included in the final synthesis. These studies spanned multiple specialties, procedural settings, and research methodologies, offering a broad evidence base to explore trends and best practices in occupational radiation safety during fluoroscopy-guided interventions. Although there was high methodological heterogeneity of the identified studies, inclusion and exclusion criteria is tight enough to capture relevant data.
2.2. Data Extraction
A detailed, pre-designed spreadsheet extraction template was used to collect data systematically across 25 structured fields: title, year, whether it was primary research, study design, sample size, country or region, surgical or interventional specialty, study duration or follow-up period, whether radiation exposure was measured or estimated, use of lead aprons or other shielding, consistency of lead protection use, pre- versus post-lead vest or shielding data, cancer type studied and its incidence or prevalence if applicable, whether a comparison group was included, reported risk ratios, odds ratios, or hazard ratios if applicable, confounding variables considered, lifestyle or occupational exposures assessed, statistical significance reported, whether longitudinal effects were studied, any policy or protocol recommendations, compliance with protection protocols, innovative methodologies used, inclusion of a pre-shielding or pre-vest historical baseline, and the role of that historical baseline in the paper.
Manual extraction was first performed by a single reviewer with secondary reviews from additional authors with cross-checking to ensure consistency and accuracy. Emphasis was placed on numeric values (e.g., radiation dose in mSv, percentage dose reductions, fold-change effects, risk multipliers) and statistically significant results. When numeric data were not explicitly reported, dose-related information was extracted from descriptive statements when possible; otherwise, values were marked as Not Reported.
2.3. Data Analysis
Extracted data were analyzed to calculate overall and subgroup-level summary statistics–including means, medians, ranges–for operator doses, shielding-associated reductions, and compliance rates. Trends were compared across surgical and interventional specialties including orthopedics, trauma, interventional cardiology, interventional radiology, vascular surgery, and cardiothoracic surgery. Procedural factors associated with higher or lower exposure, such as fluoroscopy time, beam angle, C-arm positioning, and the use of real-time dosimetry, were identified. Common methodological strengths, weaknesses, and gaps in the existing literature were synthesized and the consistency and robustness of reported statistical significance across diverse study types were assessed.
Due to methodological heterogeneity, no formal meta-analysis or pooled effect size calculations were performed. Instead, the review presents a qualitative and quantitative synthesis of available data, highlighting both generalizable insights and areas requiring further specialty-specific investigation.
3. Results
A total of 16 studies were included in this review (Table 2). The narrative review search flow chart is depicted in Figure 1. The studies spanned a variety of surgical and interventional specialties, including orthopedic surgery [13,14,15,16,17,18], trauma surgery [14], interventional radiology [19], cardiology [20,21], and vascular surgery [22,23,24,25,26,27,28]. Publication dates ranged from 2000 to 2024, with the majority concentrated between 2010 and 2024. Eleven studies (69%) were primary research studies, either prospective or retrospective, while the remaining five were high-quality review or modeling articles (Table 2). Data originated from the United States, Italy, Japan, Ireland, South Korea, and multinational datasets, including large-scale analyses such as atomic bomb survivor follow-ups and BEIR VII risk models.
3.1. Sample Characteristics
Sample sizes ranged from large-scale epidemiological datasets (n ≈ 120,000) [13] to small intraoperative measurement cohorts (n = 60 procedures) [14]. Operator-specific exposure data were reported across all studies. Vascular (7), orthopedic (6) and trauma (5) surgery represented the largest specialty groups, followed by cardiology (2), interventional radiology (1). Cardiothoracic surgery was minimally represented, largely through modeled rather than directly measured exposure data. Follow-up durations ranged from six weeks to over 50 years for studies incorporating long-term cancer risk projections, with several extrapolating annual exposure from short-term dosimetry findings.
3.2. Radiation Exposure and Shielding Effectiveness
Intraoperative exposures were consistently reported. Without protective gear, chest-level doses averaged 0.08–0.11 mSv per procedure, and eye-level doses averaged 0.04–0.05 mSv per procedure. High-volume trauma surgeons demonstrated knee-thigh doses up to 2.7 mSv annually. When shielding was employed, attenuation was substantial: 0.25 mm lead aprons reduced exposure by ~90%, while 0.5 mm aprons achieved a reduction of ~99%. Lead glasses decreased ocular doses 2.5–4.5-fold, and thyroid collars reduced neck-level exposure by approximately 60–70%. Real-time dosimetry and phantom modeling confirmed shielding efficacy, with external-to-internal dose reductions up to 91.1%.
3.3. Cancer Incidence and Modeled Risk
Direct evidence of cancer incidence was limited, largely modeled or extrapolated, but notable. One Italian orthopedic study reported a 29% cancer incidence among exposed surgeons compared with 4% in non-exposed controls [13,16]. U.S. data showed a 2.9-fold higher breast cancer rate among female orthopedic surgeons, while cardiology studies indicated a median latency of ~22 years for head and neck tumors [13]. Modeled lifetime attributable risks (LAR) per million exposed individuals, based on BEIR VII data, included colon cancer at 424 (≈1 in 236), lung cancer at 447 (≈1 in 224), all solid cancers for male surgeons at 2079 (≈1 in 48), and cancer-related mortality across all sites at 1309 (≈1 in 76) [22]. These risk estimates were based on BEIR VII reports and extrapolated occupational exposures, assuming careers spanning ages 18–65 at consistent annual doses. These extrapolated results may not imply direct causality.
3.4. Comparison Groups and Risk Ratios
Several studies incorporated internal or external comparison groups, such as non-exposed staff or population baselines [13,15,21,22]. Reported effect sizes included a relative risk (RR) of 1.6 for solid cancers per 1 Sv exposure (atomic bomb survivor data), a hazard ratio (HR) of 4.04 for high-procedure cardiologists compared to low-procedure peers, and an RR of 3.2 (p < 0.005) for posterior lens opacities (cataracts).
3.5. Protection Protocols and Compliance
Lead aprons and thyroid collars demonstrated high compliance rates (90–99%) [15], while lead glasses showed inconsistent use [15,22,23,24], often due to interference with surgical loupes [22]. Seated procedures frequently showed unshielded gaps at the apron skirt edge, raising gonadal dose exposure. Several studies highlighted routine equipment integrity checks, real-time dosimeter use, and institutional enforcement of protective protocols as key areas for improvement.
3.6. Innovative Methodologies
Methodologies included real-time electronic personal dosimeters (EPD) and thermoluminescent dosimeters (TLD) mapped across body regions, phantom models simulating scatter radiation at variable distances and angles, and procedure-specific modeling comparing exposures across endovascular aneurysm repair (EVAR), angioplasty, and trauma cases.
3.7. Summary Statistics
Summary statistics are presented in Table 3. Across studies, the mean sample size was approximately 4200 (median 1200; range 60–120,000). Mean chest-level dose was ~0.10 mSv per procedure, and mean eye-level dose without lead was ~0.05 mSv per procedure. Gonadal exposure for busy trauma surgeons averaged ~2.7 mSv annually. The estimated relative risk for solid cancer per Sv was consistently reported at 1.6 (SD 0.1).
3.8. Key Trends and Insights
Key findings included: (1) Across specialties, shielding via lead aprons, thyroid collars, and glasses provided substantial dose reductions by 60–99% depending on body region and material thickness; (2) compliance gaps persisted, particularly regarding lead glasses usage and coverage of apron skirt edges; (3) phantom and modeled data closely mirrored measured exposure patterns via dose dosimetry but highlighted variability across procedures and operator roles; (4) direct specialty-specific cancer data remain scarce, with most conclusions extrapolated from surrogate dose reductions and modeled lifetime risks; and (5) practices and safety protocols differed markedly across regions, with international comparisons often referencing U.S. and European standards.
4. Discussion
This structured narrative review across 16 studies provides valuable insights into occupational radiation exposure among surgical and interventional proceduralists. While fluoroscopy-guided techniques continue to enhance minimally invasive care, cumulative ionizing radiation exposure remains an underrecognized occupational hazard, especially due to inconsistent protective practices and insufficient long-term outcome data.
Across included studies, operator doses reported were unshielded ~0.08–0.11 mSv/procedure at the chest and ~0.04–0.05 mSv/procedure at the eye. Lead aprons reducing exposure by ~90–99% and lead glasses reducing eye dose ~2.5–4.5×) can be benchmarked against current occupational limits to judge whether fluoroscopy-guided practice is typically “acceptable.” Under contemporary international guidance, the occupational effective-dose limit is 20 mSv/year averaged over 5 years (≤50 mSv in any single year), the lens limit is 20 mSv/year averaged over 5 years (≤50 mSv in any single year), and skin/extremities are limited at 500 mSv/year [2,29,30]. U.S. regulations permit a whole-body effective dose of 50 mSv/year, 150 mSv/year to the lens, and 500 mSv/year to the skin/extremities [31]. Interpreted against these thresholds, the per-procedure doses summarized here imply that routine practice with consistent shielding is generally compatible with remaining below annual effective-dose limits, while the lens and (in specific workflows) the hands are the most plausible limit-driving components. However, meeting dose limits should not be conflated with being “risk-averse”; limits are regulatory/occupational compliance thresholds, whereas stochastic effects such as cancer are probabilistic and are reduced by dose minimization rather than eliminated below any particular cutoff. Therefore, “acceptable risk” in fluoroscopy-guided practice is best interpreted as compliance plus optimization (ALARA), emphasizing consistent PPE, geometry optimization, and dosimetry strategies that specifically capture high-risk patterns of eye and extremity exposure in high-volume operators.
4.1. Shielding Efficacy and Practice Patterns
Our synthesis reaffirms that protective gear ranging from 0.25 mm to 0.5 mm lead-equivalent aprons, thyroid collars, and lead glasses provides substantial dose reduction (60–99%) across body regions. This aligns with existing recommendations that employ a combination of time, distance, and shielding (ALARA principles) to mitigate exposure risk. Additionally, newer comparative work indicates that traditional lead aprons often outperform lightweight alternatives, underscoring the importance of material integrity and equivalent thickness. These aprons should be considered for wider use.
Despite strong evidence supporting personal protective equipment (PPE), compliance gaps remain. While there is adherence to the usage of thyroid collars and aprons, lead glasses, crucial for eye protection, are underutilized, often due to interference with surgical optics (e.g., loupes). This supports broader findings that surgical trainees and attendings often express inadequate radiation safety education and concern over long-term risk, particularly regarding fertility and cancer. This area is a current actionable recommendation.
The variability observed across specialties, procedural roles, and exposed body regions highlights that occupational radiation risk is not uniform. Orthopedic trauma surgeons, interventional cardiologists, and other high-fluoroscopy practitioners demonstrate distinct exposure patterns, dose magnitudes, and long-term risk profiles. These differences underscore the need for risk-stratified approaches to occupational protection, in which monitoring practices, shielding selection, and institutional protocols are adapted to the specific exposure characteristics of different operator groups. Such stratification reflects an individualized framework consistent with modern precision-oriented occupational health. These specialty-specific exposure differences reinforce a precision-oriented approach to occupational health in which monitoring practices and protective strategies are tailored to the operator’s individualized risk profile, aligning this work with core principles of personalized medicine for protection of physicians using fluoroscopy in their practices.
4.2. Risk Estimation and Long-Term Health Outcomes
Direct epidemiological data on cancer incidence among operators are limited but concerning, nonetheless. One study reported markedly higher cancer rates in exposed orthopedic surgeons than controls, and elevated breast cancer rates among female surgeons were highlighted in U.S. data. Most risk assessments, however, rely on modeling using BEIR VII data to estimate lifetime attributable risk of cancers and mortality (e.g., ~1 in 48 for solid cancers; ~1 in 76 for cancer-related mortality). These estimates reflect a need for comprehensive occupational registries and longitudinal research.
Risk estimates from atomic bomb survivors yielding an RR of 1.6 per 1 Sv may not directly apply to proceduralists, whose exposures are typically lower and chronic. Nevertheless, findings such as a hazard ratio of 4.04 for high-volume interventional cardiologists and a relative risk of approximately 3.2 for cataracts indicate that even procedural-level exposures may carry significant health risks, though study heterogeneity limits meta-analysis and strong causal inference.
4.3. Implications for Practice and Future Research
Institutional commitment to comprehensive safety measures is imperative to better protect operators. Strategies such as routine integrity checks for protective gear, standardized compliance monitoring with dosimetry, and appointing a Radiation Safety Officer (RSO) to oversee adherence to ALARA principles have proven effective in other settings. Education tailored to proceduralists, potentially through advanced tools such as virtual reality (VR)-based radiation field visualization, could further improve compliance [32]. The importance of local diagnostic reference levels (DRLs) in the context of risk stratification and optimization of radiation protection for operators is also emphasized by recent studies indicating that taking into account local procedural and equipment conditions allows for a more accurate assessment of exposure and more effective implementation of ALARA principles [33]. Additionally, procedural modifications such as maintaining modest distance from scatter sources, beam collimation, pulsed fluoroscopy, and integrating ceiling-mounted shielding in hybrid OR setups can cumulatively reduce exposure.
Future research should prioritize prospective studies that track cumulative exposure and long-term outcomes such as cancer and other stochastic effects. Standardized reporting is needed to enable cross-study comparisons and meta-analysis. More studies will also reduce the heterogeneity of results and should allow subgroup analysis. Incorporating real-time dosimetry, phantom modeling, and registry-linked data can improve risk estimates, while studies testing and evaluating new shielding technologies, training strategies, and workflow changes may identify effective approaches to strengthen radiation safety practices.
4.4. Limitations
This structured narrative review has several limitations. Considerable heterogeneity was present in study designs, outcome measures, and reporting methods across the included papers. Longitudinal cancer outcome data were limited, as most studies focused on immediate or modeled radiation exposure rather than long-term health effects. Some specialties were underrepresented compared with others—for example, cardiothoracic surgery had fewer studies relative to orthopedics or interventional cardiology to generate appropriate strong data. In addition, adherence to protective equipment protocols and the rigor of monitoring practices varied substantially across institutions and operator groups. In addition, cancer risk models based on BEIR VII data may not be adequate for chronic, low-dose occupational exposure characteristic of fluoroscopy operators. Nevertheless, the aggregated findings provide valuable insights into the current state of occupational radiation safety practices in fluoroscopy-guided procedural specialties.
5. Conclusions
Operators across surgical and interventional specialties face considerable exposure to ionizing radiation during fluoroscopically guided procedures. Although protective measures achieve significant dose reductions, gaps in compliance, knowledge, and protocol implementation persist. Evidence linking exposure to long-term health outcomes remains limited, underscoring the need for standardized monitoring, rigorous safety practices, and well-designed longitudinal studies to guide future recommendations. The marked variability in exposure across specialties, procedural roles, and exposed body regions indicates that occupational risk is not uniform. Integrating risk-stratified monitoring and protective protocols may better address the distinct exposure patterns encountered by different operator groups and align with emerging precision-oriented approaches to occupational health. Anchoring these strategies within a personalized medicine framework underscores the need to tailor occupational protections to operator-specific exposure patterns, ensuring safety practices that reflect the individualized risk profiles identified in this review.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith-Bindman R. Chu P.W. Firdaus H.A. Stewart C. Malekhedayat M. Alber S. Bolch W.E. Mahendra M. de González A.B. Miglioretti D.L. Projected Lifetime Cancer Risks from Current Computed Tomography Imaging JAMA Intern. Med.2025185710719 Erratum in JAMA Intern Med. 2025, 185, 74710.1001/jamainternmed.2025.050540227719 PMC 11997853 · doi ↗ · pubmed ↗
- 2El Ghissassi F. Baan R. Straif K. Grosse Y. Secretan B. Bouvard V. Benbrahim-Tallaa L. Guha N. Freeman C. Galichet L. A review of human carcinogens--part D: Radiation Lancet Oncol.20091075175210.1016/S 1470-2045(09)70213-X 19655431 · doi ↗ · pubmed ↗
- 3López P.O. Dauer L. Loose R. Martin C. Miller D. VañóE. Doruff M. Padovani R. Massera G. Yoder C. on behalf of the ICRP. ICRP Publication 139: Occupational radiological protection in interventional procedures Ann. ICRP 201847111810.1177/014664531775035629532669 · doi ↗ · pubmed ↗
- 4Stewart F.A. Akleyev A.V. Hauer-Jensen M. Hendry J.H. Kleiman N.J. Macvittie T.J. Aleman B.M. Edgar A.B. Mabuchi K. Muirhead C.R. ICRP publication 118: ICRP statement on tissue reactions and early and late effects of radiation in normal tissues and organs--threshold doses for tissue reactions in a radiation protection context Ann. ICRP 201241132210.1016/j.icrp.2012.02.00122925378 · doi ↗ · pubmed ↗
- 5Matityahu A. Duffy R.K. Goldhahn S. Joeris A. Richter P.H. Gebhard F. The Great Unknown-A systematic literature review about risk associated with intraoperative imaging during orthopaedic surgeries Injury 2017481727173410.1016/j.injury.2017.04.04128648410 · doi ↗ · pubmed ↗
- 6Hamid M.A. Younis Z. Raza A. Tauseef A. Khan M.A.H. Mir S. Abdulsattar S. Rashid N. Radiation in the Orthopedic Operating Room: What We Know, What We Do, and What Needs Attention Cureus 202517 e 9091110.7759/cureus.9091141001315 PMC 12457730 · doi ↗ · pubmed ↗
- 7Calgary Orthopaedic Resident Research Group Quantification of Radiation Exposure in Canadian Orthopaedic Surgery Residents JBJS Open Access 20249 e 23-0017010.2106/jbjs.oa.23.0017039036642 PMC 11257669 · doi ↗ · pubmed ↗
- 8National Research Council (US) Committee on Health Effects of Exposure to Low Levels of Ionizing Radiations (BEIR VII) Health Effects of Exposure to Low Levels of Ionizing Radiations: Time for Reassessment?National Academies Press Washington, DC, USA 199825101445 · pubmed ↗