The Influence of Thermal and Mechanical Aging on the Flexural Properties of Conventional and 3D-Printed Materials Used in Occlusal Splints Manufacturing
Joanna Smardz, Katarzyna Kresse-Walczak, Heike Meißner, Klaus Böning, Joanna Weżgowiec, Andrzej Małysa, Mieszko Więckiewicz

TL;DR
This study compares how different materials used in dental appliances hold up under aging conditions, finding that some materials degrade more than others.
Contribution
The study provides new empirical evidence on the aging resistance and mechanical performance of UDMA-based resins compared to conventional and 3D-printed materials.
Findings
Thermocycling significantly reduced flexural strength in PMMA and SLA-printed resins.
UDMA-based material showed significantly lower flexural strength and modulus compared to PMMA and SLA-printed resins.
UDMA-based resins showed good aging resistance but lower initial mechanical properties.
Abstract
What are the main findings? Thermocycling significantly reduced flexural strength in PMMA and SLA-printed resins. UDMA-based material stayed unaffected under aging conditions. UDMA-based material showed significantly lower values of flexural strength and modulus when compared to PMMA and SLA-printed resins. What is the implication of the main findings? Material selection should consider both initial properties and long-term environmental changes. Occlusal splints are a type of intraoral appliance that are widely used for the management of temporomandibular disorders and bruxism, yet limited evidence exists regarding the comparative effects of combined aging on conventional and digitally manufactured materials. This in vitro study evaluated the influence of thermal and mechanical aging on the flexural properties of three materials commonly used for the manufacturing of occlusal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
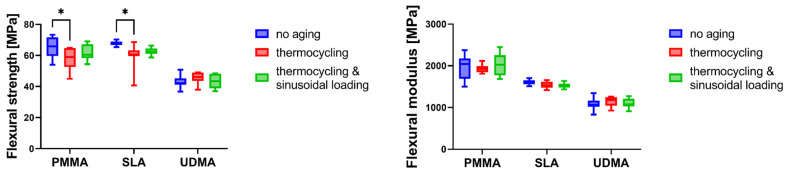 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental materials and restorations · Temporomandibular Joint Disorders · Orthodontics and Dentofacial Orthopedics
1. Introduction
Occlusal splints represent an essential element of conservative management for temporomandibular disorders (TMD) and bruxism, conditions that affect a substantial proportion of the adult population worldwide [1,2,3]. Epidemiological studies have consistently reported that TMD affects approximately 5–12% of the general population, with global prevalence estimates reaching 34% when broader diagnostic criteria are applied [2,3]. Similarly, bruxism prevalence ranges from 8% to 31% in adult populations, with significant regional variations [1,4]. Consequently, an estimated 8–12% of adults require some form of occlusal therapy during their lifetime, underscoring the clinical significance of intraoral appliance materials [1,2,3,4,5,6].
The therapeutic efficacy of occlusal splints in managing TMD and bruxism has been well-documented in the literature. Systematic reviews and meta-analyses have demonstrated that rigid stabilization splints produce significant reductions in chronic pain and improvements in mandibular mobility, with high reported improvement rates even when used as monotherapy [7,8,9]. Clinical studies examining long-term outcomes have reported significant symptom remission following splint therapy [10]. Furthermore, protective splints have been shown to potentially influence the risk of restoration failure among patients with bruxism, underscoring the importance of appliance durability for sustained clinical benefit [11].
The mechanical properties of materials used in intraoral appliance fabrication directly influence both therapeutic outcomes and clinical longevity [12,13]. Flexural strength and flexural modulus represent critical parameters that determine an appliance’s ability to withstand masticatory forces, resist deformation, and maintain dimensional stability throughout the treatment period [14,15]. The complex and dynamic oral environment subjects these materials to various degradation mechanisms, including thermal, mechanical, chemical and biological degradation [16,17,18].
Poly(methyl methacrylate) (PMMA) has long been the gold standard for denture base and splint fabrication, owing to its favorable processing characteristics, acceptable mechanical properties, and established clinical track record [19,20,21,22]. The emergence of urethane dimethacrylate (UDMA)-based resins has provided clinicians with alternative materials characterized by distinct polymerization chemistry and cross-linking characteristics [23,24]. UDMA monomers form highly cross-linked networks upon photopolymerization, potentially conferring enhanced resistance to hydrolytic degradation [25]. The flexible urethane linkages within the polymer backbone may provide improved toughness characteristics, although this structural feature can also result in reduced elastic modulus compared to PMMA-based materials [26]. Recent advances in digital dentistry have introduced additive manufacturing technologies, particularly stereolithography (SLA), as viable alternatives for occlusal devices fabrication [27,28]. Some of SLA-printed photopolymers are specifically formulated for long-term intraoral applications and have received regulatory clearance for occlusal splint production. Comparative studies have demonstrated that contemporary 3D-printed materials can be able to achieve mechanical properties comparable to or exceeding those of conventional autopolymerizing resins, although significant variability exists among different printing systems and materials [29,30,31]. Several studies demonstrate that additive manufacturing parameters, such as printing orientation and layer thickness, significantly influence the mechanical behavior and aging response of 3D-printed materials. Farkas et al. observed that thinner layers generally yielded higher tensile values [32]. In a recent in vitro investigation, Mudhaffer et al. reported that print orientation modulates flexural strength and modulus of resin materials indicated for definitive and interim dental restorations, with specimens printed at 90° exhibiting superior mechanical properties across multiple artificial aging time points (water storage at 37 °C), suggesting that orientation influences susceptibility to degradative processes [33]. Broader evidence from systematic analyses confirms that orientation affects various physical properties of 3D-printed polymeric dental restorations, including mechanical parameters that are known to deteriorate under artificial aging (e.g., water absorption, color stability, surface morphology), further supporting the need to consider these manufacturing variables in studies of long-term performance [34].
The influence of artificial aging on dental polymer properties has been extensively investigated using thermocycling protocols [35,36]. The standard thermocycling regimen (5 °C/55 °C) induces repeated thermal expansion and contraction cycles that can promote water absorption, polymer chain relaxation, and microcrack formation [35,36,37]. Studies examining PMMA-based materials have consistently reported significant reductions in flexural strength following thermocycling [38,39].
Mechanical fatigue is an additional degradation mechanism that may compromise material integrity, either independently or synergistically with thermal aging [40,41]. Cyclic loading may simulate the repetitive masticatory forces transmitted through occlusal splints during normal function and parafunctional activities [42]. It has been reported that cumulative mechanical damage can significantly reduce material longevity [43,44,45].
Despite extensive research on individual aging mechanisms, limited evidence exists regarding the combined effects of thermal and mechanical aging on materials explicitly used for the fabrication of occlusal devices. Furthermore, comparative data examining the aging behavior of conventional PMMA, UDMA-based resins, and 3D-printed photopolymers under standardized conditions remain scarce. Such information is essential for evidence-based material selection and for establishing realistic expectations regarding appliance longevity in clinical practice.
Therefore, the aim of this in vitro study was to evaluate the influence of thermal aging alone and combined thermal-mechanical aging on the flexural strength and flexural modulus of three materials commonly used for occlusal splints fabrication. The null hypotheses tested were: (1) artificial aging does not significantly affect the mechanical properties of the materials investigated, and (2) there are no significant differences among materials in their response to aging protocols.
2. Materials and Methods
2.1. Materials
The in vitro study presented evaluated three materials used to fabricate occlusal devices. These materials were selected based on their different chemical composition and manufacturing methodologies, as well as broad clinical application as reported in contemporary dental literature [46]:
- Classic self-curing poly(methyl methacrylate) (PMMA) resin (PMMA group, Estetic Ort; Wiedent, Łódź, Poland) representing the conventional approach to splints manufacturing This material consists of a powder and liquid component.
- Light-cured UDMA-based resin (UDMA group, Durasplint LC; Scheu Dental, Iserlohn, Germany). This material is supplied as pre-formed bars and consists primarily of UDMA matrix with minor additions of acrylic resin, photoinitiators, and crosslinkers.
- Photopolymer designed explicitly for 3D printing using SLA technology (SLA group, Dental LT Clear V1; Vertex Dental, Soesterberg, The Netherlands). This material is classified as a Class IIa biocompatible resin primarily composed of methacrylate oligomers, methacrylate monomers, and photoinitiators.
2.2. Preparation of Specimens
A total of 72 standardized specimens of rectangular shape were fabricated for this study (n = 24 from each material). The specimen dimensions (64 mm × 10.0 (±0.2) mm × 3.3 (±0.2) mm) were selected following the recommendations documented in similar investigations and PN-EN ISO 20795-1:2013 guidelines [46,47].
The PMMA specimens were prepared using a standardized compression molding technique with standardized metal molds to ensure dimensional accuracy [30,48,49]. The material was mixed according to the instructions of the manufacturer following powder-to-liquid ratio standardized at 3:1 by weight, packed into the molds at the dough-like stage, compressed between glass plates under 2.0 bar pressure, and allowed to polymerize for 20 min at room temperature (23 ± 1 °C), followed by 30 min in a pressure pot (Polyclav; Dentaurum, Ispringen, Germany) at 55 °C and pressure of 2.5 bar [49].
The UDMA-based specimens were prepared by compression molding using calibrated silicone molds to ensure dimensional accuracy. The specimens were then polymerized in a laboratory light-curing unit (LC-6 Light Oven; Scheu Dental, Iserlohn, Germany) for 2 × 10 min, with specimens inverted halfway through the process to ensure complete polymerization of both surfaces [46].
The SLA-printed specimens were designed using Meshmixer version 3.5.474 (Autodesk, San Francisco, CA, USA). Adding supports and setting printing parameters was made using PreForm software ver. 3.28.1 (Formlabs Inc., Somerville, MA, USA). A Form 2 printer (Formlabs) was used to print specimens at a resolution of 100 μm, and 90° printing orientation. When printed, the specimens were washed 2 × 10 min in 99% isopropanol (PPH STANLAB, Lublin, Poland), air-dried at room temperature for 30 min and postcured in a Form Cure (Formlabs) at 80 °C for 20 min. Finally, the supports were removed by cutting and grinding [46].
Following fabrication, all specimens were carefully inspected for defects such as porosities, inclusions, or dimensional irregularities to exclude and replace specimens exhibiting any visible defects. The specimen edges were polished with 1000-grit silicon carbide paper (P.S. Trading, Oltarzew, Poland) to remove processing artifacts. The water sandpaper (grit P500, P1000, P1200, P.S. Trading, Oltarzew, Poland) and 0.6 mm pumice stone powder (Everall7, Warsaw, Poland) were used to finish the specimens polishing paste for resin and metals (Everall7, Warsaw, Poland) was used to polish the upper side of each specimen using POLIRET Mini (REITEL Feinwerktechnik GmbH, Bad Essen, Germany) for 1 min. Finally, each specimen was rinsed under water [46] and underwent ultrasonic cleaning in distilled water with a mild detergent (Clean and clever, IGEFA Handelsgesellschaft mbH & Co. KG, Ahrensfelde, Germany) at 30 °C for 10 min (Elmasonic S30H; Elma Schmidbauer GmbH, Singen, Germany).
After that, the specimens of each material underwent a random division into three equal groups (n = 8 per group) according to the subsequent exposure: (1) no exposure (control group); (2) thermocycling of 10,000 cycles; (3) thermocycling of 10,000 cycles and cyclic loading of 1000 cycles.
2.3. Thermal Aging
A thermocycler (THE-1200; SD Mechatronik GmbH, Feldkirchen-Westerham, Germany) was used to simulate thermal aging with cyclical exposure to temperature-controlled distilled water (5 °C/55 °C). Each cycle lasted 77 s, with 27 s of immersion time in each water container and transfer time of 9 s. A total of 10,000 cycles were performed to simulate 12 months of use [48].
2.4. Mechanical Aging
The mechanical aging was conducted through sinusoidal alternating load (Universal Testing Machine Inspekt-Micro LC 100 N; Hegewald & Peschke, Meß- und Prüftechnik GmbH, Nossen, Germany) and resembled a cyclic three-point bending test in temperature-controlled artificial saliva at 37 °C (UKD saliva solution; University Pharmacy, Dresden, Germany). A point load (stainless steel ball Ø 10 mm) was applied to the specimen centrally. A frequency of 1 Hz, with a displacement of 2 mm, vertical deflection of the specimen under the load of 1 mm, a loading speed of 1 mm/s, and a preload of 1 N were used to perform bending cycles. A total of 1000 cycles were performed, which roughly correspond to 1 year of wear [48].
2.5. Flexural Properties Evaluation
Before testing, the specimens were conditioned in distilled water at 37 °C for 50 h. A Magnusson digital caliper (150 mm) (Limit, Alingsås, Sweden) was used to measure height and width of each specimen at 5 points. Immediately before testing, the mean cross-sectional area was calculated. The three-point bending test was performed using the Universal Testing Machine (Z10-X700; AML Instruments Ltd., Lincoln, UK) at a constant displacement rate of 5 mm/min and a span length of 50 mm between the supports [46,47]. The tests were conducted by a single investigator in accordance with the PN-EN ISO 20795-1:2013 guidelines [47].
Flexural strength (σ [MPa]) was calculated using the following formula (Equation (1)):
where F—maximum load [N]; l—distance between the supports [mm] (±0.01 mm); b—width of the specimen [mm]; and h—height of the specimen [mm].
Flexural modulus (E [MPa]) was determined using the following formula (Equation (2)):
where load (F) divided by displacement (d) is the slope in the linear elastic region of the load/displacement curve; l, b and h are as defined above [46].
2.6. Statistical Analysis
Statistical analysis was performed using GraphPad Prism version 9.0 (GraphPad Software Inc., San Diego, CA, USA). All data were expressed as mean ± standard deviation, and as box plots presenting the five-number summary of a dataset (minimum, first quartile, median, third quartile, and maximum). The normality of data distribution was verified using the Shapiro–Wilk test. All the data were normally distributed. A two-way analysis of variance (ANOVA) was employed to assess the effects of material type and aging method, as well as their interaction, on flexural strength and flexural modulus. When significant effects were detected, Tukey’s honestly significant difference post hoc test was applied for multiple pairwise comparisons. The level of statistical significance was set at α = 0.05 for all analyses.
3. Results
The flexural strength and flexural modulus values for all materials and aging conditions are presented in Table 1 and illustrated in Figure 1.
3.1. Effect of Aging on Flexural Strength
Within-group comparisons revealed a distinctive pattern in the response to aging protocols. Thermocycling alone significantly reduced flexural strength in both PMMA and SLA groups compared to baseline values (p < 0.05 for both comparisons). The PMMA group demonstrated a decrease from 65.19 ± 6.68 MPa to 57.94 ± 7.15 MPa. Similarly, the SLA group exhibited a reduction from 67.67 ± 1.54 MPa to 59.37 ± 8.80 MPa. Notably, the combined thermocycling and mechanical loading protocol yielded intermediate values that did not differ significantly from baseline in either PMMA (61.53 ± 5.11 MPa, p ≥ 0.05) or SLA (62.55 ± 2.42 MPa, p ≥ 0.05) groups. In contrast, the UDMA group demonstrated stability across all aging conditions (p ≥ 0.05 for all comparisons) (Table 1, Figure 1).
3.2. Effect of Aging on Flexural Modulus
The flexural modulus data revealed no significant within-group differences for any material following aging protocols (p ≥ 0.05 for all comparisons) (Table 1, Figure 1).
3.3. Inter-Material Comparisons
Between-group comparisons revealed highly consistent patterns across all aging conditions (Table 2 and Table 3).
For flexural strength, PMMA and SLA groups showed no statistical differences under all conditions (p > 0.05). UDMA demonstrated significantly lower flexural strength compared to both PMMA and SLA groups across all aging groups (p < 0.0001 in all comparisons). The magnitude of these differences was substantial: Flexural strength of PMMA exceeded UDMA by 12.45 to 22.06 MPa, while SLA exceeded UDMA by 13.88 to 24.54 MPa, depending on aging condition (Table 2).
For flexural modulus, all inter-material comparisons achieved statistical significance (p < 0.0001). A consistent hierarchy was observed: PMMA > SLA > UDMA across all conditions. The mean difference of flexural modulus between PMMA and UDMA ranged from 790.1 to 937.5 MPa, while the difference between PMMA and SLA ranged from 362.5 to 515.4 MPa, and between SLA and UDMA from 399.0 to 531.9 MPa (Table 3).
4. Discussion
The present study investigated the effects of thermal and mechanical aging on the flexural properties of three materials used for occlusal splints fabrication. The results demonstrated material-specific responses to aging protocols, with thermocycling alone significantly reducing flexural strength in PMMA and SLA groups, while UDMA group exhibited stability under all tested conditions. These findings lead to partial rejection of the first null hypothesis, as aging significantly affected the mechanical properties of specific materials under specific conditions. The second null hypothesis was rejected, as significant differences among materials were observed both in baseline properties and in their response to aging protocols. A consistent hierarchy was observed: PMMA > SLA > UDMA for flexural modulus; PMMA and SLA > UDMA for flexural strength across all conditions.
The significant reduction in flexural strength observed in PMMA following thermocycling is consistent with previous investigations examining the effects of thermal aging on acrylic resins [38,39]. This degradation can be attributed to several interconnected mechanisms operating at the molecular level. Water absorption during thermal cycling causes plasticization of the polymer matrix, with water molecules diffusing between polymer chains and disrupting intermolecular hydrogen bonding [50,51,52]. The repeated thermal expansion and contraction cycles induce internal stresses that may exceed the material’s yield strength locally, promoting microcrack initiation and propagation [53]. The SLA-printed resin demonstrated a similar pattern of degradation following aging, which aligns with recent literature on 3D-printed dental materials [54,55]. The layer-by-layer manufacturing process inherent to SLA technology creates interfaces between successive layers that may act as preferential pathways for water penetration and stress concentration [56,57]. Despite post-curing protocols designed to maximize degree of conversion, residual unreacted monomers may leach from the polymer network when exposed to aqueous environments, creating voids that compromise mechanical integrity [58]. The stability of UDMA-based material under thermal and mechanical aging conditions represents a noteworthy finding with important clinical implications. UDMA forms highly cross-linked networks through photopolymerization, with the urethane linkages providing both flexibility and hydrolytic resistance [25,59]. Previous investigations have reported that UDMA-based dental materials achieve degrees of conversion higher than those observed in other systems [24,60]. This enhanced conversion results in a more completely polymerized network with fewer unreacted methacrylate groups susceptible to hydrolysis. Additionally, the cross-linked architecture restricts polymer chain mobility and limits water diffusion into the bulk material [61].
Thermocycling exposes polymer-based dental materials to repeated temperature fluctuations in an aqueous environment, which can accelerate water uptake and thermo-mechanical stress development. For PMMA-based materials, absorbed water is widely described as a plasticizer that increases free volume and chain mobility, promotes polymer chain relaxation, and can reduce resistance to crack initiation/propagation under bending. This mechanism is consistent with our results, where PMMA showed a measurable decrease in flexural strength after thermocycling (≈−11%), while the flexural modulus changed only marginally (≈−2%). Similar findings have been reported for denture base and resin-based polymers subjected to thermocycling, where flexural properties decrease as a consequence of water–polymer interactions and thermal fatigue [62,63].
In contrast, the comparatively stable performance of the UDMA-based material in our study (for flexural strength ≈+6% after thermocycling and ≈+0.4% after combined aging) can be explained by the characteristics of UDMA networks. UDMA-containing materials form cross-linked polymer structures that restrict long-range segmental motion, thereby limiting water-induced softening and delaying relaxation-driven loss of strength. Structural property analyses of dental UDMA-based materials emphasize the key role of conversion/crosslink density and intermolecular interactions in controlling mechanical stability and water sorption–related effects. Moreover, experimental aging studies on UDMA networks show that water uptake may follow diffusion-governed behavior and that hydrolytic aging is strongly governed by polymer chemistry and network architecture [24,64,65].
Finally, the SLA 3D-printed resin also demonstrated a reduction in flexural strength after thermocycling (≈−12%), which aligns with the broader additive-manufacturing literature showing that such materials can present higher water sorption/solubility and measurable property shifts after thermal cycling. This may be related to factors such as residual monomer, degree of conversion, and microstructural heterogeneity (including interlayer interfaces) that can facilitate water diffusion and aging-related weakening [66,67].
The finding that combined thermal and mechanical aging did not differ significantly from baseline values, while thermocycling alone produced a significant change initially appears counterintuitive, as cumulative damage from sequential stress exposures would be expected. However, several plausible mechanisms may explain this phenomenon. The first hypothesis involves strain-induced structural reorganization. Cyclic mechanical loading may induce microstructural changes that partially compensate for thermal degradation, a phenomenon recognized in polymer science as strain hardening or stress-induced chain alignment. Repetitive bending cycles could promote reorganization of polymer chains into more mechanically favorable orientations, effectively counteracting the disruptive effects of thermal cycling on the polymer network [40,41,68,69]. However, the strain hardening hypothesis is extrapolated from general polymer physics literature and has not been directly validated for occlusal splint materials under the specific loading conditions employed in this study. Future research should directly investigate polymer chain reorganization in dental resin materials subjected to combined thermal-mechanical aging protocols as well as to mechanical aging alone, for comparative purposes. Alternatively, the water absorption occurring during thermocycling may have induced plasticization effects that allowed the polymer matrix to accommodate subsequent mechanical stresses more readily, reducing stress concentration at defect sites [25,63,70]. On the other hand, taking into consideration the explorative character of our work, the results obtained could be the effect of small sample size that could influence not detecting the difference between baseline and aging conditions.
When comparing the present results to requirements for denture base polymers, important distinctions emerge among materials. The standard minimum flexural strength of 65 MPa and flexural modulus of 2000 MPa for Type 1 (heat-polymerized) and Type 4 (light-activated) materials, with slightly relaxed requirements for Type 2 (autopolymerized) materials (60 MPa and 1500 MPa, respectively) were defined [47]. In the control (non-aged) group, both PMMA (65.19 ± 6.68 MPa) and SLA (67.67 ± 1.54 MPa) met or exceeded flexural strength requirement for the Type 1 and 4 materials, while UDMA (43.12 ± 4.37 MPa) fell substantially below this threshold. Following thermocycling, neither PMMA (57.94 ± 7.15 MPa) nor SLA (59.37 ± 8.80 MPa) maintained compliance with Type 1 requirements, although both remained close to the Type 2 threshold. However, it should be noted that PMMA values of flexural strength in control group obtained in this study were lower than those reported in the literature [71]. Regarding flexural modulus, only PMMA specimens achieved values exceeding 2000 MPa, and this occurred only in the combined aging group (2036.83 ± 263.60 MPa). SLA and UDMA materials demonstrated consistently lower modulus values across all conditions, ranging from 1077.41 to 1609.32 MPa. While lower elastic modulus may provide some advantages in terms of stress distribution and patient comfort, excessively flexible appliances may fail to provide adequate occlusal stabilization or protection against parafunctional forces, as well as they will be less resistant to deformation [10,14,15].
The flexural strength observed between PMMA and SLA materials across all conditions did not differ significantly. This supports the clinical viability of 3D-printed intraoral appliances. Recent systematic reviews suggest that contemporary additive manufacturing technologies can produce dental devices with mechanical properties equivalent to or exceeding those of conventional fabrication methods [29,30,72]. In contrast, Benli et al. reported that 3D-printed splint materials should not be considered as the primary choice for long-term treatments due to their low mechanical and chemical properties [73]. The digital workflow associated with SLA printing offers additional advantages, including improved dimensional accuracy, reduced laboratory time, and enhanced reproducibility compared to manual fabrication techniques [74]. Summarizing, the statistical similarity between PMMA and SLA flexural strength across all aging conditions represents an important finding for clinical practice. The choice between conventional PMMA and SLA-printed resin should therefore be guided by other factors, including fabrication workflow, dimensional accuracy, cost-effectiveness, and aesthetic requirements, rather than flexural strength considerations.
The significantly lower flexural strength of UDMA was consistent across all conditions. It presents both advantages and limitations for clinical application. The urethane linkages provide both flexibility and enhanced hydrolytic resistance compared to the ester linkages predominant in PMMA, while the high degree of conversion results in fewer unreacted functional groups susceptible to degradation [75]. However, the stability of UDMA comes at the cost of substantially lower absolute mechanical properties. The clinical decision therefore involves a trade-off: PMMA and SLA offer higher initial strength but with potential for some degradation over time (and in the case of SLA, with greater unpredictability), while UDMA offers substantially lower but consistent properties throughout the service life. To overcome this disadvantage, another option which could be applied includes the combination of the UDMA-based material, which is considered as an adjustment, with the base fabricated from thermoformed material, e.g., polyethylene terephthalate glycol (PET-G). This could potentially improve the low mechanical properties of UDMA. Our previous research provided evidence regarding superior chemical stability of such combination over conventional heat-activated PMMA and 3D-printable Dental LT clear resin [75]. As biological risks associated with the leakage of compounds upon long-term interaction of dental materials with the complex intraoral environment must be minimized, such observations should also be considered in the process of material selection.
Several limitations of the present study should be acknowledged. The simplified rectangular specimen geometry does not replicate the complex three-dimensional architecture of clinical intraoral appliances [76]. The aging protocols did not incorporate salivary enzymes, pH variations, or biofilm formation [17,77]. The mechanical loading protocol (1000 cycles) may not adequately simulate cumulative fatigue in patients with severe parafunctional habits [78]. Moreover, cyclic loading tests were reported to require more standardized guidelines for testing and reporting; thus, it should be clarified that current standards and the available literature do not define a universally accepted number of cycles for fatigue-based artificial aging of dental polymer materials [79]. The lack of complementary microstructural and chemical characterization before and after aging could also be considered as limitation of presented study. The scanning electron microscopy and Fourier transform infrared spectroscopy could have provided direct evidence of aging-related morphological changes (e.g., microcracks/porosity) and polymer network alterations, enabling a more mechanistic explanation of the observed mechanical property changes. Finally, only single representatives from each material category were evaluated.
5. Conclusions
Thermocycling alone significantly reduced flexural strength in both PMMA and SLA-printed materials. UDMA-based resin exhibited stability under all aging protocols but with substantially lower absolute flexural strength. Only PMMA specimens approached Type 1 requirements for flexural modulus (≥2000 MPa). While UDMA-based resin showed superior aging stability, its lower baseline mechanical properties may limit its application in high-stress clinical scenarios compared to PMMA and SLA-printed materials. Results obtained in this study suggest that material selection for occlusal splints should consider both the specific mechanical demands of the clinical application and the expected duration of service. Considering flexural strength and modulus, PMMA still seems to be material of choice for occlusal splints fabrication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zieliński G. Pająk A. Wójcicki M. Global Prevalence of Sleep Bruxism and Awake Bruxism in Pediatric and Adult Populations: A Systematic Review and Meta-Analysis J. Clin. Med.202413425910.3390/jcm 1314425939064299 PMC 11278015 · doi ↗ · pubmed ↗
- 2Zieliński G. Pająk-Zielińska B. Ginszt M. A Meta-Analysis of the Global Prevalence of Temporomandibular Disorders J. Clin. Med.202413136510.3390/jcm 1305136538592227 PMC 10931584 · doi ↗ · pubmed ↗
- 3Ohrbach R. Dworkin S.F. The Evolution of TMD Diagnosis: Past, Present, Future J. Dent. Res.2016951093110110.1177/002203451665392227313164 PMC 5004241 · doi ↗ · pubmed ↗
- 4Lobbezoo F. Ahlberg J. Raphael K.G. Wetselaar P. Glaros A.G. Kato T. Santiago V. Winocur E. De Laat A. De Leeuw R. International Consensus on the Assessment of Bruxism: Report of a Work in Progress J. Oral Rehabil.20184583784410.1111/joor.1266329926505 PMC 6287494 · doi ↗ · pubmed ↗
- 5Zhang S.H. He K.X. Lin C.J. Liu X.D. Wu L. Chen J. Rausch-Fan X. Efficacy of occlusal splints in the treatment of temporomandibular disorders: A systematic review of randomized controlled trials Acta Odontol. Scand.20207858058910.1080/00016357.2020.175981832421379 · doi ↗ · pubmed ↗
- 6Al-Moraissi E.A. Farea R. Qasem K.A. Al-Wadeai M.S. Al-Sabahi M.E. Al-Iryani G.M. Effectiveness of occlusal splint therapy in the management of temporomandibular disorders: Network meta-analysis of randomized controlled trials Int. J. Oral Maxillofac. Surg.2020491042105610.1016/j.ijom.2020.01.00431982236 · doi ↗ · pubmed ↗
- 7Fricton J. Look J.O. Wright E. Alencar F.G.P.Jr. Chen H. Lang M. Ouyang W. Velly A.M. Systematic Review and Meta-Analysis of Randomized Controlled Trials Evaluating Intraoral Orthopedic Appliances for Temporomandibular Disorders J. Orofac. Pain 20102423725420664825 · pubmed ↗
- 8Kuzmanovic Pficer J. Dodic S. Lazic V. Trajkovic G. Milic N. Milicic B. Occlusal Stabilization Splint for Patients with Temporomandibular Disorders: Meta-Analysis of Short and Long Term Effects P Lo S ONE 201712 e 017129610.1371/journal.pone.017129628166255 PMC 5293221 · doi ↗ · pubmed ↗