Immunalysis tapentadol assay reformulation resolves tramadol interference
Adeolu O Adegoke, Alexandria N Jackson, Sonia L La’ulu, Chelsie Anderson, Joseph W Rudolf, Jessica M Boyd, Kamisha L Johnson-Davis

TL;DR
A new reformulated test kit for tapentadol reduces false positives caused by tramadol interference, improving drug screening accuracy.
Contribution
A reformulated assay kit is introduced to resolve tramadol cross-reactivity in tapentadol urine screening.
Findings
61% of false-positive tapentadol samples contained tramadol below the reported cross-reactivity threshold.
The reformulated kit eliminated false positives and aligned with LC–MS/MS confirmation.
False-positive rates significantly decreased after implementing the new kit in routine testing.
Abstract
This study evaluated the performance of the Immunalysis Tapentadol 343 Urine Enzyme Immunoassay (EIA) screening kit, focusing on the prevalence of false-positive results due to cross-reactivity with tramadol. Tapentadol is a dual-action analgesic, modulating μ-opioid receptors and inhibiting norepinephrine reuptake, while tramadol, a structurally related compound, is a weak μ-opioid receptor agonist and norepinephrine/serotonin reuptake inhibitor. Cross-reactivity between these compounds can complicate urine drug screening results for adherence monitoring in chronic pain management. A total of 28 samples initially produced false-positive results for tapentadol BNl using the Immunalysis Tapentadol 343 Urine EIA screening kit. Liquid chromatography–tandem mass spectrometry (LC–MS/MS) was used to confirm the absence of tapentadol. Of the false-positive samples, 61% contained tramadol at…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
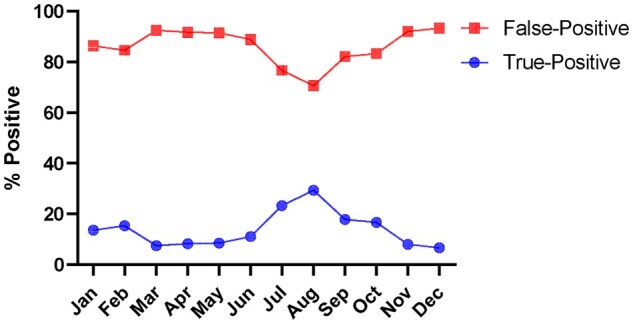 Figure 1
Figure 1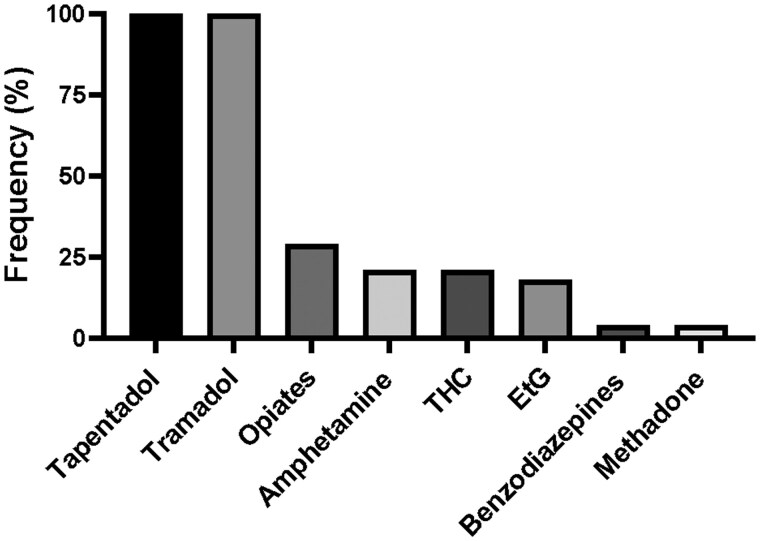 Figure 2
Figure 2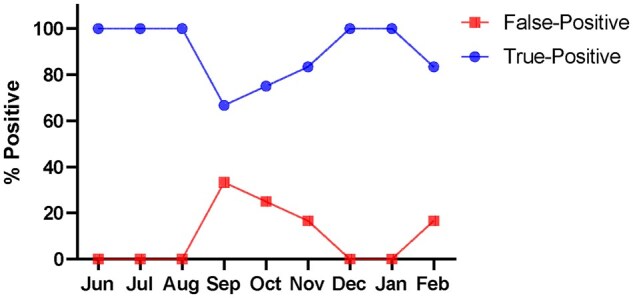 Figure 3
Figure 3| ID | Tapentadol (ng/mL) | Tramadol (ng/mL) |
|
|---|---|---|---|
| E01 | <50 | 30 000 | 8503 |
| E02 | <50 | 50 809 | 6810 |
| E03 | <50 |
| 30 174 |
| E04 | <50 | 52 389 | 3834 |
| E05 | <50 |
| 6494 |
| E06 | <50 | 53 063 | 14 020 |
| E07 | <50 | 37 702 | 14 795 |
| E08 | <50 |
| 54 062 |
| E09 | <50 | 13 908 | 5037 |
| E10 | <50 | 6901 | 6854 |
| E11 | <50 | 59 859 | 16 688 |
| E12 | <50 |
| 29 200 |
| E13 | <50 | 17 317 | 2797 |
| E14 | <50 | 14 788 | 11 040 |
| E15 | <50 |
|
|
| E16 | <50 | 17 180 | 6487 |
| E17 | <50 | 28 471 | 5943 |
| E18 | <50 | 20 833 | 6413 |
| E19 | <50 |
| 30 268 |
| E20 | <50 |
| 10 699 |
| E21 | <50 | 37 367 | 13 670 |
| E22 | <50 |
| 15 129 |
| E23 | <50 | 13 172 | 6174 |
| E24 | <50 |
| 21 447 |
| E25 | <50 | 10 027 | 1479 |
| E26 | <50 |
| 11 741 |
| E27 | <50 | 23 806 | 7795 |
| E28 | <50 |
|
|
| Assay | Old Kit-343 | ARK Tram | LC–MS/MS | New Kit-343UR | |||
|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
| ||
|
|
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
|
| Tap-Lo-Neat-01 | Tap (150) | Neg | Neg | 172 | 0 | 0 | Neg |
| Tap-Lo-Neat-02 | Tap (150) | Neg | Neg | 185 | 0 | 0 | Neg |
| Tap-Lo-Neat-03 | Tap (150) | Neg | Neg | 134 | 0 | 0 | Neg |
| Tap-Hi-Neat-01 | Tap (250) | Pos | Neg | 280 | 0 | 0 | Pos |
| Tap-Hi-Neat-02 | Tap (250) | Pos | Neg | 265 | 0 | 0 | Pos |
| Tap-Hi-Neat-03 | Tap (250) | Pos | Neg | 329 | 0 | 0 | Pos |
| Tap-Lo-Tram-01 |
Tap (150) Tram (107 000) | Pos | Pos | 156 | 119,943 | 0 | Neg |
| Tap-Lo-Tram-02 |
Tap (150) Tram (65 000) | Pos | Pos | 162 | 53,845 | 0 | Neg |
| Tap-Lo-Tram-03 |
Tap (150) Tram (48 000) | Pos | Pos | 162 | 40,430 | 0 | Neg |
| Tap-Hi-Tram-01 |
Tap (250) Tram (107 000) | Pos | Pos | 242 | 86,043 | 0 | Pos |
| Tap-Hi-Tram-02 |
Tap (250) Tram (65 000) | Pos | Pos | 267 | 54,480 | 0 | Pos |
| Tap-Hi-Tram-03 |
Tap (250) Tram (48 000) | Pos | Pos | 282 | 36,892 | 0 | Pos |
| Tap-Lo- |
Tap (150)
| Pos | Pos | 147 | 0 | 136,811 | Pos |
| Tap-Lo- |
Tap (150)
| Pos | Pos | 148 | 0 | 65,920 | Pos |
| Tap-Lo- |
Tap (150)
| Pos | Pos | 151 | 0 | 46,638 | Neg |
| Tap-Hi- |
Tap (250)
| Pos | Pos | 231 | 0 | 121,920 | Pos |
| Tap-Hi- |
Tap (250)
| Pos | Pos | 246 | 0 | 53,400 | Pos |
| Tap-Hi- |
Tap (250)
| Pos | Pos | 270 | 0 | 45,840 | Pos |
| Assay | New Kit-343UR | Old Kit-343 | ||
|---|---|---|---|---|
| Cut-off | 200 ng/mL | 200 ng/mL | ||
| Cut-off Normalized | 100 ng/mL | 100 ng/mL | ||
| ID |
| Interpretation |
| Interpretation |
| E01 | 20 | Neg | 112 | Pos |
| E02 | 31 | Neg | 120 | Pos |
| E03 | 55 | Neg | 160 | Pos |
| E04 | 8 | Neg | 122 | Pos |
| E05 | 15 | Neg | 117 | Pos |
| E06 | 11 | Neg | 134 | Pos |
| E07 | 21 | Neg | 121 | Pos |
| E08 | 50 | Neg | 118 | Pos |
| E09 | 26 | Neg | 132 | Pos |
| E10 | 9 | Neg | 106 | Pos |
| E11 | 23 | Neg | 156 | Pos |
| E12 | 52 | Neg | 120 | Pos |
| E13 | 12 | Neg | 126 | Pos |
| E14 | 22 | Neg | 109 | Pos |
| E15 | 86 | Neg | 150 | Pos |
| E16 | 9 | Neg | 113 | Pos |
| E17 | 23 | Neg | 155 | Pos |
| E18 | 12 | Neg | 128 | Pos |
| E19 | 33 | Neg | 111 | Pos |
| E20 | 19 | Neg | 115 | Pos |
| E21 | 21 | Neg | 107 | Pos |
| E22 | 25 | Neg | 113 | Pos |
| E23 | 6 | Neg | 100 | Pos |
| E24 | 51 | Neg | 114 | Pos |
| E25 | 12 | Neg | 109 | Pos |
| E26 | 25 | Neg | 145 | Pos |
| E27 | 28 | Neg | 139 | Pos |
| E28 | 71 | Neg | 150 | Pos |
- —ARUP Institute for Clinical and Experimental Pathology10.13039/100013213
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForensic Toxicology and Drug Analysis · Veterinary Pharmacology and Anesthesia · Opioid Use Disorder Treatment
Introduction
Chronic pain remains a prevalent and challenging condition, necessitating the development of effective analgesics with improved safety profiles. Tapentadol, introduced as a novel analgesic, is characterized by its dual mechanism of action, designed to address pain through μ-opioid receptor (MOR) modulation and norepinephrine (NE) reuptake inhibition [1, 2]. A similar analgesic, tramadol, demonstrates modest agonistic effects on MOR and concurrently acts as an inhibitor of serotonin and NE reuptake [3].
Tapentadol is listed under Schedule II of the United States Controlled Substances Act [4], and adherence/compliance monitoring to prescribed medication and/or misuse of tapentadol can be evaluated by urine drug screens (UDS), which may employ an immunoassay (IA) technique to identify the presence of the parent drug or its metabolite in urine. IAs are widely used in UDS due to their ease of use, automation adaptation, and quick turnaround time. However, analyte-specific antibody cross-reactivity with structurally related and unrelated compounds in sample matrices is a major limitation of IA, potentially resulting in false-positive outcomes [5, 6]. To minimize reporting false-positive UDS, confirmatory testing with gas chromatography–mass spectrometry (GC–MS) or liquid chromatography–tandem mass spectrometry (LC–MS/MS) is recommended [6].
The high costs of performing MS testing, longer turnaround time to results, and limited availability of MS methods leave the care providers with decisions regarding patient care based on “presumptive-positive” drug screening results until confirmatory testing is performed. While unconfirmed IA screening results should never be used to make definitive clinical or legal decisions, in practice, such results are sometimes inappropriately acted upon. This misuse can lead to serious consequences, including inappropriate removal from pain management programs, adverse employment actions, or unjustified involvement of child and family services [7, 8].
In addition, physicians may also have knowledge gaps regarding drug metabolism and assay limitations, such as IA cross-reactivity, the risk of false positive and false negative results, when interpreting UDS tests, which can negatively impact patient care [9–11].
In this study, we investigated the cause of increased false-positive tapentadol results in our UDS assay, utilizing both IA and LC–MS/MS methods. Our findings shed light on the complexities involved in accurately screening tapentadol in urine samples using IA method, particularly in the presence of high tramadol concentrations.
Materials and methods
Patient samples
Previously analyzed random urine samples were saved for analysis in compliance with the University of Utah Institutional Review Board (IRB #00082990). Specimens were stored at −20°C until analysis. After thawing, urine samples were mixed thoroughly before taking aliquots. The age range of the patients whose samples were selected was 34–85 years old, and their sex distribution was 9 males and 19 females.
Synthetic urine preparation
Synthetic urine was prepared in nanopure water by ARUP Laboratories Reagent Lab, (Salt Lake City, UT, USA) with the following constituents, and final concentrations: 0.33 M urea, 0.12 M sodium chloride, 0.016 M potassium diphosphate, 0.007 M creatinine and 0.004 M sodium monophosphate.
Immunoassay kits
UDS was performed using the Drug Profile, Screen with Reflex to Quantitation assay at ARUP Laboratories (Test Code: 2012312). The screening utilized IA reagents from multiple manufacturers, processed on the Beckman Coulter AU5800 Series Clinical Chemistry Analyzer. The following reagent kits were used: Tapentadol 343 Urine EIA (Old Kit-343, Cat. #343-0500) and Tapentadol 343UR Urine HEIA (New Kit-343UR, Cat. #343UR-0500) from Immunalysis Corporation, Pomona, CA, USA; Tramadol (Cat. #5040-0001-02) and Ethyl Glucuronide (EtG) from ARK Diagnostics, Inc., CA, USA; Emit^®^ II Plus Drug Screening for opiates, amphetamines, cannabinoids (THC), benzodiazepines, and methadone from Siemens Healthcare Diagnostics Inc., DE, USA. The screening cutoff concentration for each analyte is: tapentadol = 200 ng/mL, tramadol = 100 ng/mL, EtG = 500 ng/mL, opiates = 300 ng/mL, amphetamines = 300 ng/mL, THC = 50 ng/mL, benzodiazepines = 200 ng/mL, and methadone = 150 ng/mL.
Mass spectrometry confirmation
All presumptive-positive UDS IA results were confirmed by LC–MS/MS at ARUP Laboratories [12–16]. Briefly, deuterated analogs of tramadol, O-desmethyltramadol, and tapentadol were used as internal standards (IS) and added to aliquots of urine specimens to account for variability during extraction and analysis. This method does not include a hydrolysis step. Tramadol and O-desmethyltramadol were extracted using solid-phase extraction, while tapentadol was separated using liquid protein crash extraction. The tramadol extracts were reconstituted in mobile phase and analyzed using an AB Sciex Triple Quad 5500 LC–MS/MS system with positive-mode electrospray ionization, and the tapentadol extracts were injected into an Agilent 6470 Triple Quad LC–MS/MS, both instruments are equipped with an Agilent 1260 Infinity II Rapid Resolution HPLC. Analytes were separated by HPLC, followed by fragmentation of selected precursor ions into product ions by collision with neutral gas molecules, with multiple reaction monitoring used to track the transitions. Data acquisition and analysis were performed using AB Sciex Analyst and Indigo^®^ software, with quantitation based on comparison to calibration curves. A specimen was reported as positive if the drug concentration exceeded the confirmation cutoff concentration (i.e. tapentadol = 50 ng/mL; tramadol and O-desmethyltramadol = 25 ng/mL). Calibrators and controls were processed alongside the specimens to ensure calibration and procedural verification.
Statistical analysis
Statistical analysis and data visualization were performed in Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and GraphPad Prism (GraphPad Software, La Jolla, CA, USA).
Results
Presumptive-positive Tapentadol IA UDS were automatically subjected to confirmation by LC–MS/MS. However, persistently elevated rates of false-positives in the tapentadol IA were observed over 12 months. The percentage of false-positive tapentadol UDS calculated as [(# of samples Confirmed Negatives (CN)/# of samples that are Screen Positives (SP)) x100] was persistently >70% (Fig. 1).
Percentage of false-positive tapentadol UDS samples among the screen positive cases between January and December 2023.
To characterize the false-positive tapentadol UDS, 28 samples that screened presumptively-positive for tapentadol were selected for screening by our UDS panel, which also screens for opiates, methadone, benzodiazepine, tramadol, EtG, THC, and amphetamine. The drug screen results for these patients were evaluated, and all 28 (100%) samples, that were presumptive-positives for tapentadol, were also presumptively- positive for tramadol (Fig. 2). However, only 29% of the screened samples were presumptively-positive for opiates, 21% were presumptive-positives for amphetamine and THC, 18% were presumptively-positive for EtG, and 4% were presumptive-positives for benzodiazepines and methadone (Fig. 2). This suggests that tramadol might cross-react with the tapentadol IA to generate false-positive tapentadol results.
Percentage frequency of drug analyte positivity in the urine samples (n = 28) with false-positive tapentadol IA UDS.
Per the package insert of Old Kit-343 (Revision: E.0, Revision Date: 09/2015), a tramadol concentration of 60 000 ng/mL, generated 0.3% cross-reactivity with tapentadol UDS (assay cutoff = 200 ng/mL). Although cross-reactivity of 0.3% is negligible, we speculated that the 28 samples with false-positive tapentadol UDS would have tramadol concentrations significantly higher than 60,000 ng/mL (i.e. the tramadol concentration where cross-reactivity was reported in the package insert). To examine this, quantitative LC–MS/MS analysis was performed, which showed the concentrations of tramadol and its metabolite, O-desmethyltramadol, in the 28 samples were between 6901 and 297 703 ng/mL and 1479–85 956 ng/mL, respectively (Table 1). Eleven out of 28 (39%) false-positive tapentadol samples had tramadol concentrations > 60 000 ng/mL, with 2 of these 11 samples (18%) having O-desmethyltramadol concentrations of > 60 000 ng/mL (Table 1). Meanwhile, all the false-positive samples had tapentadol concentrations of <50 ng/mL as confirmed by the LC–MS/MS method (Table 1).
In contrast to tramadol cross-reactivity at 60 000 ng/mL in tapentadol Old Kit-343, the package insert of the New Kit-343UR states that tramadol concentration of 100 000 ng/mL, equivalent to 200 ng/mL of tapentadol (assay cutoff = 200 ng/mL), generated < 0.2% cross-reactivity with tapentadol UDS. To examine the performance of the New Kit-343UR versus Old Kit-343, we made three aliquots of low (150 ng/ml) and high (250 ng/ml) tapentadol controls. One aliquot each of the low and high tapentadol control was left unspiked (“Neat”), spiked with tramadol (Tram), and spiked with O‐desmethyl‐tramadol (OTram). To replicate the tramadol cross-reactivity cutoff of Old Kit-343 (i.e. 60 000 ng/mL) and New Kit-343UR (i.e. 100 000 ng/mL), a slightly lower concentration (i.e. 48 000 ng/mL), and a slightly higher concentration of Tram and OTram (i.e. 65 000 ng/mL and 107 000 ng/mL) were spiked into the low and high tapentadol controls (Table 2). As expected, UDS with the tapentadol Old Kit-343 showed a presumptive-negative tapentadol screen for the low tapentadol controls not spiked with tramadol (Tap-Lo-Neat) and a presumptive-positive tapentadol screen for the high tapentadol controls not spiked with tramadol (Tap-Hi-Neat). In contrast, a presumptive-positive tapentadol screen (100%) was obtained with the Old Kit-343 in the low tapentadol controls spiked with Tram or OTram, regardless of their concentrations. In addition, the IA ARK Tramadol assay showed a presumptive-negative tramadol screen in the unspiked “Neat” controls, and a presumptive-positive screen in the Tram and OTram spiked tapentadol controls (Table 2). These IA results were confirmed by quantitative LC–MS/MS method, which showed the concentration of each analyte in the synthetic urine (Table 2). Although the New Kit-343UR showed a superior performance in comparison to Old Kit-343, Tap-Lo-OTram-01 and Tap-Lo-OTram-02 were falsely positive with the New Kit-343UR, suggesting that OTram is still cross-reacting at concentrations between 60 000 ng/mL—107 000 ng/mL (Table 2).
Having observed the improved performance of the New Kit-343UR, we re-tested the 28 false-positive patient samples in Fig. 2 and compared it with the Old Kit-343. In contrast to 100% false-positive results obtained with the Old Kit-343, all 28 (100%) samples were negative for tapentadol with the reformulated New Kit-343UR (Table 3), which was consistent with the results obtained with LC–MS/MS analysis in Table 1. This confirmed that the reformulated New Kit-343UR was less affected by tramadol cross-reactivity. Our lab switched to the new tapentadol reformulation kit in May 2024. Figure 3 shows a 34% reduction in the false positive rate with the New Kit-343UR, for June 2024—February 2025.
Percentage of false-positive tapentadol UDS samples among the screen positive cases between June 2024 and February 2025.
Discussion
UDS with IA kits have a fast turnaround time to result, are easily accessible, and are typically less expensive, in comparison to mass spectrometry analysis, to identify drugs in urine and to monitor adherence to drug therapy. However, cases of false-positive UDS have been documented [12, 17–22]. Our investigation was prompted by observations of increased false-positive rates with our tapentadol UDS. The Immunalysis Tapentadol Urine EIA Drug Screening (343) Kit indicates a 0.3% cross-reactivity with tapentadol when tramadol concentrations reached 60 000 ng/mL. However, despite this reported threshold, we identified false-positive tapentadol results in 28 samples with tramadol concentrations ranging from 6901 to 297 703 ng/mL, as determined by LC–MS/MS analysis. Notably, a significant proportion (61%) of these false-positive samples exhibited tramadol concentrations below 60 000 ng/mL, suggesting a potential discrepancy between the reported cross-reactivity threshold and our observed outcomes. Interestingly, our LC–MS/MS analyses revealed that all false-positive tapentadol samples had tapentadol concentrations below cutoff, indicating that either the current tapentadol package insert claim of the no cross-reactivity with ≤60 000 ng/mL tramadol is incorrect or there are other cross-reacting contaminants This incongruity raises concerns regarding the accuracy of the previous tapentadol package insert claims and highlights the need for further elucidation of potential cross-reacting contaminants or assay limitations.
To investigate the tramadol cross-reactivity in tapentadol UDS, we conducted experiments involving spiked synthetic urine samples with tramadol. Tapentadol UDS with the reformulated New Kit-343UR showed significant improvements in its specificity over Old Kit-343, particularly in terms of reducing tramadol cross-reactivity. Our initial results indicated that Old Kit-343 produced a high rate of false positives for tapentadol in the presence of tramadol. Of note, many individuals in our test population are on tramadol than tapentadol. Although New Kit-343UR demonstrated superior performance, the false-positive tapentadol screening observed in Tap-Lo-OTram-01 was not surprising based on the 100 000 ng/mL tramadol cross-reactivity mentioned in the package insert. Importantly, the retesting of 28 previously identified false-positive patient samples with the New Kit-343UR yielded no false positives, aligning perfectly with LC–MS/MS analysis results. In addition, the false-positive rate has declined since implementation of the New Kit-343UR.
Although our study clearly demonstrated tramadol-related false positives in urine tapentadol IA, determining the exact mechanism of cross-reactivity was beyond the scope of our work due to proprietary constraints on assay formulation details. Also, the specific modifications made by the manufacturer in the reformulated kit were not disclosed in the package insert. However, based on our data, we observed a dramatic reduction in tramadol-related false positives, suggesting that the changes were likely aimed at improving assay specificity. Further studies evaluating the exact nature of these modifications, if such information can be obtained from the manufacturer, would be beneficial. In addition, our interference testing was limited to tramadol and its primary phase I metabolite (O-desmethyltramadol). Given that glucuronidated metabolites may also contribute to cross-reactivity, additional studies assessing their impact would provide a more comprehensive understanding of tramadol interference in urine tapentadol IA. We encourage future work in this area, particularly since phase II metabolites are often abundant in urine and may have structurally relevant epitopes that contribute to antibody cross-reactivity.
This study is an example of a cautionary tale that cross-reactivity studies, conducted by the manufacturer, may not reflect the high concentrations and drug combinations that are present in authentic patient samples. It would be important for laboratories to verify manufacturer claims for cross-reactivity at higher concentrations and drug combinations reflected in the patient population. Laboratories should have a mechanism to track true and false positive rates, and it is imperative for laboratories to reach out to the manufacturer for troubleshooting if the assay does not meet expected performance. It is also important for laboratories to assess drug testing needs for clinicians to create an optimal test menu to support patient care.
Conclusion
Our study underscores the importance of interference studies for assay verification and continuous monitoring of potential cross-reactivity in UDS assays. Further research is warranted to elucidate the underlying mechanisms of tramadol cross-reactivity and to refine tapentadol UDS methodologies, ensuring accurate and reliable detection of tapentadol in clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kress HG. Tapentadol and its two mechanisms of action: Is there a new pharmacological class of centrally-acting analgesics on the horizon?Eur J Pain 2010;14:781–3.20659810 10.1016/j.ejpain.2010.06.017 · doi ↗ · pubmed ↗
- 2Tzschentke TM , Christoph T, Kögel BY. The mu-opioid receptor agonist/noradrenaline reuptake inhibition (MOR-NRI) concept in analgesia: the case of tapentadol. CNS Drugs 2014;28:319–29.24578192 10.1007/s 40263-014-0151-9 · doi ↗ · pubmed ↗
- 3Raffa RB , Friderichs E, Reimann W et al Opioid and nonopioid components independently contribute to the mechanism of action of tramadol, an ‘atypical’ opioid analgesic. J Pharmacol Exp Ther 1992;260:275–85.1309873 · pubmed ↗
- 4Drug Enforcement Administration. 2022 Drugs of abuse. https://www.dea.gov/sites/default/files/2022-12/2022_DOA_e Book_File_Final.pdf (20 December 2023, date last accessed).
- 5Herring C , Muzyk AJ, Johnston C. Interferences with urine drug screens. J Pharm Pract 2011;24:102–8.21507878 10.1177/0897190010380463 · doi ↗ · pubmed ↗
- 6Burton AW. Urine drug testing: current recommendations and best practices. Pain Physician 2012;15:ES 119–33.22786451 · pubmed ↗
- 7Manchikanti L , Malla Y, Wargo BW et al Comparative evaluation of the accuracy of immunoassay with liquid chromatography tandem mass spectrometry (LC/MS/MS) of urine drug testing (UDT) opioids and illicit drugs in chronic pain patients. Pain Physician 2011;14:175–87.21412372 · pubmed ↗
- 8Christo PJ , Manchikanti L, Ruan X et al Urine drug testing in chronic pain. Pain Physician 2011;14:123–43.21412368 · pubmed ↗