Awareness, Attitudes, and Barriers Toward Breast Symmetry Procedures Among Women After Breast Reconstruction: A Cross-Sectional Study
Saleh Abualhaj, Mosleh M. Abualhaj, Lina Alshadfan, Yasmin Safi, Mu’taz Massad, Osama Shattarah, Yousef Albustanji, Younis Hizzani, Zain aldeen Saleh, Dima Alhawajreh, Ayyub Masoud, Mohd Said Dawod

TL;DR
This study explores how aware and willing women in Jordan are to pursue breast symmetry procedures after cancer surgery, finding that many lack awareness and face financial and communication barriers.
Contribution
The study provides novel insights into awareness, attitudes, and barriers toward breast symmetry procedures among breast cancer survivors in Jordan.
Findings
Only 6.4% of participants had undergone contralateral breast symmetry procedures.
Main barriers included satisfaction with current appearance, fear of surgery, financial constraints, and lack of physician counseling.
High trust in medical team recommendations was reported despite limited awareness and discussion about symmetry procedures.
Abstract
Background: Achieving breast symmetry is an important aesthetic goal following reconstruction post-mastectomy; however, little is known about women’s awareness, attitudes, and barriers regarding Contralateral Breast Symmetry Procedures (CBSP) in Jordan. Objectives: To assess awareness, perceptions, and barriers toward contralateral breast symmetry procedures among breast cancer survivors who underwent reconstruction at King Hussein Cancer Center. Methods: A cross-sectional study was conducted from July to Oct 2025 at KHCC, among 314 women diagnosed with breast cancer who had post-breast reconstruction. Data were collected using a structured Arabic questionnaire, which was developed based on existing literature, validated by an expert panel, and piloted on 10 women for clarity and reliability. The final tool demonstrated acceptable internal-consistency (Cronbach’s α = 0.712). The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
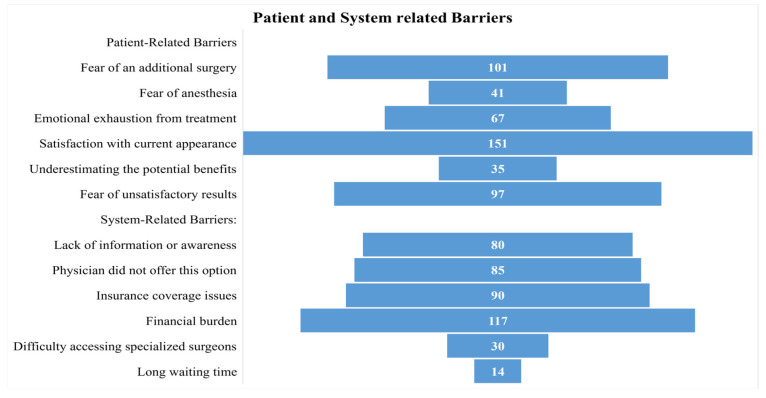 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Implant and Reconstruction · Organ and Tissue Transplantation Research · Body Image and Dysmorphia Studies
1. Introduction
Breast cancer is the most commonly diagnosed cancer among women worldwide, accounting for approximately 2.3 million new cases and 685,000 deaths in 2020, representing a major public health concern and leading cause of cancer-related morbidity and mortality in women [1]. Advances in early detection and treatment have significantly improved survival rates, resulting in a growing population of breast cancer survivors who face unique challenges related to long-term quality of life, including physical, psychological, and aesthetic outcomes [2,3,4]. In Jordan, breast cancer is the most prevalent cancer among women, representing nearly 36% of all female cancers, with an increasing incidence over the past decade [5]. This rising burden highlights the need for comprehensive survivorship care that addresses both oncologic outcomes and post-treatment quality of life, including breast reconstruction and contralateral breast symmetry procedures [6]. Breast reconstruction following mastectomy has been demonstrated to have positive effects on the psychosocial well-being, body image, and overall quality of life in breast cancer survivors [7,8,9,10]. Symmetry between the reconstructed and contralateral natural breast is a major goal following unilateral mastectomy, which in many cases is achieved through a contralateral breast symmetry procedure such as augmentation, mastopexy, or reduction [11,12].
CBSP can be performed at the same time as the initial reconstruction or can be staged. The decision is based on patient preferences, anatomy, and the oncologic treatment plan [13,14]. Achieving symmetry is usually more difficult after implant-based reconstruction than autologous techniques. This can be related to the inherent shape of implants as well as differences in tissue change over time [13,14].
Breast reconstruction awareness and availability have increased; however, disparities persist in access and utilization, particularly for symmetry procedures. These may be due to sociodemographic factors, insurance factors, providers’ communication practices and patients’ knowledge. Fear of additional surgery, financial cost, and lack of physician recommendation are also noted to be barriers to the uptake of symmetry procedures [15,16].
Despite legislative mandates (such as the Women’s Health and Cancer Rights Act) that support coverage for reconstruction, and greater awareness of its benefits, disparities in access and utilization persist worldwide. In addition, studies have revealed that in countries with established access to reconstruction, rates of utilization are less than optimal, especially among women of low socioeconomic status, women from ethnic minority groups, and those treated in rural or non-academic centers [15].
Evidence is growing that not only are aesthetic and psychosocial outcomes important to patients, but patient-reported outcome instruments such as the BREAST-Q highlight nuanced differences in satisfaction and physical well-being between those who receive contralateral breast symmetry procedures and those who do not. Emerging data also show that symmetry achieved with augmentation is most likely to result in high satisfaction, with other procedures, such as mastopexy or reduction, having lower physical well-being despite similar satisfaction with appearance, emphasizing the importance of appropriate surgical selection and counseling [14].
Crucially, Razdan et al. now suggest that surgeons should be discussing all options for reconstruction and symmetry as part of a shared decision-making process, recognizing the lasting impact of these decisions on long-term survivorship [14]. Nevertheless, persistent system-level barriers, such as hospital-level barriers, provider specialty, and reconstructive service availability, remain the largest contributors to inequities in access to care, with significant differences still found between non-urban centers and the publicly funded health system. Provider- and patient-level barriers, including cultural and information access, also impact patient decision-making [16]. In Middle Eastern cultures, including Jordan, decisions related to breast reconstruction and subsequent symmetry procedures are strongly influenced by sociocultural norms. Stigma surrounding aesthetic procedures may also limit open discussion and awareness about breast refinement options. These cultural dynamics may affect women’s willingness to pursue secondary symmetry procedures, their comfort in discussing aesthetic concerns, and their perceptions of body image after mastectomy and reconstruction [17,18]. Therefore, understanding these contextual factors is essential when evaluating patient attitudes and barriers within this population.
Therefore, efforts to improve access to symmetry procedures justly should include educating physicians and patients, changes to policy regarding coverage and referrals, and reforms to the healthcare system to reduce practical and financial obstacles [16].
This study aims to evaluate the awareness, attitudes, and barriers to contralateral breast symmetry procedures among women who have undergone breast reconstruction at a tertiary cancer center. Specifically, we assess the prevalence of knowledge about symmetry options, patient interest and satisfaction, and the sociodemographic and clinical factors—along with patient-reported barriers—that influence the consideration and uptake of these procedures. The findings are intended to inform strategies for improving patient counseling and the shared decision-making process, addressing unmet needs in breast cancer survivorship care.
2. Materials and Methods
2.1. Study Design and Setting
This study employed a cross-sectional survey design to assess patient awareness, attitudes, and perceived barriers toward contralateral breast symmetry procedures following mastectomy and reconstruction among breast cancer patients. The study was conducted at King Hussein Cancer Center (KHCC), a leading tertiary cancer center in Amman, Jordan. Data collection was carried out between 5 July 2025 and 1 October 2025.
2.2. Participants
The study population included women who had been diagnosed with breast cancer and subsequently undergone mastectomy and breast reconstruction surgery at King Hussein Cancer Center (KHCC). Eligible participants were those who:
- Had undergone mastectomy and subsequent reconstruction surgery between January 2024 and January 2025 at KHCC.
- Were 18 years or older at the time of participation.
- Were able to provide informed consent and participate in a phone-based interview in Arabic or English.
Patients were excluded if they:
- Had recurrent or metastatic breast cancer at the time of data collection.
- Had incomplete or missing contact information.
- Were unable to communicate due to cognitive or language barriers.
2.3. Sampling and Recruitment
Eligible patients were identified from the institutional breast reconstruction registry. A convenience sampling method was used. Trained research personnel contacted patients via telephone between July and October 2025 to invite them to participate in a structured follow-up survey. Verbal informed consent was obtained prior to data collection.
The sample size was calculated using the formula for estimating a single population proportion:
where:
- Z = 1.96 (for 95% confidence interval);
- p = 0.5 (assumed proportion of awareness to maximize sample size);
- d = 0.056 (margin of error 5.6%).
The minimum required sample size was ~300 participants, allowing for a 5% non-response rate.
2.4. Data Collection Instrument
Data were collected using a structured, phone-based questionnaire developed by the research team to assess awareness, attitudes, and barriers toward contralateral breast symmetry procedures. The questionnaire consisted of four domains: sociodemographic and clinical characteristics, awareness of breast symmetry options, attitudes and perceptions toward aesthetic outcomes and body image, and patient- and system-related barriers to symmetry procedures. The survey tool underwent content validation by a panel of five experts in surgical oncology, plastic surgery, and health psychology to ensure clarity, relevance, and cultural appropriateness. A pilot test was conducted on 10 participants who met the inclusion criteria to evaluate comprehensibility and timing. Necessary modifications were made based on their feedback before launching the full study. The questionnaire was administered in Arabic, following standard forward–backward translation procedures to ensure linguistic and conceptual equivalence. Additionally, the internal consistency of the questionnaire was assessed using Cronbach’s alpha, which demonstrated acceptable reliability across the relevant domains (α = 0.712).
2.5. Ethical Considerations
Ethical approval was obtained from the Institutional Review Board (IRB) of King Hussein Cancer Center (Approval No: 25 KHCC 161). All participants provided verbal informed consent prior to participation. Confidentiality was maintained throughout the study, and all responses were anonymized and stored in password-protected electronic databases accessible only to the research team.
2.6. Data Management and Analysis
Data were entered and analyzed using R version 4.5.1. Descriptive statistics were used to summarize participant characteristics and survey responses. Categorical variables were presented as frequencies and percentages. No subgroup comparisons were performed due to the small number of participants who underwent contralateral breast symmetry procedures, and the analysis is therefore primarily descriptive.
3. Results
3.1. Sociodemographic and Clinical Characteristics
Out of 364 eligible patients contacted, 314 responded and completed the survey, resulting in a response rate of 86.3%. The mean age was 45.8 years (SD = 8.8), ranging from 22 to 76 years. The majority were married (83.8%), with smaller proportions being single (8.9%), widowed (3.8%), or divorced (3.5%). Regarding educational level, most participants had a university degree or higher (65.6%), while 29.9% had completed secondary education and only 4.5% had primary education or less. Approximately one-third of the participants (32.5%) were employed at the time of the survey. The vast majority resided in urban areas (92.4%), with only 7.6% living in rural areas. The mean BMI was 28.5 kg/m^2^ (SD = 5.8), with values ranging from 17.7 to 36.6. Most participants were non-smokers (70.7%); 17.8% were current smokers and 11.5% were ex-smokers. About one-quarter of the participants (26.8%) reported having chronic diseases. In terms of menopausal status, just over half were postmenopausal (52.2%), while 47.8% were premenopausal (Table 1).
3.2. Clinical and Treatment Characteristics
In terms of cancer stage, more than one-third of participants were diagnosed at stage I (37.9%), followed by stage II (36.0%) and stage III (26.1%). Regarding type of mastectomy, the largest proportion underwent skin-sparing mastectomy (SSM) (44.9%), followed by total mastectomy (36.6%), nipple-sparing mastectomy (NSM) (12.7%), and areola-sparing mastectomy (5.7%). The vast majority of participants (94.6%) had reconstruction with silicone implants, while only 4.5% had autologous tissue reconstruction and 1.0% had a combination of both techniques. The mean time since reconstruction was 23.1 months (SD = 21.9), ranging from 1 to 168 months. With respect to adjuvant therapy, more than half of participants received radiotherapy (53.8%), 77.4% received chemotherapy, and 80.9% received hormonal therapy (Table 2).
3.3. Contralateral Breast Symmetry Procedures and Future Considerations
Only a small proportion of participants had undergone a symmetry (balancing) procedure (6.4%, n = 20). Among these, breast augmentation was the most common type (40.0%), followed by mastopexy (35.0%) and breast reduction (25.0%). Regarding timing, over half of the symmetry procedures were performed in a delayed setting (55.0%), while 45.0% were performed immediately at the time of reconstruction. The majority of patients who underwent symmetry reported satisfaction with the results (75.0%), while one-quarter (25.0%) were dissatisfied. Among those who had not yet undergone a symmetry procedure, about one-quarter (26.2%) indicated that they were considering it in the future, while half (50.3%) did not intend to pursue it and 23.5% were unsure (Table 3).
3.4. Awareness and Knowledge of Symmetry Options
Overall, only 37.9% of participants reported being aware of the possibility of a symmetry procedure after breast reconstruction. Approximately 40.4% knew that symmetry could involve reduction, augmentation, or lifting. Less than one-third (28.0%) stated that the option of a symmetry procedure had been discussed with them as part of their reconstruction plan. Only 17.5% were aware that health insurance might cover the cost of a symmetry procedure. Similarly, less than one-third (31.2%) knew that symmetry can be performed either simultaneously with reconstruction or at a later stage. Knowledge about potential complications of symmetry procedure was limited, with only 20.4% reporting awareness. In contrast, more than half of participants (57.0%) recognized that achieving symmetry may improve psychological well-being (Table 4).
3.5. Attitudes and Perceptions Toward Contralateral Breast Symmetry Procedure
More than half of the participants (53.2%) agreed that they feel comfortable discussing aesthetic concerns with their doctor, while only 12.5% disagreed or strongly disagreed.
The majority considered achieving symmetry important for their body image: 62.4% agreed and 20.1% strongly agreed, with only a small proportion disagreeing (7.0%) or strongly disagreeing (0.3%). Opinions were mixed regarding whether symmetry is necessary after cancer recovery: 31.5% agreed that it is not necessary, while 37.6% disagreed and 14.6% were neutral. Regarding surgical fears, 37.9% agreed they fear the risks of surgery more than the potential benefit, while a similar proportion (38.5%) disagreed. One-third (31.5%) agreed they are considering symmetry to improve their quality of life, while 33.1% disagreed, showing diverse views. Notably, most participants (71.7% agree, 17.5% strongly agree) expressed trust in their medical team’s recommendations. In terms of social impact, 36.3% agreed that body symmetry affects their self-confidence, but 34.7% disagreed. Over half (54.1%) were satisfied with their current breast appearance, but 40.8% still felt uncomfortable with their body after reconstruction. Around 28.0% felt that asymmetry affects their self-image, while 40.4% disagreed. Avoidance of social events due to appearance was relatively low (6.1% agree, 1.6% strongly agree), with over half disagreeing. Finally, about one-quarter (23.9% agree, 5.7% strongly agree) felt that asymmetry causes stress when choosing clothing, while 39.2% disagreed and 22.0% strongly disagreed (Table 5).
3.6. Barriers to Symmetry Procedures
Nearly half of the participants (48.1%) indicated that satisfaction with their current breast appearance was a barrier to considering further symmetry procedures. Fear of undergoing an additional surgery was also common (32.2%), followed by fear of unsatisfactory results (30.9%) and emotional exhaustion from previous treatments (21.3%). Fewer participants reported fear of anesthesia (13.1%) or underestimating the potential benefits of symmetry (11.2%) as barriers. The most commonly reported system-related barrier was the financial burden, cited by over one-third of participants (37.3%). Insurance coverage issues were also noted by 28.7% of respondents, while 27.1% indicated that their physician had not offered a symmetry procedure as an option. One-quarter (25.5%) reported a lack of information or awareness as a barrier to pursuing symmetry. Fewer participants mentioned difficulty accessing specialized surgeons (9.6%) or long waiting times (4.5%) as limiting factors (Figure 1).
4. Discussion
In our study, only 6.4% of women who underwent breast reconstruction had previously undergone a contralateral symmetry procedure, and 75% of those women were satisfied with this additional surgery. This finding is very low when compared with the studies from Western countries, which report that the rates of contralateral symmetry procedures after unilateral reconstruction varied from 22% to 67% based on the reconstruction modality and timing. For instance, Losken et al. reported that 67% of the delayed reconstruction patients and 22% of the immediate cases underwent a contralateral symmetry procedure, with higher rates in implant-based reconstructions [19]. One possible cause for the notably lower rate in our setting may be the low level of patient awareness of these symmetry options and, in turn, the suboptimal discussion with their physicians. The awareness of the available procedures among our population was as low as 37.9% and less than a third had discussed them with their doctor. Feeling satisfied with the appearance of their breasts was reported as the main reason not to pursue additional surgery by almost half of the patients, which suggests that patients’ satisfaction with the achieved result hinders the interest in pursuing further surgical intervention. Additionally, many women also expressed fear of more surgery and concerns about unsatisfactory outcomes. System-level barriers such as financial cost and insurance limitations also contributed. Both of these patient and system factors likely contribute to the lower uptake observed in our study and highlight the need for improved education, communication, and financial support to enhance access to contralateral symmetry procedures.
Only 37.9% of our respondents were aware of symmetry options, 28% of whom reported that this option had been discussed. This is much lower than Western studies have reported, where both awareness and discussion have been reported to be above 50% [19]. For example, Retrouvey et al. performed a systematic review and identified lack of patient awareness and poor communication by providers as the two biggest barriers to patients receiving breast reconstruction [20]. Our findings highlight a significant gap in patient education and provider communication, which may contribute to the low uptake of symmetry procedures.
The majority of our participants (62.4%) considered symmetry important for body image, and 75% of those who underwent symmetry procedures were satisfied. This is consistent with previous studies, which report high satisfaction rates (77–82%) among patients who undergo symmetry procedures, particularly when augmentation is performed [14]. On the other hand, in our study, satisfaction with current appearance was a significant obstacle in the pursuit of symmetry, and this was expressed by 48.1% of our participants. This contrasts with studies in Western populations, where dissatisfaction with appearance is more commonly cited as a motivator for symmetry procedures [21]. However, our study uniquely identifies satisfaction with current appearance as a primary barrier, possibly indicating substantial cultural influences specific to Middle Eastern societies, where expectations surrounding feminine identity, modesty, and reconstruction outcomes differ from Western norms [17]. In our context, many women may perceive reconstruction itself as sufficient restoration after cancer treatment, and the pursuit of additional aesthetic perfection may be viewed as less necessary or less culturally emphasized [18]. These cultural dynamics likely shape patient expectations and may partly explain why women in our study felt less compelled to pursue symmetry procedures despite objective asymmetry.
In this study, the barriers included fear of surgery (32.2%) and financial burden (37.3%). These findings are consistent with previous literature, which identifies financial concerns, fear of surgery, and lack of information as key barriers to breast reconstruction and symmetry procedures [22,23,24].
The population in our study was well-educated with urban residency; however, this sociodemographic status was not a factor that led to high rates of undertaking symmetry procedures, suggesting that there is a need to improve awareness and information exchange even among individuals who have a high baseline education and health care access. The predominance of implant-based reconstruction among participants, which is associated with greater difficulty in achieving natural symmetry compared to autologous methods, may have contributed to demand for additional corrective surgery, though this was not reflected in actual procedure rates. The majority of symmetry procedures were in fact done in a delayed setting (55%). This finding reemphasizes the fact that there is still patient reluctance; thus, more intense post-operative education and support is indicated. Patient satisfaction with breast appearance was relatively high, yet a considerable proportion reported discomfort and concerns with body image after reconstruction, highlighting complex and varied psychosocial outcomes among breast cancer survivors. In summary, all of these results highlight the complex impact of clinical factors, timing of surgery, the influence of sociodemographic and psychosocial variables on the decision-making process and outcomes following breast reconstruction.
This study has several limitations. The cross-sectional design and recruitment from a single tertiary cancer center may limit the generalizability of the findings to broader populations or other healthcare settings. Additionally, reliance on patient recall may have introduced recall bias. Although the survey was conducted by trained research personnel using a standardized and validated questionnaire, interviewer bias remains a potential limitation due to the subjective nature of telephone-based responses. Furthermore, the study did not use standardized patient-reported outcome instruments such as the BREAST-Q, which could have provided a more objective and validated assessment of satisfaction with reconstructive and symmetry procedures. Incorporating such tools in future research would strengthen the measurement of patient satisfaction and decision-making processes. Despite these limitations, the study’s strengths include clearly defined inclusion criteria, comprehensive characterization of sociodemographic and clinical variables, and the use of a structured, standardized telephone interview that ensured consistency and reliability in assessing patients’ awareness, attitudes, and perceived barriers toward breast symmetry procedures.
Beyond the above limitations and strengths, it is important to recommend strategies for improving care based on these results. Future research should focus on developing targeted patient education initiatives and enhancing provider communication about symmetry options, as greater awareness is likely to increase uptake and satisfaction with breast reconstruction outcomes. An effective strategy to overcome financial barriers would be the expansion of insurance coverage for symmetry procedures. In addition, future research is necessary to evaluate long-term psychosocial outcomes and procedural trends to address the limitations of cross-sectional studies and provide additional practice-based information. The recommendations above can help to guide breast cancer survivors to optimize breast cancer survivorship and breast symmetry decision-making.
5. Conclusions
In this study, the rate of contralateral breast symmetry procedures after reconstruction was much lower than in Western countries, even though symmetry after mastectomy has been shown to be important for quality of life and body image. Patient knowledge, provider communication and education, satisfaction with preexisting appearance, fear of surgery, and cost were found to be the largest contributing factors to the limited access to symmetry procedures. Socio-demographic factors such as high levels of education and urban residence did not translate into improved utilization, underscoring the persistent influence of system-level and informational gaps. Although most women valued symmetry and were very satisfied when they had the procedure, many remained unaware of available options or were deterred by the financial burden or not having discussed with their medical team.
To improve awareness and informed decision-making, targeted strategies are recommended, including structured patient education sessions, culturally sensitive informational materials, incorporation of decision aids in clinical consultations, and proactive discussion by healthcare providers about reconstructive options. Broader financial support and system-level interventions may further facilitate equitable access. Future efforts should also include longitudinal research on psychosocial outcomes and procedural trends to optimize clinical practice and patient-centered care in breast reconstruction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Laversanne M. Sung H. Ferlay J. Siegel R.L. Soerjomataram I. Jemal A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA. Cancer J. Clin.20247422926310.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Namoos A. Thomson N. Olson C. Sheppard V. Aboutanos M. Physical and Psychological Burdens Among Breast Cancer Survivors: Evaluating Post-Treatment Gait Impairment, Falls, and Depression Using Real-World Data Eur. J. Cancer Care 20252025555856310.1155/ecc/5558563 PMC 1258807741200408 · doi ↗ · pubmed ↗
- 3Bergerot C. Bergerot P.G. Maués J. Segarra-Vazquez B. Mano M.S. Tarantino P. Is Cancer Back?—Psychological Issues Faced by Survivors of Breast Cancer Ann. Palliat. Med.2024131221234122923410.21037/apm-24-5439168641 · doi ↗ · pubmed ↗
- 4Schmitz K.H. Speck R.M. Risks and Benefits of Physical Activity among Breast Cancer Survivors Who Have Completed Treatment Women’s Health 2010622123810.2217/WHE.10.120187728 · doi ↗ · pubmed ↗
- 5Ministry of Health Ministry of Health Non-Communicable Diseases Directorate Jordan Cancer Registry Incidence in Jordan Ministry of Health Amman, Jordan 2019
- 6Khajoei R. Azadeh P. Zohari Anboohi S. Ilkhani M. Nabavi F.H. Breast Cancer Survivorship Needs: A Qualitative Study BMC Cancer 2024249610.1186/s 12885-024-11834-538233789 PMC 10795302 · doi ↗ · pubmed ↗
- 7Kocher R. Emanuel E.J. De Parle N.-A.M. The Affordable Care Act and the Future of Clinical Medicine: The Opportunities and Challenges Ann. Intern. Med.201015353653910.7326/0003-4819-153-8-201010190-0027420733178 · doi ↗ · pubmed ↗
- 8Lang J.E. Summers D.E. Cui H. Carey J.N. Viscusi R.K. Hurst C.A. Waer A.L. Ley M.L.B. Sener S.F. Vijayasekaran A. Trends in Post-Mastectomy Reconstruction: A SEER Database Analysis J. Surg. Oncol.201310816316810.1002/jso.2336523861196 PMC 4035023 · doi ↗ · pubmed ↗