A New Hypothesis on the Etiology of Down Syndrome: The Role of Anti-Zona Pellucida Antibodies as an Age-Independent Factor
Giuseppe Noia, Tina Pasciuto, Francesco Ria, Alfredo Pontecorvi, Monica Sacco, Emanuela Teveroni, Maurizio Genuardi, Francesca Mauro, Paolo Spina, Emilia Spina, Giada Castagna, Daniela Visconti, Antonio Lanzone, Marco De Santis

TL;DR
This study suggests that anti-zona pellucida antibodies may be a new, age-independent risk factor for Down Syndrome, independent of maternal age.
Contribution
The study introduces anti-zona pellucida antibodies as a novel potential predictor of Down Syndrome.
Findings
Anti-zona pellucida antibodies were significantly higher in women with Down Syndrome pregnancies.
Anti-zona pellucida antibodies showed strong predictive performance with an AUC of 0.94.
Neither anti-zona pellucida nor anti-thyroid antibodies increased with maternal age.
Abstract
Down Syndrome (DS) is the most common chromosomal abnormality characterized by neurodevelopmental impairment. Apart from maternal age, its risk factors remain poorly understood. This prospective case-control study aimed to evaluate the role of maternal anti-zona pellucida (ZP) antibodies (Ab) and anti-thyroid-Ab in predicting DS. Correlations of anti-ZP-Ab and anti-thyroid-Ab with maternal age were also assessed. Anti-ZP-Ab were measured after childbirth using ELISA. Anti-thyroid peroxidase (aTPO) and anti-thyroglobulin (aTgII) antibodies were also analysed with the Allelica IM platform. Statistical analyses included receiver operating characteristic curve assessment, expressed as area under the curve (AUC) and linear regression modeling. Between September 2020 and October 2022, 58 women were enrolled. Anti-ZP-Ab levels were significantly higher in women with DS pregnancy with an odds…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
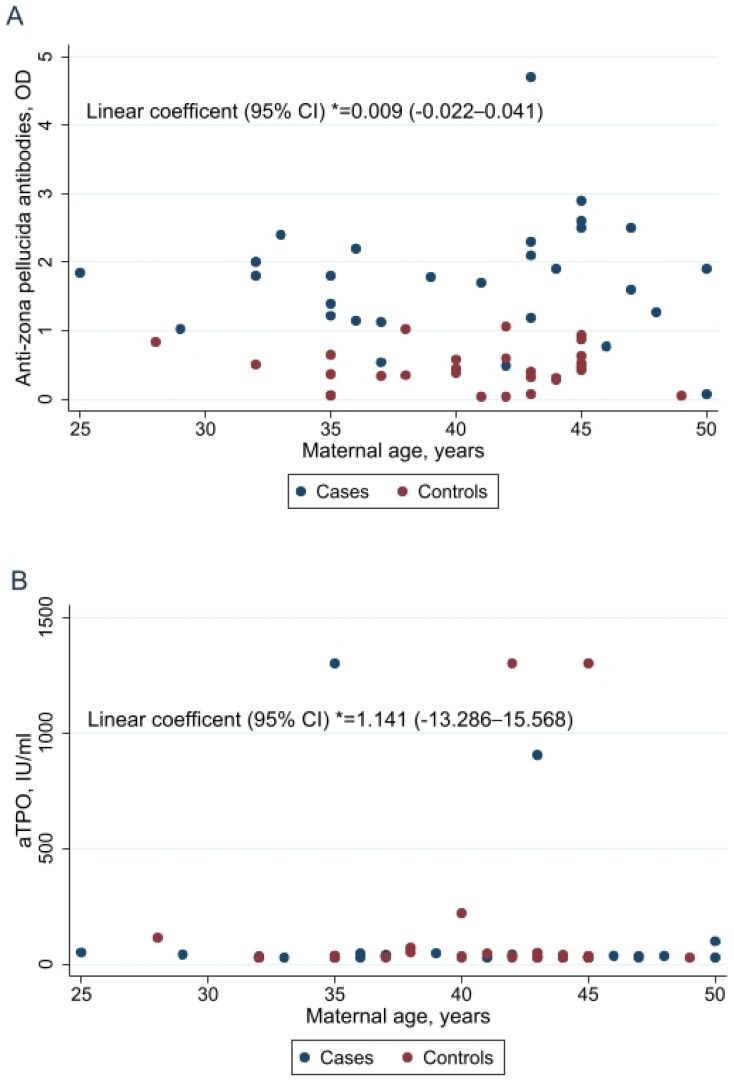 Figure 1
Figure 1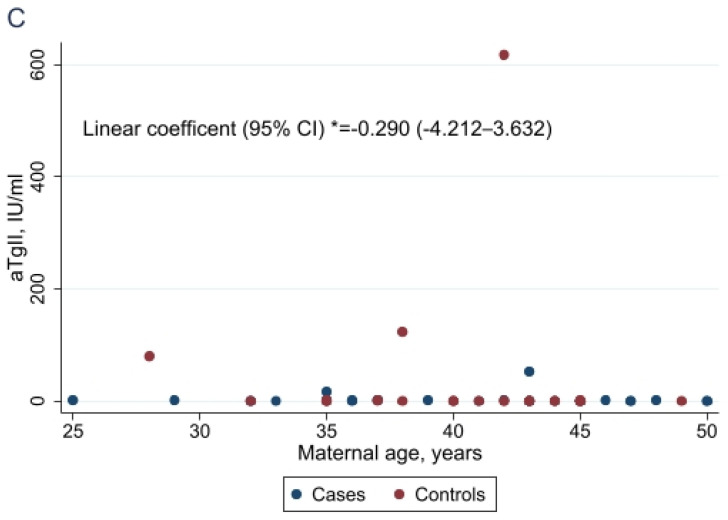 Figure 2
Figure 2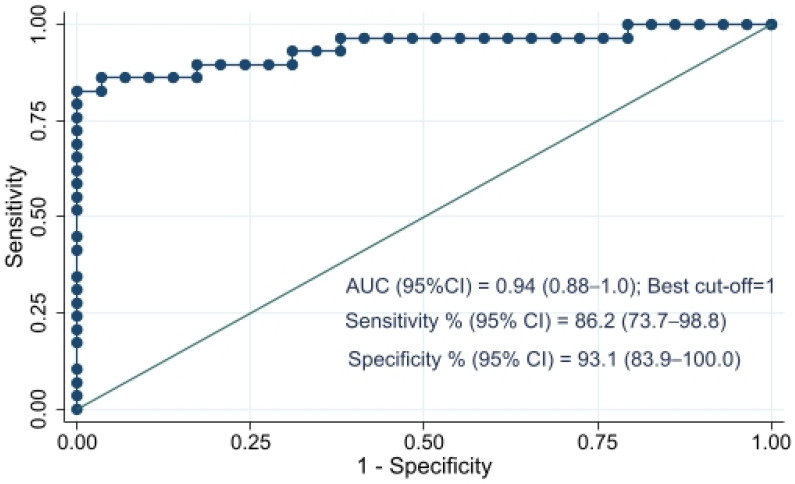 Figure 3
Figure 3- —Foundation Il Cuore in una Goccia ONLUS-Fondazione Policlinico Universitario A. Gemelli-IRCCS
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrenatal Screening and Diagnostics · Down syndrome and intellectual disability research · Gestational Diabetes Research and Management
1. Introduction
Down Syndrome (DS) is the most common chromosomal abnormality, characterized by a neurodevelopmental disorder with a prevalence of about 1/700–1/1000 live births [1,2,3]. Its frequency varies according to maternal age distribution, access to prenatal screenings, and pregnancy termination practices. DS most commonly results from free trisomy 21 (T21), which arises from meiotic nondisjunction during oogenesis. Maternal age is the strongest known risk factor for T21 and other aneuploidies related to chromosome nondisjunction during maternal meiosis, particularly the first meiotic division. In fact, the risk of a T21 birth rises from about 3% for younger women in their 20s to 30% in older women in their 40s [4,5,6]. Despite the well-established epidemiological association, the biological mechanisms linking maternal aging to meiotic errors remain incompletely understood [7,8,9]. Proposed contributors include age-related deterioration of cohesin complexes, altered recombination patterns, and impaired spindle assembly checkpoint function [5,6].
Beyond maternal age, several genetic, epigenetic, and environmental factors have been implicated in modulating DS risk. Variants in gene involved in folate metabolism—particularly MTHFR c.677C>T and c.66A>G—have been associated with altered methylation pathways and increased susceptibility to meiotic nondisjunction [10]. Additionally, influences include maternal obesity, smoking, and metabolic alterations that affect serum biomarkers and oocyte quality. However, these factors explain only a fraction of DS cases, suggesting that additional mechanisms may contribute to the etiology of T21 pregnancies [10,11,12].
A growing body of evidence indicates that autoimmune processes targeting ovarian structures may impair folliculogenesis and oocyte competence. Experimental studies have shown that immunization with zona pellucida (ZP) proteins induces ovarian inflammation, follicular depletion, and infertility in animal models [13,14]. Anti-ZP antibodies have been detected in women with premature ovarian failure and diminished ovarian reserve, supporting a role for autoimmune ovarian dysfunction in human reproductive disorders [15]. These findings suggest that immune-mediated damage to the oocyte or its surrounding structures may compromise meiotic integrity.
Interestingly, epidemiological observations have reported that mothers of children with DS tend to experience menopause at a younger age compared with mothers without DS offspring [16]. Moreover, women who delivered a child with DS at a young age often exhibit reduced ovarian reserve, including lower anti-Müllerian hormone (AMH) levels [17,18]. These data raise the possibility that intrinsic or immune-mediated ovarian dysfunction may predispose to meiotic errors independently of chronological age.
Given the established role of immune factors in ovarian aging and oocyte quality [19,20,21,22], and the evidence linking anti-ZP antibodies to impaired follicular function, we hypothesized that anti-ZP autoimmunity may contribute to the etiology of T21 pregnancies. The present study was therefore designed to investigate the association between anti-zona pellucida antibodies and the occurrence of trisomy 21, exploring whether autoimmune ovarian factors may represent an age-independent risk mechanism for DS.
2. Results
Between September 2020 and October 2022, 58 women (29 cases and 29 controls) were prospectively enrolled. Gestational and clinical characteristics of the 29 dyads—mother and DS child—are reported in Table 1. The mean maternal age for DS pregnancies was 37.1 years (SD: 5.2) with a median gestational age of 38.6 weeks (SD: 3.1). Delivery was spontaneous in 10/19 cases (52.6%). At birth, the mean weight was 2719.3 g.
Clinical and serological characteristics of cases and controls are described in Table 2. No statistically significant differences in terms of age at menarche and at serological evaluation, autoimmune disease, other concomitant pathologies and drug assumptions, including current or past hormonal therapies, were observed. The median number of parities was 3 (min–max: 1–8) and 2 (min–max: 1–3) for cases and controls (p = 0.002), respectively.
Overall, the median age at serological evaluation was 40.4 years (SD: +5.7) and no statistically significant differences were found in the distribution of the after child anti-thyroid peroxidase (aTPO) and anti-thyroglobulin (aTgII) antibodies (p = 0.81 and p = 0.24 respectively), while the anti-ZP antibodies were significantly higher in the case group (p < 0.001).
The value of anti-ZP as well anti-thyroid antibodies did not increase with age. These results were investigated both analysing separately cases and controls and analysing the overall correlation of maternal age and anti-ZP or anti-thyroid antibodies adjusting for DS pregnancy (Figure 1).
ROC analysis, shown in Figure 2, shows that the performance of anti-ZP antibodies in DS pregnancy prediction has an AUC of 0.94 (95% CI: 0.88–1.00). The sensitivity and specificity associated with the best cutoff of 1 OD retrieved through Liu’s method are 86.2% (95% CI: 73.7–98.8) and 93.1% (95% CI: 83.9–100.0), respectively, with an accuracy of 89.7% (78.2–100.0). The associated OR adjusted for maternal age was 71.52 (95% CI: 7.05–725.18).
Since the cut-off value of 2.1 OD is commonly used in the literature, we also calculated the frequency of DS pregnancies using this threshold. We found that 34.5% of women with a DS pregnancy had anti-ZP antibody values higher than 2.1 OD, whereas none of the controls exceeded this value. (Table 2).
3. Discussion
In this prospective case-control study, we found that anti-ZP antibodies are significantly associated with an increased risk of DS pregnancy. To our knowledge, this is the first prospective study investigating the role of anti-ZP antibodies in predicting the risk of DS pregnancy.
In our series many DS pregnancies occurred in women aged > 35 years, as expected [23]. Adjusting our results for maternal age, anti-ZP antibodies emerged as an additional independent risk factor for trisomy 21. Moreover, we found that values higher than 1 OD can predict DS pregnancy with an excellent AUC. This cut-off was chosen to maximize sensitivity and specificity and is tailored for DS pregnancy prediction.
3.1. Anti-ZP Antibodies as an Age-Independent Risk Factor
Maternal age is the most established determinant of meiotic nondisjunction, with error rates increasing markedly as women age [24,25]. However, several studies have shown that maternal age alone does not fully explain the occurrence of trisomy 21. Sherman et al. (1994) demonstrated that reduced recombination on chromosome 21q is linked to nondisjunction events, particularly during the meiosis I, and that these recombination patterns are not solely age-dependent [26]. Indeed, most trisomy 21 cases originate from maternal meiotic errors (92% maternal vs. 4.9% of paternal origin), with the majority occurring during meiosis I [27].
Recombination plays a critical role in ensuring proper chromosome orientation on the meiotic spindle. Reduced or absent recombination increases the risk of meiotic nondisjunction (ND). Importantly, the overall reduction in recombination frequency appears to be independent of maternal age, while the location of chiasmata influences whether errors occur in meiosis I or II [28,29,30]. Distal single exchanges are more common in younger women with meiosis I errors, whereas proximal chiasmata are more typical in older women with meiosis II errors. These findings support the existence of both age-dependent and age-independent pathways leading to ND.
Our results align with this concept, suggesting that anti-ZP antibodies may represent an additional, age-independent mechanism contributing to meiotic errors.
3.2. Autoimmunity as a Contributor to Meiotic Dysfunction
Given the multifactorial nature of nondisjunction, autoimmune mechanisms have been proposed as potential contributors to DS risk. Charkiewicz et al. (2016) identified significant differences in the expression of over 200 autoantibodies in women with DS pregnancies, including antibodies targeting proteins involved in oocyte maturation and chromosomal segregation [31]. Similarly, Mikwar et al. (2020) highlighted several pathways implicated in age-related aneuploidy—recombination failure, cohesin impairment, spindle assembly checkpoint dysfunction, epigenetic dysregulation, and mitochondrial defects—some of which may be influenced by autoantibodies [32]. Our findings reinforce the hypothesis that autoimmune dysregulation may impair oocyte quality and increase the risk of meiotic errors, independently of maternal age.
3.3. Biological Plausibility: Anti-ZP Antibodies and Ovarian Dysfunction
Anti-ZP antibodies have long been associated with infertility [33,34,35,36,37] and premature ovarian failure (POF). The broader concept that endocrine autoimmunity may contribute to ovarian dysfunction is supported by evidence of prematurely diminished ovarian reserve and by the observed association between androgen production and immune system activation. This relationship has been proposed as indirect evidence for a functional adrenal–ovarian autoimmune axis in women [38].
Experimental studies in mice demonstrated that exposure to anti-ZP antibodies impairs folliculogenesis, reducing follicle diameter, antral formation, mucification, oocyte maturation, and fertilization rates. Morphological changes included thinner zona pellucida and fewer granulosa cell microvilli penetrating the ZP, disrupting oocyte–granulosa communication [39,40,41]. These findings suggest that anti-ZP antibodies can damage follicle development and potentially contribute to meiotic nondisjunction.
Additional evidence comes from studies of thyroid autoimmunity. In women with diminished ovarian reserve, thyroid autoantibodies have been associated with poorer embryonic quality, suggesting that autoimmune activation—even when not directed specifically against ovarian structures—can negatively affect female fertility [42,43,44,45,46,47,48].
Cross-reactivity of anti-ZP antibodies with thyroid microsomal components has also been reported. Kelkar et al. (2005) [15] found that patients with POF often had anti-ovary antibodies, many of which cross-reacted with ZP and thyroid tissue. In humans, a significant proportion of women with anti-ZP antibodies also had anti-thyroid antibodies, suggesting a link between ovarian and thyroid autoimmunity [15]. This is particularly relevant given that DS itself is strongly associated with autoimmune thyroid disease. Reduced expression of the autoimmune regulator (AIRE) gene in DS thymus tissue has been linked to increased susceptibility to thyroid autoimmunity [49].
Taken together, these data support a broader framework in which autoimmune processes may influence ovarian function, oocyte competence, and ultimately the risk of trisomy 21. Anti-ZP antibodies are generally understood to arise as part of an autoimmune response directed against zona pellucida glycoproteins. Such antibodies may develop following exposure to ovarian antigens due to follicular disruption, ovarian inflammation, or other immune-modulating conditions. However, the precise trigger for their production in individual patients cannot be determined from our dataset.
Finally, our study was not designed to identify the initial immunological source of anti-ZP antibody production. Future mechanistic research will be required to clarify the pathways leading to their development and to define their role in ovarian dysfunction.
3.4. Strengths and Limitations
The strengths of this study include its prospective design, rigorous laboratory methodology, and the strong predictive performance of anti-ZP antibody levels. However, several limitations must be acknowledged. First, anti-ZP antibodies were measured postpartum, preventing us from determining whether they were present before conception or developed during or after pregnancy. Future studies incorporating pre-pregnancy sampling will be essential to establish causality. Second, because cases and controls were matched by age to ensure comparability, we could not directly evaluate the interaction between maternal age and anti-ZP antibodies.
Nevertheless, our analyses adjusted for maternal age, and the association between anti-ZP antibodies and DS remained significant.
3.5. Implications and Future Directions
For many years, maternal age has been considered the primary determinant of trisomy 21. Our findings suggest that additional factors—particularly autoimmune dysregulation involving the development of anti-ZP antibodies—may contribute to the etiology of DS, potentially playing a more prominent role in younger women. If confirmed, this hypothesis could have important implications for preconception counseling and risk assessment.
Further research is needed to clarify the temporal relationship between anti-ZP antibodies and pregnancy, to explore the mechanistic pathways linking autoimmunity to meiotic errors, and to determine whether anti-ZP antibodies could serve as a biomarker for DS risk in clinical practice.
4. Materials and Methods
4.1. Study Design and Ethical Approval
This prospective case-control study was performed at Fondazione Policlinico Universitario A. Gemelli–IRCCS. The study protocol was approved by the local Ethical Committee (Prot. N. 6826/20 ID 3012), and written informed consent was obtained from all participants prior to enrolment.
4.2. Eligibility Criteria
The study aimed to evaluate the prevalence of anti-ZP antibodies in women who had delivered a child with Down syndrome (cases) compared with women with no history of Down syndrome pregnancies (controls). Participants were considered eligible if they were aged > 20 years old, not pregnant at the time of enrolment, and had no major metabolic or vascular diseases including diabetes, hypertension, or antiphospholipid antibodies syndrome. Additional exclusion criteria for controls were any previous pregnancy affected by genetic abnormalities and/or congenital malformations. Cases and controls were matched by age.
Secondary endpoints were: (a) the association of anti-thyroid antibodies levels and DS pregnancy; (b) the correlation of anti-ZP and anti-thyroid antibodies and age.
4.3. Data Collection
Study data were prospectively collected and managed in compliance with the General Data Protection Regulation (GDPR) using REDCap electronic data capture tools hosted at Fondazione Policlinico Universitario A. Gemelli-IRCCS (https://redcap-irccs.policlinicogemelli.it/ (accessed on 20 November 2022)) [50].
Authenticated and restricted access to the platform was allowed only for people officially registered as study investigators or authorized data managers.
4.4. Sample Collection and Processing
For each participant, a venous blood sample was obtained for measurements of anti-ZP antibodies, thyroid hormones, and anti-thyroid antibodies.
Blood samples were allowed to clot for 24 h at +4–+8 °C. Serum was obtained by centrifugation at 1500× g for 10 min, aliquoted into 0.5 mL fractions, and stored at −20 °C until analysis. Samples were thawed once at room temperature and used within 2 h. Repeated freeze-thaw cycles were avoided due to loss in antibody activity.
4.5. Laboratory Analyses
4.5.1. Measurement of Human Anti-Zona Pellucida Antibodies
Human anti-ZP IgG antibodies (azp-Ab) were measured using a commercial ELISA kit (Wuhan Huamei Biotech Co., Ltd.—operating as CUSABIO—Wuhan, Hubei Province, China), following the manufacturer’s instructions. The kit used was catalog number CSB-E09082h (lot numbers C0604050604 and C0633130638). Detection was performed using an anti-human IgG secondary antibody, conjugated with Horseradish Peroxidase (HRP), reacting with the chromogenic substrate tetramethylbenzidine (TMB). Optical density (OD) was measured with a microplate reader set to 450 nm. Tests were performed in double. The Intra-assay and inter-assay precision showed a coefficient of variation (CV) <15%. According to the manufacturer’s instructions, results were expressed as OD sample/OD negative control (provided with the kit). In our study, the mean ratio ± standard deviation obtained from control and cases samples were respectively 0.44 ± 0.28 and 2.01 ± 0.67. According to the manufacturer’s cut-off, a sample was considered positive for azp-Ab when the ratio OD sample/OD negative was ≥2.1.
4.5.2. Measurement of Anti-Thyroid Antibodies
Anti-thyroid peroxidase (aTPO) and anti-thyroglobulin (aTgII) antibodies were centrally measured using the Atellica IM analyser (Siemens Healthineers, Erlangen, Germany) at the high automation CoreLab of Fondazione Policlinico Universitario A. Gemelli-IRCCS.
aTgII Assay
The aTgII method is a competitive bridge immunoassay based on chemiluminescence detection. This method uses two different types of human thyroglobulin. Briefly, the reagent containing human thyroglobulin labelled with acridinium ester was incubated with the serum sample test and, subsequently, with the solid phase containing a biotinylated human thyroglobulin bound to paramagnetic beads which, in turn, are coupled to streptavidin. The aTgII antibodies present in the serum sample bind both the acridinium esterified-thyroglobulin in the reagent and the biotinylated-thyroglobulin in the solid phase, forming a bridge that allows chemiluminescent detection. The aTgII antibodies title was expressed in IU/mL and based on a specific standard calibration curve. The aTgII cut-off value ≥ 4.5 IU/mL indicates thyroid autoimmune disorders. The sensitivity is 98.5% (95% Confidence Interval (CI): 91.7–100%); while the specificity is 94.8% (95% CI: 90.3–97.6%). The measurement range in which the method is linear, is 1.3–1000 IU/mL with LoD < 1.3 IU/mL.
aTPO Assay
Similarly, the aTPO Atellica IM method is a competitive immunoassay based on chemiluminescence detection. This method uses a mouse monoclonal aTPO antibody bound to paramagnetic beads in the solid phase which competes with the possible aTPO antibody in the serum sample test for binding with a limited quantity of human TPO complexed with a mouse monoclonal aTPO acridinium ester-labelled antibody.
The aTPO antibodies title was expressed in U/mL and based on a specific standard calibration curve. The measurement range in which the method is linear is 28–1000 IU/mL in serum and plasma samples with LoD < 28 U/mL.
4.6. Statistical Analyses
Assuming a case control design with a 1: 1 ratio, type 1 error α = 0.05, type 2 error β = 0.20 (study power 80%) and assuming that in the general population the prevalence of anti-ZP antibodies is about 20% [36,41], an enrolment of 58 total patients (29 cases and 29 controls) was estimated in order to observe a prevalence of 55% of anti-ZP antibodies in women with DS children. The sample was calculated using a two-tailed test using the STATA software version 13.
Study characteristics were presented in terms of absolute frequency (percentage relative frequency) for qualitative variables and in terms of mean (standard deviation) and median (min–max) in the case of normal and not normal distribution of quantitative variables respectively. Shapiro-Wilks’ test was used to assess the normality of continuous variables distribution. Cases and controls comparisons were made through two-sided Pearson’s χ^2^ or Fisher’s exact test and Student’s t test or Mann-Whitney’s test as appropriate.
The correlation of maternal age with anti-ZP antibodies, as well with anti-thyroid antibodies (aTPO and aTgII) was assessed separately in cases and controls, and overall, through linear regression analysis adjusting for DS pregnancy.
Receiver–operating characteristic (ROC) analysis was applied to evaluate the ability of anti-ZP antibodies to predict DS pregnancy in terms of area under the curve (AUC), as well as to determine the best cut-off value for this prediction. Best cut-off was detected according to Liu’s method which defines the best cut-point as the point maximizing the product of sensitivity and specificity index [51]. Sensitivity, specificity and accuracy were also calculated. All performance parameters were provided with 95% Confidence Intervals (CIs). AUC was classified as fair in case of values between 0.70–0.80, good for >0.8 AUC < 0.9 and excellent for values > 0.9 [52].
The effect of anti-ZP antibodies in predicting a DS pregnancy was evaluated through logistic regression analysis adjusting for maternal age and was presented in terms of Odds Ratio (OR).
All estimates were provided with 95% CI. No imputation was performed for missing data and the level of significance was set at p = 0.05. Statistical analysis was performed by an experienced biostatistician (TP) using STATA software (STATA/BE 17.0 for Windows, Stata Corp LP, College Station, TX 77845, USA).
5. Conclusions
In this prospective case–control study, we demonstrated that anti-ZP antibodies are significantly associated with an increased risk of DS pregnancy. This association remained robust even after adjusting for maternal age, suggesting that anti-ZP antibodies may represent an age-independent risk factor for T21. We also identified that anti-ZP antibody levels above 1.0 OD predict DS pregnancy with excellent performance, indicating potential clinical utility for preconception or early-pregnancy risk assessment.
These findings support the broader hypothesis that autoimmune mechanisms may contribute to meiotic errors, complementing the well-established role of maternal age. The biological plausibility of this association is reinforced by previous evidence linking anti-ZP antibodies to impaired folliculogenesis, diminished ovarian reserve, and premature ovarian failure—all conditions that may compromise oocyte quality and increase susceptibility to nondisjunction.
While our study provides novel insights, several questions remain open. Because anti-ZP antibodies were measured postpartum, the temporal relationship between antibody production and conception cannot be fully established. Future longitudinal studies with pre-pregnancy sampling will be essential to clarify causality and to determine whether anti-ZP antibodies could serve as a reliable biomarker for DS risk. Additional research is also needed to explore the mechanistic pathways through which autoimmune dysregulation may influence meiotic competence.
Overall, our results suggest that maternal autoimmunity—particularly the presence of anti-ZP antibodies—may play a previously underappreciated role in the etiology of trisomy 21. If confirmed, this hypothesis could have important implications for preconception counseling, reproductive planning, and personalized risk assessment, especially for women who may be at risk independently of age.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mai C.T. Isenburg J.L. Canfield M.A. Meyer R.E. Correa A. Alverson C.J. Lupo P.J. Riehle-Colarusso T. Cho S.J. Aggarwal D. National population-based estimates for major birth defects, 2010–2014 Birth Defects Res.20191111420143510.1002/bdr 2.158931580536 PMC 7203968 · doi ↗ · pubmed ↗
- 2Loane M. Morris J.K. Addor M.C. Arriola L. Budd J. Doray B. Garne E. Gatt M. Haeusler M. Khoshnood B. Twenty-year trends in the prevalence of Down syndrome and other trisomies in Europe: 1990–2014 Eur. J. Hum. Genet.201826110111112271380410.1038/ejhg.2012.94PMC 3522199 · doi ↗ · pubmed ↗
- 3de Graaf G. Buckley F. Skotko B.G. Estimates of the live births, natural losses, and elective terminations with Down syndrome in the United States Am. J. Med. Genet. Part A 201516775676710.1002/ajmg.a.3700125822844 · doi ↗ · pubmed ↗
- 4Hassold T. Hunt P. Maternal age and chromosomally abnormal pregnancies: What we know and what we wish we knew Curr. Opin. Pediatr.20092170370810.1097/MOP.0b 013e 328332 c 6ab 19881348 PMC 2894811 · doi ↗ · pubmed ↗
- 5Nagaoka S.I. Hassold T.J. Hunt P.A. Human aneuploidy: Mechanisms and new insights Nat. Rev. Genet.20121349350410.1038/nrg 324522705668 PMC 3551553 · doi ↗ · pubmed ↗
- 6Gruhn J.R. Zielinska A.P. Shukla V. Blanshard R. Capalbo A. Cimadomo D. Nikiforov D. Chan A.C.-H. Newnham L.J. Vogel I. Chromosome errors in human eggs shape natural fertility over reproductive life span Science 20193651466146910.1126/science.aav 732131604276 PMC 7212007 · doi ↗ · pubmed ↗
- 7Eichenlaub-Ritter U. Staubach N. Trapphoff T. Chromosomal and cytoplasmic context determines predisposition to maternal age-related aneuploidy: Brief overview and update on MCAK in mammalian oocytes Biochem. Soc. Trans.2010381681168610.1042/BST 038168121118147 · doi ↗ · pubmed ↗
- 8Hunt P. Hassold T. Female meiosis: Coming unglued with age Curr. Biol.201020 R 699R 70210.1016/j.cub.2010.08.01120833308 · doi ↗ · pubmed ↗