Systemic Immunomodulatory Therapy, Anterior Chamber Inflammation, and the Use of Topical Corticosteroids in Juvenile Idiopathic Arthritis-Associated Uveitis: A Long-Term Real-Life Observational Study
Marija Barišić Kutija, Sanja Perić, Mario Šestan, Petra Kristina Ivkić, Martina Galiot Delić, Tomislav Jukić, Josip Knežević, Marijan Frković, Vladimir Trkulja, Marija Jelušić, Nenad Vukojević

TL;DR
This study examines long-term treatment effects in children with arthritis-related eye inflammation, finding that certain drugs significantly reduce inflammation and steroid use.
Contribution
The study provides real-life evidence on the effectiveness of sDMARD and bDMARD therapies in reducing uveitis severity and corticosteroid use in JIA-U patients.
Findings
sDMARD use was linked to a 15–20% lower probability of severe anterior chamber inflammation.
bDMARD or bDMARD + sDMARD use reduced severe inflammation by around 50% and steroid use by 60–65%.
Findings align with randomized trial results for adalimumab in treating JIA-U.
Abstract
Background: Juvenile idiopathic arthritis-associated uveitis (JIA-U) is a rare condition, and assessment of the efficacy of disease-modifying antirheumatic drugs, synthetic (sDMARD) or biological (bDMARD), in randomized trials is hindered by this fact. Methods: In this prospective longitudinal study, we observed 38 children aged 1.3 to 15.2 years, with 69 eyes affected with JIA-U for 1970 overall eye examinations (6–59, median 16) irregularly scattered across 4.4–87.6 months (median 21.6) of follow-up, with on- and off-periods of DMARD use and use of topical treatments. Results: With adjustment for several time-invariant and time-varying covariates, periods of exposure to sDMARD vs. no DMARD exposure were associated with peak benefits of 15–20% lower probability of having more severe anterior chamber (AC) inflammation and a similar relative reduction in the daily use of topical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
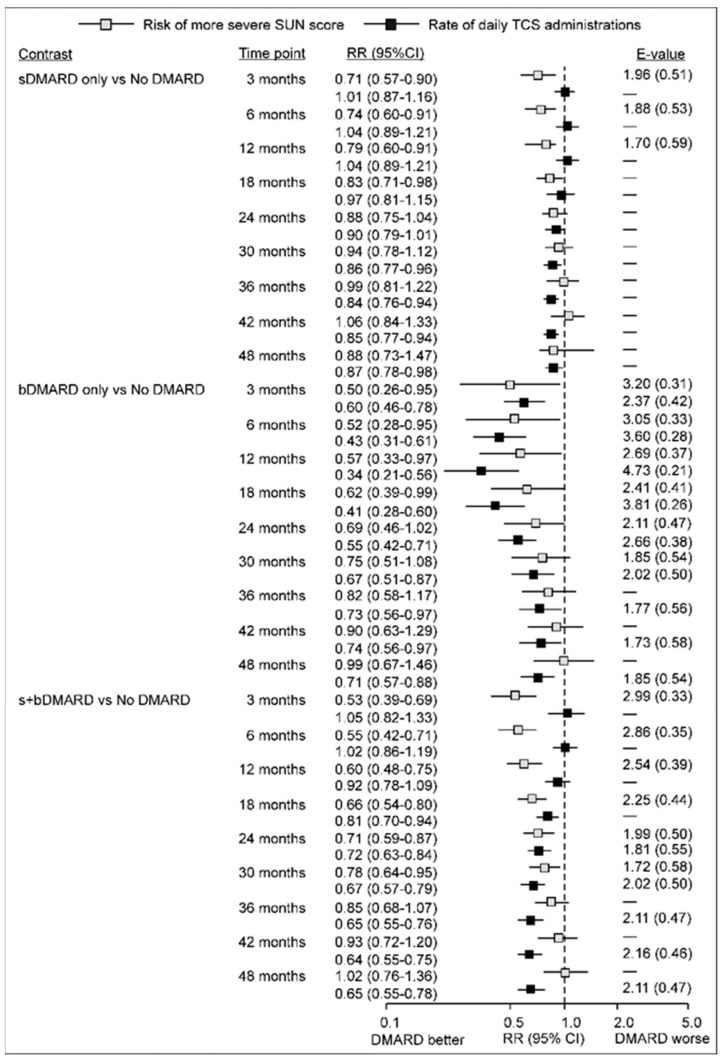 Figure 1
Figure 1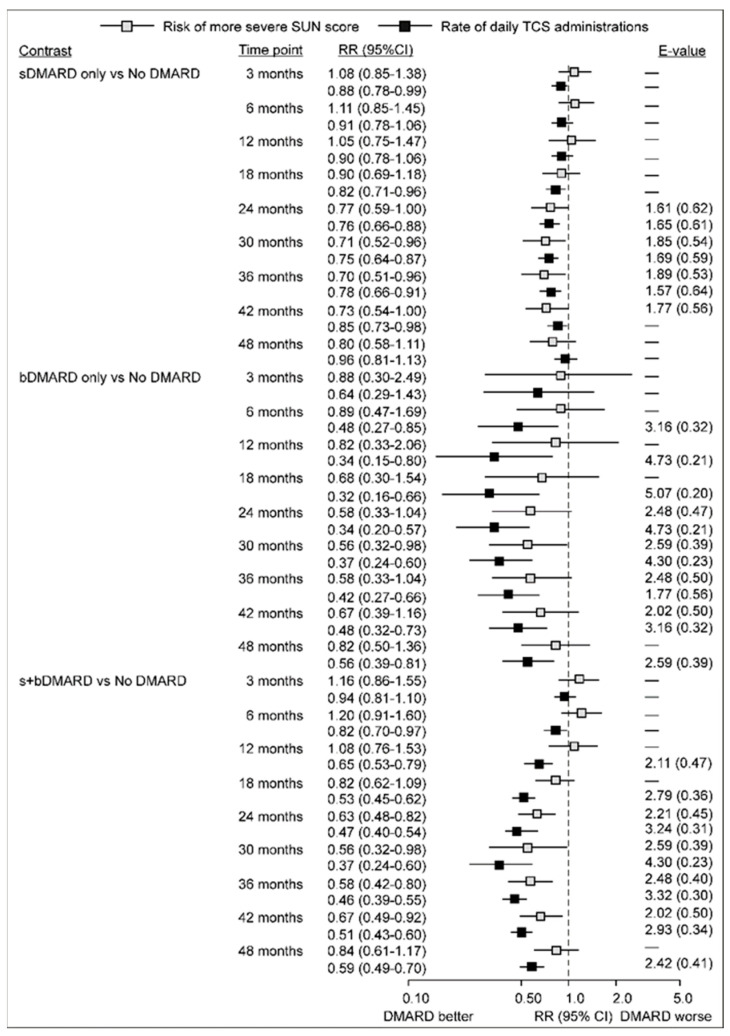 Figure 2
Figure 2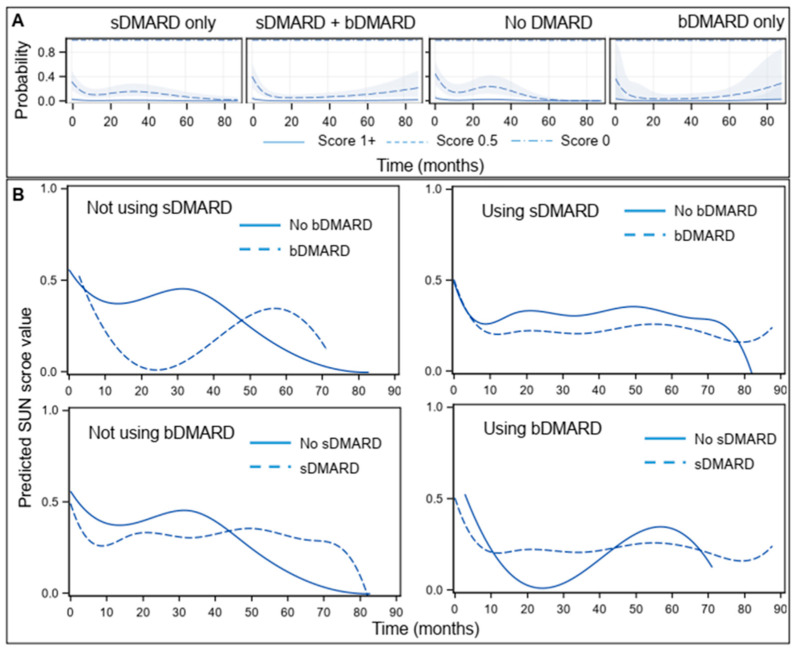 Figure 3
Figure 3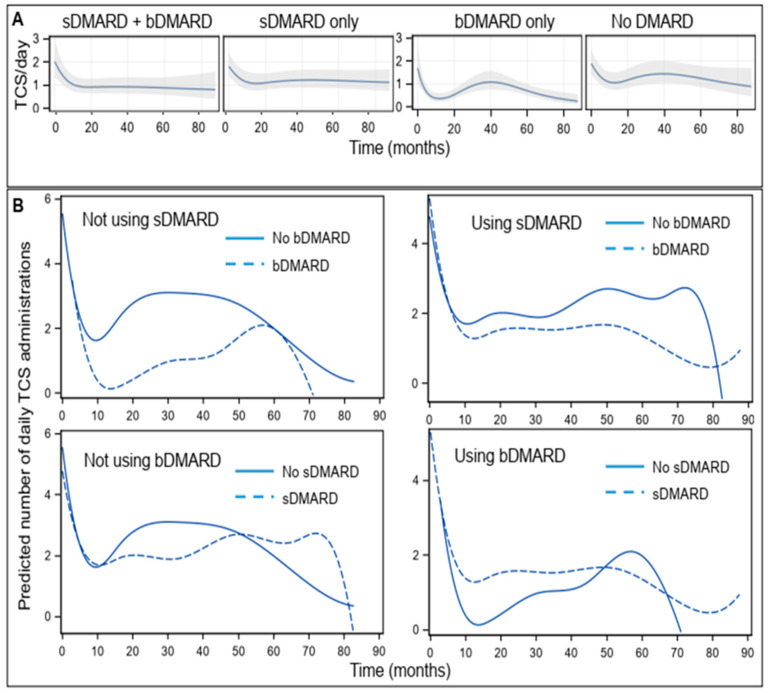 Figure 4
Figure 4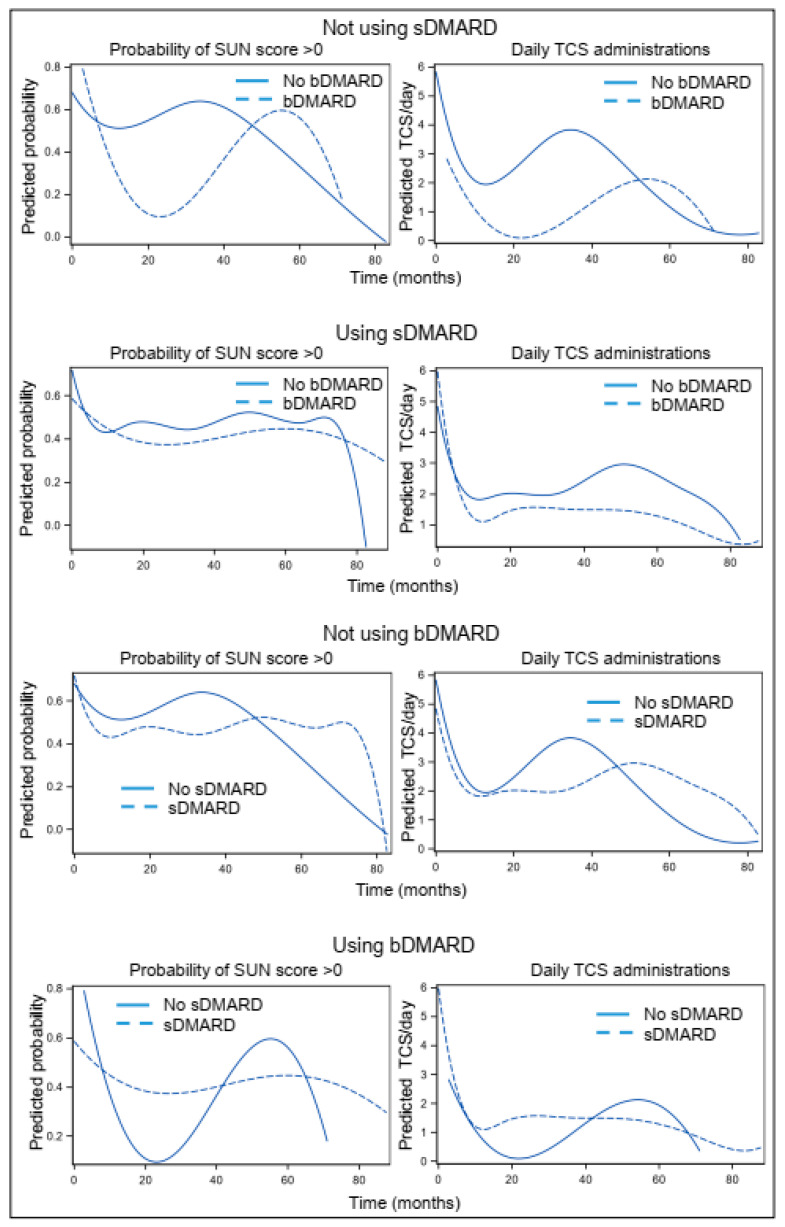 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Autoimmune and Inflammatory Disorders Research · Otitis Media and Relapsing Polychondritis
1. Introduction
Juvenile idiopathic arthritis-associated uveitis (JIA-U) is the most common extra-articular manifestation of JIA, and the main cause of childhood uveitis in developed countries [1,2,3,4,5,6,7]. Despite advances in JIA-U management [8,9], it remains one of the leading causes of vision impairment in childhood [10,11,12,13,14,15,16], and markedly reduces quality of life [17].
The goal in long-term therapy for chronic, refractory, or recurrent JIA-U is to suppress inflammation in the anterior chamber (AC) and to minimize the use of systemic and topical corticosteroids (TCS) [12,18,19] in order to avoid systemic and local adverse effects. Immunomodulatory treatment (IMT), which includes conventional (synthetic) and biologic disease-modifying antirheumatic drugs (sDMARD, bDMARD, respectively), is a corticosteroid-sparing therapy that may improve the disease course and outcomes [2,8,10,20,21,22].
Assessing treatment efficacy through randomized placebo-controlled or comparative trials (RCTs) in rare diseases is hindered by the low incidence/prevalence of eligible patients, a well-known issue in JIA-U [23,24]. In particular, the eligibility of JIA-U patients in whom IMT is indicated is even lower [14,25,26,27,28,29]. Only one moderately sized trial has assessed a bDMARD (adalimumab) (adalimumab versus placebo on top of a stable methotrexate (MTX)) with indicators of AC inflammation and systemic or topical corticosteroid use among primary and secondary endpoints [22]. Observational (real-life) data complement the estimates generated in RCTs by illustrating the extent to which treatment potentials are transferred to daily life (effectiveness), since they could be modified by circumstances not captured or intentionally avoided in RCTs. In rare diseases like JIA-U, observational data are particularly important, not only due to the lack of estimates from randomized settings, but also due to the complexity of the condition and a variety of intertwined factors that may affect the disease course and response to treatment [2,22,30]. Efforts towards standardized outcome measures and reporting across clinical studies evaluating treatment efficacy in JIA-U should increase the relevant knowledge base to define recommendable choices [31,32,33]. However, existing observational data typically stem from methodologically variable studies with different definitions of the outcomes and outcome measures, and with heterogeneous reporting [8,20,21,31,34,35,36,37,38,39]. As an illustration, we used two recent systematic reviews of the literature [34,35] to extract the main methodological characteristics of several larger (>20 patients) observational studies assessing the efficacy of IMT in pediatric JIA-U [38,40,41,42,43,44] (Appendix A). With respect to IMT specifically, this has two major consequences: (i) comparison of the results across studies is difficult or impossible; (ii) although “qualitative” conclusions are closely similar (IMT is or may be beneficial in JIA-U), it is difficult or impossible to generate reasonably accurate estimates of this benefit, including the type and extent of benefit that one could expect in daily treatment of JIA-U by introducing compounds from the IMT armamentarium.
In this context, we aimed to estimate the benefits (effectiveness) of systemic IMT, conventional or biological, in pediatric JIA-U patients over a long(er) follow-up period. Although several outcomes are informative about various aspects of the disease [32,33], we focused on two core ophthalmological outcomes: AC inflammation graded by the Standardization of Uveitis Nomenclature (SUN) criteria [45,46,47], and the extent of TCS use.
2. Materials and Methods
This longitudinal study was conducted at the Department of Ophthalmology, University Hospital Centre Zagreb, University of Zagreb School of Medicine, Croatia, between January 2011 and January 2018. The study enrollment period was up to 1 June 2017, in order to allow for at least a 6-month follow-up for the last enrolled patient. The study was strictly observational, in that study-related procedures pertained exclusively to the structured collection of the data of interest—no diagnostic or therapeutic procedure, nor the pattern of follow-up visits related to either JIA or JIA-U, were affected by study participation, and they remained solely at the discretion of the attending consultant. All ophthalmological examinations were conducted at a single site by the same consultant.
2.1. Patients and Patient Management
Those eligible for inclusion were (i) children aged 1 to 18 years, (ii) with verified JIA-U receiving sDMARD and/or bDMARD [48], and (iii) had written informed consent given by parents/guardians for the use of anonymized data for research and scientific publication. The starting point of observation was the first visit to our Department with verified JIA-U during the index period, whether incident (first diagnosis of JIA-U) or prevalent (e.g., the first control visit of patients with ongoing JIA-U during the index period, or prevalent patients referred from other institutions). The follow-up period lasted until 1 January 2018, or until loss to follow-up for any reason resulting in discontinuation of management at our institution. In such a case, the last visit recorded at our institution was the end of follow-up. Patients with uveitis of other etiologies and those with intense corneal opacities, disabling assessment of the cell counts in AC, were not included. Post hoc, we excluded a few initially enrolled patients with follow-up shorter than 3 months, as we considered this period insufficient for reliable evaluation and likely to introduce bias (e.g., a chance that findings would not be representative of disease evolution or response to treatment).
Patients were managed by a team of pediatric ophthalmologists and rheumatologists. Topical treatments (TCS drops or ointment, topical nonsteroidal anti-inflammatory drugs (NSAID), mydriatics) were steered by ophthalmologists, whereas systemic treatments (corticosteroids, NSAID, sDMARD, or bDMARD) were coordinated between specialists, and could be indicated based on the JIA status or JIA-U status, in line with the professional guidelines [2,8,9]. The first-line sDMARD was MTX, whereas leflunomide or mycophenolic acid were used sporadically as second-line options. The first-line bDMARDs were anti-TNF-alpha compounds, predominantly adalimumab, occasionally infliximab or etanercept. When adalimumab treatment was considered ineffective, the next-line choice was tocilizumab, or occasionally, etanercept/infliximab. If judged ineffective, first-line etanercept/infliximab was replaced with adalimumab, followed by tocilizumab if required. Similarly, treatments could be transiently (e.g., infection, side effects) or permanently withdrawn as deemed appropriate by the attending consultant. The pattern of scheduled ophthalmological follow-up visits was at the discretion of the attending consultant, depending on current AC inflammation severity. However, compliance with scheduled visits and treatment compliance (topical, systemic) could not be influenced beyond straightforward instructions to patients emphasizing their importance. Consequently, intervals between actual visits ranged from a few days or weeks to several months or even longer, influenced by unpredictable disease developments or intercurrent events (e.g., intensification, adverse events, local infections), and by patient-related factors. Appendix B. illustrates patterns of actual ophthalmological visits, findings, and treatments in two of the included patients. Overall, actual patient management reflected routine practice. Since all available data were considered without predefined study schedules in a controlled study protocol, the dataset is characterized by variability in examination frequency, follow-up time, demographic characteristics, and patterns of IMT.
2.2. Exposures, Outcomes, and Covariates of Interest
Exposures of interest were conventional and biological IMTs, or their combination: all sDMARDs were considered jointly (with a predominance of MTX), and all bDMARDs were considered jointly (with a predominance of adalimumab), as were their combinations. Exposure to these compounds was considered as a time-varying treatment with each patient contributing both “on-” and “off-” periods.
Outcomes of interest were the intensity of AC inflammation, graded as 0, 0.5, 1, 2, 3, or 4 (SUN criteria [46,47]), and the average total daily number (over the preceding week) of TSC applications (solution and ointment combined). Patient age at the start of follow-up, sex, age at JIA and at JIA-U onset, and whether the JIA was oligoarticular (vs. all other types) were recorded at the initial visit. Along with exposures and outcomes, other variables recorded at each visit were those considered possibly related to either exposures or outcomes, or both, directly or through mutual interplay: other systemic treatments (corticosteroids, NSAIDs), local findings (glaucoma or status post glaucoma, synechiae, cataract or status post cataract, keratitis) and local treatments (topical NSAID, mydriatics).
2.3. Data Analysis
The present data are specific, in that (i) patients underwent unequal numbers of unequally spaced follow-up visits, and their timing was likely driven by factors related and unrelated to the treated condition; (ii) indications for the installment of IMTs varied over time, and could have been determined not only by the ophthalmological status, but also by the underlying disease (JIA), and could have been commenced even when the local ophthalmological status per se would not have required them. As a consequence, individual patients contributed both “on-treatment” and “off-treatment” data, where the former occasionally might not have been informative about the treatment effect since the ophthalmological status was stable. Likewise, intercurrent events (e.g., infections) might have postponed or interrupted the treatment that was actually needed, resulting in enhanced AC inflammation or TCS use, thus “inflating” the difference between “on” and “off” treatment periods; (iii) in a setting with a varying treated condition (JIA-U), with a varying indicator (AC inflammation) prompting TCS or DMARD use, the basic condition of the temporal sequence in which presumed cause (treatment) precedes the outcome (e.g., local inflammation) is expectedly violated over time—the fact that a treatment was present at a certain time point could have been the outcome, and disease severity could have been a cause. In a classical observational cohort study with a clearly defined baseline and equally spaced post-baseline visits, time-varying treatment (arising from, e.g., inadequate compliance or intercurrent events) can be modelled by inverse probability of treatment weighting in marginal structural models, g-estimation of the structural nested models, or by g-computation [49], but none of these options were suitable for the current data structure. With this in mind, we aimed to estimate associations between exposures and outcomes of interest, while accounting for a reasonable number of covariates selected based on medical/biological rationale (“independent associations”). For interpretation of these associations, we relied on subject matter knowledge, and not exclusively on the formal proofs of no-reverse-causation or lack of selection.
If, repeatedly over the observational period, exposure to, for example, bDMARDs is associated with both less extensive TCS use and milder AC inflammation, while controlling for concomitant use of possibly interfering systemic treatments (corticosteroids, NSAIDs, sDMARD), topical treatments (topical NSAID, mydriatics), or local conditions that may influence decisions about topical or systemic treatment use (e.g., keratitis, cataract, glaucoma, synechiae), the association is suggestive of a causal effect. This inference is strengthened if effect estimates remain reasonably insensitive to residual confounding.
For the analysis of total daily TCS applications and the SUN score of the AC inflammation, the unit of observation was the eye. We fitted generalized mixed models for unequally spaced longitudinal data, with time in months as a continuous variable, and eye nested in patient as a random effect to account for correlation between repeated measures in the same eye and subject, and correlation between eyes in the same subject.
The total number of daily TCS applications/24 h was analyzed by fitting a Poisson model with fixed effects: (i) time-invariant covariates—age at the start of observation, age at JIA-U onset, and whether JIA was oligoarticular; (ii) time-varying covariates—use of systemic corticosteroids, use of systemic NSAIDs, presence of keratitis, synechiae, cataract or status post-cataract, glaucoma or status post-glaucoma, use of mydriatics, use of topical NSAID, and the SUN score of AC inflammation; (iii) time (in months) modelled as restricted cubic spline with 5 knots (placed by the Harrell’s rule); (iv) time-varying treatments of interest—sDMARD, bDMARD. A three-way interaction between time, sDMARD, and bDMARD was used to estimate differences between (a) bDMARD use vs. no DMARD, (b) sDMARD use vs. no DMARD, and (c) combined bDMARD and sDMARD use vs. no DMARD at different times since the start of observations (3, 6, 12, 18, 24, 30, 36, 42, and 48 months). The effect measured was the rate ratio, i.e., the relative (%) difference in TCS use.
The SUN score of AC inflammation was modelled as an ordered categorical variable (cumulative logit model). Since a score of 2 or 3 was observed only in a small fraction of the 1970 individual eye assessments, it was collapsed to 3 levels (0, 0.5, and 1 or higher). The fixed effects were the same as in the analysis of TCS use, except that (i) time was modelled as linear, since for cumulative logit models, cross-product matrix cannot be obtained for constructed effects (restricted cubic spline for time); (ii) while AC inflammation was a covariate in the analysis of TCS applications, TCS use was not included as a covariate in the analysis of the association between DMARD use (exposure) and AC inflammation (outcome). We reasoned as follows: (a) a certain level of AC inflammation prompts TCS use/intensification, and may also prompt the use of DMARDs. The expected benefit of introducing DMARDs (treatment) is to reduce the TCS use (outcome) for a given AC inflammation (a condition requiring either or both treatments); (b) in the RCT of adalimumab vs. placebo [22], the primary composite endpoint implied that for the avoidance of “treatment failure,” at least some improvement was required in the AC inflammation, indicating a benefit of adalimumab on this disease characteristic. At the same time, however, the use of TCS was restricted [22]. Current data were generated in daily practice without restrictions on TCS use, and TCS use was likely commonly prompted by the outcome of interest (reverse causation)—we deemed that conditioning on TCS use while assessing the association between exposure to DMARDs and AC inflammation was more likely to induce than to reduce bias. The outcome measured was the odds ratio, indicating the relative odds of having more severe AC inflammation. For data presentation, odds ratios were converted to relative risks by the optimal approximate conversion [50]: cumulative probabilities of having SUN score of 0.5 or 1+ were high (>10% of examined eyes); hence, odds ratios were numerically different from relative difference between treated and untreated eyes in probabilities (risks). Although the relative risk for such conversion is still somewhat biased vs. the true risk, it is less biased than the odds ratio and is more intuitive for interpretation. Finally, since AC inflammation and TCS use are closely correlated, the two were analyzed jointly by fitting a generalized model for joint analysis of binary (AC inflammation dichotomized to score 0 vs. any score > 0) (logit, with odds ratio finally converted to relative risk) and count data (number of TCS daily applications) (Poisson, rate ratio), with time modelled as a restricted cubic spline, and with fixed effects as in other models. All models employed robust (sandwich) variance estimation and Laplace approximation. All calculations were performed in SAS for Windows version 9.4 (SAS Inc., Cary, NC, USA).
To assess the sensitivity of the generated estimates to residual confounding, we calculated the E-value. This is expressed on a relative risk scale and quantifies the strength of association between (hypothesized) residual confounder(s) and both the exposure and the outcome that is needed to explain away the observed estimate [51].
3. Results
3.1. Eligible Patients and Follow-Up Data
We observed 38 children [32 (84.2%) girls] aged 1.3–15.2 years at the start of the observation, most [21 (55.2%)] suffering from oligoarticular JIA (Table 1). In 16 (42.1%) children, JIA-U was incident without complications, in an additional 11 (28.9%), it was incident with complications, and 11 (28.9%) children were referred to our institution with JIA-U previously treated elsewhere. Half of the children suffered JIA-U complications at the start of the observation (Table 1). Systemic treatment with sDMARDs, almost exclusively MTX, was already in place or was started at the first visit for 24 (63.1%) children, systemic corticosteroids were in place for 4 (10.5%), and NSAIDs for 18 (47.4%) children. At the first visit, a bDMARD was started or in use for 8 (21.0%) children (Table 1).
Of the 38 enrolled children, JIA-U was bilateral in 31 and unilateral in 7 children, for a total of 69 eyes. At the starting visit, most eyes had a SUN score of 0.5 or 1 [20 (29.0%) and 26 (37.7%), respectively] (Table 1), 9 (13.0%) had a score of 0, and no eye was scored 4+ (Table 1). The most common complications were cataract in 17 (26.4%) eyes, synechiae in 20 (29.0%) eyes, and keratopathy in 15 (21.7%) eyes (Table 1). At the start of the observation, all 38 children were administering TCS as drops or ointment to at least one affected eye, and 33 were using both. Of the 69 eyes, 8 were untreated with TCS, 61 were treated with TCS drops, and 52 with TCS ointment (combined with drops) (Table 1). The total number of daily TCS applications ranged from 0 to 20, with a median of 6 (Table 1).
Patients were followed-up with a median of 21.6 months (range 4.4 to 87.6, quartiles 7.6 and 40.2 months). During this time, they were examined on 6 to 59 occasions (including the initial visit, with a median of 16, and quartiles of 8 and 27). The time between visits varied from a few days to several months. Overall, 1970 eye examinations were performed.
Table 2 summarizes data considered in the present analysis grouped in 6-month intervals. Within the initial 6-month period, all 38 were examined at least once, and for a maximum of 12 times (median 6.5), resulting in 476 examined eyes. The number of examined children and eyes gradually declined over time. Between months 48 and 54, fewer than 20 children were examined, and this number progressively declined further (Table 2). Hence, we used all available data across time in analytical models, but we generated estimates of interest only up to month 48.
Across the time intervals, most eyes were treated with TCS at the time of examination, with sDMARD (MTX) in use. Approximately 30% of all eye examinations were undertaken while bDMARDs were in use (Table 2).
3.2. sDMARDs, bDMARDs, and Their Combination vs. AC Inflammation and TCS Use
Table 3 summarizes adjusted predicted probabilities of SUN score and the predicted average number of daily TCS applications at specific time points generated in separate models for the AC inflammation (AC SUN score) (cumulative logit) and TCS applications (Poisson). Appendix C, Figure A1 illustrates data for the SUN score categories, and Figure A2 illustrates data for the TCS applications over the entire observed period.
The probabilities of SUN scores of 1+ or 0.5 gradually declined over time under all conditions of interest: no DMARD in use, sDMARD in use, bDMARD in use, or both sDMARD and bDMARD in use (Table 3). Across most time points, the probability of a score of 0 was the highest, and the probability of a score of 1+ or 0.5 was the lowest for eyes assessed when bDMARD (only) was in use. The values were similar for assessments when both sDMARD and bDMARD were in use (Table 3). The probabilities for assessments while sDMARD was in use appeared somewhat more favourable than those obtained with no DMARD in use, but not unequivocally (Table 3). The total number of daily TCS applications oscillated over time under all four conditions, but the values appeared consistently lower for the condition of bDMARD use or both sDMARD and bDMARD use, compared to no DMARD or sDMARD use (Table 3).
Figure 1 summarizes the estimated differences at specific time points after the start of observation in the probability of a more severe SUN score and in the total daily number of TCS applications between eyes assessed when an sDMARD (only) or a bDMARD (only) or both s+bDMARD were in use vs. eyes assessed when no DMARD was in use with each outcome analyzed in a separate model.
Regarding specific contrasts (Figure 1), (i) between months 3 and 18, the risk of a more severe SUN score appeared 20–30% lower under exposure to sDMARD compared to no DMARD, while the rate of daily TCS applications appeared similar (RRs around 1.0). After that, the risk of more severe SUN scores tended to be similar under sDMARD and no DMARD, but the rate of TCS applications appeared 10–15% lower under the former condition; (ii) a similar pattern was observed for eyes assessed under s+bDMARD exposure compared to no DMARD, except that the difference in risk of more severe SUN scores was more pronounced and persistent: it varied from being 50% lower at 3 months to 22% lower at month 30 of the observation, whereas between month 18 and month 48 of the observation, s+bDMARD exposure was associated with a 20% to 35% lower rate of TCS use; (iii) estimates generated for the bDMARD vs. no DMARD contrast had wide confidence intervals, since bDMARD only was less commonly in use than an sDMARD or their combination. Eyes assessed under bDMARD (only) exposure were associated with a 50% to 25% lower risk of more severe SUN scores between months 3 and 30 of the observation compared to eyes assessed under no DMARD exposure. In later months, this risk tended to be comparable for the two conditions, but exposure to bDMARD was consistently associated with a lower rate of TCS use—the rate appeared 65–25% lower across the time points. Since the rate of TCS use was estimated while accounting for the concurrent SUN score, data are in line with the expectations based on the randomized trial of adalimumab vs. placebo: at a comparable level of AC inflammation, DMARD-exposed vs. non-exposed patients are likely to use relatively less TCS, or, if the TCS use is comparable, DMARD exposure vs. non-exposure is likely to be associated with less severe AC inflammation. The observed patterns reflect the daily-life development in which the disease status prompts (“causes”) use of topical or systemic treatments, which in turn reduces the disease intensity; hence, at certain time points, exposure (expected to be therapeutic) might transiently associate with poorer disease status, or appear to produce no benefit regarding either AC inflammation, or TCS use, or both, but over segments of time, the association of treatment with some form of benefit is apparent.
Figure 2 summarizes the estimated differences between sDMARD, bDMARD, or s+bDMARD exposure and no DMARD exposure at different time points assessed in a model that jointly analyzed the probability of having a SUN score > 0 and TCS daily applications (Appendix C, Figure A3 illustrates predictions across the entire observed period). Generally, the observed patterns are similar to those in Figure 1, but with some specifics. At the earlier time points, both outcomes appeared similar in eyes assessed under DMARD exposures and eyes assessed with no DMARD exposure. This might be due to the fact that 27/38 children had incident JIA-U, and 11 were referred to us from other institutions due to unsuccessful treatment; hence, the start of the present observations coincided with the start of adequate treatment. Differences between exposure to sDMARD alone and no DMARD were apparent at month 24 to month 42 of observation: the probability of SUN scores > 0 was 30% to 27% lower, and the rate of TCS daily applications was 15% to 25% lower with exposure to sDMARD (Figure 2). Differences between exposure to bDMARD alone and no DMARD in TCS use were apparent at month 6 to month 48: the rate of daily applications was lower by 52% to 68% (Figure 2). Differences in the probability of SUN scores > 0 were apparent at months 24, 30, and 36 (42–44% lower) (Figure 2). Differences between exposure to both sDMARD and bDMARD and no DMARD in TCS use were apparent at months 12 to 42: the rate of daily applications was lower by 35% to 63% (Figure 2). Differences in the probability of SUN scores > 0 were apparent at months 24, 30, 36, and 42 (33% to 42% lower) (Figure 2).
4. Discussion
In the present study we aimed to assess the benefits of systemic IMTs, i.e., sDMARDs and bDMARDs, that one could reasonably expect in the real-life treatment of children with JIA-U. We focused on two straightforwardly identifiable and practically meaningful outcomes commonly used to guide the use of topical or systemic treatment [31,33,52,53]: the intensity of AC inflammation (the SUN score) and intensity of TCS use represented by the total number of applications over 24 h. Treatments (exposures) of interest were defined in line with the up-to-date practice regarding IMT use in this indication [2,8,9,19]: sDMARDs (preferably MTX) are the first-line IMT choice; bDMARDs (preferably anti-TNF-alpha compounds) are an alternative (contraindications or adverse effects of sDMARD, inefficacy), or an add-on treatment. They were assessed in comparison to no exposure to DMARDs. Hence, we report on medically relevant exposures and outcomes, where neither was susceptible to misclassification.
Assessing treatment effects implies the estimation of causal effects, a goal difficult to achieve in non-randomized settings. Even under “ideal” circumstances, such efforts are susceptible to a number of biases. With this in mind, we interpret the present estimates as indicators of the strength of association between the exposures and the outcomes of interest. However, the biological and medical plausibility of actions undertaken in the management of children suffering JIA-U over time strengthens the view that these associations predominantly reflect treatment effects.
The present cohort included all children with JIA-U on systemic IMT managed at our institution over the index period, with only a few exceptions (when the observed period was shorter than 3 months, or AC inflammation was physically impossible to assess). Hence, they represent a sample of unselected consecutive children, most of whom were incident JIA-U patients (27/38). Over time, however, some form of patient selection most likely occurred: those achieving remission were likely less commonly seen or attended fewer/no ophthalmological visits, whereas those with more intense JIA-U might have been assessed more frequently and over a longer period of time. The apparent loss of association between DMARD exposure and lower probability of more severe SUN score (Figure 1) or score > 0 (Figure 2) supports such a view: the estimates at month 42 and 48 could have been based on data collected in children with difficult-to-treat AC inflammation who likely did not benefit much in this respect, although the association with less-frequent TCS use seemed clear. These observations are in agreement with the fluctuating nature of JIA and JIA-U [8], which are conditions that require flexible treatments (types and dosage). In this regard, the present data resemble a pragmatic trial with treatments guided by the development of the disease and treatment tolerability, with no restrictions imposed. Under such circumstances, associations between the exposures and outcomes at some time points might be due to reverse causation, while a lack of such associations (despite the expectations based on the current knowledge) might be due to the fact that the moment of assessment represents a “new baseline” as a consequence of a relapse of a previously (due to treatment) remitted disease. These facts may be viewed as limitations of the present study in the sense that they obscure quantification of causal treatment effects. On the other hand, they may also be considered as strengths, since they reflect developments of the disease in JIA-U patients over time. Finally, these characteristics distinguish the present study from most prior observational studies (also susceptible to various biases), which typically assessed outcomes at single time points, failing to capture clinically meaningful variation across variably timed prescheduled examinations—variation that may reflect transient spikes in inflammation, subsequent intensified corticosteroid exposure, and increased risk of ocular complications.
The present study is based on a sample of patients that might be considered reasonably large for a rare disease, with repeated ophthalmological assessments over a reasonably long period. As such, we believe it is more informative about treatment effectiveness (ability of a treatment to control the disease in daily life) than the observations focused on single time points [54].
Further strengths of the present study arise from the fact that we accounted for a number of time-varying covariates that could be reasonably viewed as confounders, and that the generated estimates showed closely similar patterns and values with two different data analysis approaches (i.e., were not model-dependent). When the estimates suggested associations between the exposure and outcomes, the E-values were rather high, indicating reasonable “resistance” of the estimates to residual confounding. Although this fact does not render the interpretation of the associations to be causal (in the treatment–outcome direction), it does support a conclusion that these associations were very likely “independent associations”.
Our present observations are in agreement with expectations based on the current knowledge and experience regarding the benefits of DMARDs in children with JIA-U [2,20,21,22,34,35]. Considering the lack of data, they cannot be assessed in relation to effects estimated in randomized trials, but under the elaborated conditions—since the rate of TCS use was estimated while accounting for the concurrent SUN score—the data are consistent with the expectations based on the randomized trial of adalimumab vs. placebo [22]: DMARD-exposed vs. non-exposed patients were likely to have less-severe AC inflammation and to use relatively less TCS. Therefore, our study enables certain reasonably supported conclusions: (i) over time, children with JIA-U treated with sDMARD (typically MTX, compared to no DMARD) should be expected to experience a relevant reduction in the need for TCS. This benefit may fluctuate due to a variety of reasons, but it could amount to as much as 25% reduction in TCS use. This may also be accompanied by a reduction in AC inflammation indicated by, e.g., an around 15% lower probability of “more severe” inflammation (e.g., SUN score 1 or higher vs. 0.5 or 0, or as SUN score 0 vs. any score > 0), or a maintenance of stable low-level AC inflammation. These expectations assume adequate sDMARD compliance, not compromised by disruptions; (ii) under the same conditions, children treated with bDMARD (typically anti-TNF-alpha compounds) should be expected to experience even greater average reductions in TCS use (e.g., up to a 50% or 60% reduction), with concomitant clinical improvements indicated by reduced probability (e.g., 30–40% on average) of more severe SUN scores, or any score > 0; (iii) children exposed to combined sDMARD and bDMARD could be reasonably expected to experience similar benefits regarding JIA-U.
To date, many other studies have suggested good effectiveness of IMT in controlling JIA-U but have reported short-term, methodologically heterogeneous observational results with likely considerable biases. As such, whether considered individually or jointly (e.g., in systematic reviews), they do not allow for uniform or subpopulation-specific estimates of treatment benefits of IMT (sDMARD, bDMARD) that one could consider to be most likely accurate [8,20,21,34,35,36,37,55,56]. Consequently, an urgent need for well-designed, long-term, and pragmatic comparative trials with standardized methodological features has been repeatedly advocated [8,34,35,55,56].
The only published RCT on the topic (evaluating AC inflammation and TCS use as outcome measures) [22] is a formal regulatory phase III trial of adalimumab vs. placebo in a moderately sized sample of children with JIA-U on “background” MTX treatment, with at least SUN grade 1+ AC inflammation, and a limited topical (and restricted during the trial) and systemic glucocorticoid use (intensification prohibited during the trial). Over an 18-month period, the cumulative risk of treatment failure (no improvement or worsening of inflammation by several criteria) was 60% lower in the treated children (RR = 0.40, 95% CI 0.22–0.73) [22]. At the same time, among children using TCS at a rate of at least one drop/day, reduction to zero drops/day was achieved in 47% of treated and 16% of control children (i.e., a three-fold higher probability) [22]. In the present study, periods “on bDMARD” or “on bDMARD + sDMARD” were compared to periods with no DMARD, which, to some extent, corresponds with the RCT: the peak benefits (although differently defined) in AC inflammation associated with the exposure were around 50% less inflammation, and the peak TCS use benefits were around a 60–65% reduction (this would correspond to a three-times-higher probability of reduced/none TCS use, e.g., 1/(1 − 0.65) = 2.9). In this respect, it seems plausible to conclude that the present observations are in agreement with the RCT results, not only qualitatively, but also quantitatively.
5. Conclusions
In this longitudinal observation study, we evaluated 38 children aged 1.3 to 15.2 years with 69 eyes affected with JIA-U for a total of 1970 eye examinations (minimum 6, maximum 59, median 16) irregularly scattered across 4.4–87.6 months (median 21.6 months) of follow-up. With adjustment for time-invariant (age at the start of observation, age at JIA onset, age at JIA-U onset, whether JIA was oligoarticular) and time-varying covariates (topical and systemic treatments, local ophthalmological conditions), periods of exposure to sDMARD (MTX) vs. no DMARD exposure were associated with peak benefits of 15–20% lower probability of having more severe AC inflammation (SUN score 1+ vs. 0.5 vs. 0), and a similar relative reduction in TCS daily applications. Periods of bDMARD exposure or of bDMARD+sDMARD exposure vs. no DMARD use were associated with peak benefits of around 50% reduction in probability of having more severe AC inflammation, and peak benefits of around 60–65% reduction in TCS use. The observations regarding bDMARD (only) or bDMARD + sDMARD exposure are in agreement with the extent of benefit suggested for adalimumab vs. placebo (+background MTX) in a randomized trial [22].
We underscore the need for harmonized standards in future JIA-U research. Unified protocols for database construction, outcome selection, and statistics methodology are essential to improve comparability and clinical interpretability across studies. We hope that the insights provided here—both regarding data structures and analytical approaches—will contribute to the ongoing development of consensus recommendations and enhance the quality of evidence in this field.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Renton W.D. Jung J. Palestine A.G. Tumor Necrosis Factor (TNF) Inhibitors for Juvenile Idiopathic Arthritis-Associated Uveitis Cochrane Database Syst. Rev.202210 CD 01381810.1002/14651858.CD 013818.pub 236239193 PMC 9562090 · doi ↗ · pubmed ↗
- 2Bani Khalaf I.M. Jain H. Vora N.M. Ul Ain N. Murtaza F. Ram M.D. Nankani A. Motwani J. A Clearer Vision: Insights into Juvenile Idiopathic Arthritis-Associated Uveitis Bayl. Univ. Med. Cent. Proc.20243730331110.1080/08998280.2024.2305567 PMC 1085745338343470 · doi ↗ · pubmed ↗
- 3Clarke S.L.N. Mageean K.S. Carlton H. Simonini G. Sharp G.C. Relton C.L. Ramanan A.V. Environmental Risk Factors Associated with Juvenile Idiopathic Arthritis Associated Uveitis: A Systematic Review of the Literature J. Ophthalmic Inflamm. Infect.2021111510.1186/s 12348-021-00247-134027581 PMC 8141477 · doi ↗ · pubmed ↗
- 4Prakken B. Albani S. Martini A. Juvenile Idiopathic Arthritis Lancet 20113772138214910.1016/S 0140-6736(11)60244-421684384 · doi ↗ · pubmed ↗
- 5Thorne J.E. Woreta F. Kedhar S.R. Dunn J.P. Jabs D.A. Juvenile Idiopathic Arthritis-Associated Uveitis: Incidence of Ocular Complications and Visual Acuity Loss Am. J. Ophthalmol.2007143840846.e 210.1016/j.ajo.2007.01.03317362866 · doi ↗ · pubmed ↗
- 6Clarke S.L.N. Sen E.S. Ramanan A.V. Juvenile Idiopathic Arthritis-Associated Uveitis Pediatr. Rheumatol.2016142710.1186/s 12969-016-0088-2PMC 484880327121190 · doi ↗ · pubmed ↗
- 7Heiligenhaus A. Heinz C. Edelsten C. Kotaniemi K. Minden K. Review for Disease of the Year: Epidemiology of Juvenile Idiopathic Arthritis and Its Associated Uveitis: The Probable Risk Factors Ocul. Immunol. Inflamm.20132118019110.3109/09273948.2013.79170123713827 · doi ↗ · pubmed ↗
- 8Angeles-Han S.T. Lo M.S. Henderson L.A. Lerman M.A. Abramson L. Cooper A.M. Parsa M.F. Zemel L.S. Ronis T. Beukelman T. Childhood Arthritis and Rheumatology Research Alliance Consensus Treatment Plans for Juvenile Idiopathic Arthritis–Associated and Idiopathic Chronic Anterior Uveitis Arthritis Care Res.20197148249110.1002/acr.23610 PMC 626170429806733 · doi ↗ · pubmed ↗