Anterior Cervical Abscess Following Anterior Cervical Discectomy and Fusion Caused by Moraxella catarrhalis: A Case Report and Focused Literature Review
Helen Mary Hall, Finley Bettsworth, Imran Haq, Mario Ganau

TL;DR
A rare case of a post-surgery neck abscess caused by a respiratory bacteria is reported, emphasizing the importance of considering unusual pathogens in high-risk patients.
Contribution
This case report is the first to document Moraxella catarrhalis as a cause of postoperative anterior cervical abscess following ACDF.
Findings
Moraxella catarrhalis was identified as the causative agent in a postoperative cervical abscess.
The patient recovered fully with surgical drainage and targeted antibiotic therapy.
The case highlights the need to consider respiratory tract organisms in postoperative infections.
Abstract
Background: Anterior cervical discectomy and fusion (ACDF) is widely performed and has a low incidence of postoperative infection. Anterior cervical abscess is a rare but potentially life-threatening complication, typically caused by skin or oral flora. Identification of atypical pathogens has important implications for diagnostic vigilance and antimicrobial management. Case Presentation: We report a 56-year-old man with degenerative cervical myelopathy and significant respiratory comorbidity who underwent single-level ACDF and developed progressive dysphagia and neck pain in the early postoperative period. Imaging demonstrated a prevertebral abscess requiring urgent surgical drainage. Intraoperative cultures identified Moraxella catarrhalis, a respiratory tract commensal rarely implicated in postoperative spinal infections. No evidence of esophageal perforation or superficial wound…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
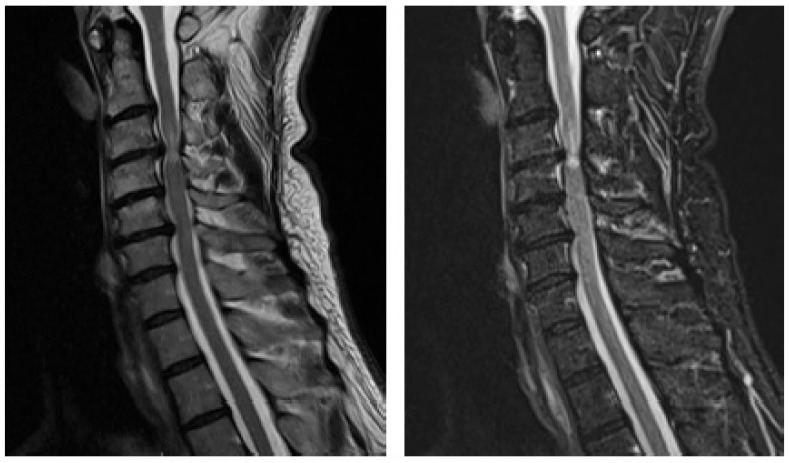 Figure 1
Figure 1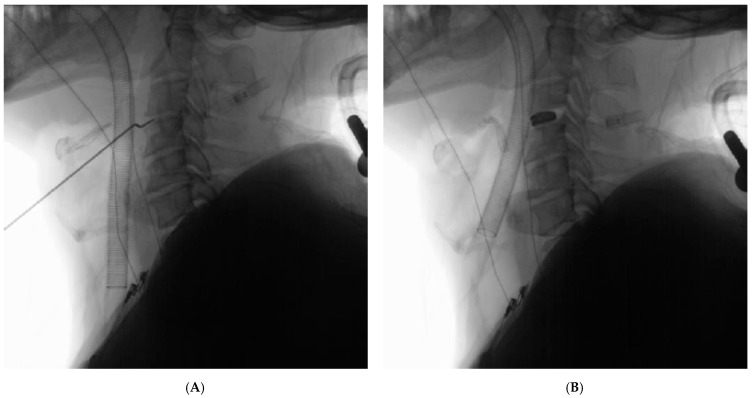 Figure 2
Figure 2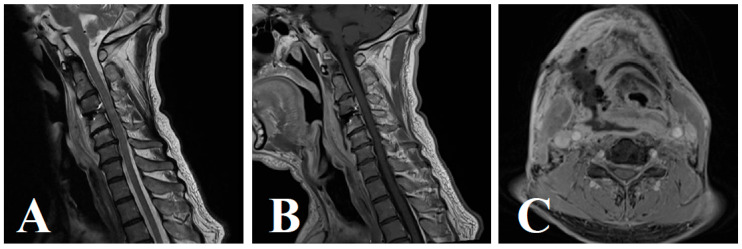 Figure 3
Figure 3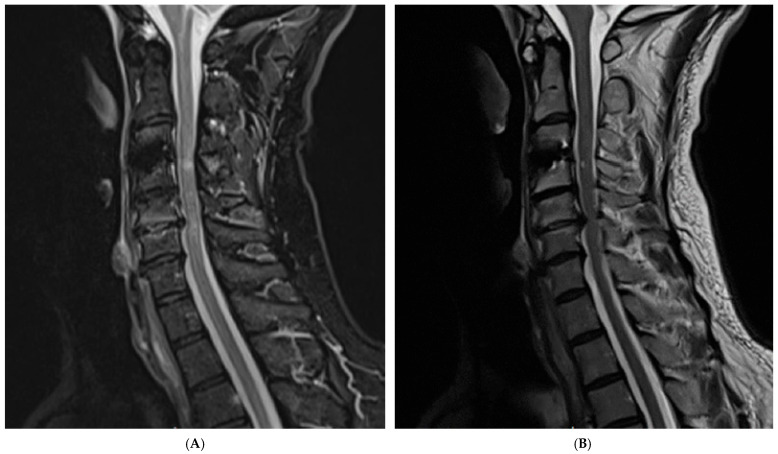 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Otolaryngology and Infectious Diseases · Bacterial Infections and Vaccines
1. Introduction
Anterior cervical abscesses (ACAs) are a rare but potentially serious surgical complication following anterior cervical discectomy and fusion (ACDF) [1]. ACAs typically present in the early postoperative period with nonspecific symptoms, including neck pain and stiffness, fever, dysphagia, neck swelling or erythema, and neurological deficits [2,3]. Infections following ACDF are most commonly caused by skin and oral flora, with Staphylococcus aureus being the most frequently isolated pathogen [1,2]. Other reported organisms include Streptococcus intermedius, Serratia marcescens, and Propionibacterium acnes [4].
Here, we report a case of ACA following ACDF caused by Moraxella catarrhalis, an organism that is typically regarded as a benign colonizer of the upper respiratory tract [5]. To the best of our knowledge, M. catarrhalis has not previously been reported as the causative pathogen in post-ACDF cervical abscess formation. In this case, abscess development was attributed to transient M. catarrhalis bacteremia at the time of surgery. A contributory factor may have been mucosal microtrauma related to endotracheal intubation, highlighting a potentially under-recognized iatrogenic mechanism for postoperative ACA formation.
This case underscores the importance of maintaining a high index of suspicion for atypical pathogens in postoperative spinal infections, particularly in patients with respiratory risk factors such as chronic obstructive pulmonary disease requiring corticosteroid therapy, active smoking, and reduced respiratory reserve secondary to degenerative cervical myelopathy. In addition, it draws attention to the vulnerability of the anterior cervical anatomy in the context of airway management and surgical exposure.
To contextualize the novelty of this case, we performed a focused literature review to situate this report within the existing body of evidence. We therefore present the first reported case of an anterior cervical abscess following ACDF caused by Moraxella catarrhalis. This report expands the spectrum of recognized post-ACDF pathogens and emphasizes the need for comprehensive microbiological evaluation and individualized, culture-directed management in postoperative spinal infections.
2. Case Presentation
A 56-year-old right-hand-dominant male presented with an 18-month history of progressive cervical myelopathy, characterized by clumsiness, frequent dropping of objects, gait instability, and urinary urgency. His symptoms had deteriorated significantly over the preceding 6 months. His past medical history included chronic obstructive pulmonary disease (COPD), managed with daily oral prednisone (5 mg), and a prior non-ST elevation myocardial infarction (NSTEMI), for which he was taking clopidogrel. He was an active smoker at the time of surgery.
On neurological examination, motor strength was preserved in both upper and lower limbs. However, the patient exhibited bilateral hypoesthesia, reduced proprioception in the lower limbs, brisk reflexes throughout, a positive Babinski reflex, and an unsteady tandem gait. No clonus was observed. Clinical findings proved consistent with advanced DCM. The Modified Japanese Orthopedic Association (mJOA) scale is widely used and validated for assessing the severity of degenerative cervical myelopathy [6]. As per the mJOA scoring system, the patient was found to have a score of 10/18 (indicating severe cervical myelopathy) due to difficulties with fine motor control, mobility aid requirement, sensory disturbance, and bowel and bladder symptoms.
MRI of the cervical spine demonstrated multilevel degenerative disc disease from C3/C4 to C5/C6, with the most pronounced spinal cord compression and T2-weighted signal hyperintensity at C3/C4, suggestive of myelomalacia (Figure 1).
Following discussion in a multidisciplinary team (MDT) meeting and consultation in the neurosurgical outpatient clinic, the patient was counseled regarding surgical options. These included ACDF at C3/C4 or posterior decompression with laminectomy and fusion from C3 to C6 [7]. After discussion of benefits and risks, including the potential for watchful waiting or a posterior approach with lateral mass screw fixation, the patient consented to proceed with ACDF at C3/C4.
The procedure was performed under general anesthesia without intraoperative complication. Intubation proved difficult as a result of moderate degree of oropharyngeal obstruction (Mallampati Class III) and limited cervical mobility attributed to the patient’s DCM. No mucosal injury was identified intraoperatively.
A right-sided anterior cervical approach was used. After disc excision and decompression, a 3D-printed titanium interbody cage with lordotic profile was implanted. No visceral injury nor cerebrospinal fluid (CSF) leak was recorded. Intraoperative fluoroscopy confirmed correct implant placement (Figure 2). Hemostasis was secured, and a subfascial drain was placed prior to layered closure.
The patient was discharged on postoperative day-1 in a stable condition without any clinical concerns. This early discharge was in line with enhanced recovery after surgery (ERAS) principles, aiming to reduce hospital stays and complications while promoting early mobilization [8]. By day 5, he developed mild dysphagia and low-grade fever. Clinical examination was unremarkable, and laboratory findings revealed normal leukocyte count with mildly elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). A cervical CT scan was obtained but showed stable positioning of the C3–4 interbody cage without evidence of hardware migration, subsidence, or prevertebral collection. The patient was discharged with advice for symptomatic care.
Two days later (postoperative day 7), the patient re-presented with worsening neck pain, swelling, and tenderness. Repeat bloods demonstrated stable inflammatory markers. Given clinical suspicion for deep space infection, the patient underwent a diagnostic workup, starting with dynamic barium swallow studies. Lateral barium swallow fluoroscopy demonstrated mild prevertebral impression without evidence of contrast leak, and anteroposterior view confirmed symmetrical esophageal transit.
Given the persistent symptoms, an urgent contrast-enhanced MRI of the cervical spine was obtained. Imaging revealed a rim-enhancing prevertebral fluid collection at the C3–4 level, with displacement of the trachea and esophagus, consistent with a deep cervical abscess (Figure 3A–C). These imaging studies confirmed the presence of a prevertebral abscess, prompting urgent surgical exploration and drainage.
The patient underwent emergent surgical exploration and drainage of the prevertebral abscess. Approximately 30 mL of purulent material was evacuated. ENT consultation confirmed no evidence of esophageal perforation or other visceral injury. Intraoperative ultrasound (IoUS) confirmed complete washout of the surgical site. Intraoperative cultures identified Moraxella catarrhalis, a respiratory commensal rarely implicated in postoperative spinal infections. Intraoperative swabs from the skin and suprafascial layers were also obtained and yielded no bacterial growth. In addition, extended cultures of deep neck wound specimens showed no growth of Actinomyces species after 2 weeks of incubation.
The organism was resistant to amoxicillin but sensitive to trimethoprim–sulfamethoxazole and azithromycin. In consultation with the infectious diseases team, the patient was commenced on a 3-month course of dual oral antibiotics (trimethoprim-sulfamethoxazole [TMP-SMX] and azithromycin) guided by microbiological sensitivities and clinical response. No further surgical intervention was required.
All microbiological analyses were performed by the hospital diagnostic microbiology laboratory as part of routine clinical care; representative intraoperative microscopy or culture plate images were therefore not available for inclusion, and results are described in the text.
At 6-month follow-up, the patient demonstrated marked clinical improvement, with resolution of dysphagia and return to neurological baseline. Repeat MRI showed no residual abscess, spinal cord compression, or new instability (Figure 4). No recurrent infection was observed, no long-term antibiotic-related adverse effects were reported, and the fusion construct remained well-aligned.
Detailed perioperative timelines and laboratory values are available from the authors on request. The clinical course is summarized in Figure 5.
3. Discussion and Review of the Literature
ACDF is the most commonly adopted anterior approach to surgically address cervical spine pathologies [1,9], with alternative surgical corridors being the lateral and posterior routes [7,10]. Our patient underwent ACDF, having presented with symptoms associated with cervical myelopathy including clumsiness, urinary symptoms, unsteady gait, and sensory disturbance. Following mJOA scoring, this was found to be a case of severe cervical myelopathy with an mJOA score of 10/18 [6]. Following the patient’s ACDF, he re-presented on postoperative day 5 with mild dysphagia and low-grade fever, which was later found to be an ACA, a form of deep surgical site infection. Surgical drainage and intraoperative cultures revealed the causative agent to be M. catarrhalis, a benign colonizer of the upper respiratory tract [5]. This case highlights how uncommon respiratory tract organisms may cause serious postoperative spinal infections in selected high-risk patients, despite adherence to standard perioperative protocols.
3.1. Pathogen Characteristics
To the best of our knowledge, the current literature has no reported cases of ACA formation following ACDF attributed to M. catarrhalis. Rather, infections following ACDF are most commonly caused by skin and oral flora, with Staphylococcus aureus being the most frequently isolated pathogen [1,2]. The typical microorganisms involved in post-ACDF anterior cervical deep wound infections also include Streptococcus species and anaerobic bacteria [1,2,5]. Indeed, several causative pathogens have been implicated in both early and late infectious complications following spinal surgery. However, the vast majority of reported organisms are derived from cutaneous or oropharyngeal flora, making the identification of M. catarrhalis in this context particularly unusual.
In contrast to typical post-ACDF pathogens such as Staphylococcus aureus, streptococcal species, and anaerobic flora, Moraxella catarrhalis is primarily a respiratory tract commensal [5]. This distinction is clinically relevant because empiric regimens for suspected postoperative cervical infections often prioritize coverage of skin and oral flora, with subsequent narrowing based on culture results [4]. Identification of a respiratory commensal in a deep surgical site should prompt consideration of host factors and perioperative events that may predispose to transient bacteremia, particularly in patients with chronic pulmonary disease or immunosuppression.
The emergence of M. catarrhalis as a causative agent in a post-ACDF ACA is unprecedented, highlighting the evolving microbial landscape in the context of spinal surgery infectious complications. We have identified reports of spinal infections attributed to Moraxella, although none occurred in the context of cervical spine surgery, and none described prevertebral or anterior cervical abscess formation following ACDF. To contextualize the novelty of this case, we performed a focused narrative review of the published literature on spinal infections attributable to Moraxella catarrhalis. All cases of M. catarrhalis spinal infection meeting inclusion criteria are documented in Table 1.
A review of the published literature identified four non-retracted reports of spinal infection attributable to Moraxella catarrhalis. These comprised two cases of vertebral osteomyelitis (Prallet et al.; Mousa et al.), one case of concomitant discitis and bacteremia (Brunckhorst et al.), and one case of vertebral osteomyelitis associated with infective endocarditis (Maierean et al.). All reported cases were attributed to hematogenous seeding, most frequently in medically vulnerable hosts with chronic respiratory disease or immunosuppression. None occurred in the context of cervical spine surgery, and none described prevertebral or anterior cervical abscess formation. To our knowledge, no previous postoperative spinal infections attributable to Moraxella catarrhalis have been reported.
3.2. Mechanism of Infection
Given that patients with chronic obstructive pulmonary disease (COPD) are frequently colonized with Moraxella catarrhalis and are predisposed to transient bacteremia, hematogenous dissemination represents a compelling explanation for the present case [15,16,17]. However, the localized prevertebral distribution of the infection, its delayed postoperative onset, and the organism’s origin as an upper airway commensal also make airway instrumentation with transient mucosal microtrauma a plausible contributory mechanism [5]. It is therefore likely that a combination of heavy airway colonization and perioperative vulnerability facilitated pathogen entry, culminating in the first described anterior cervical abscess following ACDF caused by M. catarrhalis.
Additional microbiological findings further support a hematogenous rather than iatrogenic mechanism of infection. Preoperative nasal screening for methicillin-resistant Staphylococcus aureus (MRSA) was negative, and intraoperative swabs obtained from the skin and suprafascial layers at the time of surgical washout demonstrated no microbial growth. In addition, prolonged culture of deep neck wound specimens showed no growth of Actinomyces species after two weeks of incubation, arguing against preexisting colonization, superficial wound contamination, or a chronic cervicofacial or contiguous oropharyngeal source of infection. In contrast, the causative organism isolated from the deep surgical site is a recognized respiratory tract commensal, supporting transient bacteremia as the most likely mechanism of dissemination, despite the absence of identifiable aerodigestive tract injury. Importantly, transient bacteremia may resolve rapidly, meaning that negative blood cultures at re-presentation do not exclude a hematogenous source.
These observations are consistent with previous reports suggesting that M. catarrhalis may act as an opportunistic pathogen in vulnerable hosts [11,12,13,14]. Maierean et al. described a patient with COPD who developed vertebral osteomyelitis attributed to M. catarrhalis, presumed to have arisen via hematogenous spread, albeit in a non-postoperative setting [11]. Given the vulnerable local anatomy involved in anterior cervical spinal surgery, this pathogenic mechanism may pose an even greater risk for infectious complications in patients with similar respiratory and immunological risk profiles.
Taken together, these findings support the concept that M. catarrhalis may act as an opportunistic pathogen when host defenses are impaired, even in the absence of overt mucosal disruption.
3.3. Perioperative Considerations in High-Risk Patients
Patients receiving long-term corticosteroid therapy or those with chronic respiratory disease represent a higher-risk subgroup for postoperative infection following ACDF [1,4]. Preoperative optimization should include careful respiratory assessment, smoking cessation counseling, and multidisciplinary perioperative planning involving anesthesia, infectious diseases, and respiratory medicine [8]. Although routine extended postoperative antibiotic prophylaxis is not currently recommended following clean spinal surgery [18,19,20], heightened vigilance is warranted in immunosuppressed patients. In such cases, early postoperative review, a low threshold for imaging in the presence of dysphagia or neck symptoms, and prompt culture-directed antimicrobial therapy are essential. At present, evidence does not support routine prolonged prophylactic antibiotics solely based on corticosteroid use; however, individualized risk assessment is advised [4,21]. These considerations may be particularly relevant as ACDF is increasingly performed in older patients with complex medical comorbidities.
3.4. Timelines for Infection
The rate of occurrence of postoperative infections following ACDF is cited as 0.07% (range 0–0.39%) [22], indicating that ACDF is associated with a low overall risk of postoperative infection. Among these, ACAs are uncommon complications. Risk is increased in medically vulnerable patients and in the setting of instrumentation; longer operative time is also associated with increased adverse events after ACDF [21,23,24]. In the case of our patient, his key risk factors for infection included his steroid-controlled COPD, resulting in reduced immune capacity, as well as the COPD itself, with point prevalence studies indicating that 5 to 32% of adults with COPD are colonized with M. catarrhalis at any given time, making it a particularly common commensal bacteria in this demographic [15,16,17].
Most postoperative infections occur in the early postoperative period; however, delayed deep infections have been reported months to years after ACDF [2,25,26]. Postoperative infection may result from intraoperative inoculation, hematogenous seeding, or less commonly, contiguous spread from adjacent structures [5,23]. We postulate that given the lack of intraoperative damage to the aerodigestive viscera, the development of our patient’s ACA can be attributed to an M. catarrhalis bacteremia present at the time of surgery, made likely by his aforementioned pulmonary risk factors. This temporal pattern is consistent with early hematogenous seeding rather than delayed contiguous spread.
Delayed presentations (>6 months) warrant careful evaluation for occult aerodigestive pathology or delayed esophageal perforation in the context of anterior cervical instrumentation. Christiano et al. reported a prevertebral abscess presenting with acute dysphagia 2 years after ACDF without an identifiable mucosal breach at exploration [26]. Similarly, Jin et al. described infection presenting with dysphagia 20 years after ACDF, again without clear predisposing features at the index procedure [25]. In our patient, intubation was difficult (Mallampati class III), and although no visceral injury was identified intraoperatively, minor mucosal microtrauma cannot be excluded. Nevertheless, the overall findings support a hematogenous route as the most likely mechanism of bacterial translocation.
3.5. Treatment Strategy and Outcomes
Understanding the pathogenesis in our patient allows us to contextualize current best practices in the management of anterior cervical abscesses following ACDF. Management of ACAs following ACDF typically involves a combination of surgical treatment and systemic antibiotic therapy. Recent multicenter experience with minimally invasive surgical management of cervical spondylodiscitis further supports the importance of early source control and multidisciplinary decision-making in deep cervical infections, with surgical strategy tailored to anatomy, stability, and patient comorbidity [27]. Following surgical intervention, patients are usually initiated on empirical broad-spectrum IV antibiotics, such as Vancomycin for MRSA cover in combination with a 3rd generation Cephalosporin such as Ceftriaxone or Cefepime to cover Gram-negative pathogens [19,21,24]. Once culture and sensitivity results are available, antibiotic therapy should be narrowed accordingly. Our case suggests these principles may still be applied, though vigilance is needed when culture reveals atypical pathogens.
A defining microbiological characteristic of M. catarrhalis is its ability to produce BRO-type beta-lactamases, which confer resistance to penicillin and amoxicillin in the majority of clinical isolates [5,28]. This resistance profile necessitates careful antimicrobial selection and highlights the importance of culture-directed therapy in invasive infections. Agents such as third-generation cephalosporins, macrolides, fluoroquinolones, and trimethoprim–sulfamethoxazole generally retain activity against this organism, though resistance patterns may vary regionally [5,28].
The typical duration of antibiotic therapy for deep postoperative spinal infections ranges from 6 to 8 weeks, beginning with IV administration and, in cases with good clinical and laboratory response, transitioning to an oral step-down regimen [19,20]. Monitoring of CRP and ESR is essential during therapy to guide response and duration [21]. In selected patients with effective source control and favorable clinical and laboratory response, an early transition to oral therapy may be appropriate, although regimens and duration should be individualized in conjunction with infectious diseases specialists [19,21,24]. Prolonged therapy and close follow-up are particularly important in the setting of spinal instrumentation [29], where incomplete treatment may increase the risk of recurrence or persistent infection [23,30].
In this case, prompt surgical source control combined with prolonged culture-directed antimicrobial therapy resulted in complete clinical and radiological resolution without recurrence.
3.6. Antibiotic Management of Atypical Pathogens
Antibiotic therapy remains the cornerstone of treatment for invasive deep surgical site infections, including those attributable to Moraxella catarrhalis. Antimicrobial management should be guided by culture and susceptibility results whenever possible. In a previously reported case of vertebral osteomyelitis caused by M. catarrhalis, initial treatment with intravenous ceftriaxone followed by oral doxycycline was effective [11]. In general, antibiotic therapy for spinal infections is administered over several weeks, with duration and regimen adjusted according to clinical response and inflammatory markers [19,20,21]. In the postoperative setting, surgical debridement combined with prolonged antimicrobial therapy remains the mainstay of management [24], particularly in the presence of compressive symptoms, neurological deficit, or failure of conservative treatment [19,21,24].
The emergence of M. catarrhalis in invasive spinal infections also necessitates consideration of its characteristic antimicrobial resistance patterns. Most clinical isolates produce beta-lactamases, which may confer resistance to penicillin and amoxicillin [5,28]. In the present case, empirical antibiotic therapy was initiated promptly and subsequently refined based on microbiological sensitivities, underscoring the importance of culture-directed treatment in atypical postoperative infections.
3.7. Implications for Airway Management and Surgical Protocols
Given the widespread use of ACDF and continued advances in spinal instrumentation and perioperative care [1], clinicians must remain vigilant for rare and atypical pathogens that may be introduced through respiratory manipulation, such as endotracheal intubation. This is particularly relevant when patients present with unexpected organisms or delayed postoperative symptoms. Early multidisciplinary involvement, including consultation with infectious diseases specialists and meticulous microbiological evaluation, is critical to optimizing outcomes in these unconventional presentations [19,21,24]. These considerations should be integrated with patient-specific risk stratification, particularly in populations known to be at increased risk of postoperative infection [4,21,24].
In the present case, dynamic barium swallow studies demonstrated no evidence of esophageal or tracheal injury and no fistulous communication, making direct iatrogenic contamination of the surgical site unlikely and supporting a hematogenous mechanism of infection. This interpretation is reinforced by the absence of superficial wound contamination and negative cultures from the skin and suprafascial layers.
This mechanism is particularly plausible in the context of this patient’s multiple risk factors for transient bacteremia, including chronic obstructive pulmonary disease, long-term oral corticosteroid use, active smoking, reduced cervical mobility due to degenerative cervical myelopathy, and upper airway manipulation during intubation. Although M. catarrhalis is rarely reported as a cause of postoperative spinal infection, existing reports of invasive disease most commonly support hematogenous seeding in medically vulnerable hosts [11,12,13,14]. In the perioperative setting, transient mucosal microtrauma related to airway instrumentation may plausibly facilitate bacteremia, although this mechanism is difficult to confirm in individual cases.
Overall, this case reinforces the need for heightened postoperative surveillance in high-risk spinal surgery patients and consideration of respiratory tract commensals as potential causative pathogens. Importantly, negative blood cultures at the time of clinical re-presentation do not exclude a transient perioperative bacteremia, as bacteremia may have resolved or been suppressed by prior antimicrobial exposure, limiting diagnostic yield.
As ACDF continues to be widely performed, clinicians should remain alert to rare but clinically significant postoperative complications [1]. The identification of Moraxella catarrhalis as the causative organism in an anterior cervical abscess following ACDF expands the recognized spectrum of postoperative spinal pathogens and highlights the importance of comprehensive microbiological evaluation and tailored antimicrobial therapy [19,21,24]. In patients with pulmonary comorbidities, particularly COPD and chronic corticosteroid exposure, respiratory tract organisms such as M. catarrhalis may warrant increased consideration in the differential diagnosis of postoperative deep cervical infection [5,15,16,17].
Given the limited number of reported cases, specific management guidelines for postoperative spinal infection caused by M. catarrhalis are lacking. Accordingly, treatment should follow established principles for deep postoperative spinal infection, including timely surgical source control when indicated and antimicrobial therapy tailored to susceptibility results [11,12,13,14,19,21,24]. Careful evaluation for aerodigestive injury remains essential in patients presenting with postoperative dysphagia, and adjunctive intraoperative tools, such as ultrasound, may assist in confirming adequate surgical washout in selected cases. Finally, this case highlights the value of early multidisciplinary collaboration between spine surgery, otolaryngology, and infectious diseases in optimizing outcomes for complex postoperative infections [19,21,24].
4. Conclusions
Anterior cervical abscess formation following anterior cervical discectomy and fusion is rare, but when it occurs, it carries significant morbidity and requires prompt recognition and management. This case demonstrates that postoperative deep cervical infection may arise from atypical organisms not traditionally associated with spinal surgery, including respiratory tract commensals such as Moraxella catarrhalis.
The identification of this pathogen in a prevertebral abscess following ACDF highlights the importance of maintaining diagnostic vigilance in medically vulnerable patients, particularly those with chronic pulmonary disease, smoking history, or long-term corticosteroid exposure. In such individuals, early postoperative symptoms such as dysphagia or neck discomfort should prompt a low threshold for advanced imaging, even in the absence of marked laboratory abnormalities.
Effective management relies on timely surgical source control, thorough microbiological evaluation, and tailored antimicrobial therapy based on susceptibility testing. This case expands the spectrum of recognized pathogens in postoperative cervical spine infection and underscores the need for individualized, multidisciplinary care when managing uncommon but clinically significant complications of ACDF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yee T.J. Swong K. Park P. Complications of anterior cervical spine surgery: A systematic review of the literature J. Spine Surg.2020630232210.21037/jss.2020.01.1432309668 PMC 7154369 · doi ↗ · pubmed ↗
- 2Chen Y.-C. Zhang L. Li E.-N. Ding L.-X. Zhang G.-A. Hou Y. Yuan W. Late deep cervical infection after anterior cervical discectomy and fusion: A case report and literature review BMC Musculoskelet. Disord.20192043710.1186/s 12891-019-2783-x 31554516 PMC 6761726 · doi ↗ · pubmed ↗
- 3Wang H. Wang L. Yang Y. Lu F. Ma X. Xia X. Jiang J. Enterobacter cloacae infection after anterior cervical decompression and fusion: Case study and literature review Int. J. Clin. Exp. Med.201583438 Available online: https://pmc.ncbi.nlm.nih.gov/articles/PMC 4443068/(accessed on 2 June 2025)26064234 PMC 4443068 · pubmed ↗
- 4Tsantes A.G. Papadopoulos D.V. Vrioni G. Sioutis S. Sapkas G. Benzakour A. Benzakour T. Angelini A. Ruggieri P. Mavrogenis A.F. Spinal Infections: An Update Microorganisms 2020847610.3390/microorganisms 804047632230730 PMC 7232330 · doi ↗ · pubmed ↗
- 5Verduin C.M. Hol C. Fleer A. Van Dijk H. Van Belkum A. Moraxella catarrhalis: From emerging to established pathogen Clin. Microbiol. Rev.20021512514410.1128/cmr.15.1.125-144.200211781271 PMC 118065 · doi ↗ · pubmed ↗
- 6Martin A.R. Jentzsch T. Wilson J.R. Moghaddamjou A. Jiang F. Rienmueller A. Badhiwala J.H. Akbar M.A. Nater A. Oitment C. Inter-rater Reliability of the Modified Japanese Orthopedic Association Score in Degenerative Cervical Myelopathy: A Cross-sectional Study Spine 2021461063106910.1097/BRS.000000000000395633492085 · doi ↗ · pubmed ↗
- 7Kato S. Ganau M. Fehlings M.G. Surgical decision-making in degenerative cervical myelopathy—Anterior versus posterior approach J. Clin. Neurosci.20185871210.1016/J.JOCN.2018.08.04630279123 · doi ↗ · pubmed ↗
- 8Zaed I. Bossi B. Ganau M. Tinterri B. Giordano M. Chibbaro S. Current state of benefits of Enhanced Recovery After Surgery (ERAS) in spinal surgeries: A systematic review of the literature Neurochirurgie 202268616810.1016/j.neuchi.2021.04.00733901525 · doi ↗ · pubmed ↗