Anemia as a Potent and Underrecognized Driver of Venous Thromboembolism: A Systematic Review
Ghaith K. Mansour, Walaa A. Alshahrani, Lama Alfehaid, Abdulmajeed M. Alshehri, Majed S. Al Yami

TL;DR
This paper reviews evidence showing that anemia, especially iron-deficiency anemia, is linked to increased venous thromboembolism risk and worse outcomes.
Contribution
The study is the first systematic review to synthesize clinical and genetic evidence linking nutritional deficiency anemia to venous thromboembolism.
Findings
Anemia is consistently associated with adverse venous thromboembolism outcomes across multiple study designs.
Iron-deficiency anemia increases the odds of venous thromboembolism in population-based data.
Mendelian randomization suggests a potential causal link between anemia traits and thrombosis at unusual anatomical sites.
Abstract
Background: Nutritional deficiency anemias—including iron, vitamin B12, and folate deficiencies—are common worldwide and are increasingly recognized as potential contributors to venous thromboembolism (VTE). Mechanistic and epidemiologic data suggest that anemia may promote thrombosis through hypoxia, endothelial activation, reactive thrombocytosis, and hyperhomocysteinemia. However, a focused synthesis of clinical and genetic evidence specifically linking nutritional deficiency anemia to VTE has been lacking. Methods: We conducted a systematic search of PubMed and the Cochrane Library from inception to 30 September 2025 to identify studies assessing nutritional deficiency anemia in relation to VTE outcomes. Eligible studies included observational designs, case reports, case series, and Mendelian randomization (MR) analyses. Quality assessment followed the Newcastle–Ottawa Scale (NOS),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
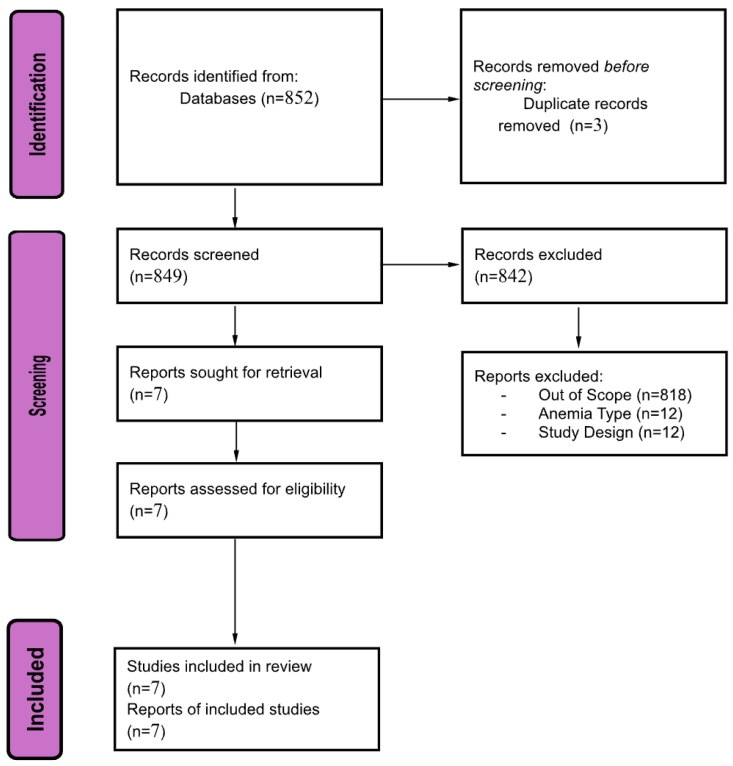 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFolate and B Vitamins Research · Iron Metabolism and Disorders · Venous Thromboembolism Diagnosis and Management
1. Introduction
Anemia remains one of the most significant global health burdens, affecting an estimated 1.92 billion individuals worldwide and contributing substantially to morbidity, impaired functional capacity, and adverse clinical outcomes [1]. Nutritional deficiency anemias—including iron-deficiency anemia (IDA), vitamin B12-deficiency anemia, and folate-deficiency anemia—constitute the predominant etiologies, with IDA alone accounting for more than two-thirds of all anemia cases and disproportionately affecting women and younger populations [1,2]. These conditions result in reduced hemoglobin concentration and diminished oxygen-carrying capacity, triggering compensatory physiological responses such as increased cardiac output, systemic hypoxia, heightened oxidative stress, and reactive thrombocytosis [3]. Such alterations establish a biologically plausible foundation for a prothrombotic state.
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), is the third most common cardiovascular disorder globally, with an incidence ranging from 100 to 200 per 100,000 individuals annually and substantial rates of recurrence, disability, and mortality [4]. The classical risk factors for VTE—immobilization, malignancy, hormonal therapy, surgery, and inherited thrombophilia—do not fully explain the burden observed in clinical practice. Emerging evidence suggests that nutritional deficiency anemia may serve as an overlooked modifier of VTE risk, supported by epidemiologic, mechanistic, and preliminary genetic data [5,6,7,8,9,10,11,12].
IDA has been linked to hypercoagulability through several distinct mechanisms, including reactive thrombocytosis, platelet hyper-reactivity, increased blood viscosity due to microcytosis, endothelial dysfunction caused by chronic tissue hypoxia, and reduced antioxidant defenses leading to increased oxidative stress and platelet activation [5,6]. Additionally, iron deficiency has been associated with elevated factor VIII levels, which represent a robust and well-established risk factor for thrombosis [7]. Vitamin B12 and folate deficiencies further amplify thrombotic potential by inducing hyperhomocysteinemia, which promotes endothelial injury, increases expression of tissue factor, and disrupts the protein C-mediated anticoagulant pathway [8,9]. Collectively, these mechanisms suggest that nutritional deficiency anemia may contribute to thrombogenesis through multiple converging pathways.
Clinical and epidemiologic studies have increasingly supported this association. Large population-based analyses have demonstrated that individuals with anemia exhibit higher rates of VTE, including DVT and PE, compared with non-anemic populations, even after adjustment for comorbidities and traditional risk factors [10,11]. In particular, IDA has been linked to increased odds of both provoked and unprovoked VTE, and several clinical series have reported VTE events in otherwise healthy young adults presenting with moderate to severe IDA [12]. The presence of anemia in patients with established VTE has also been associated with increased mortality, higher bleeding risk, and worse long-term outcomes [13]. Moreover, recent Mendelian randomization studies provide preliminary genetic-level support for a potential causal relationship between anemia-related traits and thrombotic risk [14].
Despite these important observations, the evidence remains fragmented across heterogeneous study designs, patient populations, and anemia subtypes. No prior systematic review has comprehensively synthesized the association between nutritional deficiency anemia—including iron, vitamin B12, and folate deficiency—and the risk of VTE across observational, descriptive, and genetic studies. Clarifying this relationship is essential for improving risk stratification, refining VTE prediction models, and informing screening and prevention strategies in anemic patients. The present systematic review aims to address this critical gap by evaluating the association between nutritional deficiency anemia and VTE across the totality of available evidence, integrating findings from cohort, case–control, case-based, and genetic studies.
2. Materials and Methods
2.1. Search Strategy, Study Selection, and Data Extraction
A systematic search was conducted in PubMed and the Cochrane Library to identify studies evaluating the association between iron-deficiency anemia, vitamin B12 deficiency anemia, and folate-deficiency anemia with venous thromboembolism (VTE). The PubMed search strategy combined the terms: (“Anemia” [Mesh] OR “Iron-Deficiency Anemia” [Mesh] OR “Anemia, Vitamin B 12 Deficiency” [Mesh] OR “Folic Acid Deficiency” [Mesh]) AND (“Venous Thromboembolism” [Mesh] OR “Pulmonary Embolism” [Mesh] OR “Deep Vein Thrombosis” [Mesh] OR “Venous Thrombosis” [Mesh]). A similar conceptual strategy was applied to the Cochrane Library using equivalent free-text keywords. The electronic search included all English-language records published from inception to 30 September 2025, consistent with the search settings used by the investigator. Eligible studies included adult participants (≥18 years) and reported an association between nutritional deficiency anemia and VTE outcomes (PE, DVT, or composite VTE). Observational designs were included—prospective or retrospective cohort studies, registry-based analyses, and descriptive studies such as case–control and case series. We excluded secondary evidence (systematic reviews, meta-analyses, or guidelines), non-eligible designs (animal studies, conference abstracts), studies outside the scope (pediatric populations, non-nutritional anemia types such as hemolytic disorders, or lacking VTE outcomes), and studies in non-English languages.
2.2. Quality Assessment and Risk of Bias
The methodological quality and risk of bias of the included studies were assessed according to the design-specific, internationally accepted appraisal tools. Observational analytical studies (cohort and case–control) were evaluated using the Newcastle–Ottawa Scale (NOS), which assesses three domains: Selection (0–4 stars), Comparability (0–2 stars), and Outcome (0–3 stars), with a maximum score of 9. Based on established criteria, studies scoring 7–9 stars were classified as high quality, 5–6 stars as moderate quality, and ≤4 stars as low quality. Four studies in this review [15,16,17,18] were eligible for NOS assessment, all demonstrating good to high methodological quality [19].
Studies that were not eligible for NOS due to their descriptive or non-comparative design were appraised using the appropriate validated tools. The case report [18] and case series [20] were assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklists for Case Reports and Case Series, respectively. These tools evaluate clarity of clinical presentation, diagnostic accuracy, completeness of patient information, intervention detail, and outcome reporting. Based on JBI criteria, the case report demonstrated moderate quality, while the case series demonstrated low to moderate quality due to limited sample size and lack of consecutive recruitment [21].
The Mendelian randomization study [22] was evaluated using the Risk of Bias in Mendelian Randomization Studies (ROB-MR) tool, which examines instrument strength, independence from confounders, absence of horizontal pleiotropy, heterogeneity, and robustness of sensitivity analyses. This study demonstrated a low risk of bias, supported by strong genetic instruments and multiple sensitivity analyses (MR-Egger, weighted median, MR-PRESSO) [23].
All assessments were conducted independently by two reviewers, and any discrepancies were resolved through discussion and consensus. No study was excluded on the basis of methodological quality alone, and the interpretation of results accounted for the inherent strengths and limitations of each study design. A comprehensive summary of all risk-of-bias evaluations and quality ratings is presented in Table 1. The study was conducted according to PRISMA guidelines and registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD420251235479. The PRISMA Checklist is in the Supplementary Material (Table S1).
2.3. Data Synthesis and Analysis
A meta-analysis was not feasible due to substantial heterogeneity across the included studies. The designs (cohort, case–control, randomized trial substudy, Mendelian randomization, case series, and case report), populations, definitions of nutritional deficiency anemia, VTE outcome measures, and follow-up durations varied widely. Because of these differences, the effect estimates (HRs, RRs, ORs, and adjusted measures) were extracted and presented exactly as reported in the original publications, without statistical transformation or standardization.
A structured narrative synthesis was therefore conducted following PRISMA 2020 guidelines. Analytical studies were summarized based on effect direction and magnitude, whereas case-based studies were synthesized descriptively to identify recurrent clinical patterns without inferring causality. The Mendelian randomization study was evaluated separately, given its distinct genetic instrumental-variable approach. Importantly, none of the included studies shared overlapping patient cohorts or utilized the same datasets, ensuring independence of results. No subgroup or sensitivity analyses were performed due to the limited number and heterogeneity of studies.
3. Results
3.1. Search Results and Study Characteristics
A total of 852 records were identified through the database search. After the removal of 3 duplicate records, 849 records proceeded to title and abstract screening. Of these, 842 records were excluded for not meeting the eligibility criteria. The remaining 7 reports were retrieved for full-text assessment, all of which met the inclusion criteria. Ultimately, seven studies were included in the systematic review, as shown in (Figure 1). The systematic search identified seven eligible studies examining the association between anemia and venous thromboembolism (VTE). These included four observational analytical studies (three cohort studies and one case–control study), one Mendelian randomization study, one case series, and one case report. The observational studies varied in sample size, ranging from 764 to over 3000 patients, while the genetic study included multiple large-scale GWAS datasets. Two descriptive clinical reports described individual or paired cases of IDA-associated DVT or PE. Across studies, anemia definitions varied (hemoglobin thresholds or ICD coding), and outcomes included mortality, symptomatic VTE, recurrent VTE, major bleeding, or site-specific thrombotic events. It is important to note that the authors defined anemia based on hemoglobin level only without investigating its underlying etiology. This could explain that nutritional deficiency anemia has no direct association with causing VTE.
Follow-up periods ranged from 77 days to over three years, as shown in Table 2. The methodological quality of the included studies was generally acceptable across designs, as summarized in Table 2.
3.2. Summary of the Included Studies
Jiménez 2009 et al. conducted a prospective cohort study of 764 patients with acute pulmonary embolism and found that lower hemoglobin levels were significantly associated with worse short-term outcomes. Patients in the lowest hemoglobin quartile had a markedly reduced 3-month survival rate of 75% compared with 86–91% in higher quartiles. Each 1 g/dL decrease in hemoglobin increased the risk of all-cause mortality by 16% (HR 1.16, 95% CI 1.05–1.28), and anemia was also linked to a higher unadjusted risk of fatal PE [15].
Hung 2015 et al. conducted a nationwide population-based case–control study including 2522 VTE cases and 12,610 controls. Prior iron-deficiency anemia was independently associated with a 43% higher odds of developing VTE (adjusted OR 1.43, 95% CI 1.10–1.87). IDA was also specifically associated with deep-vein thrombosis (OR 1.43, 95% CI 1.08–1.90), although no significant relationship was observed with isolated pulmonary embolism [16].
Chi 2018 et al. conducted a secondary analysis of the APEX trial including 6861 acutely ill hospitalized patients and found that low baseline hemoglobin significantly increased the risk of symptomatic VTE despite prophylaxis. Low hemoglobin was associated with higher rates of total symptomatic VTE (RR 1.94, 95% CI 1.27–2.98), DVT (RR 2.29, 95% CI 1.12–4.68), and non-fatal PE (RR 2.63, 95% CI 1.22–5.65). After adjustment, anemia remained an independent predictor of VTE (adjusted OR 1.71, 95% CI 1.09–2.69) [11].
Yamashita 2019 et al. conducted a multicenter prospective cohort study of 3012 VTE patients and demonstrated that baseline anemia was strongly associated with long-term bleeding and mortality outcomes. Moderate/severe anemia significantly increased the risk of major bleeding (HR 1.91, 95% CI 1.42–2.58) and all-cause mortality (HR 2.89, 95% CI 2.45–3.42), while mild anemia also increased bleeding risk (HR 1.41, 95% CI 1.00–1.98). Anemia was not associated with recurrent VTE (HR 1.05, 95% CI 0.76–1.45) [17].
Ezeh 2021 et al. described a 72-year-old woman with severe iron-deficiency anemia who developed recurrent bilateral PE and DVT. Management with blood transfusion, iron supplementation, and anticoagulation stabilized her hemoglobin, after which no further thromboembolic events occurred, highlighting severe IDA as a possible driver of recurrent VTE [18].
Yadav 2023 et al. reported two young adults with moderate iron-deficiency anemia who presented with unprovoked lower-limb DVT. Both exhibited reactive thrombocytosis and lacked alternative provoking factors. Correction of anemia along with anticoagulation led to clinical improvement, suggesting that IDA may contribute to unprovoked DVT even in low-risk individuals [24].
Yu 2025 et al. applied a two-sample Mendelian randomization approach using large GWAS datasets and found a potential causal relationship between anemia and thrombosis. Genetic predisposition to anemia increased the risk of thrombosis in unusual anatomical sites (OR 1.446, 95% CI 1.104–1.895), while aplastic anemia showed a mild association with overall VTE (OR 1.065, 95% CI 1.003–1.131). No strong causal effect was detected for classic DVT or PE [20].
3.3. Outcomes
Across all included studies, anemia was consistently associated with adverse thrombotic or clinical outcomes, although the magnitude and nature of risk varied by study design. Nevertheless, study design, patient groups, and anemia classifications demonstrated significant variation across these cohorts, reflecting the importance of interpreting these findings with caution. Observational studies demonstrated that anemia predicted higher short-term mortality in acute PE (HR 1.16 per 1 g/dL decrease), greater risk of symptomatic VTE in hospitalized medically ill patients (RR 1.94), and increased risk of long-term major bleeding and mortality in established VTE cohorts (HRs 1.41–2.89). IDA specifically increased the odds of VTE in population-level data (OR 1.43) and was linked to unprovoked DVT in young individuals in descriptive reports. Genetic evidence supported a potential causal relationship between anemia and thrombosis, particularly in unusual sites (OR 1.446). All clinical outcomes from the included studies are shown in Table 3.
4. Discussion
This systematic review provides comprehensive evidence linking nutritional deficiency anemia—including iron-deficiency anemia, vitamin B12 deficiency, and folate-deficiency anemia—to an increased risk of venous thromboembolism (VTE). However, only one study clearly demonstrates an independent effect of iron deficiency on the risk of VTE [16]. In several other key studies, the specific type or etiology of anemia was not further defined [11,15,17,24]. Furthermore, one study analyzed genetic risk profiles for a broad spectrum of anemias, including non-nutritional forms such as hereditary hemolytic anemia and aplastic anemia [20]. Vitamin B12 and folate-deficiency anemias may contribute to thrombogenesis through hyperhomocysteinemia-mediated endothelial injury and disruption of anticoagulant pathways [8,9]. Iron deficiency promotes reactive thrombocytosis and platelet hyper-reactivity, increases platelet activation markers, and elevates factor VIII levels—an established VTE risk factor [7]. Microcytosis in IDA may impair blood flow and contribute to venous stasis, while chronic hypoxia amplifies endothelial dysfunction and oxidative stress, resulting in a hypercoagulable state [6]. Consistently, deficiencies in vitamin B12 and folate elevate homocysteine levels, leading to endothelial activation, tissue-factor expression, and reduced protein C activity [8,9]. These mechanisms strongly reinforce the epidemiologic associations observed in clinical studies.
Our findings align with broader epidemiologic evidence. The Swedish–Danish blood donor cohort demonstrated that individuals with subnormal hemoglobin experienced up to a two-fold increase in VTE risk after adjustment for confounders [10]. Similarly, the GARFIELD-VTE registry showed that anemic VTE patients had significantly higher long-term mortality and major bleeding risk compared with non-anemic patients, underscoring the prognostic significance of anemia in thrombosis [13]. Additionally, preliminary genetic evidence from Mendelian randomization suggests a potential causal effect of anemia-related traits on thrombotic susceptibility [20]. Clinically, these findings highlight anemia as an underrecognized VTE risk modifier. Routine assessment of hemoglobin, ferritin, vitamin B12, and folate levels may help identify individuals at increased thrombotic risk. Correction of nutritional anemia could represent a modifiable therapeutic target, although prospective trials are required to confirm benefit. Importantly, widely used VTE risk-assessment models currently omit anemia-related variables, despite increasing evidence supporting their relevance [11,25].
This review has notable strengths. It is the first to synthesize evidence specifically on nutritional deficiency anemia and VTE across observational, descriptive, and genetic methodologies. Use of validated appraisal tools (NOS, JBI, ROB-MR) enhances confidence in study quality. Integrating mechanistic and genetic research provides a multidimensional understanding of the anemia–VTE connection. However, several limitations must be acknowledged. Only a limited number of high-quality analytic studies exist, with significant heterogeneity in anemia definitions and population characteristics. Observational designs are subject to confounding, and case-based evidence provides low-level support. Only one Mendelian randomization study was identified, limiting the strength of causal inference. The current evidence on nutritional deficiency anemia remains limited, particularly regarding vitamin B12- and folate-deficiency anemia. Moreover, most included studies did not account for the underlying cause of anemia or other critical risk factors for VTE, such as renal failure and cancer. Therefore, the observed association should be interpreted with caution, as anemia in many included populations may represent a surrogate marker of disease severity rather than an independent causal factor. Future research should focus on large, well-designed prospective cohorts that clearly differentiate anemia subtypes and quantify their independent contributions to VTE risk.
5. Conclusions
In conclusion, the available evidence suggests that nutritional deficiency anemia may contribute to a clinically relevant yet underappreciated determinant of venous thromboembolic risk across heterogeneous study designs. Despite the biologically plausible pathways linking anemia to prothrombotic states, the current literature remains insufficient to establish definitive causality. Accordingly, rigorously designed prospective investigations and targeted interventional studies are warranted to delineate this relationship more clearly and to determine whether integrating anemia-related parameters into existing VTE risk-assessment frameworks could enhance prognostic accuracy and clinical decision-making.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kassebaum N.J. GBD 2013 Anemia Collaborators. The global burden of anemia Hematol. Oncol. Clin. N. Am.20163024730810.1016/j.hoc.2015.11.00227040955 · doi ↗ · pubmed ↗
- 2Camaschella C. Iron-deficiency anemia N. Engl. J. Med.20153721832184310.1056/NEJ Mra 140103825946282 · doi ↗ · pubmed ↗
- 3Short M.W. Domagalski J.E. Iron deficiency anemia: Evaluation and management Am. Fam. Physician 2013879810423317073 · pubmed ↗
- 4Raskob G.E. Angchaisuksiri P. Blanco A.N. Bueller H. Gallus A. Hunt B.J. Hylek E.M. Kakkar A. Konstantinides S.V. Mc Cumber M. Thrombosis: A major contributor to global disease burden Arterioscler. Thromb. Vasc. Biol.2014342363237110.1161/ATVBAHA.114.30448825304324 · doi ↗ · pubmed ↗
- 5Franchini M. Targher G. Montagnana M. Lippi G. Iron and thrombosis Ann. Hematol.20088716717310.1007/s 00277-007-0416-118066546 PMC 2226003 · doi ↗ · pubmed ↗
- 6Al-Samkari H. Kessler C.M. Auerbach M. Recognition of thrombotic risk of thrombocytosis in iron deficiency Haematologica 202110666166310.3324/haematol.2020.27049633645945 PMC 7927881 · doi ↗ · pubmed ↗
- 7Folsom A.R. George K.M. Appiah D. Lack of association of plasma factor XI with incident stroke and coronary heart disease: The Atherosclerosis Risk in Communities (ARIC) Study Atherosclerosis 201524318118510.1016/j.atherosclerosis.2015.09.01526386215 PMC 4620543 · doi ↗ · pubmed ↗
- 8den Heijer M. Koster T. Blom H.J. Bos G.M. Briet E. Reitsma P.H. Vandenbroucke J.P. Rosendaal F.R. Hyperhomocysteinemia as a risk factor for deep-vein thrombosis N. Engl. J. Med.199633475976210.1056/NEJM 1996032133412038592549 · doi ↗ · pubmed ↗