Exploring the Role of Skull Base Anatomy in Surgical Approach Selection and Endocrinological Outcomes in Craniopharyngiomas
Alessandro Tozzi, Giorgio Fiore, Elisa Sala, Giulio Andrea Bertani, Stefano Borsa, Ilaria Carnicelli, Emanuele Ferrante, Giulia Platania, Giovanna Mantovani, Marco Locatelli

TL;DR
This study examines how skull base anatomy influences surgical approach choices and endocrinological outcomes in patients with craniopharyngiomas.
Contribution
The study introduces a quantitative method using 3D modeling to inform surgical decisions based on skull base anatomy.
Findings
Larger sphenoid sinus volumes correlate with endoscopic endonasal approach selection.
Postoperative BMI and diabetes insipidus incidence increased significantly after surgery.
Endocrinological outcomes were more influenced by tumor characteristics than surgical approach.
Abstract
Background/Objectives: Craniopharyngiomas (CPs) are rare, generally benign tumors predominantly located in the sellar and suprasellar regions, associated with significant morbidity and complex surgical management. Despite high overall survival rates, patients frequently experience complications including visual impairment, pituitary dysfunction, diabetes insipidus (DI), and hypothalamic syndrome. Among these, hypothalamic obesity (HO) represents one of the most clinically challenging sequelae, often occurring early, lacking standardized medical treatment, and leading to substantial comorbidity and reduced quality of life. This study reports a single-center experience focusing on the relationship between skull base anatomy, surgical approach selection, and endocrinological outcomes. Methods: A retrospective analysis was conducted on patients diagnosed with CPs who underwent surgery by a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
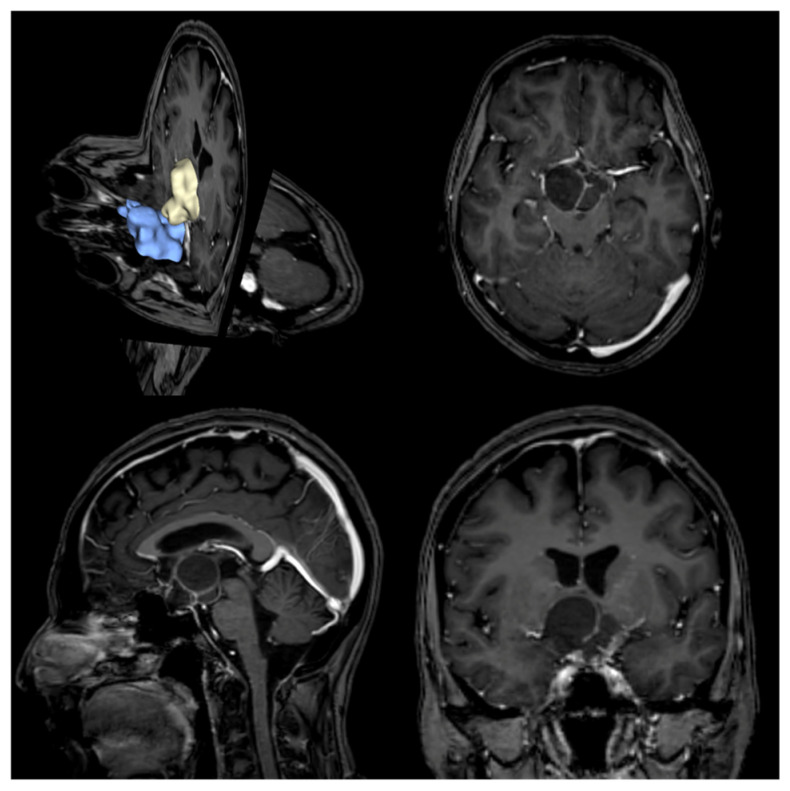 Figure 1
Figure 1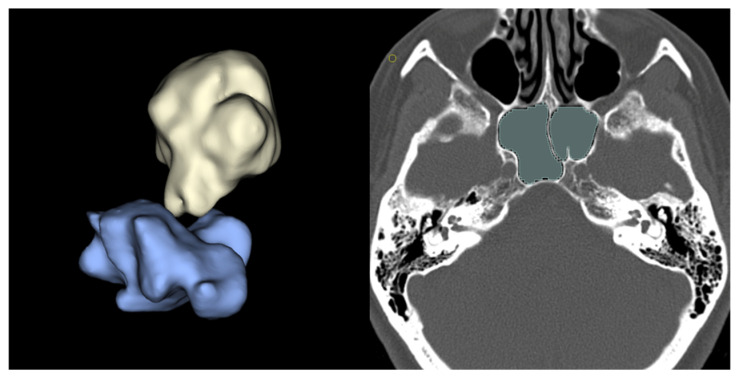 Figure 2
Figure 2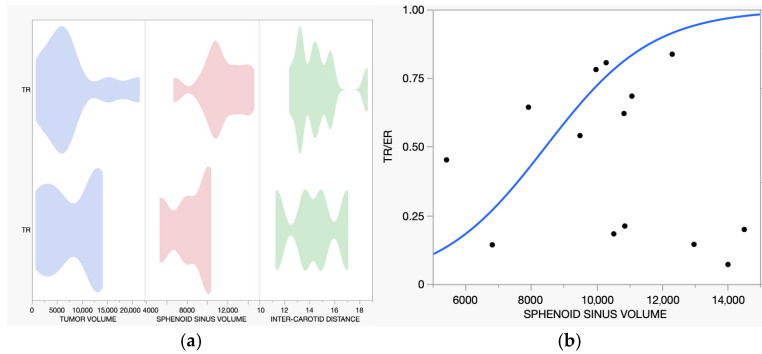 Figure 3
Figure 3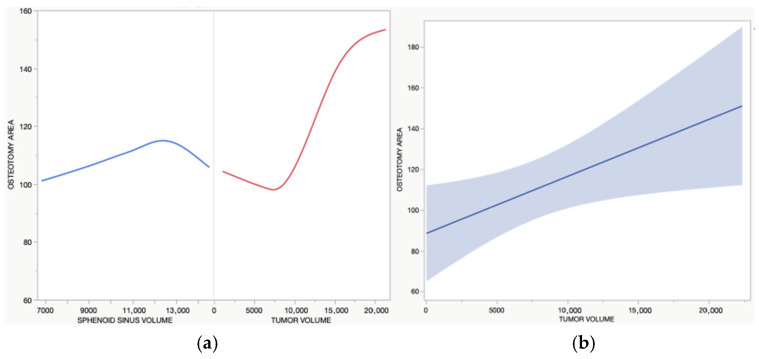 Figure 4
Figure 4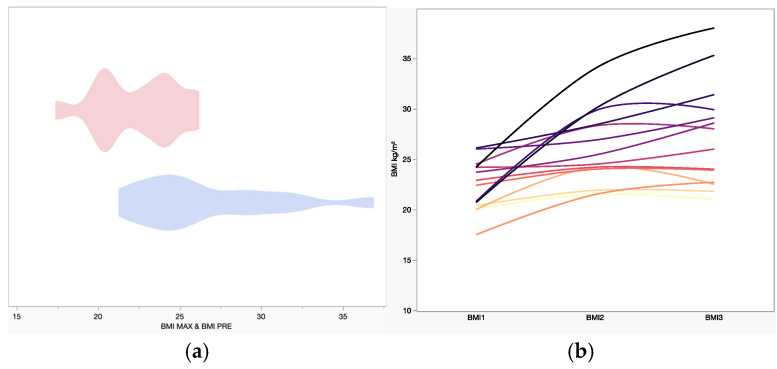 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPituitary Gland Disorders and Treatments · Head and Neck Surgical Oncology · Growth Hormone and Insulin-like Growth Factors
1. Introduction
Craniopharyngiomas (CPs) are rare, histologically benign tumors arising in the sellar and suprasellar regions, typically involving three regions of the hypothalamic-pituitary axis: the tuber cinereum, pituitary stalk, and pituitary gland [1,2]. Their incidence exhibits a bimodal distribution, with peaks in children and adults [1,2,3]. Histologically, CPs are classified into two main subtypes: adamantinomatous and papillary [3,4]. Surgical resection remains the treatment of choice, with reported 20-year overall survival rates of 87–95% in mixed adult and pediatric cohorts [5,6].
Despite their benign nature, CPs are associated with substantial recurrence rates and poor postoperative quality of life (QoL) [2,7], making them a clinical challenge [2,8]. Recent studies have focused on identifying preoperative predictors and intraoperative factors associated with reduced endocrinological and neurological morbidity, such as visual impairment, pituitary dysfunction, diabetes insipidus (DI), and hypothalamic obesity (HO) [2,3,9,10]. Key determinants of the extent of resection, recurrence risk, and postoperative hypothalamic dysfunction include tumor size and its relationship to the hypothalamus, whereas the surgical approach itself appears to play a more limited role [2,3,9,10].
Traditionally, CPs have been managed through transcranial routes (TRs). However, with the widespread adoption of endoscopic techniques, endoscopic transnasal resection (ER) has become increasingly utilized, with endoscopy in skull base surgery contributing to better outcomes [11,12]. This study aims to identify anatomical factors, derived from patient-specific 3D models, that may influence surgical approach selection. Additionally, we sought to explore the relationship between surgical route and long-term endocrinological outcomes.
2. Materials and Methods
2.1. Patients and Study Design
We retrospectively reviewed patients with CPs who underwent surgery at Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, University of Milan, Italy, between January 2014 and January 2024. Inclusion criteria were histological diagnosis of CPs (both papillary and adamantinomatous subtypes), availability of pre- and postoperative contrast-enhanced 3D T1-weighted MRI and preoperative volumetric CT imaging, and clinical data with a minimum follow-up of one year.
Data collected included demographic information (age and sex), clinical presentation, surgical approach, tumor histology, anatomical skull base parameters, resection outcomes, and rates of recurrence.
Given the retrospective design, the Ethics Committee waived study registration and the requirement for written informed consent for participation. Reporting followed the STROBE guidelines for cohort studies.
2.2. Data Collection
2.2.1. Surgical Approaches
Surgical resection was performed by a dedicated multidisciplinary team led by the senior author. Two main approaches were employed:
- Endoscopic resection (ER), performed via a transnasal-sphenoidal corridor using a four-hand technique, including anterior sphenoidotomy and partial posterior nasal septectomy. Extended transsphenoidal approaches were employed when needed. Tumor removal involved the use of ring curettes, surgical aspirators, and sharp dissection. The osteo-dural defect was repaired using the 3F technique [13].
- Transcranial resection (TR) through a pterional craniotomy.
The choice of approach was individualized based on detailed preoperative anatomical assessment, tumor location and extent, and surgical expertise; these selection criteria are further discussed in the Section 4.
Data on pre-resection surgical procedures, such as third ventriculostomy (IIIVCS) or external ventricular drains (EVD), were also collected.
2.2.2. Imaging Study
As a part of standard preoperative care, all patients underwent volumetric brain MRI and CT imaging for surgical planning, as follows:
- MRI imaging: Using a 3-Tesla Philips Achieva scanner (Philips Healthcare, Best, The Netherlands), 3D T1w (before and after gadolinium injection), FLAIR and T2w images were acquired.
- CT imaging: Acquired using a General Electric OPTIMA 660 scanner (GE Healthcare, Chicago, IL, USA), including a volumetric acquisition with bone window reconstruction.
Within 48 h after surgery, all patients underwent brain CT imaging to rule out surgical complications. Three months after surgery, an MRI was performed to identify residual pathology. Cases with radiologically evident residual tumor were classified as subtotal resections. Long-term follow-up included annual brain MRIs to monitor for tumor recurrence or progression. The time to progression or recurrence was measured in months from surgery date.
2.3. Outcomes
2.3.1. Volumetric Analysis
Three-dimensional models were generated from DICOM imaging data. Preoperative MR and CT scans were processed using 3D Slicer software (version 5.8.0 for macOS) Tumors (from T1-weighted MR images) and sphenoid sinuses (from bone-windowed CT scans) were manually segmented, with individual volumes calculated in cubic millimeters. Each segmentation was converted to a 3D object and exported in STL format. Segmentations were performed by an experienced neuroradiologist (G.P.). Additionally, the intercavernous carotid distance (ICD) was measured in millimeters at the narrowest point between intracavernous carotid siphons using coronal multiplanar reconstructions on MR T1w sequences (Figure 1 and Figure 2) [14]. For ER cases, the osteotomy area (in square millimeters) was approximated by simplifying the shape to a rectangle. The area was calculated using the maximum cranio-caudal and latero-lateral diameters measured on the sellar floor plane, obtained from MPR of postoperative CT scans. All measurements and 3D model segmentations were performed blinded to clinical outcomes and surgical approach.
2.3.2. Endocrinological Analysis
All clinical and metabolic follow-up was conducted by experienced neuroendocrinologists at our institution. Pituitary function was assessed both at diagnosis and after surgery. The first postoperative evaluation was scheduled for all patients one month after the surgical procedure, with subsequent hormonal assessments tailored to each patient’s specific needs. Follow-up duration was variable among patients; in general, all patients undergo lifelong surveillance, although the timing of evaluations differs on an individual basis. For the purpose of this study, postoperative data were recorded from the last available follow-up. Hypopituitarism was defined as the presence of one or more hormonal deficits. Hypoadrenalism was defined by basal cortisol level < 100 nmol/L or an abnormal response of cortisol in a dynamic test [15]. In particular, before June 2016 we considered inadequate a peak of cortisol 500 nmol/L, during 1 μg corticotrophin stimulation test (ACTH 1 mcg) or insulin tolerance test (ITT); after that time the diagnostic cut-off associated with the assay used at our institution (Roche 2) was 351 nmol/L [16,17]. A free thyroxine (fT4) under reference range in combination with not adequately increased TSH concentration was indicative of TSH deficiency [18]. Central hypogonadism was suggested in premenopausal women with low estradiol and low LH/FSH in conjunction with oligomenorrhea or amenorrhea, and in postmenopausal women in the presence of FSH levels inappropriately low for menopausal status. In men, central hypogonadism was defined by testosterone under reference range for age and normal/low LH/FSH in combination with clinical signs and symptoms [19]. Normal prolactin values were considered to be in the range of 2 to 20 mg/mL, with differences between sexes [20].
For diabetes insipidus, a urinary output > 40 ml/kg/day was considered an initial screening criterion [20]. The diagnosis was corroborated by the presence of hypernatremia and/or the requirement for desmopressin therapy. Only patients with diabetes insipidus at the time of hospital discharge were considered affected by DI in the early postoperative evaluation, whereas transient postoperative polyuria resolving before discharge was not classified as DI.
All hormonal deficits were appropriately treated with hormonal replacement therapy. BMI was calculated as body weight divided by squared height (kg/m^2^), both at diagnosis and at the last follow-up available [21]. Values of BMI ≥ 30 kg/m^2^ were considered suggestive of first-grade obesity, ≥25 and ≤29.9 kg/m^2^ suggestive of overweight [21]. Hypothalamic obesity was defined as postoperative weight gain resulting in obesity, defined by a BMI ≥ 30 kg/m^2^, documented in the medical record and occurring after surgery [22].
2.3.3. Statistical Analysis
Given the observational design, regression analyses were planned as exploratory and hypothesis-generating. Variables of interest were reported and compared as follows:
- Frequencies were reported as a percentage and compared by chi-squared and Fisher exact tests according to sample size.
- The continuous normally distributed variables were reported as mean and compared through Student’s t-test or variance analyses.
- The continuous skewed distributed variables were reported as median and compared using the Mann–Whitney U-test.
Exploratory logistic regression models were used to examine associations between radiological and anatomical features, surgical approach selection, and endocrinological outcomes. The relevant explanatory variables were chosen based on the available literature as well as the statistical significance of the univariate analysis. Statistical significance was reached for p-values less than 0.05. A ROC analysis was performed for the models, using the area under the curve (AUC) as the performance metric.
All statistical analyses were performed using JMP Pro (version 15, SAS Institute Inc., Cary, NC, USA, 1989–2023) and R studio software (version 4.2.2, R Foundation for Statistical Computing, Vienna, Austria).
3. Results
Between January 2014 and January 2024, 18 patients with CPs underwent surgical resection at our department; 14 were included in the final analysis, while 4 were excluded due to incomplete data. A summary of the patient characteristics, clinical findings, and outcomes is provided in Table 1, Table 2 and Table 3.
Female patients were slightly more prevalent (female-to-male ratio 4:3), with a median age of 43 years (range 16–67) (Table 1). The mean follow-up was 60 ± 72 months (range 12–218, Table 1). Endoscopic resections were more prevalent than transcranial approaches (2:1), with 11 cases being primary surgical interventions. Three patients underwent cyst puncture combined with the placement of a subcutaneous reservoir (Rickham) via stereotactic or endoscopic techniques (cases no. 1, 2, 12). Postoperative complications included cerebrospinal fluid (CSF) leaks in 21.3% of cases (cases 4, 8, 14) and infections in 14.29% of cases (cases 11 and 13). All patients with CSF leaks underwent dural flap reconstruction via the endoscopic route as previously described [23]. One patient (case 2) experienced postoperative hemorrhage, requiring initial external and subsequent peritoneal ventricular shunting. No deaths were reported during the follow-up period. Residual tumor was detected in three patients (21.43%) who underwent adjuvant radiosurgery (cases 4, 5, 7). Tumor recurrence occurred in one patient (case 5), who had undergone STR via the transcranial approach (Table 2).
3.1. Volumetric Study
Radiological and anatomical features are summarized in Table 2. According to the Kassam classification [24], a high prevalence of high-grade tumors was observed, with types 3a/3b representing 71.43% of cases. The mean tumor volume was 7768 mm^3^ (1047–21,345), while the mean sphenoid sinus volume was 10,509 mm^3^ (5424–14,519). The mean intercarotid distance was 14.46 mm (11.42–18.58). For the ER subgroup, the mean osteotomy area was 102.15 mm^2^ (76.48–127.59).
Linear regression analysis demonstrated that larger sphenoid sinus volumes were associated with the selection of ER (R^2^ = 0.265, p = 0.0351). The Receiver Operating Characteristic (ROC) curve demonstrated good discriminatory ability, with an area under the curve (AUC) of 0.875 (Figure 3).
Postoperative imaging demonstrated moderate inter-patient variability in the osteotomy area within the cohort, with a mean of 109.67 mm^2^ (SD = 25.58 mm^2^). Exploratory multivariate linear regression identified tumor volume as the only variable significantly associated with the osteotomy area (R^2^ = 0.465, p = 0.0297). Larger tumors required larger osteotomies, independent of other factors such as Kassam grade, sphenoid sinus volume, intercarotid distance, age, or hypothalamic invasion (Figure 4).
3.2. Endocrinological Outcome
Diabetes insipidus was observed more frequently after surgery (Table 3, p = 0.0272) without a clear differential association with surgical approach. A significant postoperative increase in BMI was observed across the cohort (p = 0.0049). The mean preoperative BMI was 22.39 kg/m^2^ (range: 17.50–31.6), increasing to 26.65 kg/m^2^ (range: 21.5–36.7) postoperatively (Table 4). The most substantial BMI increase occurred in case 10 (+77.29%), while case 14 showed minimal change (+2.04%), remaining essentially stable (Figure 5). BMI changes did not show a clear association with the surgical route. Hypopituitarism increased after surgery (Table 3), without a clear differential pattern between endoscopic and transcranial approaches. Exploratory regression analyses did not demonstrate a clear association between surgical approach and endocrinological outcomes, including diabetes insipidus, hypopituitarism, or BMI increase.
4. Discussion
The optimal management of CPs remains debated [9,25,26], with no consensus regarding the preferred surgical approach, the extent of resection, or postoperative management strategy [26,27]. Despite excellent long-term survival rates, surgical treatment is frequently associated with substantial morbidity, particularly involving visual function and the hypothalamic–pituitary axis, with enduring consequences for quality of life [2,3,9,10]. Within this context, our study aimed to explore whether patient-specific skull base anatomy influences surgical approach selection and to examine long-term endocrinological outcomes in a contemporary adult cohort.
Surgical approach selection in CPs is inherently multifactorial, reflecting the interplay between tumor characteristics, skull base anatomy, surgeon experience, and institutional practice. Although transcranial approaches remain appropriate for lesions with marked lateral extension or a predominant intraventricular component, they have been associated with higher perioperative morbidity in several series [28]. Conversely, endoscopic endonasal approaches have gained increasing acceptance, supported by improved visualization of the sellar and suprasellar regions and potential advantages in optic apparatus decompression and stalk identification [27,29,30,31]. Nevertheless, available evidence, particularly in adult populations, does not consistently demonstrate superiority of one approach over the other, underscoring the need for individualized decision-making rather than algorithmic selection [30]. In our Center, an endoscopic endonasal approach was favored when tumor configuration and skull base anatomy were considered favorable, in accordance with established endoscopic classifications such as the Kassam one [24]. Key factors included a predominantly midline tumor location and an adequately developed sphenoid sinus, allowing a safe and effective transsphenoidal corridor. Conversely, a transcranial approach was preferentially selected in cases with marked lateral extension beyond the parasellar region, a predominant intraventricular component, or unfavorable sphenoid sinus anatomy limiting endonasal access. This individualized selection strategy should be considered when interpreting comparative outcomes, as it may have influenced the distribution of anatomical complexity between surgical groups.
In this framework, our findings highlight the relevance of skull base anatomy as a contributory factor in approach feasibility. Specifically, larger sphenoid sinus volumes were associated with selection of an endoscopic endonasal route. This observation is clinically intuitive: when the nasal phase is excluded, the transsphenoidal corridor is constrained primarily by the sphenoid and the sellar floor osteotomy [32]. Volumetric assessment captures these spatial relationships more comprehensively than linear measurements, supporting its use as an adjunct to surgical planning rather than as a stand-alone determinant. Importantly, these data are exploratory and should be interpreted within the broader clinical context and not as rigid anatomical thresholds.
The use of 3D modeling represents a methodological strength of this study. By integrating volumetric reconstructions of both tumor and skull base anatomy, this approach provides a more realistic appraisal of the operative corridor and its constraints. In line with this hypothesis, de Notaris et al. demonstrated the feasibility of generating high-fidelity 3D reconstructions of the sphenoid sinus and sellar region, capturing spatial constraints that are not fully appreciated with conventional 2D imaging. Although primarily proposed for educational purposes, these techniques reinforce the relevance of volumetric assessment of the surgical corridor, which is particularly critical in EAs [33]. Our experience suggests that patient-specific 3D modeling may facilitate surgical planning and multidisciplinary discussion, although reproducibility across centers and operators warrants further validation.
Among patients undergoing endoscopic surgery, the sellar floor osteotomy area, representing the narrowest segment of the transnasal corridor [27], was directly related to tumor volume and independent of sphenoid sinus size, intercarotid distance, or patient-specific anthropometric variables. This finding aligns with prior reports indicating that sphenoid sinus geometry alone does not dictate sellar exposure [14,34,35]. Rather, osteotomy size appears to be deliberately tailored to tumor burden, balancing adequate exposure against the risk of cerebrospinal fluid leakage and vascular injury [14,27,34,35]. When patients are appropriately selected for an endoscopic approach, anatomical variability does not appear to limit exposure or extent of resection.
With respect to oncological outcomes, gross total resection was achieved in the majority of cases, with subtotal resection reserved for lesions with significant hypothalamic adherence. This reflects contemporary practice, in which the absence of a clear surgical plane and the risk of hypothalamic injury represent the principal constraints to radical resection [36]. While gross total resection is associated with lower recurrence rates, subtotal resection followed by adjuvant radiotherapy remains a valid strategy in selected cases [36,37]. In our cohort, all patients undergoing subtotal resection received adjuvant radiosurgery, with only one recurrence observed during follow-up.
Endocrinological morbidity remains a major determinant of long-term outcome after CP surgery. Hypothalamic obesity, in particular, represents one of the most disabling sequelae, typically manifesting early after surgery and often stabilizing over time. The postoperative increase in body mass index observed in our cohort, together with the characteristic pattern of early gain followed by plateau [7], is consistent with hypothalamic involvement described in prior series [25]. These effects frequently require long-term, multidisciplinary management and may persist despite optimal surgical technique. In this series, endocrinological morbidity appeared more closely related to tumor anatomy and hypothalamic involvement than to the surgical corridor itself. The present analyses were observational in nature and were not designed to establish causal relationships between surgical technique and endocrine outcomes.
Diabetes insipidus was also a frequent postoperative finding, in line with the existing literature [30,38]. Its occurrence has been linked to both direct hypothalamic injury and vascular compromise, even in stalk-sparing resections, and does not consistently differ between endoscopic and transcranial approaches [5,37,38]. The close association between diabetes insipidus and hypothalamic obesity, particularly in high-grade tumors, further supports the concept that posterior hypothalamic involvement plays a central role in postoperative endocrine dysfunction [39]. Several studies propose that DI may serve as an early marker of HO, given their shared association with posterior hypothalamic injury [27,29,40]. We support this theory: the hypothalamus, particularly its posterior region, has a mean volume of ~25.93 mm^3^, while the mean tumor volume in our cohort was ~7768 mm^3^ [41]. Given the marked disparity between tumor volume and hypothalamic size, some degree of hypothalamic disturbance may be unavoidable in many cases.
This study has several strengths, including long-term follow-up with detailed endocrinological assessment and the application of volumetric skull base analysis, which remains underreported in the craniopharyngioma literature. The consistency of surgical technique, with all procedures performed by the same senior surgeon, further limits procedural heterogeneity. This is an exploratory study, and the retrospective design, small cohort size, and prolonged inclusion period should be considered when interpreting the findings. While it is not possible to entirely exclude a selection bias in the choice of surgical approach, potentially influenced by sphenoid sinus anatomy, these factors do not diminish the potential utility of our volumetric planning tool as an adjunct in preoperative assessment.
5. Conclusions
The management of craniopharyngiomas remains complex and requires individualized surgical planning. In this series, endoscopic endonasal and transcranial approaches resulted in similar outcomes, although this study was not powered to definitively establish equivalence. Quantitative assessment of skull base anatomy, particularly sphenoid sinus volume derived from 3D modeling, was associated with the selection of an endoscopic approach and may contribute to preoperative feasibility assessment. These findings support the role of patient-specific anatomical evaluation as an adjunct to surgical decision making rather than as a stand-alone determinant. Both gross total and subtotal resection strategies showed distinct risk–benefit profiles, underscoring the importance of balancing tumor control with hypothalamic preservation. Larger, prospective studies are warranted to further refine anatomy-informed surgical planning and its impact on long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Beckhaus J. Friedrich C. Boekhoff S. Calaminus G. Bison B. Eveslage M. Timmermann B. Flitsch J. Müller H.L. Outcome after pediatric craniopharyngioma: The role of age at diagnosis and hypothalamic damage Eur. J. Endocrinol.202318830030910.1093/ejendo/lvad 02736857103 · doi ↗ · pubmed ↗
- 2Hu W. Qiu B. Mei F. Mao J. Zhou L. Liu F. Fan J. Liu Y. Wen G. Qi S. Clinical impact of craniopharyngioma classification based on location origin: A multicenter retrospective study Ann. Transl. Med.20219116410.21037/atm-21-292434430605 PMC 8350632 · doi ↗ · pubmed ↗
- 3Diaz M.J. Kwak S.H. Root K.T. Fadil A. Nguyen A. Ladehoff L. Batchu S. Lucke-Wold B. Current Approaches to Craniopharyngioma Management Front. Biosci.-Landmark 20222732810.31083/j.fbl 271232836624954 · doi ↗ · pubmed ↗
- 4Jensterle M. Jazbinsek S. Bosnjak R. Popovic M. Zaletel L.Z. Vesnaver T.V. Kotnik B.F. Kotnik P. Advances in the management of craniopharyngioma in children and adults Radiol. Oncol.20195338839610.2478/raon-2019-003631652121 PMC 6884937 · doi ↗ · pubmed ↗
- 5Müller H.L. Emser A. Faldum A. Bruhnken G. Etavard-Gorris N. Gebhardt U. Oeverink R. Kolb R. Sörensen N. Longitudinal Study on Growth and Body Mass Index Before and After Diagnosis of Childhood Craniopharyngioma J. Clin. Endocrinol. Metab.2004893298330510.1210/jc.2003-03175115240606 · doi ↗ · pubmed ↗
- 6Bogusz A. Boekhoff S. Warmuth-Metz M. Calaminus G. Eveslage M. Müller H.L. Posterior hypothalamus-sparing surgery improves outcome after childhood craniopharyngioma Endocr. Connect.2019848149210.1530/ec-19-007430925462 PMC 6479199 · doi ↗ · pubmed ↗
- 7Iersel L.V. Brokke K.E. Adan R.A.H. Bulthuis L.C.M. van den Akker E.L.T. van Santen H.M. Pathophysiology and Individualized Treatment of Hypothalamic Obesity Following Craniopharyngioma and Other Suprasellar Tumors: A Systematic Review Endocr. Rev.20184019323510.1210/er.2018-0001730247642 · doi ↗ · pubmed ↗
- 8Castle-Kirszbaum M. Shi M.D.Y. Goldschlager T. Quality of Life in Craniopharyngioma: A Systematic Review World Neurosurg.2022164424435.e 210.1016/j.wneu.2022.05.03835580780 · doi ↗ · pubmed ↗