Osteogenic and Biocompatibility Potential of Polylactic Acid-Based Materials: A Systematic Review of Human Primary Cells Studies
Mario Guerrero-Torres, Silvia M. Becerra-Bayona, Martha L. Arango-Rodríguez, Emilio A. Cafferata

TL;DR
This review examines how polylactic acid-based materials affect human bone and gum cells, showing that modifications can improve their performance for bone regeneration.
Contribution
The study systematically evaluates how specific modifications to PLA/PLGA enhance bioactivity in primary human cells for GBR applications.
Findings
Native polylactic acid-based materials have limited bioactivity.
Modifications like bioceramics and growth factors enhance osteogenic differentiation and mineralization.
Surface topography changes guide fibroblast alignment and affect proliferation.
Abstract
Background: Guided Bone Regeneration (GBR) relies on barrier membranes, for which polylactic acid (PLA) and its copolymer poly(lactic-co-glycolic acid) (PLGA) are promising biodegradable polymers. However, their inherent hydrophobicity limits biological performance, and the evidence regarding how specific modifications affect key human cell types, particularly osteoblasts and fibroblasts, remains scattered. Methods: A systematic review was conducted to synthesize the in vitro evidence on the response of primary human osteoblasts and fibroblasts to polylactic acid-based materials. Following a pre-registered protocol (10.17605/OSF.IO/CE8KB), a comprehensive search was performed across four major databases, and the risk of bias in the included studies was assessed using an adapted OHAT tool. Results: Twenty-six studies were included, which showed that polylactic acid-based materials have…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
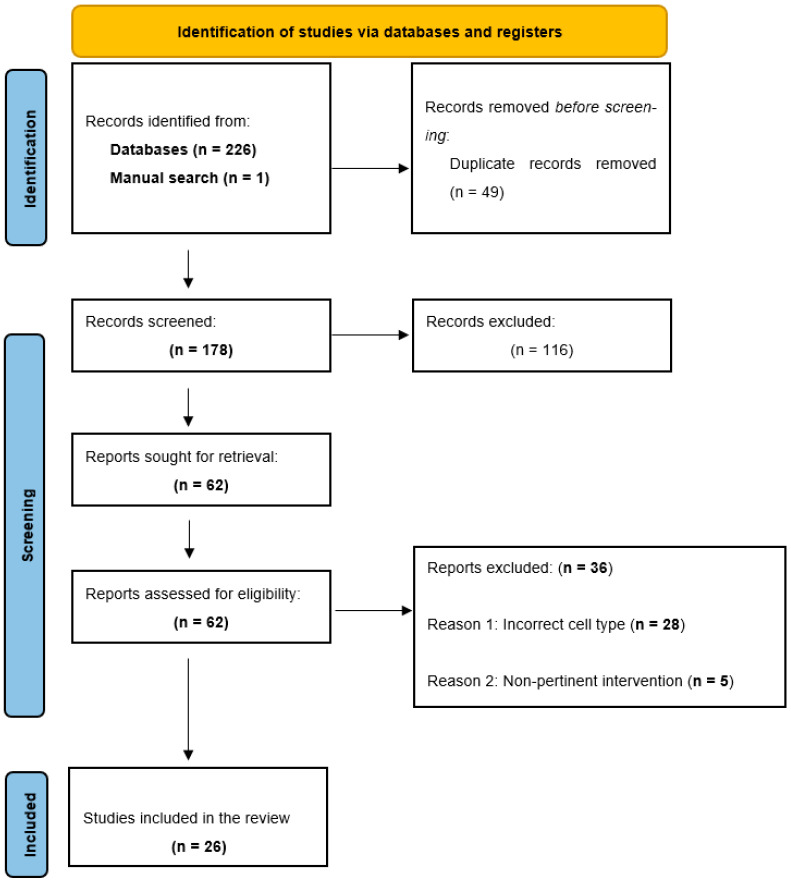 Figure 1
Figure 1- —Universidad Científica del Sur
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tissue Engineering Materials · Periodontal Regeneration and Treatments · Dental Implant Techniques and Outcomes
1. Introduction
Guided bone regeneration is a cornerstone technique for the management of alveolar bone defects arising from tooth loss or periodontal disease, and implant site development [1]. Its clinical success is critically dependent on the use of a barrier membrane that selectively promotes bone regeneration while preventing the ingrowth of soft tissue. However, currently available membranes present inherent limitations [2].
Non-resorbable membranes, made from expanded polytetrafluoroethylene (e-PTFE) and titanium mesh, provide superior space maintenance and structural integrity but require a second surgical procedure for removal and are highly susceptible to bacterial contamination if exposed [3]. On the other hand, resorbable membranes, typically collagen-based, eliminate the need for membrane retrieval but often lack sufficient mechanical stability, frequently leading to the collapse of the regenerative space, present inconsistent resorption rates and limited bioactivity [3]. These limitations highlight the ongoing demand for a next-generation membrane that combines complete resorbability with the mechanical robustness of its non-resorbable counterparts, a predictable degradation profile, and osteogenic potential. While there is no universal solution for every clinical situation, it is widely acknowledged that the future of GBR lies in the development of membranes capable of promoting bone regeneration, rather than serving as passive barriers [2,3].
Polylactic acid (PLA), a synthetic biodegradable polymer, has emerged as a promising material for GBR resorbable membranes development, due to its favorable biocompatibility, tunable degradation profile and adjustable mechanical properties. It has been investigated for a wide range of clinical applications, including horizontal and vertical ridge augmentation, treatment of intrabony periodontal defects, and coverage of implant-related dehiscence and fenestration defects [1]. Despite its potential, the clinical translation of unmodified PLA remains hampered by intrinsic limitations [4]. First, its inherent hydrophobicity interferes with early biological events, such as blood clot stabilization and protein adsorption, critical for cell adhesion and tissue integration [5]. Then, PLA degradation produces acidic byproducts, primarily lactic acid, which can lower the local microenvironment pH. This acidic shift may not only compromise cell viability but also activate immune cells, such as macrophages, through metabolic reprogramming [6]. This can lead to a sterile inflammatory response characterized by increased proinflammatory cytokines production, which may promote fibrous encapsulation, impair osseous integration and, in some cases, induce localized bone resorption instead of regeneration [7]. These biological drawbacks have driven the development of numerous modifications aimed at transforming PLA from a passive barrier into a bioactive scaffold capable of supporting and promoting bone regeneration [8].
To overcome these limitations, a broad array of physicochemical and biological strategies have been explored to enhance the functionality of PLA [9]. These include the incorporation of bioceramics such as hydroxyapatite (HA), tricalcium phosphate (TCP), amorphous calcium phosphate, or bioactive glass to enhance osteoconductivity [10,11]; blending with biopolymers like collagen to improve cellular affinity and matrix interaction; surface functionalization with inorganic coatings or bioactive molecules to modulate cell behavior; and the incorporation of growth factors such as bone morphogenetic protein (BMP)-2 or transforming growth factor (TGF)-β1 to actively promote osteogenic differentiation and tissue regeneration [9,12,13].
To start, guide and validate the rational development of next-generation PLA membranes, a thorough understanding of their interaction with the primary human cells most relevant to GBR is required. These mainly include osteoblasts, responsible for bone formation, and gingival fibroblasts, which are critical for soft tissue sealing and barrier integration. Therefore, an ideal membrane must exhibit a “dual biofunctionality”: its internal surface (facing the bone defect) should be osteoinductive, while the external surface (facing the soft tissue) should support the integration with the connective tissue and prevent epithelial ingrowth [2].
Despite substantial progress, the current body of in vitro evidence regarding primary human cell responses to PLA membranes and its modifications remains scattered and often based on non-human or immortalized cell models. These models often exhibit altered genetic, phenotypic, and signaling profiles leading to altered responses to biomaterial properties and limited physiological relevance. In contrast, primary human cells retain native characteristics and donor-specific variability, offering a more accurate representation of clinical conditions [14]. This lack of consolidated data hinders the identification of the most effective material modifications and prevents progress towards the design of clinically optimized PLA membranes for GBR [15,16].
In this review, we use the term “PLA-based materials” to encompass both polylactic-acid homopolymers (PLLA/PDLLA) and the copolymer PLGA. This choice is justified because they share the lactic repeat unit and hydrolytic degradation pathway with lactic acid release; PLGA is widely used as a barrier membrane for GBR and undergoes the same families of modifications and comparing PLA vs. PLGA helps disentangle the influence of copolymer composition, crystallinity, and degradation kinetics on primary human osteoblast/progenitor and gingival fibroblast responses.
Therefore, the objective of this systematic review was to address a specific and under-synthesized question: how polylactic acid–based membranes and their modifications influence the behavior of primary human osteoblasts/progenitors and gingival fibroblasts relevant to GBR. Previous reviews have provided valuable overviews of this field, yet they have largely relied on heterogeneous sources of evidence, including observational human studies [17], diverse and non-comparable animal models [18], immortalized cell lines [19], and network meta-analyses that aggregate animal data without discriminating species or defect models [20]. In contrast, the present analysis focuses exclusively on primary human cells to maximize translational relevance. The evidence is interpreted within the framework of the dual biofunctionality requirement for GBR membranes—osteogenic performance towards the defect and soft-tissue integration on the opposite face—allowing material modifications to be evaluated against clear, clinically grounded functions. Beyond a descriptive synthesis, the review employs standardized data extraction by outcome domains and systematically maps categories of PLA-based material modifications (inorganic phase incorporation, surface chemistry and energy tuning, topographical control, and immobilized bioactive cues) to specific cellular responses. This translational and function-oriented approach generates evidence-based design principles that are directly actionable for the development and refinement of next-generation PLA-based GBR membranes.
2. Materials and Methods
2.1. Protocol and Registration
The protocol for this systematic review was registered a priori in the Open Science Frameworks (OSF) Registries platform (Charlottesville, VA, USA) under the digital object identifier (DOI): 10.17605/OSF.IO/CE8KB. The review was conducted and reported in accordance with the PRISMA 2020 statement, ensuring transparency and reproducibility of the methodology employed [21].
2.2. Eligibility Criteria
The present systematic review was designed to answer the following PICO research question:
In primary human osteoblast and/or gingival fibroblast cultures (P), what is the cellular response—including viability, proliferation, adhesion, osteogenic differentiation, extracellular matrix production, and inflammatory response—(O) upon exposure to polylactic acid-based materials and its various modifications (I), compared to negative controls, conventional barrier membranes for GBR, or alternative polylactic acid-based materials formulations (C)?
2.2.1. Inclusion Criteria
Study type: in vitro studiesCell population: studies using primary cultures of human osteoblasts (including those derived from mesenchymal stem cells) or primary cultures of human gingival fibroblasts.Intervention: studies evaluating the cellular response to pure polylactic acid-based materials or any of its modifications.Comparison: studies that included at least one comparison against a control group, standard barrier membranes used in GBR, or between different polylactic acid-based materials formulations.Outcomes: studies that reported at least one outcome of interest, such as cell viability, proliferation, adhesion, osteogenic differentiation markers, mineralization, or extracellular matrix production.
2.2.2. Exclusion Criteria
Study type: letters to the editor, editorials, conference abstracts, and book chapters.Cell population: studies using immortalized cell lines, non-human cells, or infected or genetically modified human cells.Accessibility: articles whose full text was not available.
Studies using immortalized cell lines and animal (in vivo) models were excluded to avoid nonspecific responses to PLA material modifications that fall outside the objectives of this review.
2.3. Information Sources and Search Strategy
A comprehensive literature search was conducted from inception up to October 2025 in four electronic databases: Medline (via Pubmed), Biblioteca Virtual En Salud (BVS), Scopus, and Web of Science. The search strategies combined controlled vocabulary terms and free-text terms to cover all aspects of the PICO question. Additionally, a manual search of the reference lists of the included studies was performed to identify relevant records not captured in the initial search. No date or language restrictions were applied.
2.4. Selection of Studies
The selection process was carried out in three phases. First, duplicates were removed using Rayyan software (Version 1.7, Cambridge, MA, USA). Next, two independent reviewers screened the titles and abstracts. Finally, the same two reviewers independently assessed the full text of the pre-selected articles to determine their final eligibility based on the inclusion and exclusion criteria. Any discrepancies during the process were resolved through discussion or with the intervention of a third reviewer to reach a consensus.
2.5. Data Collection
Data extraction was performed by two authors independently and in duplicate, using a standardized spreadsheet. For each study, the following data were extracted: (1) reference information (author, year); (2) sample characteristics (cell type, origin, number of donors); (3) PLA material and modifications (polymer type, specific modifications, material form); (4) comparison group(s); (5) main outcomes (reported quantitative and qualitative cellular responses); (6) authors’ conclusions; and (7) declared conflict of interest. A third author verified the accuracy and completeness of the extracted data, and any discrepancies were resolved through discussion to reach a consensus.
2.6. Data Items—Complementary
Characterization of materials—Standardized extraction of characterization parameters was performed for native and functionalized PLA/PLGA surfaces. The following features were recorded: topography (SEM, AFM; Ra/Rq metrics), surface chemistry (XPS/FTIR), wettability (contact angle), surface energy (Owens–Wendt method), crystallinity (XRD/DSC), zeta potential and mechanical properties, as well as coating stability when applicable.
Culture conditions—Extraction was standardized for cell type, seeding density, medium composition (serum/antibiotics), evaluation time points, incubation parameters (CO_2_/°C) and substrate preconditioning.
2.7. Risk of Bias Assessment
The Office of Health Assessment and Translation (OHAT) risk of bias (RoB) rating tool adaptation for in vitro studies was used to assess the RoB of the included studies. This tool was selected for its specific applicability to experimental in vitro studies, allowing for a structured evaluation of the credibility of the findings. The assessment focused on several key domains pertinent to the included studies, such as selection bias, confounding, characterization of the intervention (exposure), blinding of outcome assessment, and selective reporting of results [22].
The assessment was performed independently and in duplicate by two reviewers. To ensure consistent application of the tool’s criteria, the reviewers first conducted a calibration exercise on a subset of the included studies, supervised by a third author. For each domain within each study, a judgment of ‘low risk’, ‘unclear risk’, or ‘high risk’ of bias was assigned based on the signaling questions provided by the OHAT tool. Any disagreements between the two primary reviewers during the assessment process were resolved through discussion to reach a consensus. If an agreement could not be reached, the third author was consulted to make a final decision.
2.8. Outcome Measures
The primary outcomes were defined according to the cell type:
For osteoblasts and their progenitors: The assessment focused on cell viability, proliferation, cell adhesion and morphology, osteogenic differentiation (evaluated through markers such as alkaline phosphatase (ALP) and osteocalcin (OCN) expression), and extracellular matrix production and mineralization (e.g., evaluated by calcium deposition) [23].
For gingival fibroblasts: The outcomes of interest included cell viability, proliferation, cell adhesion, morphology, and migration, and extracellular matrix production (e.g., type I collagen) [24].
2.9. Data Synthesis
A narrative and qualitative synthesis of the included studies was conducted. Findings were thematically grouped according to cell type (osteoblasts/progenitors and gingival fibroblasts) and, within each group, were organized by type of outcome (e.g., adhesion, proliferation, differentiation). The results from each study were described systematically, highlighting the direction and magnitude of the observed effects and referencing the comparisons with relevant control groups.
3. Results
A total of 226 records were retrieved through the initial database search: Medline (n = 91), Scopus (n = 73), Web of Science (n = 60), and BVS (n = 2). After duplicate records removal (n = 49), 177 unique articles remained for screening. During title and abstract screening phase, 116 articles were excluded for being unrelated to the research question. Subsequently, the remaining 61 articles were selected for full-text review. In addition, 1 record was identified through manual searching; this record was also assessed in full and met the eligibility criteria. In total, 26 studies were included in the qualitative synthesis (Figure 1).
Flowchart depicting the studies selection for inclusion in the present systematic review.
3.1. Characteristics of the Included Studies
The 26 included studies were published between 1996 and 2023, reflecting a sustained and growing interest in the application of PLA-based materials for GBR. The studies originate from a diverse geographic range, with notable contributions from Asia (n = 12), Europe (n = 10), and North America (n = 4).
Among the included studies, 21 evaluated the response of primary human osteoblasts or their progenitor cells —including mesenchymal stem cells from bone marrow, adipose-derived stem cells, periodontal ligament, amnion, dental pulp, or skeletal sources—[25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46] (Table 1), while the remaining 5 studies focused on primary human gingival fibroblasts [31,47,48,49,50] (Table 2). The interventions were highly varied, ranging from unmodified polylactic acid-based materials, which were evaluated in 7 studies, to complex modifications. These included the creation of composites with bioceramics like hydroxyapatite (HA) or TiO_2_ [28,35,41], surface functionalization with inorganic coatings such as SiO_2_ or collagen [27,38]; alteration of microtopography through micro-grooves [31,49]; and loading with growth factors like BMP-2 or TGF-β1 [26,33,36]. The most common comparison groups were tissue culture polystyrene (TCPS) [30,32], unmodified polylactic acid-based materials, and other commercial membranes (e.g., ePTFE, collagen). Detailed information for each study is presented in Table 1 and Table 2.
3.2. Osteoblasts and Osteogenic Progenitors Response to Polylactic Acid-Based Materials
The response of osteoblastic lineage cells towards polylactic acid-based materials is strongly influenced by material formulation. A consistent trend shows that modifications to the polylactic acid-based materials matrix base, through the addition of bioceramics composites, the functionalization of its surface with coatings, and the incorporation of bioactive molecules like growth factors, are essential to enhance favorable cellular behavior [28,29,34,35]. Additionally, micro/nanotopographic patterning exemplified by PLA nanopillar arrays with controlled pillar diameters (≈100–300 nm; 450 nm pitch) can by itself steer osteogenic commitment of primary hADSCs without exogenous osteogenic supplements; notably, ≈200 nm pillars maximized ALP at day 14, upregulated RUNX2/OPN/OCN, enhanced mineralization in vitro, and improved ectopic osteogenesis versus planar PLA [46].
Characterization of materials
In the osteoblast/progenitor group, the most frequently used characterization technique was scanning electron microscopy (SEM) (n = 16; [27,28,29,30,31,32,33,34,35,36,38,39,42,43,44,45,46]). Less frequently, studies reported mechanical properties (n = 8; [29,33,37,38,39,41,43,45]), atomic force microscopy (AFM) roughness (Ra/Rq) (n = 4; [29,30,39,44]), contact angle (n = 3; [30,38,40]), X-ray photoelectron spectroscopy (XPS/ESCA) (n = 3; [29,30,44]), and X-ray diffraction (XRD) (n = 2; [29,35]). Fourier transform infrared spectroscopy (FTIR) was reported once (n = 1; [38]), and only a single study provided surface energy determined by the Owens–Wendt method (n = 1; [44]).
When key physicochemical metrics were reported (e.g., wettability/surface energy, AFM roughness Ra/Rq, and surface chemistry by XPS/ESCA), the trend was consistent: more hydrophilic surfaces with controlled sub-micrometric roughness were associated with more mature focal adhesions, higher ALP activity and RUNX2/OCN expression, and greater mineralization than native PLA/PLGA [29,30,33,35,38,40,44]. Strategies combining inorganic phases or bioactive coatings further reinforced these effects [27,29,30,33,35,38,44]. However, the low frequency of AFM/XPS reporting limits fine quantitative comparisons across studies.
Culture conditions
Culture conditions. Most studies incubated cells under standard conditions—37 °C and 5% CO_2_ (explicitly reported in n = 23; [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,49])—using either DMEM (n = 9; [28,31,33,34,36,38,39,41,44]) or α-MEM (n = 5; [32,33,35,38,46]) as basal media, supplemented with fetal bovine serum (FBS) (n = 14; [28,31,32,33,34,35,36,38,39,40,41,42,44,45,46]). Antibiotics/antimycotics (mostly penicillin–streptomycin) were added in n = 14 studies ([27,28,31,32,34,35,38,39,40,41,42,44,46,49]). Notably, Ref. [46] maintained osteogenic progenitors under growth-factor–free conditions.
Osteogenic induction using ascorbic acid, β-glycerophosphate, dexamethasone, or osteogenic medium was frequent (n = 14; [26,27,28,30,32,33,34,35,36,37,42,44,45,49]). While these approaches accelerate the RUNX2→OCN differentiation pathway and subsequent mineralization, they can create a ceiling effect that reduces detectable differences between surface conditions. By contrast, at least one study deliberately withheld osteogenic supplements to isolate material-driven effects; under growth-factor–free conditions, PLA nanopillar arrays still enhanced ALP, osteogenic gene expression, and mineralization [46].
Seeding density was reported in n = 13 studies ([25,26,27,30,33,34,35,36,37,38,39,41,44]) and acted as a confounder. High seeding densities favor paracrine signaling and early confluence, dampening sensitivity to micro/nanotopographic cues, whereas low densities amplify differences in adhesion and ALP activity.
Readouts were most often taken at day 7 (D7) (n = 10; [27,28,32,34,35,36,41,43,44,46]) and D14 (n = 6; [27,32,39,43,44,46]) for early events, and at D21 (n = 7; [27,32,39,43,44,46]) and D28 (n = 3; [34,43,44]) for mineralization. Thus, restricting observation to fewer than 14 days may fail to capture late effects of inorganic additives or PDA coatings; conversely, topography-driven responses can peak around D14 [46].
Substrate preconditioning was highly heterogeneous. Any form of preconditioning (n = 10; [27,30,32,33,36,37,38,39,42,44])—including protein coatings (collagen/fibronectin; n = 2; [25,30]), plasma treatment (n = 4; [30,39,42,44]), and PDA precoating (n = 6; [27,33,36,38,42,44])—tended to homogenize the initial protein-adsorption layer and was associated with faster cell attachment/spreading and higher osteogenic readouts, consistent with increased surface wettability and surface energy. Notably, one study intentionally avoided preconditioning and osteogenic supplements yet still observed enhanced ALP, osteogenic gene expression, and mineralization driven by nanoscale topography [46]. Nevertheless, under strong osteogenic induction, preconditioning may mask subtle differences attributable to the base surface properties.
Cell adhesion, spreading, and morphology:
Unmodified PLA clearly demonstrates limited suitability as a substrate for initial cell adhesion. For instance, Ellis and Chaudhuri reported that significantly fewer human bone-derived cells (HBDC) attached to pure PLA membranes at 6 h compared with tissue culture polystyrene (TCP) (p < 0.05), with the adhered cells exhibiting a predominantly rounded morphology suggesting a state of cellular stress and poor surface adhesion [30]. Similarly, Chen et al. noted restricted spreading and disorganized cytoskeletal organization of hMSCs on PLLA films, a specific PLA isomer [29].
In contrast, surface or compositional modifications to polylactic acid-based materials have been shown to significantly improve cell adhesion. In this line, studies by Terriza et al. showed that the functionalization of poly(lactic-co-glycolic) acid (PLGA) membranes—a copolymer derived from PLA—nanolayers of TiO_2_ or SiO_2_ via plasma-enhanced chemical vapor deposition significantly increased focal adhesion formation (p < 0.001), by inducing the reorganization of the actin cytoskeleton [37,38]. Likewise, Liu et al. reported a significant increase in osteoblast attachment on composites with 20 wt% nanophase titania compared to pure PLGA after 4 h of culture (p < 0.05) [28].
Cell proliferation
Evidence on cellular proliferation is mixed, suggesting that while the polylactic acid-based materials are cytocompatible, it does not consistently promote proliferation superior to standard controls. For instance, Ellis and Chaudhuri found significantly reduced proliferation of HBDCs on 50:50 and 75:25 PLGA membranes compared to TCP after 7 days (p < 0.05) [23]. In contrast, Hasan et al. observed no significant differences in DNA content between glass fiber-reinforced PLA composites and TCPs over a period of 14–21 days, indicating that certain formulations can provide adequate support for long-term cell proliferation [25].
Bioactive modifications appear to consistently improve the proliferative response to the PLA matrix. In this context, Fu et al. demonstrated that PLGA/nHA composite membranes yielded significantly higher CCK-8 absorbance values at 7 days than pure PLGA membranes (p < 0.05). This indicates a greater metabolic activity, which serves as a proxy for enhanced cell proliferation on the nano-hydroxyapatite functionalized surface [34].
Osteogenic differentiation and mineralization
This outcome is the most responsive to polylactic acid-based materials modifications, with the most compelling enhancements observed in bioactive formulations.
ALP activity: polylactic acid-based materials demonstrate a capacity to maintain the osteoblastic phenotype. Marinucci et al. reported a 59% increase in ALP activity on Poly DL-lactide membranes compared to ePTFE controls [25]. However, bioactivation by incorporating composites or growth factors significantly amplifies this effect. Liu et al. observed a two- to three-fold increase in ALP activity on PLGA composites containing 30–40 wt% nanophase titania compared to pure PLGA at 21 days [28]. While Cho et al. reported an approximately five-fold increase of ALP levels in PLLA/Polydopamine/BMP-2 scaffolds compared to PLLA scaffolds alone at 14 days [26]. Additionally, a topography-only approach PLA nanopillar arrays (≈100–300 nm diameter; 450 nm pitch) under growth-factor free conditions produced the highest ALP on ≈200 nm pillars, peaking at day 14 [46].The expression of key osteogenic differentiation genes is markedly enhanced in modified scaffolds. Specifically, Wang et al. found that functionalizing PLGA/collagen nanofibers with the recombinant fusion peptide rFN/CDHs (Fibronectin/Cadherin) led to a significant upregulation of key osteogenic markers in hMSCs after 14 days: RUNX2 (~3-fold), ALP (~4.5-fold), and OCN (~5-fold) [45]. Similar patterns of osteogenic markers upregulations have been observed with BMP-2 or nHA incorporation into PLA/PLGA scaffolds in multiple studies using hMSCs or other osteoblastic progenitors (hAMSCs, hPDLSCs) [36,42,43,45].Matrix production and mineralization. Unmodified polylactic acid–based materials generally show minimal mineralization (Von Kossa or Alizarin Red). Ellis and Chaudhuri quantified <1 mineralized nodule/cm^2^ on PLGA membranes versus ~2.4 nodules/cm^2^ on TCPS [30]. In contrast, bioactive modifications promoted extensive calcium deposition [36,41]. Topography only PLA nanopillar arrays further increased mineralization and improved ectopic osteogenesis in vivo compared with planar PLA [46].
3.3. Gingival Fibroblasts Cells Response to PLA
The interaction of human gingival fibroblasts (HGFs) with PLA-based membranes is critical for soft tissue healing and maintenance of the barrier function during GBR.
Characterization of materials
In human gingival fibroblast (FGH) studies, characterization was more limited: SEM was reported (n = 2; [47,49]), along with single reports of contact angle (n = 1; [47]) and surface energy (n = 1; [49]). This limited dataset restricts the ability to correlate surface properties with adhesion and potential soft tissue sealing. Even so, studies reporting higher wettability consistently reported improved cell spreading and cytoskeletal organization than less hydrophilic or unmodified surfaces, supporting a more stable epithelial seal [47,49]. Integrin–FAK signaling on 3D-PLGA was also reported as a plausible substrate-mediated mechanotransduction pathway [50]. The near absence of AFM/XPS combined with the heterogeneity in seeding density and readout times may explain part of the interstudy variability.
Culture conditions
Reporting was sparse: DMEM and FBS were each specified (n = 1; [50]), antibiotics (n = 1; [47]), seeding density (n = 1; [47]), 37 °C (n = 2; [47,50]) and 5% CO_2_ (n = 1; [50]). Even so, studies that explicitly reported standard incubator conditions and serum supplementation described improved cell spreading and stress-fiber organization on more wettable or higher-energy surfaces, consistent with a more stable soft-tissue seal. However, the absence of explicit preconditioning, combined with heterogeneity in FBS concentration and seeding density and the lack of late (≥D21) readouts, limits robust correlation between culture handling and sealing behavior. Future studies should at minimum standardize serum concentration, seeding density, and evaluation windows (D7/D14 and ≥D21) to enable reproducible comparisons.
Adhesion, morphology, and migration
Early studies have consistently reported a poor fibroblast response to unmodified polylactic acid–based materials. Paynet observed no detectable migration (0.00 mm) of HGFs on PLA membranes, with cells adopting an abnormal “fried egg” morphology [47]. Similarly, Unsal et al., found significantly lower HGF attachment on PLA/PGA membranes (12.80 ± 0.47 cells/area) compared to collagen membranes (>21 cells/area) (p < 0.01) [48].
Surface modifications, however, have demonstrated the ability to modulate HGF behavior. Owen et al. showed that micro-grooved PLGA films induced an alignment of 80% of HGFs along the groove axis, despite reducing cell spreading area by ~35% [49]. More recently Wei et al. reported that HGFs cultured on a 3D PLGA scaffold under mechanical loading (25 g/cm^2^) reorganized their cytoskeleton and formed stress fibers, suggesting a functional and adaptive cell–material interaction in conditions that better simulate the vivo environment [18].
Proliferation and extracellular matrix production
HGF proliferation on smooth PLGA was comparable to standard controls but was significantly reduced (~40%) on micro-grooved films at day 7 [49]. In contrast, mechanical stimulation of HGFs on 3D PLGA scaffolds significantly upregulated type I collagen mRNA and protein expression by ~2-fold, indicating that scaffold architecture and biomechanical cues can enhance extracellular matrix deposition [50].
3.4. Risk of Bias of the Included Studies
The RoB assessment, conducted using the OHAT tool adapted for in vitro studies, revealed consistent methodological features across the included literature.
For the 21 studies evaluating osteoblasts and their progenitor cells, the overall risk of bias was judged to be low in domains related to material characterization, consistency of experimental conditions, and completeness of outcome reporting. Importantly, formal sample randomization was not considered critical in this context, since nearly all studies clearly stated that cells were treated under identical conditions, thereby minimizing the risk of systematic selection bias. Similarly, allocation concealment was rated as adequate whenever experimental groups were explicitly described, which was the case for the majority of the included works. The main limitation remained the lack of blinding in outcome assessment, which was rarely reported and thus represents a potential source of detection bias (Table 3).
The assessment was performed using the OHAT tool adapted for in vitro studies. Risk of bias was judged across key domains including exposure definition, allocation concealment, consistency of experimental conditions, blinding of outcome assessment, completeness of outcome data, selective reporting, and other potential sources of bias. Symbols represent the following: (++) low risk of bias; (+) probably low risk of bias; (-) high or unclear risk of bias.
The five studies that focused on human gingival fibroblasts displayed a comparable profile. As with the osteoblast studies, the experimental execution was generally robust, supported by clear descriptions of materials and conditions, while again showing deficiencies in blinding procedures (Table 4).
The same OHAT-based criteria were applied as in Table 3. Domains included allocation concealment, experimental consistency, blinding of outcome assessment, completeness of outcome data, selective reporting, and replication procedures. Symbols represent the following: (++) low risk of bias; (+) probably low risk of bias; (-) high or unclear risk of bias.
Finally, in the category of other sources of bias, a substantial proportion of the included studies reported conducting experiments in duplicate or triplicate. This practice enhances reproducibility and strengthens confidence in the reliability of their findings.
Taken together, this RoB assessment suggests that while the technical execution and reporting of in vitro studies on PLA-based materials are generally strong, the limited use of blinding and occasional lack of detail in replication procedures remain the primary methodological concerns.
4. Discussion
The main findings of this systematic review, derived from the analysis of 26 in vitro studies, conclude that polylactic acid and its copolymers are biocompatible, yet inherently bioinert. Their clinical potential for GBR is not fully realized in their unmodified form but is unlocked through targeted modifications that transform them into bioactive scaffolds capable of directing specific cellular responses. This marks a significant conceptual shift: from considering PLA as a passive barrier to recognizing it as a highly tunable platform for regeneration. The cumulated evidence suggests that targeted functionalization of PLA can be tailored to fulfill “dual bifunctionality” required for GBR: promoting osteogenesis on the side facing the defect, while guiding soft tissue integration on the external surface.
Across the 26 studies analyzed, several consistent patterns emerge that can inform evidence-based design strategies for optimizing osteogenic and soft-tissue responses. First, surface physicochemical properties appear to be a primary determinant of cell behavior: materials exhibiting increased wettability and surface energy, combined with controlled sub-micrometric roughness, consistently promote faster focal adhesion maturation and the upregulation of early osteogenic markers [29,30,33,35,38,40,44]. The incorporation of inorganic, osteoconductive phases such as calcium phosphates further enhances osteoblastic differentiation, as reflected by elevated ALP activity and calcium deposition compared to unmodified PLA/PLGA matrices [27,33,39]. Beyond compositional tuning, the mode of bioactive cue presentation also plays a decisive role. Covalent or polydopamine (PDA)-mediated immobilization of osteogenic molecules ensures stable and localized signaling, thereby amplifying differentiation and mineralization outcomes [28,44,45]. Interestingly, several reports demonstrate that even in the absence of exogenous supplements, nanoscale topographical features—particularly around 200 nm—can bias stem cell fate toward osteogenic lineages, emphasizing the instructive capacity of geometry itself [46]. Finally, at the soft-tissue interface, tailored micro-groove architectures and moderate surface energy were found to promote fibroblast alignment and robust adhesion while limiting excessive proliferation, contributing to the establishment of a stable and functional soft-tissue seal [47,49]. Collectively, these findings delineate a coherent set of design principles that transcend isolated experimental observations, providing a rational framework for the development of next-generation biomaterial surfaces supporting both hard- and soft-tissue integration.
Data from studies using human gingival fibroblasts indicate that the membrane’s outer face should be engineered to optimize submicrometric roughness and surface energy, thereby stabilizing the matrix-protein layer and promoting the formation of mature focal adhesions [50]. This fine-tuning of topography and surface chemistry regulates protein adsorption, cytoskeletal organization, and resistance to detachment under shear forces —factors that collectively determine the establishment of a stable soft-tissue seal [47,49,50]. However, the comparability across studies remains limited due to heterogeneity between seeding densities, evaluation times, and adhesion assessment methods, as well as the frequent omission of key features of the oral environment in most in vitro models [47,48,49,50].
The poor performance of unmodified PLA aligns with well-established principles of cell–biomaterial interaction. Indeed, the hydrophobic nature of PLA, assessed in different studies, hinders the adsorption of adhesion mediating proteins like vitronectin and fibronectin, which are essential for integrin-mediated cell attachment. This, at least partially, explains the poor spreading and rounded morphology of hMSCs and hBDCs observed by Chen et al., respectively [29]. Similarly, Payne et al. reported a complete inhibition of HGFs on PLA membranes, reinforcing the notion that PLA’s surface chemistry is suboptimal for initial cell attachment [47].
Long-term performance of PLA/PLGA-based materials is conditioned by hydrolytic and autocatalytic degradation, which generate an acidic microenvironment and local pH gradients. Progressive reductions in molecular weight and alterations in crystallinity can modify surface wettability and energy, directly influencing protein adsorption and the subsequent cellular responses. These physicochemical changes may attenuate or reverse the initial benefits of coatings and inorganic fillers observed during short culture periods. Accordingly, future studies should incorporate extended follow-up periods, monitor pH and lactate accumulation, while document coating stability together with the retention of mechanical and surface properties. This approach will help identify modification strategies that maintain their effects under realistic conditions of polymer degradation [4,7,8].
The success of PLA modification strategies can be interpreted through their ability to overcome these early shortcomings. By modifying the surface chemistry and topography, Terriza showed that coating PLA with a thin nanolayer of TiO_2_ or SiO_2_ is sufficient to significantly enhance osteoblast adhesion and cytoskeletal organization (p < 0.001) [30,31]. Similarly, Owen et al., demonstrated that micro-topographic cues alone can direct HGF alignment [41], while Graziano et al., found such cues may even induce osteogenic differentiation in DPSCs [31]. These suggests that the initial cell “sensing” of the surface chemistry is a critical modulating event. On the other side, the incorporation of bioactive cues showed the most dramatic osteogenic responses when bioceramics like HA or growth factors like BMP-2 were incorporated [41].
Topography-only evidence. Beyond chemical or biochemical functionalization, nanoscale geometry alone can be instructive. In the topography-only study [46], PLA nanopillar arrays (≈100–300 nm diameter; 450 nm pitch) induced osteogenic commitment of primary hADSCs under growth-factor–free conditions. Pillars of ≈200 nm maximized ALP around day 14, up-regulated RUNX2/OPN/OCN with increased Alizarin Red mineralization by day 21 and enhanced ectopic osteogenesis versus planar PLA. These findings reinforce that surface nanotopography can drive fate decisions independently of biochemical cues and dovetail with the dual-biofunctionality design principle for GBR membranes. Nevertheless, this evidence comes from a single primary cell source and short timeframes with limited blinding, warranting validation across donors and under conditions that simulate hydrolytic degradation.
Liu et al. reported a 2- to 3-fold increase in ALP activity with titania composites [28], while Cho et al. observed a 5-fold increase when BMP-2 was immobilized on PLA scaffolds [33]. These findings are consistent with the known osteoconductive properties of calcium phosphates, by providing nucleation sites for mineralization, and the potent osteogenic potential of BMP-2, thus highlighting a shift from a merely osteoconductive to an actively osteoinductive material.
Despite the overall consistency, some variability in results warrants further discussion. For instance, while Ellis and Chaudhuri reported reduced proliferation of human bone-derived cells on PLGA membranes compared to controls [30], Hasan et al. observed comparable long-term proliferation on PLA composites [32]. This could be explained due to differences in degradation kinetics, where faster degradation of the PLGA membranes might have led to a more acidic microenvironment that temporarily inhibited proliferation, an effect less pronounced in more stable PLA composites. Moreover, heterogeneity between primary cells sources may also account for inherent biological variability affecting the magnitude of the observed effects across studies. Otherwise, an important unresolved question is the long-term impact of acidic degradation by products on mature, mineralized matrix integrity, an issue not addressed by the included short-term studies.
The findings of this review carry practical implications for the design of next-generation GBR membranes. The cumulated evidence suggests that passive barriers should no longer be the gold standard, and that GBR membrane must be engineered instead with a dual-sided functionality. For instance, an internal surface functionalized with HA or a low dose of BMP-2, to actively recruit and promote the differentiation osteoprogenitor cells [36,41]. And complementarily, an external surface with a tailored micro-topography to align gingival fibroblasts and limit over-proliferation [49], potentially enhancing flap stability and minimizing fibrous encapsulation. As Chen et al. notes, it is essential to distinguish between statistically significant and clinically meaningful differences. While minor increases in ALP activity may not directly impact clinical performance, the multi-fold increases observed with functionalized PLA modifications are more likely to translate into clinically relevant improvements in bone regeneration [29].
While this review synthesized a valuable body of in vitro evidence, several limitations must be acknowledged. The most significant limitation is the high methodological heterogeneity across studies, which prevented the performance of a pooled quantitative analysis. There is a clear lack of standardization in cell culture protocols, the specific formulation and characterization of PLA materials, and the time points chosen for evaluation. Secondly, the risk of bias assessment revealed that many studies failed to report on key methodological aspects, particularly the blinding of outcome assessment, introducing potential for detection bias. Finally, and most critically, these are all in vitro studies. Despite providing invaluable mechanistic insights, these cannot fully replicate the complexity of the in vivo environment, including the immune response, angiogenesis, and mechanical loading.
Therefore, to elaborate on the state of the evidence and address the current gap, future research should prioritize: the development of guidelines for the in vitro testing of membranes for GBR, including a minimum set of material characterization and cellular outcomes to be reported, which would improve their comparability and reliability [29]. The RoB assessment indicates that most in vitro studies on PLA-based materials demonstrate strong technical execution and consistent reporting, particularly in material characterization and standardized experimental conditions. However, the limited reporting of blinding procedures and occasional lack of detail regarding replication remain important considerations, underscoring the need for greater methodological transparency in future research. Moreover, further studies should move towards more complex cellular models, such as co-cultures osteoblast-fibroblast on opposite sides of a test membrane, or macrophage-inclusive of to assess the material’s inflammatory response profile [51]. In this context, the most promising modifications, such as those combining bioceramic composites with growth factors or specific topographies, should undergo rigorous validation in preclinical GBR animal models to evaluate the cellular regenerative performance under physiologic conditions.
This review was deliberately restricted to primary human cells to maximize the physiological relevance of in vitro outcomes in the context of GBR and to reduce methodological artifacts. Immortalized cell lines were excluded because they may exhibit genomic alterations and non-physiological proliferation rates that distort adhesion, ALP, osteogenic marker expression (RUNX2, OCN), and mineralization, compromising the validity of comparisons among PLA/PLGA-based surfaces [14,52]. Accordingly, the methodological scope was defined to obtain mechanistic inferences with higher biological validity in humans and comparable outcomes on native and functionalized PLA/PLGA surfaces, acknowledging that clinical translation will require subsequent preclinical validation in appropriate models.
The next generation of polylactic acid–based biomaterials for GBR should adopt a more explicitly translational approach, emphasizing human-relevant in vitro standards. This includes harmonizing donor reporting and using canonical time points that mirror the temporal dynamics of GBR in clinical settings. Technically, adopting a core outcome set—encompassing cell adhesion and focal adhesion maturation, ALP activity, RUNX2 and OCN expression, and matrix mineralization—would enable more robust comparisons of effect sizes across studies. Technically, adopting a core outcome set —including cell adhesion and focal adhesion maturation, ALP activity, RUNX2 and OCN expression, and matrix mineralization—would enable more robust comparisons of osteogenic effect sizes across studies. Equally important is the explicit evaluation of two-sided membrane designs that decouple bone-facing osteoinductivity from soft-tissue sealing, for instance through asymmetric topographies or surface chemistries. Another key priority is the rigorous quantification of coating and functionalization stability under physiologic conditions, linking retention over time to degradation kinetics, pH shifts, and lactic acid release, and correlating these parameters with cellular responses. Finally, future studies should incorporate immunoregulatory and tissue cross-talk models, such as macrophage–osteoblast and fibroblast–epithelial co-cultures, to better capture early immune polarization, soft-tissue sealing dynamics, and the influence of surface energy and topography on these intercellular processes.
5. Conclusions
This systematic review of in vitro studies using primary human cells shows that polylactic acid-based materials are cytocompatible but relatively bioinert when compared with functionalized surfaces or matrices. Incorporating inorganic phases, optimizing surface topography and energy, and immobilizing or releasing signaling factors into PLA consistently enhance osteoblasts and progenitors’ responses—including cell adhesion, alkaline phosphatase activity, osteogenic differentiation (RUNX2 and OCN expression), and matrix mineralization—compared with native PLA. For human gingival fibroblasts, the available evidence supports its cytocompatibility and potential for soft-tissue sealing, although the body of comparable data is smaller and more heterogeneous.
Persistent knowledge gaps concern the long-term stability of surface modifications and the biological effects of polymer degradation products beyond short-term culture experiments. Taken together, these data support the development of barrier membranes with dual biofunctionality as a promising strategy for guided bone regeneration. Future research should consider standardized outcome measures, followed by its validation applying adequate in vivo GBR models in maxillary bones before clinical translation.
Take-Home Messages
PLA and PLGA are biocompatible but exhibit limited osteogenic potential without functional modification.Inorganic modifications and controlled surface properties improve adhesion, alkaline phosphatase activity, osteogenic differentiation and mineralization.Human gingival fibroblasts show compatibility with polylactic acid-based materials, but the evidence base is small and heterogeneous.Long-term data on polylactic acid-based materials modifications stability and the effects of acidifying degradation of the polymer are lacking.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Buser D. Chappuis V. Belser U.C. Chen S. Implant Placement Post-Extraction in Esthetic Single-Tooth Sites: When Immediate, When Early, When Late?Periodontol. 20002017738410210.1111/prd.1217028000278 · doi ↗ · pubmed ↗
- 2Mizraji G. Davidzohn A. Gursoy M. Gursoy U. Shapira L. Wilensky A. Membrane Barriers for Guided Bone Regeneration: An Overview of Available Biomaterials Periodontol. 2000202393567610.1111/prd.1250237855164 · doi ↗ · pubmed ↗
- 3Buser D. Urban I. Monje A. Kunrath M.F. Dahlin C. Guided Bone Regeneration in Implant Dentistry: Basic Principle, Progress over 35 Years, and Recent Research Activities Periodontol. 200020239392510.1111/prd.1253938194351 · doi ↗ · pubmed ↗
- 4Feng P. Jia J. Liu M. Peng S. Zhao Z. Shuai C. Degradation Mechanisms and Acceleration Strategies of Poly(Lactic Acid) Scaffold for Bone Regeneration Mater. Des.202121011006610.1016/j.matdes.2021.110066 · doi ↗
- 5Chiapasco M. Casentini P. Horizontal Bone-Augmentation Procedures in Implant Dentistry: Prosthetically Guided Regeneration Periodontol. 200020187721324010.1111/prd.1221929478251 · doi ↗ · pubmed ↗
- 6Joseph T.M. Kallingal A. Suresh A.M. Mahapatra D.K. Hasanin M.S. Haponiuk J. Thomas S. 3D Printing of Polylactic Acid: Recent Advances and Opportunities Int. J. Adv. Manuf. Technol.20231251015103510.1007/s 00170-022-10795-y 36644783 PMC 9822698 · doi ↗ · pubmed ↗
- 7Maduka C.V. Alhaj M. Ural E. Habeeb O.M. Kuhnert M.M. Smith K. Makela A.V. Pope H. Chen S. Hix J.M. Polylactide Degradation Activates Immune Cells by Metabolic Reprogramming Adv. Sci.202310230463210.1002/advs.20230463237737614 PMC 10625072 · doi ↗ · pubmed ↗
- 8Shalem A. Yehezkeli O. Fishman A. Enzymatic Degradation of Polylactic Acid (PLA)Appl. Microbiol. Biotechnol.202410841310.1007/s 00253-024-13212-438985324 PMC 11236915 · doi ↗ · pubmed ↗