Real-World Utilization of Midostaurin in Combination with Intensive Chemotherapy for Patients with FLT3 Mutated Acute Myeloid Leukemia: A Multicenter Study
Sema Seçilmiş, Sibel Kabukçu Hacıoğlu, Fehmi Hindilerden, Burhan Turgut, Düzgün Özatlı, Gülsüm Akgün Çağlıyan, Abdulkadir Baştürk, Aslı Yüksel Öztürkmen, Yavuz Katırcılar, Sinem Namdaroğlu, Başak Ünver Koluman, Cenk Sunu, Serdal Korkmaz, Ayşe Uysal, Yusuf Bilen

TL;DR
This study shows midostaurin combined with chemotherapy is effective and well-tolerated for treating FLT3-mutated AML in real-world settings.
Contribution
The study provides real-world evidence of midostaurin's effectiveness and safety in FLT3-mutated AML patients outside clinical trials.
Findings
Midostaurin combined with intensive chemotherapy achieved an 87.7% overall response rate in FLT3-mutated AML patients.
Treatment discontinuation due to intolerance or toxicity was low at 3.5%.
Median overall survival was 21.4 months with 52.6% of patients undergoing allogeneic stem cell transplantation.
Abstract
Background/Objectives: Real-world data on the therapeutic use of FLT3 inhibitors in Turkey remain limited. Therefore, we retrospectively evaluated outcomes from 13 academic centers nationwide, focusing on the multikinase inhibitor midostaurin in patients with newly diagnosed FLT3-mutated acute myeloid leukemia (AML). Methods: We collected comprehensive information regarding treatment efficacy, safety, and tolerability. Results: The overall response rate to intensive chemotherapy (3 + 7) plus midostaurin was 87.7%, with a complete remission rate of 84.2%, consistent with previously reported clinical trial results. Treatment discontinuation due to intolerance or toxicity was low (3.5%). One patient discontinued therapy because of septic shock during induction, and another due to a drug–drug interaction during consolidation. Median overall survival was 21.4 months. Allogeneic stem cell…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
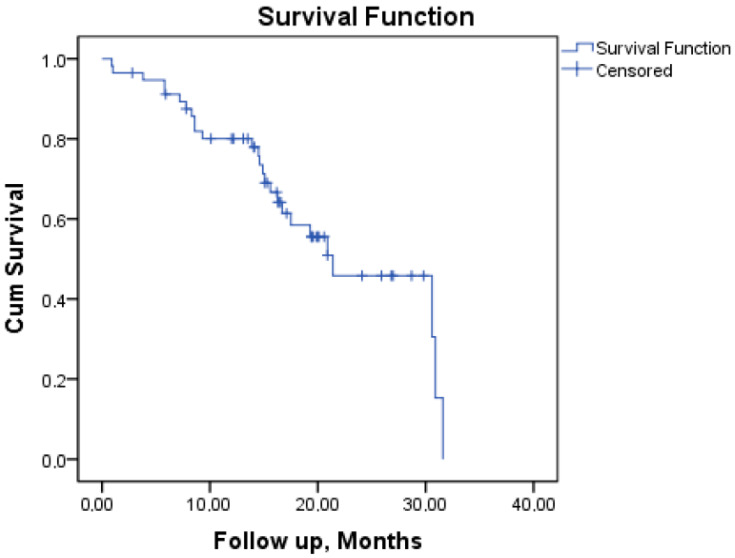 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Chronic Lymphocytic Leukemia Research · Nuclear Structure and Function
1. Introduction
Acute myeloid leukemia (AML) is a group of hematopoietic progenitor stem cell cancers that exhibit varying clinical outcomes due to their cytogenetic and molecular diversity [1]. AML occurs more frequently in males (male–female ratio: 1.5) [2]. The median age at diagnosis exceeds 65 years, and its incidence increases progressively with age [3].
Despite improvements in the treatment of AML, the risk of relapse remains significant. This risk is influenced by the patient’s age and the genetic traits of the leukemia. The five-year relative survival rate for AML is around 35%, but this rate declines to less than 10% for patients older than 65 [4]. Prognostic risk in AML is determined at the time of diagnosis based on specific cytogenetic and molecular abnormalities. Our understanding of the molecular foundations of AML continues to expand. Genetic alterations in AML are recurrent and include amplifications, deletions, rearrangements, and point mutations [1]. These findings guide treatment decisions.
The Fms-like tyrosine kinase 3 gene (FLT3) is a receptor tyrosine kinase expressed by hematopoietic stem and progenitor cells, playing a crucial role in the early stages of developing myeloid and lymphoid lineages. FLT3 mutations disrupt the physiological balance between proliferation and differentiation, leading to overexpression or constitutive activation of the receptor, thereby driving leukemic cell expansion and supporting AML blast survival [5].
Mutations in the FLT3 gene are found in approximately 30% of all AML cases and are particularly common in patients with a normal karyotype. There are two subtypes of FLT3 mutations, with the most prevalent being the internal tandem duplication (ITD), which accounts for 25% of all AML cases. FLT3-ITD is a driver mutation associated with high leukemic burden, poor prognosis, and increased relapse risk. ITD mutations induce constitutive activation of the FLT3 signaling pathway, promoting leukemic proliferation and therapy resistance. The second subtype, FLT3 tyrosine kinase domain (TKD) mutations, occurs in 7–10% of AML cases. Its prognostic significance remains uncertain. Furthermore, FLT3 mutational status is dynamic and may change during the disease course, reinforcing the importance of assessing clonal evolution at diagnosis and relapse [6].
Given the adverse prognostic impact of FLT3 mutations, several small-molecule FLT3 inhibitors have been developed to improve outcomes when combined with intensive chemotherapy. Recent evidence demonstrates that incorporating FLT3 inhibition into frontline AML therapy decreases relapse and improves overall survival, particularly with midostaurin [7]. These findings reinforce the role of FLT3 inhibitors as an important component of intensive induction and consolidation regimens.
Midostaurin is the first FLT3 inhibitor approved for treating adult patients with newly diagnosed AML with FLT3 mutations. It is used in combination with standard induction therapy consisting of cytarabine and daunorubicin, as well as cytarabine for consolidation therapy. Adding midostaurin to the standard intensive chemotherapy regimen [8] was found to improve median event-free survival (EFS) significantly (p = 0.009) and median overall survival (OS) (p = 0.002) [9,10]. This approval is based on the results of the pivotal phase 3 study known as RATIFY [11]. In the RATIFY study, midostaurin was shown to enhance overall survival (OS) in all types of FLT3 mutations, including those with TKD, low allelic ratio ITD, and high allelic ratio ITD, regardless of the FLT3-ITD allelic ratio [10].
The RATIFY study included de novo AML patients aged 18–59; however, midostaurin has received approval for use across all age groups and for newly diagnosed AML patients, including those with secondary AML. In the German–Austrian Acute Myeloid Leukemia Study Group (AMLSG) 16–10 phase 2 clinical trial, midostaurin was demonstrated to be safe and effective, leading to a significant improvement in outcomes for FLT3-ITD positive AML patients aged 60 to 70 years, as well as for younger patients, compared to historical controls [12].
Currently, data regarding the safety and efficacy of midostaurin with an idarubisin-based 7 + 3 AML induction regimen and consolidation therapy with cytarabine in AML populations remain limited. In this study, we conducted a multicenter retrospective analysis of our experience using midostaurin in induction and consolidation therapy. We specifically evaluated the effects and toxicity of adding midostaurin, a multikinase FLT3 inhibitor, to standard chemotherapy in AML patients with FLT3 mutations.
2. Materials and Methods
The study was carried out with the permission of Ankara Dr. Abdurrahman Yurtaslan, Oncology Training and Research Hospital Ethics Committee, on 26 January 2022, with decision number 2022-01/1608. All procedures strictly adhered to the principles outlined in the 1964 Helsinki Declaration, ensuring the ethical conduct of the study. Each patient provided written informed consent prior to participation. Each participating center obtained local ethics approval in accordance with institutional requirements for retrospective data collection.
2.1. Patients and Study Design
This retrospective observational study focused on patients with AML who were newly diagnosed with FLT3 mutations (ITD and/or TKD) through molecular analysis. Eligible patients had not received prior antineoplastic therapy other than hydroxyurea and/or cytarabine for cytoreduction. The study was conducted at 13 academic centers in Turkey between September 2019 and May 2022.
This research included FLT3-positive AML patients aged between 18 and 70 years, with an ECOG performance score of 0 to 2, who were deemed eligible for intensive chemotherapy. Acute promyelocytic leukemia patients were excluded. Patients with significant comorbidities accompanying AML and those with bilirubin levels exceeding 2.5 times the upper limit of the normal range were also excluded.
FLT3 mutation assessment was performed using PCR-based fragment analysis for the identification of both ITD and TKD mutations, according to each center’s standard molecular diagnostic procedures. Allelic ratio measurement was not consistently available across all centers and was therefore not incorporated into the analysis.
These patients received intensive induction chemotherapy in combination with midostaurin, followed by consolidation therapy using cytarabine and midostaurin. Data were collected manually from medical records. All centers used a unified case report form to ensure standardized data extraction, including demographics, laboratory values, molecular findings, treatment details, toxicities, and clinical outcomes. Missing data were handled through complete-case analysis. The institutional review board at each participating center reviewed and approved the trial protocol.
2.2. Treatment Protocol
The same chemotherapy doses and transplantation protocols were consistently utilized across all participating centers throughout the study. The 3 + 7 induction therapy consisted of 12 mg/m^2^ of idarubicin, administered via rapid intravenous injection on days 1, 2, and 3, along with 100 mg/m^2^ of cytarabine, given as a continuous intravenous infusion from days 1 to 7. A bone marrow examination was conducted around day 30 to evaluate remission status.
Patients who achieved complete remission after induction therapy received either medium-dose (1.5 to 2 g/m^2^) or high-dose (3 g/m^2^) cytarabine, with dose reductions at the physician’s discretion based on age and/or comorbidities. This cytarabine was administered as a 3-h infusion every 12 h on days 1, 3, and 5 for a total of 1 to 4 cycles, within a 28-day cycle.
Furthermore, midostaurin was given orally at a dose of 50 mg twice daily for 14 days, starting on the eighth day after initiating induction and consolidation chemotherapy. Midostaurin was not administered if a patient’s corrected QT interval exceeded 500 ms or if they experienced a grade 3 or 4 adverse effect related to midostaurin. Any missed doses of midostaurin were not readministered.
Across all centers, anti-infective prophylaxis (including antibacterial, antiviral, and antifungal agents) was administered according to institutional standards, and all patients received transfusion support based on routine hematologic thresholds. Tumor lysis syndrome prophylaxis (hydration and allopurinol or rasburicase) was provided before induction chemotherapy. Growth factor support (G-CSF) during post-induction marrow aplasia was used at the discretion of the treating physician. Electrocardiographic monitoring was routinely performed during midostaurin administration to assess QTc intervals.
During induction, patients received inpatient care with daily monitoring of complete blood counts, renal and hepatic function tests, and infection parameters. Microbiological cultures, imaging studies, and empirical antibiotic escalation followed center-specific febrile neutropenia guidelines. Similarly, patients were also hospitalized during consolidation therapy, with daily monitoring of laboratory values, toxicity assessments, and infection surveillance in accordance with institutional supportive-care protocols.
The decision to perform allogeneic stem cell transplantation and the timing of the procedure were left to the treating physician’s discretion. Patients who were eligible for transplantation and had an available donor were referred for the procedure during the consolidation treatment process. Institutional policies ensured supportive care throughout therapy. Transplant eligibility evaluation included donor availability, remission status, comorbidity assessment, and institutional transplant board approval. Conditioning regimens (myeloablative or reduced-intensity) and graft-versus-host disease prophylaxis protocols were selected according to the standard practices of each participating center.
2.3. Study Outcomes
The primary endpoint was median overall survival (OS), which was defined as the time from start of induction therapy to death from any cause. Overall response rate (ORR) is defined as the proportion of patients who achieved either a complete remission (CR) or complete remission with incomplete count recovery (CRi). CR was determined by bone marrow blasts < 5% by morphological evaluation, an absolute neutrophil count (ANC) > 1000 cells/μL, and platelet count >100,000/μL (in addition to the absence of circulating blasts, Auer rod-containing blasts, and extramedullary disease). Patients with CRi met all CR criteria except with residual neutropenia (ANC < 1000 cells/μL) or thrombocytopenia (<100,000/μL). Treatment response was evaluated according to standard, internationally accepted criteria for acute myeloid leukemia.
Secondary endpoints were the 30-day mortality rate, the rate of documented infections, and the incidence of adverse events during both induction and consolidation phases. Infections were categorized based on clinical presentation, microbiological identification, or radiologic confirmation. Relapse assessments were recorded according to standard institutional timelines, while bone marrow evaluations for remission assessment were uniformly performed around day 30. Induction mortality was defined as death occurring within the first 30 days of treatment.
Additionally, we analyzed disease- and patient-specific parameters and the toxicity and efficacy results. Toxicity was classified based on the Common Terminology Criteria for Adverse Events (CTCAE) version 4.03 [13], and adverse events were categorized as “any grade” and “grade 3–4” toxicities in accordance with this classification.
2.4. Statistical Analysis
Patient characteristics were summarized using frequencies (numbers and percentages) for categorical variables and median and range for continuous variables. Kaplan-Meier analysis was used for survival analysis. Less than 0.05 was considered statistically significant for all analyses. All statistical analyses were performed with the SPSS software package (Version 26, IBM, Armonk, NY, USA).
3. Results
A total of 57 patients were included in the analysis, with those who survived having a median follow-up period of 15.6 months (ranging from 0.9 to 31.6 months). The median age of the patients was 55 years, ranging from 20 to 70. Among the patients, 31.5% were over the age of 60, and 3.5% were over 70. FLT3-ITD mutations were found in 48 patients, accounting for 84.2% of the group, while FLT3/TKD mutations were identified in 7 patients, representing 12.3%. Additionally, two patients (3.5%) had both TKD and ITD mutations. The majority of patients (86%) had de novo AML. Of the samples studied, 82.5% displayed a normal karyotype, while 21.1% exhibited NPM1 mutations. Details of the patients’ clinical and demographic characteristics are given in Table 1.
Most patients completed the full 14-day course of midostaurin during the induction phase. Treatment was discontinued for two patients (3.5%) due to severe side effects. One patient discontinued treatment due to septic shock during induction therapy, while another patient stopped treatment because of a drug-drug interaction during consolidation therapy. In four patients (7%), dose reductions or treatment interruptions occurred at various stages of therapy. This included two patients who experienced severe sepsis, one patient with a prolonged QT interval, and one patient with severe refractory thrombocytopenia and purpura. See Table 2.
Forty-eight patients (84.2%) achieved CR and two (3.5%) achieved CRi. Death during induction was reported in 2 (3.5%) patients (due to sepsis). Five patients (8.8%) did not respond to the induction therapy. Additionally, relapse was observed in 21.1% of the cases, affecting 12 patients. Median OS was 21.4 months (95% confidence interval [CI]) (See Figure 1). Transplantation was performed at some point during the disease course in 54.4% of the patients (31 patients); it was performed during the first complete remission in 52.6% of the patients. Survival and treatment response outcomes for the overall cohort are seen in Table 3.
The rate of grade 3 or 4 neutropenia, lymphopenia, thrombocytopenia, and anemia was 80.7%, 71.9%, 84.2%, and 68.4%, respectively. Grade 3/4 diarrhea, vomiting, and hypocalcemia were reported in 5.2% of patients each. Grade 3/4 fatigue occurred in 10.5% of patients, while grade 3/4 nausea was seen in 14%. Grade 3/4 hypokalemia was observed in 26.3%, and all these side effects were manageable. Additionally, pneumonitis or pulmonary infiltrates were noted in 43.8% of patients, rectitis in 12.2%, rash in 24.5%, and sepsis in 7%. Other common adverse events during the induction and consolidation courses are summarized in Table 4.
4. Discussion
This multicenter retrospective study evaluated the real-world effectiveness and safety of combining intensive 3 + 7 induction chemotherapy with midostaurin, followed by consolidation therapy, in patients with FLT3-mutated AML treated across 13 centers in Turkey between 2019 and 2022. Our findings contribute to the growing body of evidence supporting FLT3 inhibition in routine clinical practice and offer insight into patient groups underrepresented in pivotal trials.
AML is most commonly diagnosed in older adults, with a median age of 68 years [8]. In contrast, the RATIFY trial included a younger population (median age 47 years; range 18–59) [9] and excluded both patients ≥60 years and those with secondary AML. Although midostaurin has no age-based restrictions, its use in older adults requires careful assessment of comorbidities and fitness for intensive therapy [14]. In a multicenter cohort of patients ≥60 years with newly diagnosed FLT3-mutated AML, midostaurin combined with intensive chemotherapy demonstrated acceptable efficacy [15]. Our study extends these observations by including a substantial proportion of older adults (31.3%) and secondary AML cases, reflecting a more heterogeneous real-world population.
Patients in our study were older overall (median age 55, range 20–70) and had a higher frequency of normal karyotype (82.5%). Baseline leukemic burden was also greater, with a median WBC count of 43,990/μL—approximately 9000 cells/μL higher than in the RATIFY cohort. Moreover, the prevalence of FLT3-ITD was higher in our population (84.2%), while FLT3-TKD mutations were less common (12.3%) compared to RATIFY (77.5% ITD; 22.5% TKD).
Despite these higher-risk characteristics, the real-world CR rate in our study was 84.2%, markedly higher than the 58.9% reported in the RATIFY trial. This finding is notable given the inclusion of older adults, a higher proportion of FLT3-ITD, and patients with secondary AML. The absence of allelic ratio assessment may have influenced the interpretation of FLT3-ITD risk. Additionally, because midostaurin is a multikinase inhibitor, inhibition of other oncogenic pathways may have contributed to improved response rates. Similar favorable outcomes have been reported in other real-world studies evaluating FLT3 inhibitors during induction therapy [16,17,18,19].
Early pharmacovigilance studies identified anemia, rash, nausea, vomiting, and fever as common grade ≥3 events with midostaurin. An FDA Adverse Event Reporting System analysis recorded 5938 midostaurin-related adverse events reported from 2015–2022, with sepsis, pneumonia, and diarrhea being the events most strongly associated with mortality [20]. European Medicines Agency (EMA) reviews similarly identified febrile neutropenia, nausea, exfoliative dermatitis, vomiting, headache, petechiae, and fever as the most frequent adverse reactions [21].
In our study, toxicity patterns largely mirrored expectations for intensive AML therapy. The most common grade 3–4 adverse events were cytopenias and infections, consistent with the RATIFY trial, where febrile neutropenia occurred in 82% and infections in 52% of patients. We observed febrile neutropenia in 82.5% of patients, nearly identical to RATIFY, and the predominant treatment-related deaths were infection-related. Unlike RATIFY, however, no grade ≥3 rash was observed in our cohort. Overall, toxicity profiles remained manageable within standard supportive-care protocols.
Allogeneic stem cell transplantation (allo-SCT) in first CR improves long-term outcomes for patients with FLT3-ITD AML. RATIFY demonstrated that allo-SCT in CR1 was associated with favorable survival outcomes [22].
In RATIFY, 28.1% of patients receiving midostaurin proceeded to allo-SCT in CR1. In our real-world cohort, CR1 transplantation was substantially higher (52.6%), and 54.4% underwent transplantation at any time during the disease course, reflecting national practice patterns and donor availability.
Prior studies have suggested that NPM1/FLT3-ITD genotypes, WBC count at diagnosis, and allo-SCT are independent prognostic factors for OS [23]. In contrast, our study found no significant impact of NPM1 mutation status, FLT3-ITD, FLT3-TKD, WBC count, or transplantation on OS. This may be related to sample size limitations, heterogeneity across centers, lack of allelic ratio data, and relatively short follow-up, emphasizing the need for larger prospective studies.
Overall, this study provides additional real-world evidence supporting the use of midostaurin in FLT3-mutated AML. Our findings confirm high remission rates, manageable toxicity, and transplantation feasibility in routine practice, consistent with clinical trial data. However, larger comparative trials incorporating molecular risk stratification, allelic ratio evaluation, and long-term survival endpoints are needed to refine prognostic interpretation and optimize treatment strategies for this high-risk patient population.
5. Conclusions
This study demonstrates that oral midostaurin, administered at 50 mg twice daily for 14 days beginning on day 8 of induction and consolidation therapy, can be used safely and effectively in patients with FLT3-mutated AML. The regimen showed high remission rates, an acceptable toxicity profile, and remained feasible even in older patients and those with secondary AML. These findings support the continued adoption of FLT3 inhibition in real-world clinical practice, while highlighting the need for larger prospective studies to further clarify prognostic factors and long-term outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Döhner H. Weisdorf D.J. Bloomfield C.D. Acute Myeloid Leukemia N. Engl. J. Med.20153731136115210.1056/NEJ Mra 140618426376137 · doi ↗ · pubmed ↗
- 2Siegel R.L. Miller K.D. Jemal A. Cancer Statistics, 2017 CA Cancer J. Clin.20176773010.3322/caac.2138728055103 · doi ↗ · pubmed ↗
- 3Ferrara F. Lessi F. Vitagliano O. Birkenghi E. Rossi G. Current Therapeutic Results and Treatment Options for Older Patients with Relapsed Acute Myeloid Leukemia Cancers 20191122410.3390/cancers 1102022430769877 PMC 6406399 · doi ↗ · pubmed ↗
- 4Park E.H. Lee H. Won Y.J. Ju H.Y. Oh C.M. Ingabire C. Kong H.J. Park B.K. Yoon J.Y. Eom H.S. Nationwide statistical analysis of myeloid malignancies in Korea: Incidence and survival rate from 1999 to 2012 Blood Res.20155020421710.5045/br.2015.50.4.20426770948 PMC 4705046 · doi ↗ · pubmed ↗
- 5Grafone T. Palmisano M. Nicci C. Storti S. An overview on the role of FLT 3-tyrosine kinase receptor in acute myeloid leukemia: Biology and treatment Oncol. Rev.20126 e 810.4081/oncol.2012.e 825992210 PMC 4419636 · doi ↗ · pubmed ↗
- 6Daver N. Schlenk R.F. Russell N.H. Levis M.J. Targeting FLT 3 mutations in AML: Review of current knowledge and evidence Leukemia 20193329931210.1038/s 41375-018-0357-930651634 PMC 6365380 · doi ↗ · pubmed ↗
- 7Larson R.A. Mandrekar S.J. Huebner L.J. Sanford B.L. Laumann K. Geyer S. Bloomfield C.D. Thiede C. Prior T.W. Döhner K. Midostaurin reduces relapse in FLT 3-mutant acute myeloid leukemia: The Alliance CALGB 10603/RATIFY trial Leukemia 2021352539255110.1038/s 41375-021-01179-433654204 PMC 8591906 · doi ↗ · pubmed ↗
- 8Short N.J. Rytting M.E. Cortes J.E. Acute myeloid leukaemia Lancet 201839259360610.1016/S 0140-6736(18)31041-930078459 PMC 10230947 · doi ↗ · pubmed ↗