Efficacy of Transcatheter Renal Arterial Embolization to Contract Renal Size and Increase Muscle Mass in Patients with Polycystic Kidney Disease
Che-Ming Lin, Tai-Shuan Lai, Ting-Wei Liao, Trianingsih, Ying-Hui Wu, Chun-Jung Cheng, Chih-Horng Wu

TL;DR
This study shows that a medical procedure called renal arterial embolization can shrink kidney size and increase muscle mass in patients with a genetic kidney disease.
Contribution
The study demonstrates that RAE increases muscle mass in PKD patients, a previously unexplored benefit.
Findings
RAE significantly reduced total kidney volume over 12 months.
Psoas and paraspinal muscle areas increased significantly after RAE.
Muscle mass improvement was more pronounced in sarcopenic patients.
Abstract
Background/Objectives: Autosomal dominant polycystic kidney disease (ADPKD) is a major cause of end-stage kidney disease (ESKD), accounting for approximately 5–10% of patients receiving dialysis worldwide. The large and numerous cysts in the liver and kidneys cause abdominal distention and poor appetite. Previous studies showed that renal arterial embolization (RAE) reduces total kidney volume (TKV), increases appetite, and improves quality of life. This article aims to evaluate the efficacy of RAE in increasing psoas muscle (PM) and paraspinal muscle (PS) mass in patients with polycystic kidney disease. Methods: A retrospective study was conducted from May 2016 to December 2020. Thirty-five patients with PKD and ESKD who received RAE were enrolled. The clinical data, including age, sex, body weight, abdominal circumference, and laboratory results, including albumin, creatinine,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
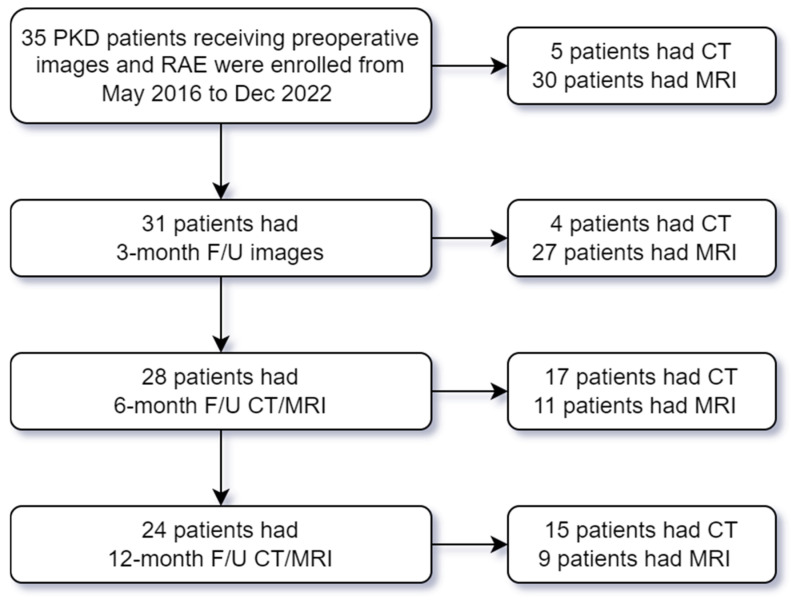 Figure 1
Figure 1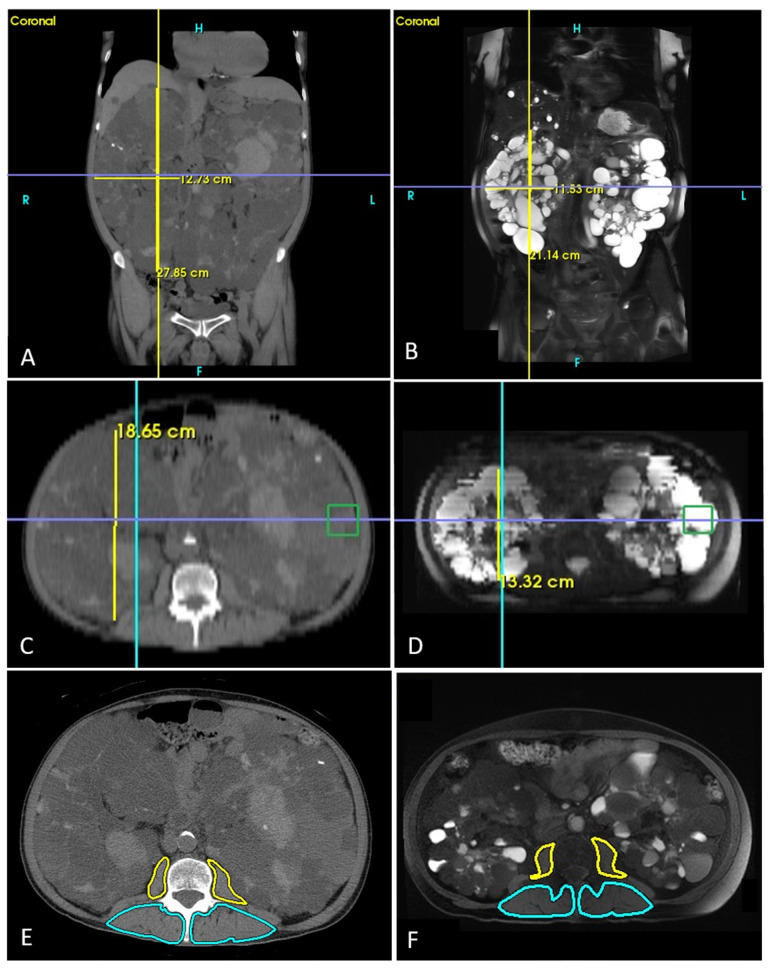 Figure 2
Figure 2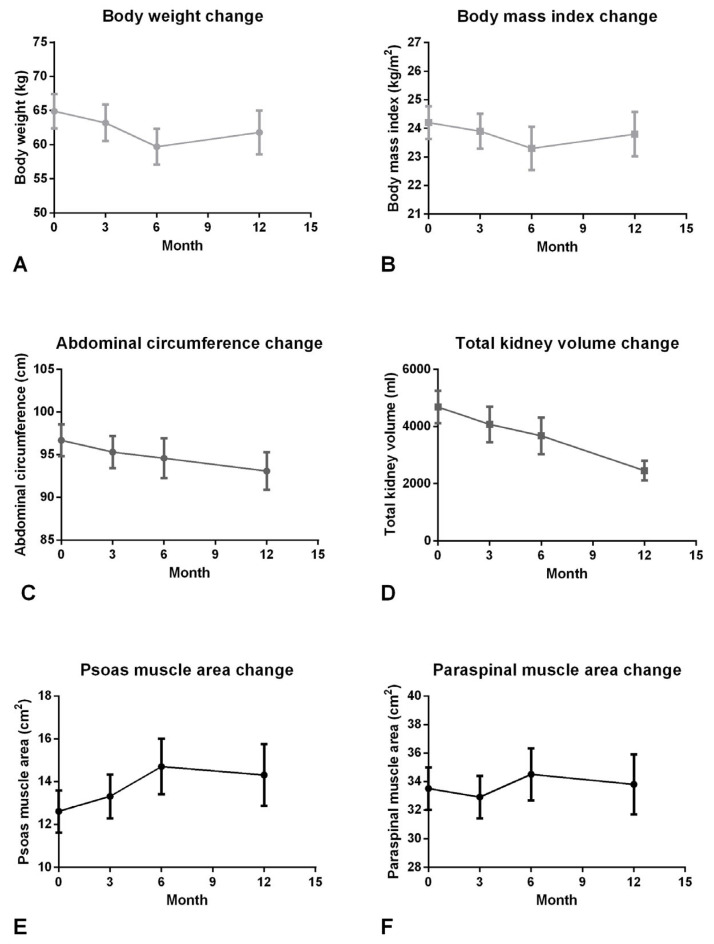 Figure 3
Figure 3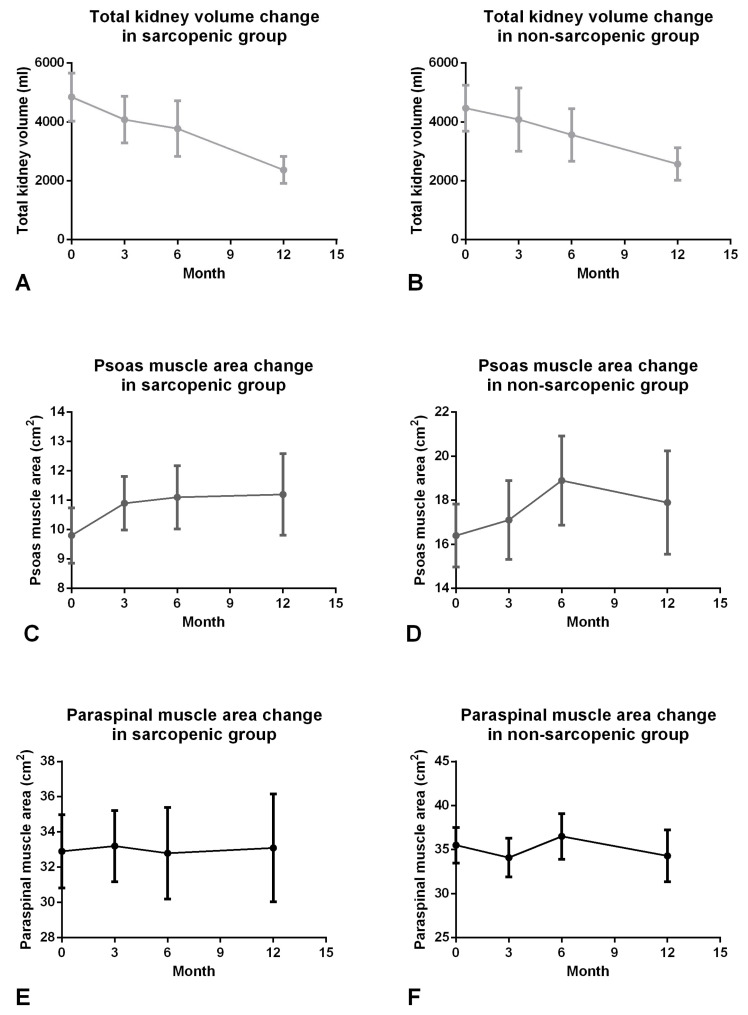 Figure 4
Figure 4- —National Taiwan University Hospital
- —Ministry of Science and Technology
- —National Science and Technology Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and Kidney Cyst Diseases · Renal and Vascular Pathologies · Renal cell carcinoma treatment
1. Introduction
Patients with chronic kidney disease (CKD) and those who undergo dialysis usually present with sarcopenia [1]. A study reported that 20% of patients with end-stage kidney disease (ESKD) undergoing long-term hemodialysis experienced muscle mass loss [2], and another study indicated that patients with muscle wasting had poorer quality of life and prognosis than those without muscle mass loss [3]. In addition, recent studies have demonstrated that CKD is a chronic catabolic condition caused by a persistent imbalance between protein degradation and synthesis in skeletal muscle [4] and is associated with various inflammatory biomarkers [5], a condition known as malnutrition–inflammation (MIA) syndrome. Therefore, exercise, nutrition supplements, and anti-inflammation therapies may help attenuate muscle loss in patients with CKD. In addition, optimization of dialysis therapy, including achieving dialysis adequacy targets such as Kt/V and the use of biocompatible hemodialysis membranes, may further contribute to improving nutritional status and reducing inflammation in patients with CKD [6,7,8].
Polycystic kidney disease (PKD) is the most common hereditary disease causing CKD [9]. Large and numerous cysts in the liver and kidneys cause abdominal distention and poor appetite, accelerating muscle mass loss. In addition, organomegaly also limits physical activity and worsens poor muscle strength and performance. A recent study has demonstrated the inverse correlation between abdominal muscle mass and total kidney volume (TKV) [10]. Therefore, it is challenging to improve sarcopenia and increase muscle mass in patients with PKD.
Ubara et al. first reported a case of PKD with long-term hemodialysis receiving renal artery embolization (RAE) and a series demonstrating RAE reduced the size of numerous cysts in the kidneys and a 46% to 54% decrease in TKV [11,12]. In addition, Yamakoshi et al. showed that RAE could improve lung function in patients with PKD. Suwabe et al. demonstrated that RAE to PKD effectively improved the quality of life and alleviated the symptoms of abdominal fullness and poor appetite [13]. Petitpierre and Del Tatoo et al. also found that some PKD patients contraindicated for kidney transplantation because of excessive renal volume had successful decreases in TKV, making their contraindications withdrawn in 5.6 to 19.5 months on average after RAE [14,15]. However, Ubara et al. and another recent study by Sakuhara have reported that dry weight in patients with PKD continuously decreased in the first half-year and gradually increased six months after RAE [12,16]. These results do not agree with the finding of TKV reduction, and the inconsistency might be explained by changes in body composition, such as muscle gain, which may be masked by the measurement of dry weight only.
Therefore, we hypothesize that RAE can decrease TKV and increase abdominal muscle mass. However, no previous study has quantified the muscle mass change before and after RAE in patients with PKD through cross-sectional imaging. This study aimed to measure the psoas muscle (PM) and paraspinal muscle (PS) areas at the third lumbar vertebral (L3) level at baseline, 3-month, 6-month, and 12-month images after RAE with adjustment of body height (BH) and to investigate the correlation between TKV and muscle mass change.
2. Materials and Methods
2.1. Study Population
A single-center retrospective cohort study was conducted from May 2016 to December 2022 at the National Taiwan University Hospital (NTUH). We enrolled adult patients with PKD under hemodialysis or peritoneal dialysis. The diagnosis of PKD was based on Ravine’s criteria [17]. The inclusion criteria were as follows: (1) patients who underwent computed tomography (CT) or magnetic resonance imaging (MRI) for pre-procedural evaluation, and (2) patients who received RAE within two weeks after imaging evaluation. Follow-up CT or MRI examinations were performed at 3, 6, and 12 months after RAE, and patients were followed until December 2023. Clinical characteristics, laboratory data, and CT or MRI images were retrospectively collected for analysis. The exclusion criteria included the following: (1) incomplete clinical or laboratory data, (2) missing or inadequate CT or MRI images for body composition analysis, and (3) loss to follow-up. The flowchart of patient enrollment is shown in Figure 1. Informed consent was obtained from all subjects involved in the study. This study was approved by the Institutional Review Board of NTUH (No. 201512117RINB and No. 202006139RINA) and registered at ClinicalTrial.gov (NCT05215964).
2.2. Study Variables and Imaging Acquisition
Clinical data, including age, sex, body weight (BW), BH, body mass index (BMI), abdominal circumference (AC), and laboratory data (albumin, hemoglobin, and creatinine levels and estimated glomerular filtration rate [eGFR]) were collected from electronic medical records within two weeks of CT or MRI scans.
Primary outcomes of this study were the changes in TKV and skeletal muscle mass indices after RAE, including PM and PS area and index measured on CT or MRI. Secondary outcomes included changes in anthropometric parameters (BW, BMI, and AC) and laboratory parameters (serum albumin, hemoglobin, and creatinine levels) during follow-up.
If patients had no contraindication for MRI (e.g., claustrophobia, metal implants, or pacemakers) or could tolerate multiple sessions of suspended respiration for image acquisition, we performed MRI because of the absence of radiation exposure during the examination. A 3.0-Tesla unit (Magnetom Verio; Siemens Medical Solutions, Erlangen, Germany) was used for MRI. We performed the following sequences: chemical-shift imaging (Dixon method with the following parameters: repetition time (TR): 9.65 ms/time to echo (TE): 2.45 ms for IP and 3.67 ms for OP, 5 mm slice thickness), coronal T2 half-Fourier acquisition single-shot turbo spin-echo (HASTE) with a TR of 2000 ms, TE of 92 ms, and a slice thickness of 3 mm for the abdomen and pelvis to observe the cyst extension and to determine TKV [18]. In addition, T1 and T2-weighted axial images with fat suppression and a slice thickness of 5 mm were also collected from the xiphoid process to pubic symphysis.
CT scan was performed only in patients with contraindications for MRI or who could not suspend respiration. A 64-slice CT scanner (Lightspeed VCT; GE Medical System, Waukesha, WI, USA) was used with the following parameters: 120 Kv, dose modulation according to body size, and reconstruction with a 1 mm slice thickness. Then, the coronal and axial images of the abdomen and pelvis with 3 mm and 5 mm thickness, respectively. CT or MRI was used to evaluate TKV, PM, and PS muscle, depending on patient compliance and imaging availability. Muscle and kidney measurements were performed using modality-specific, previously reported method [10]. CT- and MRI-based measurements were analyzed separately in the serial follow-up of the same patient, and no direct comparison between the two imaging modalities was intended. We performed only CT or MRI images without contrast injection to avoid contrast-induced nephropathy, which refers to acute deterioration of renal function after iodine-based contrast exposure for CT, or nephrogenic systemic fibrosis, a rare but serious systemic fibrotic disorder associated with gadolinium-based contrast agents for MRI in patients with advanced kidney disease.
2.3. Imaging Processing
TKV was estimated with an ellipsoid formula through multiplanar reformation and measured using the SoliPACS Web Viewer (EBM Technologies, Taipei, Taiwan). First, the maximal longitudinal length (L) of the kidney was determined on coronal CT or T2 HASTE with tilted coronal slices parallel to the long renal axis (Figure 2A,B). Next, the maximal width (W) was determined perpendicular to the L in the same plane where the L was localized. Finally, the maximal depth (D) was determined perpendicular to the L in a sagittal thick slice (Figure 2C,D) [18]. As a result, TKV was estimated as follows:
Non-enhanced CT images and T1-weighted axial images with fat suppression MRI at the L3 level were analyzed to determine PM and PS areas, also processed by SoliPACS Web Viewer (EBM Technologies, Taipei, Taiwan). Contours were obtained using a manual tracing method (Figure 2E,F). A radiologist (C.-H.W.) with 10 years of experience in abdominal imaging processed the images based on the method described previously [19]. The PM and PS indices were calculated as follows:
If patients had a PM index < 6.36 cm^2^/m^2^ in males or <3.92 in females, they were diagnosed with sarcopenia based on a previous study in the Asian population [20].
2.4. Renal Artery Embolization (RAE)
RAE was performed for PKD patients with symptoms such as abdominal distention or hematuria. RAE is a minimally invasive procedure in patients under hemodialysis or peritoneal dialysis in our institute [21]. The RAE was performed via transfemoral puncture after groin area shaving, disinfection with iodine, and local anesthesia with lidocaine. A guidewire is inserted through the femoral artery to the abdominal aorta, and a 5-French sheath (Radiofocus Introducer II; Terumo Cooperation, Tokyo, Japan) is placed at the femoral artery. The renal arteries were catheterized with a 5-French reverse-curve angiographic catheter (RLG, Cook Beacon Tip 5.0 Fr Angiographic Catheter; COOK Medical, Bloomington, IN, USA). While leaving the reverse-curve angiographic catheter placed at either one of the renal arteries, a 2.7-French microcatheter kit (Progreat; Terumo Cooperation, Tokyo, Japan) was inserted into the branches of the renal arteries, which are embolized with multiple platinum pushable coils (Nester and Tornado 0.018″ Microcoil; COOK Medical, Bloomington, IN, USA) and detachable coils (Interlock-18; Boston Scientific, Marlborough, MA, USA or Concerto detachable coil systems; Medtronic, Minneapolis, MN, USA) from distal to stump of renal arteries. We usually left 0.5 to 1.0 cm renal arteries stump without embolization for possible surgical intervention in the future. After embolization, the sheath was removed, and the puncture site of the femoral artery was compressed for at least 5 min, followed by sandbag compression for 4 h and bedrest for 8 h. No major procedure-related complications were observed. Mild post-procedural pain was reported in some patients and was adequately controlled with analgesics. No clinically significant anemia or procedure-related bleeding requiring blood transfusion was noted.
2.5. Statistical Analysis
Data were analyzed using the following tools: Excel 2016 (Microsoft, Redmond, WA, USA) and R 3.4.3. Categorical and continuous variables were compared using the chi-square test and Student’s t-test, respectively. Continuous data were expressed as mean ± standard deviation. Before performing paired t-tests, the normality of continuous variables was assessed using the Shapiro–Wilk test. A paired t-test was used to compare pre- and post-procedural measurements. A two-sided p value < 0.05 was considered statistically significant. We determined the required sample size to be approximately 8 for continuous variables with a paired t-test, assuming a significance of 5% (α = 0.05), a power of 95% (β = 0.05), a mean of 1500 mL with a standard deviation of 1000 mL for TKV. A p-value of <0.05 was considered statistically significant.
3. Results
3.1. Clinical and Laboratory Assessment
We consecutively recruited 35 patients (19 females and 16 males) with a mean age of 59.9 (41–84) years. No patients had mortality during follow-up, and the mean follow-up period was 23.3 months. Among these patients, the indications for renal artery embolization included abdominal distension (n = 29) and hematuria (n = 6). Based on symptom severity and laterality, 22 patients underwent bilateral RAE, 7 underwent right-sided RAE, and 6 underwent left-sided RAE. Twenty-eight patients received hemodialysis, and 7 patients had peritoneal dialysis. The sarcopenic group has a significantly larger age, lower BMI, PM area/index, and creatinine level. The peritoneal dialysis group only has a significant higher creatinine level. The demographic characteristics of the patients are presented in Table 1.
3.2. TKV and Muscle Mass Change After RAE
TKV decreased significantly in 3-, 6-, and 12-month follow-up after RAE compared to baseline images (4684 ± 3361 vs. 4079 ± 3456, 3675 ± 3401, 2459 ± 1706, all p < 0.001; Table 2). The trend of TKV decreases continuously from baseline to 12-month follow-up (Figure 3D). During the follow-up period, no patients required subsequent traditional surgical intervention after RAE. One patient underwent renal transplantation during follow-up. Notably, imaging demonstrated an increased available space in the iliac fossa for graft kidney placement following RAE. Furthermore, the PM area in 3, 6, and 12 months after RAE was significantly larger than the baseline (12.6 ± 5.8 vs. 13.3 ± 5.7, 14.7 ± 6.9, 14.3 ± 7.1, all p < 0.05; Table 2). The PM area continuously increased from baseline to 3-month and 6-month follow-up and became stable after 6-month to 12-month follow-up (Figure 3E). Similarly, the PS area significantly increased from baseline to 6-month follow-up (33.5 ± 8.8 vs. 34.5 ± 9.7, p = 0.013; Figure 3F). On the other hand, there was non-significant decrease in BW and BMI at the 6-month follow-up after RAE (64.9 ± 14.8 vs. 59.7 ± 13.9, p = 0.178 and 24.2 ± 3.4 vs. 23.3 ± 4.0, p = 0.069; Figure 3A,B; Table 2), and there was also a non-significantly continuous decrease trend in AC (96.7 ± 11.0 vs. 95.3 ± 10.4, p = 0.147; 94.6 ± 12.3, p = 0.095; 93.1 ± 10.8, p = 0.380; Figure 3C). The albumin, hemoglobin, creatinine, and eGFR had no significant change before and after the procedure.
3.3. Subgroup Analysis Stratified by the Presence of Sarcopenia and Sex
In total, 10 of 19 female patients and 10 of 16 male patients were diagnosed with PM-defined sarcopenia, according to a previous Asian study [20]. Patients with sarcopenia were significantly older (63.2 ± 8.8 vs. 55.5 ± 7.6, p = 0.010), with a lower BMI (23.0 ± 2.8 vs. 25.9 ± 3.5, p = 0.009), creatinine level (7.9 ± 3.3 vs. 10.6 ± 4.3, p = 0.041), PM area (9.8 ± 4.2 vs. 16.4 ± 5.5, p < 0.001) and index (3.65 ± 1.50 vs. 6.00 ± 1.65, p < 0.001) than non-sarcopenia.
TKV continuously decreased in 3-, 6-, and 12-month follow-up compared to baseline images in sarcopenic (4847 ± 3658 vs. 4079 ± 3456, 3772 ± 3661, 2368 ± 1664, all p < 0.05; Figure 4A and Table 3) and non-sarcopenic groups (4467 ± 3033 vs. 4080 ± 3719, 3562 ± 3219, 2567 ± 1828; Figure 4B and Table 3). The PM are at 3-, 6-, and 12-month follow-ups were also significantly larger than the baseline in the sarcopenic group (9.8 ± 4.2 vs. 10.9 ± 4.0, 11.1 ± 4.2, 11.2 ± 5.0, all p < 0.05; Figure 4C and Table 3). The PS area at 6-, and 12-month follow-up after RAE also had a significant increase compared to the baseline in the sarcopenic group (32.0 ± 9.3 vs. 32.8 ± 10.1, 33.1 ± 11.0, all p < 0.05; Figure 4E and Table 3) but not significant at the 3-month follow-up after RAE. On the other hand, the PM and PS only increased in the 6-month follow-up but did not differ significantly in 3- and 12-month follow-ups in the non-sarcopenic group (Figure 4D,F).
For the gender difference, TKV decreased significantly in 3-, 6-, and 12-month follow-ups compared to baseline images in female and male patients. The PM area and index continuously increased from baseline to the 12-month follow-up in male patients but became stable from the 6-month to the 12-month follow-up in female patients (Table 4).
4. Discussion
This study demonstrated that RAE could effectively decrease TKV and significantly increase PM and PS mass in patients with PKD. Although PM and PS mass increased after RAE, BW and BMI did not differ during 3 to 12-month follow-ups. Sarcopenia is common in patients with CKD because muscle loss is associated with aging and the progression of CKD [1,22]. Furthermore, several studies have also shown that sarcopenia is associated with mortality in patients undergoing hemodialysis or peritoneal dialysis [3,23]. Therefore, possible nutrition supplements, medication, or procedures to recover muscle loss are needed, but many clinical trials have failed to improve muscle mass [24]. Moreover, a recent study indicated that muscle mass was negatively correlated with TKV [10], and another study also demonstrated that minimally invasive intervention may increase muscle mass in patients with liver cirrhosis [25]. Transcatheter RAE is generally preferred over traditional surgery because it is a minimally invasive procedure associated with lower perioperative morbidity and mortality, particularly in patients with ESKD or multiple comorbidities. In addition, it avoids general anesthesia, allows selective targeting of the renal vasculature, and is associated with shorter recovery time compared with surgical nephrectomy [11,12,13,14,15,16]. In our cohort, no major adverse events related to the procedure were observed. Although transient post-embolization pain occurred in a subset of patients, it was self-limited and managed conservatively. No patients experienced significant hemoglobin decline or required blood transfusion following the procedure.
There are many methods to evaluate muscle mass. Previous studies have shown that cross-sectional studies are more robust and stable than bioimpedance and dual-energy X-ray absorptiometry without interference by dialysate or ascites [26,27,28]. CT-based muscle measurement also correlated with lean body mass well [23]. Furthermore, both CT and MRI might evaluate the increment of PM and PS at the same time [25]. The increment of PM and PS mass may imply different mechanisms. The PM is the only flexor connecting the hip girdle, while PS provides postural support of the lumbar spine among the abdominal skeletal muscle. Therefore, CT and MRI can clarify specific muscle groups contributing to particular functions. Many recent studies also proposed PM or PS-defined sarcopenia as a prognostic predictor in patients with pancreatic cancer, hepatocellular carcinoma, liver cirrhosis, and undergoing peritoneal dialysis [23,25,29,30,31,32].
CT and MRI are also essential for pre-operative evaluation before RAE, which can demonstrate the origin of renal arteries from the aorta and estimate TKV by the ellipsoid formula. In patients with PKD, renal parenchyma is replaced by a lot of fluid in the renal cysts. Our study revealed that TKV may be high, up to 4.5 L, and may deviate from the lean body mass based on creatinine kinetics [33,34]. The effect of shrinkage of kidney size in our study is around 50% of the original TKV after RAE, similar to previous studies in patients under hemodialysis or before renal transplantation [11,13]. We also used coils for embolization, a permanent embolizer with a long-term effect and lower side effects than ethanol [16]. Our results also indicated a persistent decrease in TKV from RAE up to 12-month follow-up. On the other hand, the PM and PS had risen to a 6-month follow-up but remained steady at a 12-month follow-up. In addition to symptom relief and muscle gain, RAE may offer an additional clinical benefit by facilitating subsequent renal transplantation. In our cohort, RAE resulted in increased space within the iliac fossa in one case, which may simplify graft kidney placement during transplantation, particularly in patients with PKD characterized by massively enlarged native kidneys. Importantly, no patients required traditional surgery during follow-up, suggesting that RAE can serve as an effective and durable alternative to surgical intervention in selected patients.
We further analyzed the subgroup data stratified by the presence of sarcopenia. We found a continuous increase in PM and PS indices in the sarcopenic group but not in the non-sarcopenic group. The possible reason may be a lower baseline of muscle mass in the sarcopenic group and a relatively higher baseline in the non-sarcopenic group, which made it easier to saturate despite the persistent decrease in TKV. Therefore, the RAE may increase muscle mass more effectively in the sarcopenic group.
In addition, we conducted a subgroup analysis stratified by sex. Although the absolute values of AC, TKV, PM area, and index were lower in females than males, the RAE reduced TKV and increased the PM similarly. Finally, we also found that the BW and BMI decreased until the 6-month follow-up but increased in the 12-month follow-up (Figure 3). The dynamic change in TKV and muscle mass was the possible reason to explain the curve change. However, the persistent decrease in AC still contributed to relieving abdominal distention. As previous studies indicated, the relief of symptoms and the restoration of muscle mass contribute to increased quality of life and lung function [13,35].
Our study has some limitations. First, it is a single-center study with a small number of patients. Nonetheless, our RAE procedure and results are similar to those of other study groups [12,14,16], so the generality to other institutes is possible. The number of enrolled patients in the entire cohort or subgroup analyses is also beyond the sample size requirement (n = 8) in our study design, and we use a paired comparison to minimize the sample size. Second, we did not use the volumetric method to calculate TKV or muscle mass. Although the volumetric method is more accurate for measuring TKV, processing the three-dimensional images is time-consuming. Most studies and guidelines also approved using some formula to estimate TKV [18,36,37,38,39]. Additionally, many studies have revealed a high correlation between the PM area and volume [32,33,34,35], so the PM area at the 3rd lumbar represents PM volume but is very time-saving. Therefore, further large-scale studies with automatic kidney and psoas muscle segmentation are expected. Third, CT and MRI were used interchangeably to assess TKV, PM, and PS based on clinical availability and patient compliance. Although previous studies have used CT and/or MRI to evaluate the change in TKV, PM, and PS [10,24], the concordance of quantitative measurements between CT and MRI has not been fully validated; therefore, direct comparisons between CT- and MRI-derived parameters were not performed. This may limit the comparability of muscle mass assessments across imaging modalities. Fourth, dietary management was provided according to routine clinical practice for dialysis patients; however, detailed dietary intake data were not systematically collected in this study. Finally, there was no mortality in our study during follow-up. The long-term benefits of RAE on survival have been shown [40], but PM change should be further investigated.
5. Conclusions
In conclusion, RAE can effectively decrease TKV and increase muscle mass in PKD patients. The increment of PM and PS was more evident in the sarcopenic group than in the non-sarcopenic group. The RAE showed significant benefits in PKD patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pereira R.A. Cordeiro A.C. Avesani C.M. Carrero J.J. Lindholm B. Amparo F.C. Amodeo C. Cuppari L. Kamimura M.A. Sarcopenia in chronic kidney disease on conservative therapy: Prevalence and association with mortality Nephrol. Dial. Transplant.2015301718172510.1093/ndt/gfv 13325999376 · doi ↗ · pubmed ↗
- 2Isoyama N. Qureshi A.R. Avesani C.M. Lindholm B. Bàràny P. Heimbürger O. Cederholm T. Stenvinkel P. Carrero J.J. Comparative associations of muscle mass and muscle strength with mortality in dialysis patients Clin. J. Am. Soc. Nephrol.201491720172810.2215/CJN.1026101325074839 PMC 4186520 · doi ↗ · pubmed ↗
- 3Kim J.K. Kim S.G. Oh J.E. Lee Y.K. Noh J.W. Kim H.J. Song Y.R. Impact of sarcopenia on long-term mortality and cardiovascular events in patients undergoing hemodialysis Korean J. Intern. Med.20193459960710.3904/kjim.2017.08329161801 PMC 6506738 · doi ↗ · pubmed ↗
- 4Wang X.H. Mitch W.E. Mechanisms of muscle wasting in chronic kidney disease Nat. Rev. Nephrol.20141050451610.1038/nrneph.2014.11224981816 PMC 4269363 · doi ↗ · pubmed ↗
- 5Carrero J.J. Chmielewski M. Axelsson J. Snaedal S. Heimbürger O. Bárány P. Suliman M.E. Lindholm B. Stenvinkel P. Qureshi A.R. Muscle atrophy, inflammation and clinical outcome in incident and prevalent dialysis patients Clin. Nutr.20082755756410.1016/j.clnu.2008.04.00718538898 · doi ↗ · pubmed ↗
- 6Barcellos F.C. Santos I.S. Umpierre D. Bohlke M. Hallal P.C. Effects of exercise in the whole spectrum of chronic kidney disease: A systematic review Clin. Kidney J.2015875376510.1093/ckj/sfv 09926613036 PMC 4655802 · doi ↗ · pubmed ↗
- 7Taskapan H. Baysal O. Karahan D. Durmus B. Altay Z. Ulutas O. Vitamin D and muscle strength, functional ability and balance in peritoneal dialysis patients with vitamin D deficiency Clin. Nephrol.20117611011610.5414/CN 10716021762642 · doi ↗ · pubmed ↗
- 8Hung A.M. Ellis C.D. Shintani A. Booker C. Ikizler T.A. IL-1β receptor antagonist reduces inflammation in hemodialysis patients J. Am. Soc. Nephrol.20112243744210.1681/ASN.201007076021310819 PMC 3060437 · doi ↗ · pubmed ↗